Comparative Epidemiology and Resistance Trends of Common Urinary Pathogens in a Tertiary-Care Hospital: A 10-Year Surveillance Study




Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design, Data Collection
2.2. Identification of Isolates
2.3. Antimicrobial Susceptibility Testing
2.4. Statistical Analysis
3. Results
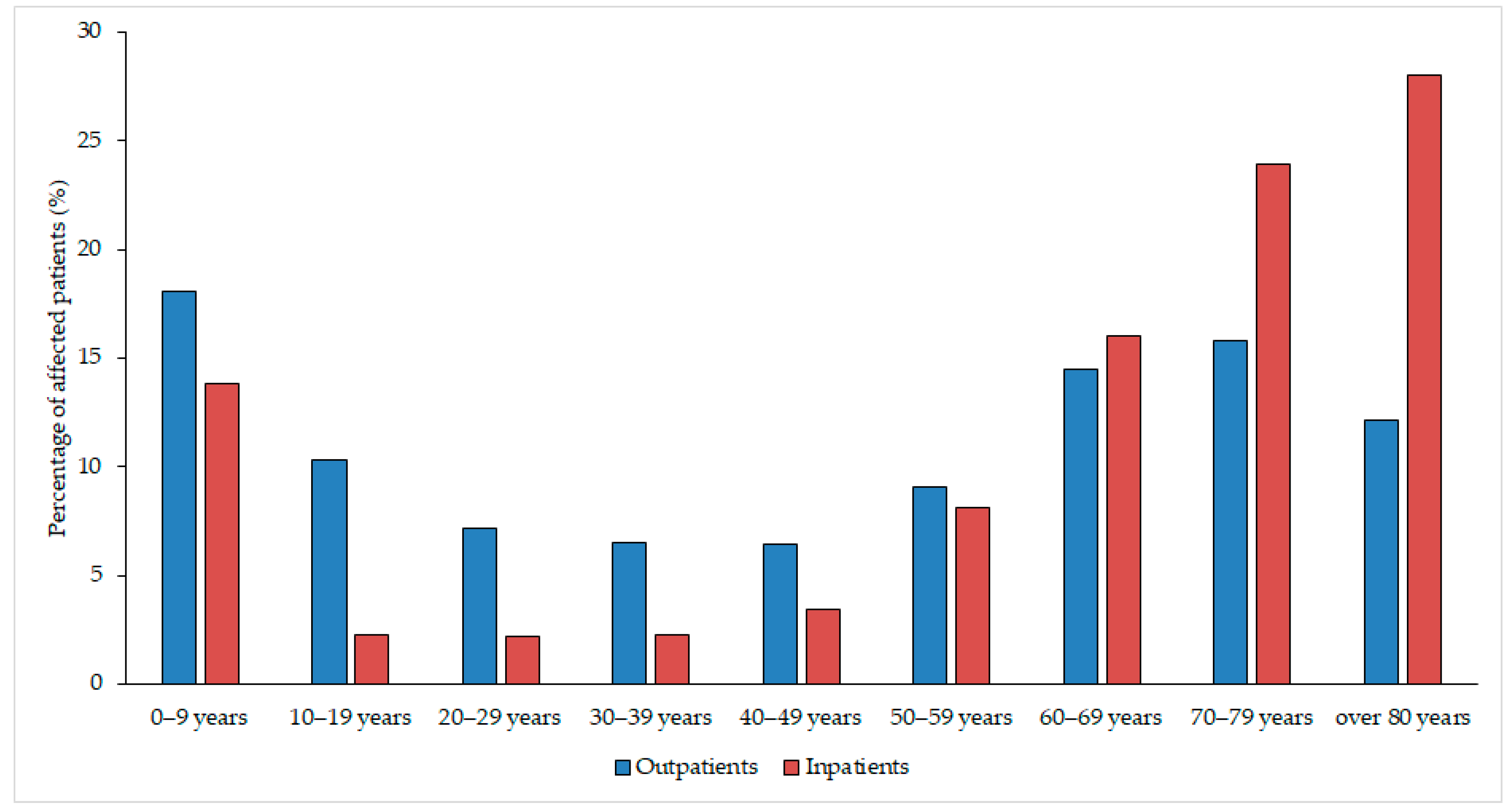
3.1. Demographic Characteristics, Sample Types
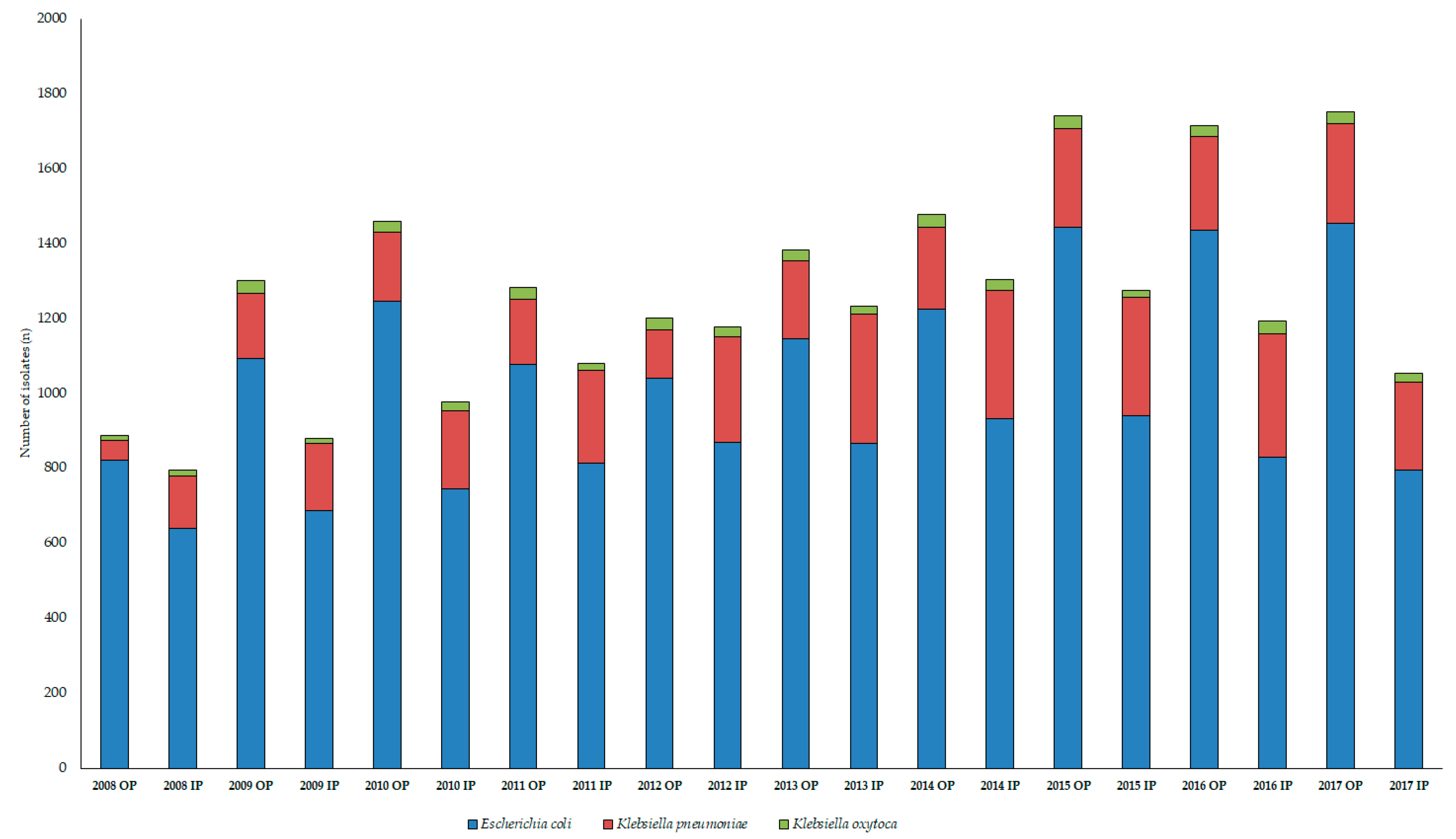
3.2. Epidemiology of Escherichia coli and Klebsiella spp. Isolates
3.3. Antibiotic-Susceptibility Trends among Isolates
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Sobel, J.D.; Kaye, D. 74—Urinary Tract Infections. In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 8th ed.; Bennett, J.E., Dolin, R., Blaser, M.J., Eds.; Elsevier: Philadelphia, PA, USA, 2015; pp. 886–913.e3. ISBN 978-1-4557-4801-3. [Google Scholar]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef] [PubMed]
- Wiedemann, B.; Heisig, A.; Heisig, P. Uncomplicated urinary tract infections and antibiotic resistance-epidemiological and mechanistic aspects. Antibiotics 2014, 3, 341–352. [Google Scholar] [CrossRef]
- Hooton, T.M.; Bradley, S.F.; Cardenas, D.D.; Colgan, R.; Geerlings, S.E.; Rice, J.C.; Saint, S.; Schaeffer, A.J.; Tambayh, P.A.; Tenke, P.; et al. Diagnosis, Prevention, and Treatment of Catheter-Associated Urinary Tract Infection in Adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 625–663. [Google Scholar] [CrossRef] [PubMed]
- Stefaniuk, E.; Suchocka, U.; Bosacka, K.; Hryniewicz, W. Etiology and antibiotic susceptibility of bacterial pathogens responsible for community-acquired urinary tract infections in Poland. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Abbo, L.M.; Hooton, T.M. Antimicrobial Stewardship and Urinary Tract Infections. Antibiotics (Basel) 2014, 3, 174–192. [Google Scholar] [CrossRef] [PubMed]
- Adeolu, M.; Alnajar, S.; Naushad, S.; S Gupta, R. Genome-based phylogeny and taxonomy of the “Enterobacteriales”: proposal for Enterobacterales ord. nov. divided into the families Enterobacteriaceae, Erwiniaceae fam. nov., Pectobacteriaceae fam. nov., Yersiniaceae fam. nov., Hafniaceae fam. nov., Morganellaceae fam. nov., and Budviciaceae fam. nov. Int. J. Syst. Evol. Microbiol. 2016, 66, 5575–5599. [Google Scholar]
- Calzi, A.; Grignolo, S.; Caviglia, I.; Calevo, M.G.; Losurdo, G.; Piaggio, G.; Bandettini, R.; Castagnola, E. Resistance to oral antibiotics in 4569 Gram-negative rods isolated from urinary tract infection in children. Eur. J. Pediatr. 2016, 175, 1219–1225. [Google Scholar] [CrossRef]
- Behzadi, P.; Behzadi, E.; Ranjbar, R. Urinary tract infections and Candida albicans. Cent. Eur. J. Urol. 2015, 68, 96–101. [Google Scholar] [CrossRef]
- Rizwan, M.; Akhtar, M.; Najmi, A.K.; Singh, K. Escherichia coli and Klebsiella pneumoniae Sensitivity/Resistance Pattern Towards Antimicrobial Agents in Primary and Simple Urinary Tract Infection Patients Visiting University Hospital of Jamia Hamdard New Delhi. Drug Res. (Stuttg.) 2018, 68, 415–420. [Google Scholar] [CrossRef]
- Yüksel, S.; Oztürk, B.; Kavaz, A.; Ozçakar, Z.B.; Acar, B.; Güriz, H.; Aysev, D.; Ekim, M.; Yalçinkaya, F. Antibiotic resistance of urinary tract pathogens and evaluation of empirical treatment in Turkish children with urinary tract infections. Int. J. Antimicrob. Agents 2006, 28, 413–416. [Google Scholar] [CrossRef] [PubMed]
- Alexander, B.T.; Marschall, J.; Tibbetts, R.J.; Neuner, E.A.; Dunne, W.M.; Ritchie, D.J. Treatment and clinical outcomes of urinary tract infections caused by KPC-producing Enterobacteriaceae in a retrospective cohort. Clin. Ther. 2012, 34, 1314–1323. [Google Scholar] [CrossRef][Green Version]
- Cullen, I.M.; Manecksha, R.P.; McCullagh, E.; Ahmad, S.; O’Kelly, F.; Flynn, R.; McDermott, T.E.D.; Murphy, P.; Grainger, R.; Fennell, J.P.; et al. An 11-year analysis of the prevalent uropathogens and the changing pattern of Escherichia coli antibiotic resistance in 38,530 community urinary tract infections, Dublin 1999–2009. Ir. J. Med. Sci. 2013, 182, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Behzadi, P.; Behzadi, E.; Yazdanbod, H.; Aghapour, R.; Akbari Cheshmeh, M.; Salehian Omran, D. A survey on urinary tract infections associated with the three most common uropathogenic bacteria. Maedica (Buchar) 2010, 5, 111–115. [Google Scholar] [PubMed]
- Luo, Y.; Ma, Y.; Zhao, Q.; Wang, L.; Guo, L.; Ye, L.; Zhang, Y.; Yang, J. Similarity and divergence of phylogenies, antimicrobial susceptibilities, and virulence factor profiles of Escherichia coli isolates causing recurrent urinary tract infections that persist or result from reinfection. J. Clin. Microbiol. 2012, 50, 4002–4007. [Google Scholar] [CrossRef] [PubMed]
- Terlizzi, M.E.; Gribaudo, G.; Maffei, M.E. UroPathogenic Escherichia coli (UPEC) Infections: Virulence Factors, Bladder Responses, Antibiotic, and Non-antibiotic Antimicrobial Strategies. Front. Microbiol. 2017, 8, 1566. [Google Scholar] [CrossRef]
- Marques, C.; Menezes, J.; Belas, A.; Aboim, C.; Cavaco-Silva, P.; Trigueiro, G.; Telo Gama, L.; Pomba, C. Klebsiella pneumoniae causing urinary tract infections in companion animals and humans: population structure, antimicrobial resistance and virulence genes. J. Antimicrob. Chemother. 2019, 74, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Ejrnæs, K. Bacterial characteristics of importance for recurrent urinary tract infections caused by Escherichia coli. Dan. Med. Bull. 2011, 58, B4187. [Google Scholar]
- Takhar, S.S.; Moran, G.J. Diagnosis and management of urinary tract infection in the emergency department and outpatient settings. Infect. Dis. Clin. North Am. 2014, 28, 33–48. [Google Scholar] [CrossRef]
- Wiles, T.J.; Kulesus, R.R.; Mulvey, M.A. Origins and Virulence Mechanisms of Uropathogenic Escherichia coli. Exp. Mol. Pathol. 2008, 85, 11–19. [Google Scholar] [CrossRef]
- Vading, M.; Nauclér, P.; Kalin, M.; Giske, C.G. Invasive infection caused by Klebsiella pneumoniae is a disease affecting patients with high comorbidity and associated with high long-term mortality. PLoS ONE 2018, 13, e0195258. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Sun, G.; Yu, Y.; Li, N.; Chen, M.; Jin, R.; Jiao, Y.; Wu, H. Increasing occurrence of antimicrobial-resistant hypervirulent (hypermucoviscous) Klebsiella pneumoniae isolates in China. Clin. Infect. Dis. 2014, 58, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Righi, E.; Carnelutti, A.; Graziano, E.; Russo, A. Multidrug-resistant klebsiella pneumoniae: Challenges for treatment, prevention and infection control. Expert Rev. Anti Infect. Ther. 2018, 16, 749–761. [Google Scholar] [CrossRef] [PubMed]
- Bader, M.S.; Loeb, M.; Brooks, A.A. An update on the management of urinary tract infections in the era of antimicrobial resistance. Postgrad. Med. 2017, 129, 242–258. [Google Scholar] [CrossRef] [PubMed]
- Hooton, T.M. The current management strategies for community-acquired urinary tract infection. Infect. Dis. Clin. North Am. 2003, 17, 303–332. [Google Scholar] [CrossRef]
- Kong, K.-F.; Schneper, L.; Mathee, K. Beta-lactam Antibiotics: From Antibiosis to Resistance and Bacteriology. APMIS 2010, 118, 1–36. [Google Scholar] [CrossRef]
- Dhillon, R.H.-P.; Clark, J. ESBLs: A Clear and Present Danger? Crit. Care Res. Pract. 2012, 2012, 625170. [Google Scholar] [CrossRef]
- Rupp, M.E.; Fey, P.D. Extended spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae: considerations for diagnosis, prevention and drug treatment. Drugs 2003, 63, 353–365. [Google Scholar] [CrossRef]
- Paterson, D.L.; Bonomo, R.A. Extended-spectrum beta-lactamases: A clinical update. Clin. Microbiol. Rev. 2005, 18, 657–686. [Google Scholar] [CrossRef]
- Jacoby, G.A. AmpC beta-lactamases. Clin. Microbiol. Rev. 2009, 22, 161–182. [Google Scholar] [CrossRef]
- Hanson, N.D. AmpC β-lactamases: what do we need to know for the future? J. Antimicrob. Chemother. 2003, 52, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Bush, K. Past and Present Perspectives on β-Lactamases. Antimicrob. Agents Chemother. 2018, 62, e01076-18. [Google Scholar] [CrossRef] [PubMed]
- Leclercq, R.; Cantón, R.; Brown, D.F.J.; Giske, C.G.; Heisig, P.; MacGowan, A.P.; Mouton, J.W.; Nordmann, P.; Rodloff, A.C.; Rossolini, G.M.; et al. EUCAST expert rules in antimicrobial susceptibility testing. Clin. Microbiol. Infect. 2013, 19, 141–160. [Google Scholar] [CrossRef] [PubMed]
- Bilchenko, A.V.; Chub, O.I. Prevalence of Types TEM, SHV and CTX-M βLES Among Pathogens of Chronic Pyelonephritis. Antibiot. Khimioter. 2014, 59, 24–26. [Google Scholar] [PubMed]
- Cantón, R.; González-Alba, J.M.; Galán, J.C. CTX-M Enzymes: Origin and Diffusion. Front. Microbiol. 2012, 3, 110. [Google Scholar] [CrossRef] [PubMed]
- Bonkat, G.; Müller, G.; Rieken, M.; Frei, R.; Widmer, A.F.; Feicke, A.; Wyler, S.; Rentsch, C.A.; Ebinger-Mundorff, N.; Subotic, S.; et al. Epidemiology of urinary tract infections caused by extended-spectrum beta-lactamase (ESBL) producing pathogens at a tertiary care swiss University Hospital. J. Urol. 2011, 185, e545. [Google Scholar] [CrossRef]
- Walker, K.J.; Lee, Y.R.; Klar, A.R. Clinical Outcomes of Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae Infections with Susceptibilities among Levofloxacin, Cefepime, and Carbapenems. Can. J. Infect. Dis. Med. Microbiol. 2018, 2018, 3747521. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.; Lyman, A.; Gupta, K.; Mahoney, M.V.; Snyder, G.M.; Hirsch, E.B. Clinical Management of an Increasing Threat: Outpatient Urinary Tract Infections Due to Multidrug-Resistant Uropathogens. Clin. Infect. Dis. 2016, 63, 960–965. [Google Scholar] [CrossRef]
- Hsieh, C.-J.; Shen, Y.-H.; Hwang, K.-P. Clinical implications, risk factors and mortality following community-onset bacteremia caused by extended-spectrum β-lactamase (ESBL) and non-ESBL producing Escherichia coli. J. Microbiol. Immunol. Infect. 2010, 43, 240–248. [Google Scholar] [CrossRef]
- Pallett, A.; Hand, K. Complicated urinary tract infections: Practical solutions for the treatment of multiresistant gram-negative bacteria. J. Antimicrob. Chemother. 2010, 65, iii25–iii33. [Google Scholar] [CrossRef]
- Sherry, N.; Howden, B. Emerging Gram negative resistance to last-line antimicrobial agents fosfomycin, colistin and ceftazidime-avibactam—Epidemiology, laboratory detection and treatment implications. Expert Rev. Anti Infect. Ther. 2018, 16, 289–306. [Google Scholar] [CrossRef] [PubMed]
- Beuk, C.; Hill, C.; Whitehead, S.; Blondel-Hill, E.; Wagner, K.; Cheeptham, N. Determination of susceptibility to fosfomycin and tigecycline of Enterobacteriaceae, particularly Escherichia coli isolates, producing extended-spectrum β-lactamases from multiple regional Canadian hospitals. Can. J. Infect. Dis. Med. Microbiol. 2013, 24, e80–e82. [Google Scholar] [CrossRef] [PubMed]
- Gajdács, M. Extra deaths due to pandrug resistant bacteria: A survey of the literature. Egészségfejlesztés 2019, 60, 31–36. [Google Scholar]
- Chapman, A.L.N. Outpatient parenteral antimicrobial therapy. BMJ 2013, 346, f1585. [Google Scholar] [CrossRef] [PubMed]
- Denes, E.; Prouzergue, J.; Ducroix-Roubertou, S.; Aupetit, C.; Weinbreck, P. Antibiotic prescription by general practitioners for urinary tract infections in outpatients. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 3079–3083. [Google Scholar] [CrossRef] [PubMed]
- Bryce, A.; Hay, A.D.; Lane, I.F.; Thornton, H.V.; Wootton, M.; Costelloe, C. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: systematic review and meta-analysis. BMJ 2016, 352, i939. [Google Scholar] [CrossRef]
- Fasugba, O.; Mitchell, B.G.; Mnatzaganian, G.; Das, A.; Collignon, P.; Gardner, A. Five-Year Antimicrobial Resistance Patterns of Urinary Escherichia coli at an Australian Tertiary Hospital: Time Series Analyses of Prevalence Data. PLoS ONE 2016, 11, e0164306. [Google Scholar] [CrossRef]
- Magyar, A.; Köves, B.; Nagy, K.; Dobák, A.; Arthanareeswaran, V.K.A.; Bálint, P.; Wagenlehner, F.; Tenke, P. Spectrum and antibiotic resistance of uropathogens between 2004 and 2015 in a tertiary care hospital in Hungary. J. Med. Microbiol. 2017, 66, 788–797. [Google Scholar] [CrossRef]
- Yang, B.; Yang, F.; Wang, S.; Wang, Q.; Liu, Z.; Feng, W.; Sun, F.; Xia, P. Analysis of the spectrum and antibiotic resistance of uropathogens in outpatients a tertiary hospital. J. Chemother. 2018, 30, 145–149. [Google Scholar] [CrossRef]
- Morrissey, I.; Hackel, M.; Badal, R.; Bouchillon, S.; Hawser, S.; Biedenbach, D. A Review of Ten Years of the Study for Monitoring Antimicrobial Resistance Trends (SMART) from 2002 to 2011. Pharmaceuticals (Basel) 2013, 6, 1335–1346. [Google Scholar] [CrossRef]
- Sader, H.S.; Farrell, D.J.; Flamm, R.K.; Jones, R.N. Antimicrobial susceptibility of Gram-negative organisms isolated from patients hospitalised with pneumonia in US and European hospitals: Results from the SENTRY Antimicrobial Surveillance Program, 2009–2012. Int. J. Antimicrob. Agents 2014, 43, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Gajdács, M.; Paulik, E.; Szabó, A. The opinions of community pharmacists related to antibiotic use and resistance. Acta Pharmaceutica Hungarica 2018, 88, 249–252. (In Hungarian) [Google Scholar]
- Gajdács, M.; Paulik, E.; Szabó, A. The attitude of community pharmacists towards their widening roles in the prevention and treatment of infectious diseases in the southeast region of Hungary. Gyógyszerészet 2019, 63, 26–30. (In Hungarian) [Google Scholar]
- National Health Insurance Fund of Hungary. Hospital Bed Count and Patient Turnover Report 2017; National Health Insurance Fund of Hungary: Budapest, Hungary, 2017. [Google Scholar]
- Gajdács, M.; Spengler, G.; Urbán, E. Identification and Antimicrobial Susceptibility Testing of Anaerobic Bacteria: Rubik’s Cube of Clinical Microbiology? Antibiotics (Basel) 2017, 6, 25. [Google Scholar] [CrossRef] [PubMed]
- Ábrók, M.; Lázár, A.; Szécsényi, M.; Deák, J.; Urbán, E. Combination of MALDI-TOF MS and PBP2’ latex agglutination assay for rapid MRSA detection. J. Microbiol. Methods 2018, 144, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Nagy, E.; Becker, S.; Kostrzewa, M.; Barta, N.; Urban, E. The value of MALDI-TOF MS for the identification of clinically relevant anaerobic bacteria in routine laboratories. J. Med. Microbiol. 2012, 61, 1393–1400. [Google Scholar] [CrossRef]
- Benkő, R.; Matuz, M.; Hajdú, E.; Bor, A.; Doró, P.; Viola, R.; Soós, G. Antibiotic use in the Hungarian hospitals in the last two decades (1996–2015). Orv. Hetil. 2016, 157, 1839–1846. [Google Scholar] [CrossRef]
- Matuz, M.; Benkő, R.; Hajdú, E.; Viola, R.; Soós, G. Evaluation of ambulatory antibiotic use in Hungary using drug-specific quality indicators. Orv. Hetil. 2013, 154, 947–956. [Google Scholar] [CrossRef]
- Garau, J. Other antimicrobials of interest in the era of extended-spectrum beta-lactamases: fosfomycin, nitrofurantoin and tigecycline. Clin. Microbiol. Infect. 2008, 14 (Suppl. 1), 198–202. [Google Scholar] [CrossRef]
- Al-Zarouni, M.; Senok, A.; Al-Zarooni, N.; Al-Nassay, F.; Panigrahi, D. Extended-spectrum β-lactamase-producing Enterobacteriaceae: In vitro susceptibility to fosfomycin, nitrofurantoin and tigecycline. Med. Princ. Pract. 2012, 21, 543–547. [Google Scholar] [CrossRef]
- European Antimicrobial Resistance Surveillance Network (EARS-Net). Available online: https://ecdc.europa.eu/en/about-us/partnerships-and-networks/disease-and-laboratory-networks/ears-net (accessed on 28 May 2019).
- Hsueh, P.-R.; Chen, W.-H.; Luh, K.-T. Relationships between antimicrobial use and antimicrobial resistance in Gram-negative bacteria causing nosocomial infections from 1991–2003 at a university hospital in Taiwan. Int. J. Antimicrob. Agents 2005, 26, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Spengler, G.; Kincses, A.; Gajdacs, M.; Amaral, L. New Roads Leading to Old Destinations: Efflux Pumps as Targets to Reverse Multidrug Resistance in Bacteria. Molecules 2017, 22, 468. [Google Scholar] [CrossRef] [PubMed]
- Rice, L.B. Mechanisms of Resistance and Clinical Relevance of Resistance to β-Lactams, Glycopeptides, and Fluoroquinolones. Mayo Clin. Proc. 2012, 87, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Melegh, S.; Schneider, G.; Horváth, M.; Jakab, F.; Emődy, L.; Tigyi, Z. Identification and characterization of CTX-M-15 producing Klebsiella pneumoniae clone ST101 in a Hungarian university teaching hospital. Acta Microbiol. Immunol. Hung. 2015, 62, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Tandogdu, Z.; Wagenlehner, F.M.E. Global epidemiology of urinary tract infections. Curr. Opin. Infect. Dis. 2016, 29, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Van Duin, D.; Doi, Y. The global epidemiology of carbapenemase-producing Enterobacteriaceae. Virulence 2016, 8, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef]
- Codjoe, F.S.; Donkor, E.S. Carbapenem Resistance: A Review. Med. Sci. (Basel) 2017, 6, 1. [Google Scholar] [CrossRef]
- Matuz, M.; Benko, R.; Doro, P.; Hajdu, E.; Nagy, G.; Nagy, E.; Monnet, D.L.; Soos, G. Regional variations in community consumption of antibiotics in Hungary, 1996–2003. Br. J. Clin. Pharmacol. 2006, 61, 96–100. [Google Scholar] [CrossRef]
- European Surveillance of Antimicrobial Consumption Network (ESAC-Net). Available online: http://ecdc.europa.eu/en/about-us/partnerships-and-networks/disease-and-laboratory-networks/esac-net (accessed on 28 May 2019).
- Gajdács, M. The Concept of an Ideal Antibiotic: Implications for Drug Design. Molecules 2019, 24, 892. [Google Scholar] [CrossRef]
- Candel, F.J.; Peñuelas, M. Delafloxacin: Design, development and potential place in therapy. Drug Des. Devel. Ther. 2017, 11, 881–891. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discovery, and Development of New Antibiotics; WHO: Geneva, Switzerland, 2017; pp. 1–7. [Google Scholar]
- Gajdács, M.; Dóczi, I.; Ábrók, M.; Lázár, A.; Burián, K. Epidemiology of candiduria and Candida urinary tract infections in inpatients and outpatients: Results from a 10-year retrospective survey. Cent. Eur. J. Urol. 2019, 72, 209–214. [Google Scholar]
- Gajdács, M.; Ábrók, M.; Lázár, A.; Burián, K. Susceptibility patterns of extended-spectrum beta-lactamase-producing (ESBL) urinary pathogens: single-center experience. Gyógyszerészet 2019. accepted. (In Hungarian) [Google Scholar]
- Gajdács, M.; Urbán, E. Resistance Trends and Epidemiology of Citrobacter-Enterobacter-Serratia in Urinary Tract Infections of Inpatients and Outpatients (RECESUTI): A 10-Year Survey. Medicina (Kaunas) 2019, 55, 285. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | Statistics | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CIP R% | Outpatient | 13.28 | 16.12 | 21.53 | 21.80 | 19.13 | 21.64 | 21.31 | 25.57 | 25.69 | 25.95 | p = 0.0003 |
| Inpatient | 20.19 | 23.62 | 26.85 | 33.42 | 37.28 | 38.41 | 34.73 | 40.60 | 40.41 | 33.25 | ||
| NIT R% | Outpatient | 4.99 | 7.33 | 12.37 | 9.00 | 6.06 | 3.05 | 3.59 | 3.12 | 2.42 | 1.03 | n.s. (p = 0.264) |
| Inpatient | 7.98 | 12.39 | 20.81 | 17.57 | 7.36 | 3.34 | 5.04 | 2.76 | 2.05 | 1.39 | ||
| GEN R% | Outpatient | 3.17 | 5.77 | 6.35 | 7.51 | 5.58 | 4.54 | 6.37 | 7.76 | 5.16 | 6.88 | p < 0.0001 |
| Inpatient | 7.82 | 8.75 | 11.68 | 14.62 | 16.69 | 19.84 | 17.01 | 17.85 | 18.21 | 13.10 | ||
| SUM R% | Outpatient | 21.44 | 22.16 | 23.61 | 25.32 | 20.87 | 24.69 | 24.82 | 26.68 | 24.88 | 28.08 | n.s. (p = 0.189) |
| Inpatient | 25.82 | 22.45 | 21.34 | 25.55 | 11.62 | 35.29 | 34.83 | 36.24 | 39.08 | 28.21 | ||
| CRO R% | Outpatient | 8.99 | 7.74 | 7.55 | 7.33 | 5.58 | 6.46 | 8.57 | 9.56 | 8.85 | 9.70 | p = 0.0003 |
| Inpatient | 6.10 | 12.39 | 16.24 | 18.55 | 20.48 | 26.99 | 40.94 | 25.19 | 30.41 | 20.03 | ||
| ESBL% | Outpatient | 6.31 | 4.33 | 5.50 | 6.94 | 9.15 | 7.32 | 9.02 | p = 0.0028 | |||
| Inpatient | 8.85 | 10.59 | 25.72 | 38.97 | 23.06 | 29.08 | 18.39 | |||||
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | Statistics | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CIP R% | Outpatient | 37.31 | 41.48 | 45.16 | 35.47 | 40.77 | 40.38 | 33.03 | 38.78 | 31.60 | 34.08 | n.s. (p = 0.641) |
| Inpatient | 23.40 | 30.00 | 35.10 | 37.50 | 34.28 | 35.76 | 48.40 | 45.57 | 38.18 | 37.45 | ||
| GEN R% | Outpatient | 27.69 | 34.09 | 25.81 | 24.53 | 27.69 | 27.40 | 21.10 | 28.14 | 18.80 | 19.10 | p = 0.0002 |
| Inpatient | 26.24 | 13.33 | 14.42 | 13.31 | 16.96 | 15.41 | 17.99 | 16.14 | 16.36 | 13.62 | ||
| SUM R% | Outpatient | 25.38 | 39.77 | 33.33 | 35.00 | 33.08 | 35.58 | 37.61 | 39.16 | 32.80 | 37.45 | n.s. (p = 0.399) |
| Inpatient | 27.66 | 21.67 | 34.62 | 30.24 | 23.43 | 29.07 | 43.15 | 43.99 | 36.06 | 35.74 | ||
| CRO R% | Outpatient | 23.85 | 31.25 | 37.63 | 26.74 | 36.15 | 35.10 | 27.52 | 35.36 | 27.20 | 25.09 | p = 0.132 |
| Inpatient | 23.40 | 21.11 | 17.31 | 20.56 | 23.67 | 19.77 | 41.98 | 28.48 | 38.18 | 25.79 | ||
| ESBL% | Outpatient | 26.74 | 30.00 | 31.73 | 25.69 | 34.22 | 26.00 | 23.22 | p = 0.243 | |||
| Inpatient | 10.89 | 13.43 | 18.60 | 33.53 | 28.48 | 36.06 | 23.36 | |||||
| Local Resistance Data (2008–2012) | EARS-Net Surveillance Data for Hungary; 2012 [63] | Local Resistance Data (2013–2017) | EARS-Net Surveillance Data for Hungary; 2017 [63] | ||
|---|---|---|---|---|---|
| 3rd generation cephalosporins | E. coli | 5.58–26.99% | 17.40% | 6.46–40.94% | 20.10% |
| Klebsiella spp. | 17.31–37.63% | 43.00% | 19.77–35.36% | 41.10% | |
| Fluoroquinolones | E. coli | 13.28–21.80% | 28.90% | 21.31–25.95% | 30.60% |
| Klebsiella spp. | 23.40–45.16% | 41.60% | 31.60–48.40% | 41.45% | |
| Aminoglycosides | E. coli | 3.17–16.69% | 15.10% | 4.54–19.84% | 17.10% |
| Klebsiella spp. | 13.31–34.09% | 37.80% | 18.80–27.40% | 41.50% | |
| Carbapenems | E. coli | <0.05% | <0.05% | <0.05% | 0.10% |
| Klebsiella spp. | <0.05% | 0.30% | <0.05% | 0.30% | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gajdács, M.; Ábrók, M.; Lázár, A.; Burián, K. Comparative Epidemiology and Resistance Trends of Common Urinary Pathogens in a Tertiary-Care Hospital: A 10-Year Surveillance Study. Medicina 2019, 55, 356. https://doi.org/10.3390/medicina55070356
Gajdács M, Ábrók M, Lázár A, Burián K. Comparative Epidemiology and Resistance Trends of Common Urinary Pathogens in a Tertiary-Care Hospital: A 10-Year Surveillance Study. Medicina. 2019; 55(7):356. https://doi.org/10.3390/medicina55070356
Chicago/Turabian StyleGajdács, Márió, Marianna Ábrók, Andrea Lázár, and Katalin Burián. 2019. "Comparative Epidemiology and Resistance Trends of Common Urinary Pathogens in a Tertiary-Care Hospital: A 10-Year Surveillance Study" Medicina 55, no. 7: 356. https://doi.org/10.3390/medicina55070356
APA StyleGajdács, M., Ábrók, M., Lázár, A., & Burián, K. (2019). Comparative Epidemiology and Resistance Trends of Common Urinary Pathogens in a Tertiary-Care Hospital: A 10-Year Surveillance Study. Medicina, 55(7), 356. https://doi.org/10.3390/medicina55070356