Comparison of the Body Composition of Caucasian Young Normal Body Mass Women, Measured in the Follicular Phase, Depending on the Carbohydrate Diet Level




Abstract
1. Introduction
2. Materials and Methods
2.1. Recruitment of Participants and Inclusion Criteria
2.2. Study Design
2.2.1. Preparation for the Measurement
2.2.2. Dietary Record
2.2.3. Bioelectrical Impedance Measurement
2.3. Statistical Analysis
- (1)
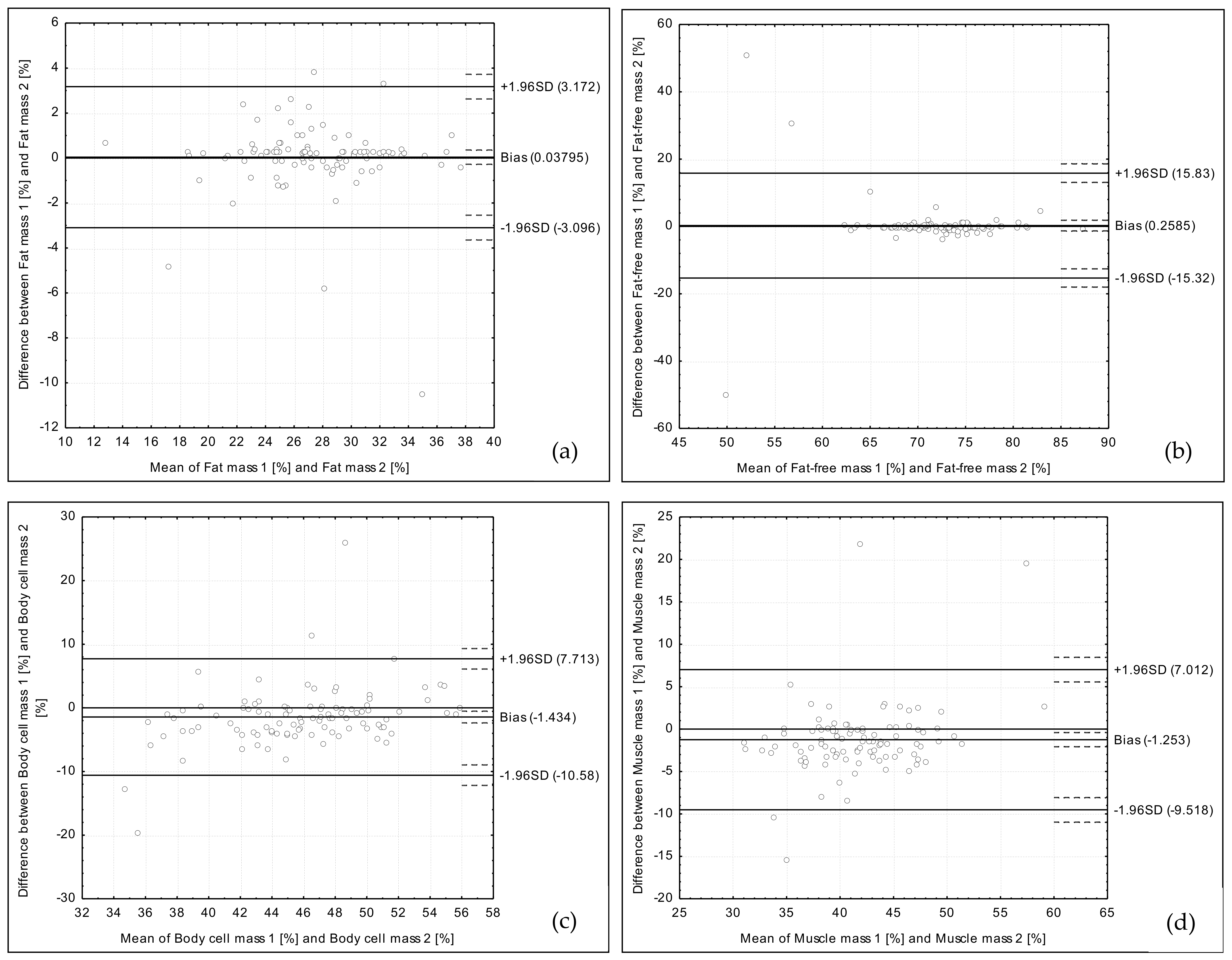
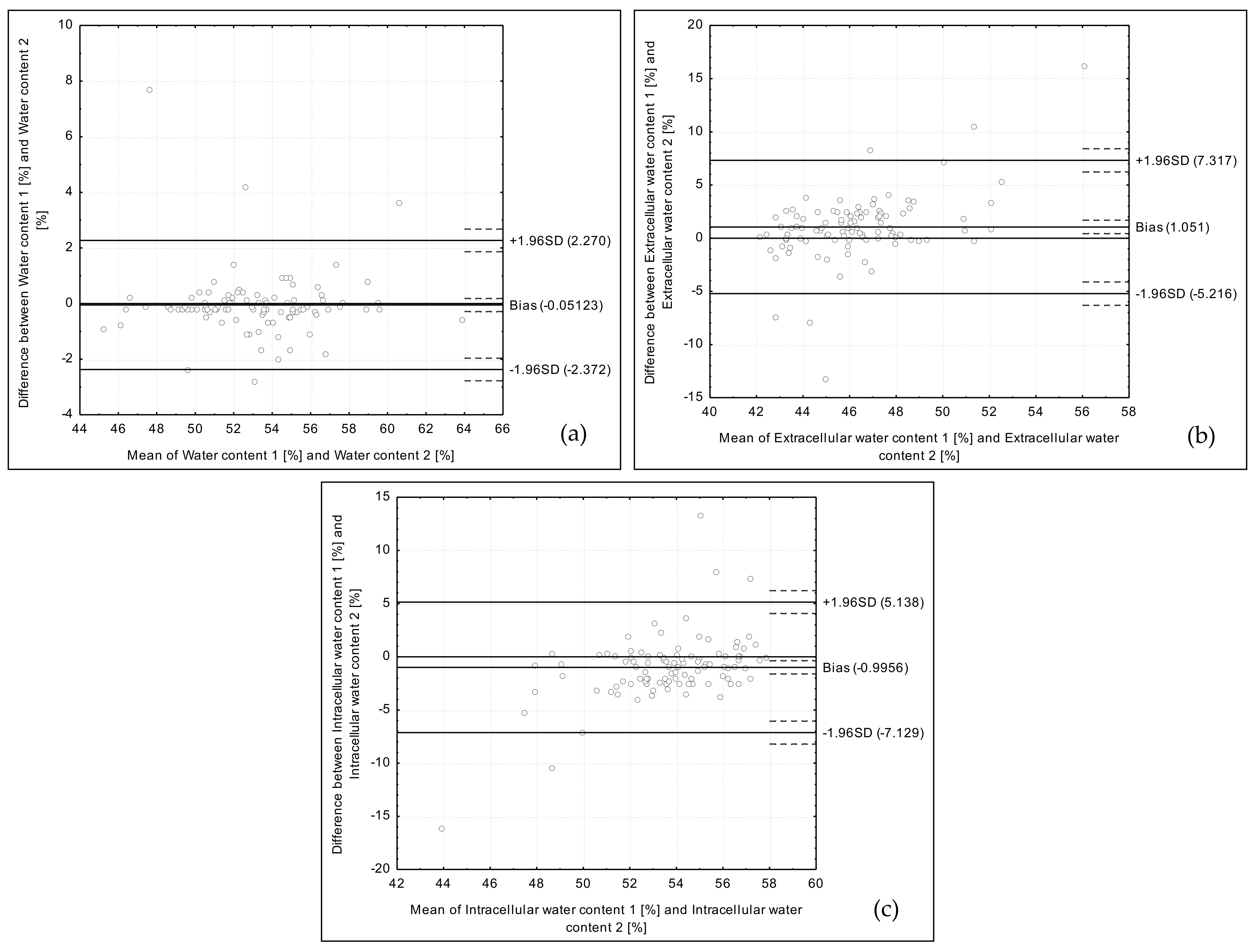
- validation of the reproducibility of obtained data of the body composition assessment (fat mass, fat-free mass, body cell mass, muscle mass, water content, extracellular water content, and intracellular water content) conducted using two types of bioelectrical impedance devices,
- (2)
- comparison of the data of the body composition assessment conducted using the bioelectrical impedance, obtained for groups of participants characterized by carbohydrate content lower than 50% of the energy value of the diet (n = 55), and higher than 50% of the energy value of the diet (n = 45).
- (1)
- Analysis of the Bland–Altman plots—a Bland–Altman index ≤5% (attributed to 95% of individuals observed to be within the LOA) was interpreted as a positive validation of the method [30], while a Bland–Altman index ≤10% (attributed to 90% of individuals observed to be within the LOA) was interpreted as a borderline significant [31].
- (2)
- Analysis of the correlations between results conducted using Pearson correlation (for the parametric distribution) or Spearman’s rank correlation (for the nonparametric distribution), while the distribution was assessed using the Shapiro-Wilk test.
- (3)
- Analysis of the quartiles cross-classification.
- (4)
- Analysis of the weighted κ statistic with linear weighting for quartiles cross-classification—values lower than 0.20 were interpreted as slight agreement, 0.21–0.40—fair, 0.41–0.60—moderate, 0.61–0.80—substantial, and 0.81–1.0—almost perfect agreement [32].
3. Results
4. Discussion
4.1. Carbohydrate Intake Level
4.2. Water Content Changes
4.3. Role of Water-Electrolyte Balance
4.4. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis—Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Böhm, A.; Heitmann, B.L. The use of bioelectrical impedance analysis for body composition in epidemiological studies. Eur. J. Clin. Nutr. 2013, 67, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Heydari, S.-T.; Ayatollahi, S.-M.-T.; Zare, N. Diagnostic Value of Bioelectrical Impedance Analysis versus Body Mass Index for Detection of Obesity among Students. Asian J. Sports Med. 2001, 2, 68–74. [Google Scholar] [CrossRef]
- Dehghan, M.; Merchant, A.T. Is bioelectrical impedance accurate for use in large epidemiological studies? Nutr. J. 2008, 7, 26. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.C.Y.; Powell, A.; Khow, K.S.F.; Visvanathan, R. The Performance of Five Bioelectrical Impedance Analysis Prediction Equations against Dual X-ray Absorptiometry in Estimating Appendicular Skeletal Muscle Mass in an Adult Australian Population. Nutrients 2016, 8, 189. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Manuel Gómez, J.; Lilienthal Heitmann, B.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis-part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef] [PubMed]
- Dixon, C.B.; Masteller, B.; Andreacci, J.L. The effect of a meal on measures of impedance and percent body fat estimated using contact-electrode bioelectrical impedance technology. Eur. J. Clin. Nutr. 2013, 67, 950–955. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, M.; Walker, K.Z.; O’Dea, K. The influence of a breakfast meal on the assessment of body composition using bioelectrical impedance. Eur. J. Clin. Nutr. 1998, 52, 94–97. [Google Scholar] [CrossRef]
- Slinde, F.; Rossander-Hulthén, L. Bioelectrical impedance: Effect of 3 identical meals on diurnal impedance variation and calculation of body composition. Am. J. Clin. Nutr. 2001, 74, 474–478. [Google Scholar] [CrossRef]
- González-Correa, C.H.; Caicedo-Eraso, J.C. Bioelectrical impedance analysis (BIA): A proposal for standardization of the classical method in adults. J. Phys. Conf. Ser. 2012, 407, 012018. [Google Scholar] [CrossRef]
- Gonzalez, C.H.; Evans, J.A.; Smye, S.W.; Holland, P. Variables affecting bioimpedance analysis measurements of body water. Med. Biol. Eng. Comput. 1999, 37, 106–107. [Google Scholar]
- Androutsos, O.; Gerasimidis, K.; Karanikolou, A.; Reilly, J.J.; Edwards, C.A. Impact of eating and drinking on body composition measurements by bioelectrical impedance. J. Hum. Nutr. Diet. 2015, 28, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Dixon, C.B.; Ramos, L.; Fitzgerald, E.; Reppert, D.; Andreacci, J.L. The effect of acute fluid consumption on measures of impedance and percent body fat estimated using segmental bioelectrical impedance analysis. Eur. J. Clin. Nutr. 2009, 63, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Dixon, C.B.; LoVallo, S.J.; Andreacci, J.L.; Goss, F.L. The effect of acute fluid consumption on measures of impedance and percent body fat using leg-to-leg bioelectrical impedance analysis. Eur. J. Clin. Nutr. 2006, 60, 142–146. [Google Scholar] [CrossRef]
- Luotonen, I. Effects of Carbohydrate Content on Body Composition during Weight Loss in Female Fitness Competitors. Available online: https://jyx.jyu.fi/dspace/handle/123456789/54388 (accessed on 26 October 2017).
- Nunes, C.L.; Matias, C.N.; Santos, D.A.; Morgado, J.P.; Monteiro, C.P.; Sousa, M.; Minderico, C.S.; Rocha, P.M.; St-Onge, M.P.; Sardinha, L.B.; et al. Characterization and Comparison of Nutritional Intake between Preparatory and Competitive Phase of Highly Trained Athletes. Medicina 2018, 54, 41. [Google Scholar] [CrossRef] [PubMed]
- Scalfi, L.; Bedogni, G.; Marra, M.; Di Biase, G.; Caldara, A.; Severi, S.; Contaldo, F.; Battistini, N. The prediction of total body water from bioelectrical impedance in patients with anorexia nervosa. Br. J. Nutr. 1997, 78, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Salinari, S.; Bertuzzi, A.; Mingrone, G.; Capristo, E.; Scarfone, A.; Greco, A.V.; Heymsfield, S.B. Bioimpedance analysis: A useful technique for assessing appendicular lean soft tissue mass and distribution. J. Appl. Physiol. 2003, 94, 1552–1556. [Google Scholar] [CrossRef] [PubMed]
- Gaarthuis, J.A.C.; Gerdes, S.M. The Effect of the Menstrual Cycle on the Body Composition of Weight-Stable Woman through BIA. Available online: Kennisbank.hva.nl/document/221478 (accessed on 26 October 2017).
- Bowen, D.J.; Grunberg, N.E. Variations in food preference and consumption across the menstrual cycle. Physiol. Behav. 1990, 47, 287–291. [Google Scholar] [CrossRef]
- Harrison, G.G.; Galal, O.M.; Ibrahim, N.; Khorshid, A.; Stormer, A.; Leslie, J.; Saleh, N.T. Underreporting of food intake by dietary recall is not universal: A comparison of data from Egyptian and American women. J. Nutr. 2000, 130, 2049–2054. [Google Scholar] [CrossRef]
- Baranauskas, M.; Stukas, R.; Tubelis, L.; Žagminas, K.; Šurkienė, G.; Švedas, E.; Giedraitis, V.R.; Dobrovolskij, V.; Abaravičius, J.A. Nutritional habits among high-performance endurance athletes. Medicine 2015, 51, 351–362. [Google Scholar] [CrossRef]
- Ortega, R.M.; Pérez-Rodrigo, C.; López-Sobaler, A.M. Dietary assessment methods: Dietary records. Nutr. Hosp. 2015, 26, 38–45. [Google Scholar]
- Szponar, L.; Wolnicka, K.; Rychlik, E. Atlas of Food Products and Dishes Portion Sizes; IŻŻ: Warsaw, Poland, 2012. (In Polish) [Google Scholar]
- Kunachowicz, H.; Nadolna, I.; Przygoda, B.; Iwanow, K. Food Composition Tables; PZWL Państwowy Zakład Wydawnictw Lekarskich (State Publishing House for Medicine): Warsaw, Poland, 2005. (In Polish) [Google Scholar]
- Głąbska, D.; Guzek, D.; Lech, G. Nutritional Status of Men with Ulcerative Colitis in Remission in a Pair–Matched Case–Control Study J. Clin. Med. 2018, 7, 438. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Correa-Bautista, J.E.; Martínez-Torres, J.; González-Ruíz, K.; González-Jiménez, E.; Schmidt-RioValle, J.; Garcia-Hermoso, A. Performance of Two Bioelectrical Impedance Analyses in the Diagnosis of Overweight and Obesity in Children and Adolescents: The FUPRECOL Study. Nutrients 2006, 8, 575. [Google Scholar] [CrossRef] [PubMed]
- Głąbska, D.; Guzek, D.; Sidor, P.; Włodarek, D. Vitamin D dietary intake questionnaire validation conducted among young Polish women. Nutrients 2016, 8, 36. [Google Scholar] [CrossRef] [PubMed]
- Głąbska, D.; Guzek, D.; Ślązak, J.; Włodarek, D. Assessing the Validity and Reproducibility of an Iron Dietary Intake Questionnaire Conducted in a Group of Young Polish Women. Nutrients 2017, 9, 199. [Google Scholar] [CrossRef] [PubMed]
- Myles, P.S.; Cui, J. Using the Bland-Altman method to measure agreement with repeated measures. Br. J. Anaesth. 2007, 99, 309–311. [Google Scholar] [CrossRef] [PubMed]
- Głąbska, D.; Uroić, V.; Guzek, D.; Pavić, E.; Bival, S.; Jaworska, K.; Giljević, Z.; Lange, E. The Possibility of Applying the Vitamin D Brief Food Frequency Questionnaire as a Tool for a Country with No Vitamin D Data in Food Composition Tables. Nutrients 2018, 10, 1278. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Khalil, S.F.; Mohktar, M.S.; Ibrahim, F. The Theory and Fundamentals of Bioimpedance Analysis in Clinical Status Monitoring and Diagnosis of Diseases. Sensors 2014, 14, 10895–10928. [Google Scholar] [CrossRef]
- World Health Organization; Food and Agriculture Organization of the United Nations. Carbohydrates in Human Nutrition; Report of a Joint FAO/WHO Expert Consultation; WHO: Rome, Italy, 1998. [Google Scholar]
- Wylie-Rosett, J.; Aebersold, K.; Conlon, B.; Isasi, C.R.; Ostrovsky, N.W. Health Effects of Low-Carbohydrate Diets: Where Should New Research Go? Curr. Diabetes Rep. 2013, 13, 271–278. [Google Scholar] [CrossRef]
- Bueno, N.B.; de Melo, I.S.; de Oliveira, S.L.; da Rocha Ataide, T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2013, 110, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Noto, H.; Goto, A.; Tsujimoto, T.; Noda, M. Low-Carbohydrate Diets and All-Cause Mortality: A Systematic Review and Meta-Analysis of Observational Studies. PLoS ONE 2013, 8, e55030. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, L.M.; Winkvist, A.; Johansson, I.; Lindahl, B.; Hallmans, G.; Lenner, P.; Guelpen, B.V. Low-carbohydrate, high-protein diet score and risk of incident cancer; a prospective cohort study. Nutr. J. 2013, 12, 58. [Google Scholar] [CrossRef] [PubMed]
- Saslow, L.R.; Kim, S.; Daubenmier, J.J.; Moskowitz, J.T.; Phinney, S.D.; Goldman, V.; Murphy, E.J.; Cox, R.M.; Moran, P.; Hecht, F.M. A Randomized Pilot Trial of a Moderate Carbohydrate Diet Compared to a Very Low Carbohydrate Diet in Overweight or Obese Individuals with Type 2 Diabetes Mellitus or Prediabetes. PLoS ONE 2014, 9, e91027. [Google Scholar] [CrossRef] [PubMed]
- Volek, J.S.; Westman, E.C. Very-low-carbohydrate weight-loss diets revisited. Clevel. Clin. J. Med. 2002, 69, 849, 853, 856–858. [Google Scholar] [CrossRef]
- Pogozelski, W.; Arpaia, N.; Priore, S. The metabolic effects of low-carbohydrate diets and incorporation into a biochemistry course. Biochem. Mol. Biol. Educ. 2005, 33, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Vist, G.E.; Maughan, R.J. The effect of osmolality and carbohydrate content on the rate of gastric emptying of liquids in man. J. Physiol. 1995, 486, 523–531. [Google Scholar] [CrossRef]
- Osterberg, K.L.; Pallardy, S.E.; Johnson, R.J.; Horswill, C.A. Carbohydrate exerts a mild influence on fluid retention following exercise-induced dehydration. J. Appl. Physiol. 2010, 108, 245–250. [Google Scholar] [CrossRef]
- Forgac, M.T. Carbohydrate loading—A review. J. Am. Diet. Assoc. 1979, 75, 42–55. [Google Scholar]
- Martinoli, R.; Mohamed, E.I.; Maiolo, C.; Cianci, R.; Denoth, F.; Salvadori, S.; Iacopino, L. Total body water estimation using bioelectrical impedance: A meta-analysis of the data available in the literature. Acta Diabetol. 2003, 40, 203. [Google Scholar] [CrossRef]
- Marken Lichtenbelt, W.D.; Fogelholm, M. Increased extracellular water compartment, relative to intracellular water compartment, after weight reduction. J. Appl. Physiol. 1999, 87, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Adam-Perrot, A.; Clifton, P.; Brouns, F. Low-carbohydrate diets: Nutritional and physiological aspects. Obes. Rev. 2006, 7, 49–58. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A.; Cooke, C.R.; Andres, R.; Faloona, G.R.; Davis, P.J. The effect of insulin on renal handling of sodium, potassium, calcium, and phosphate in man. J. Clin. Investig. 1975, 55, 845–855. [Google Scholar] [CrossRef]
- Landsberg, L.; Krieger, D.R. Obesity, metabolism, and the sympathetic nervous system. Am. J. Hypertens. 1989, 2, 125–132. [Google Scholar] [CrossRef]
- Rabast, U.; Vornberger, K.H.; Ehl, M. Loss of weight, sodium and water in obese persons consuming a high- or low-carbohydrate diet. Ann. Nutr. Metab. 1981, 25, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Manninen, A.H. Metabolic Effects of the Very-Low-Carbohydrate Diets: Misunderstood “Villains” of Human Metabolism. J. Int. Soc. Sports Nutr. 2004, 1, 7–11. [Google Scholar] [CrossRef]
- Weder, A.B. Membrane sodium transport and salt sensitivity of blood pressure. Hypertension 1991, 17, 74–80. [Google Scholar] [CrossRef]
- Leaf, A. Maintenance of concentration gradients and regulation of cell volume. Ann. N. Y. Acad. Sci. 1959, 72, 396–404. [Google Scholar] [CrossRef]
- Kurbel, S. Are extracellular osmolality and sodium concentration determined by Donnan effects of intracellular protein charges and of pumped sodium? J. Theor. Biol. 2008, 252, 769–772. [Google Scholar] [CrossRef]
- Baumgarten, C.M.; Feher, J.I. Osmosis and regulation of cell volume. In Cell Physiology Sourcebook: A Molecular Approach, 3rd ed.; Sperelakis, N., Ed.; Academic Press: San Diego, CA, USA, 2001; p. 339. [Google Scholar]
- Kimball, J.W. Biology; Wm. C. Brown Publishers: Dubuque, IA, USA, 1994. [Google Scholar]
- Shiose, K.; Yamada, Y.; Motonaga, K.; Sagayama, H.; Higaki, Y.; Tanaka, H.; Takahashi, H. Segmental extracellular and intracellular water distribution and muscle glycogen after 72-h carbohydrate loading using spectroscopic techniques. J. Appl. Physiol. 2016, 121, 205–211. [Google Scholar] [CrossRef]
- Bone, J.L.; Ross, M.L.; Tomcik, K.A.; Jeacocke, N.A.; Hopkins, W.G.; Burke, L.M. Manipulation of Muscle Creatine and Glycogen Changes Dual X-ray Absorptiometry Estimates of Body Composition. Med. Sci. Sports Exerc. 2017, 49, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Escobar, K.A.; Morales, J.; Vandusseldorp, T.A. The Effect of a Moderately Low and High Carbohydrate Intake on Crossfit Performance. Int. J. Exerc. Sci. 2016, 9, 460–470. [Google Scholar] [PubMed]
- Sawka, M.N.; Pandolf, K.B. Effects of body water loss on physiological function and exercise performance. In Perspectives in Exercise Science and Sports Medicine Fluid Homeostasis during Exercise; Gisolfi, C.V., Lamb, D.R., Eds.; Benchmark Press: Indianapolis, IN, USA, 1990; Volume 3, pp. 1–38. [Google Scholar]
- Barrero, A.; Erola, P.; Bescós, R. Energy Balance of Triathletes during an Ultra-Endurance Event. Nutrients 2015, 7, 209–222. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Analysis of Correlation | Analysis of Quartile Distribution (%) | Weighted κ Statistic | ||||
|---|---|---|---|---|---|---|
| p-Value | R | The Same Quartile | The Adjacent Quartiles | The Opposite Quartiles | ||
| Fat mass | <0.0001 * | 0.9379 | 81 | 18 | 0 | 0.840 |
| Fat-free mass | <0.0001 ** | 0.8648 | 72 | 25 | 1 | 0.744 |
| Body cell mass | <0.0001 * | 0.6413 | 55 | 38 | 2 | 0.568 |
| Muscle mass | <0.0001 ** | 0.8047 | 61 | 35 | 1 | 0.648 |
| Water content | <0.0001 * | 0.9367 | 81 | 18 | 0 | 0.840 |
| Extracellular water content | <0.0001 ** | 0.5954 | 50 | 38 | 4 | 0.472 |
| Intracellular water content | <0.0001 ** | 0.6394 | 49 | 41 | 3 | 0.488 |
| Carbohydrate Content <50% of Energy Value of Diet, n = 55 | Carbohydrate Content >50% of Energy Value of diet, n = 45 | p-Value ** | |
|---|---|---|---|
| Rz (Ω) | 669.0 ± 56.1 | 681.9 ± 63.8 | 0.3033 |
| Xc (Ω) | 73.0 * (20.0–93.0) | 76.0 (46.0–98.0) | 0.1400 |
| Fat mass (%) | 27.4 ± 5.0 | 27.4 ± 4.1 | 0.9632 |
| Fat-free mass (%) | 73.0 * (26.6–87.6) | 72.7 (63.5–81.6) | 0.8164 |
| Body cell mass (%) | 46.5 ± 4.6 | 46.6 ± 4.6 | 0.8924 |
| Muscle mass (%) | 42.3 ± 5.2 | 42.1 ± 4.5 | 0.8614 |
| Water content (%) | 53.2 ± 3.6 | 53.11 ± 3.0 | 0.9472 |
| Extracellular water content (%) | 46.0 (41.8–50.6) | 45.1 * (42.1–51.7) | 0.1766 |
| Intracellular water content (%) | 53.9 (49.4–58.2) | 54.8 * (48.3–57.9) | 0.0851 |
| Carbohydrate Content <50% of Energy Value of Diet, n = 55 | Carbohydrate Content >50% of Energy Value of Diet, n = 45 | p-Value ** | |
|---|---|---|---|
| Rz (Ω) | 665.5 * (588.0–860.0) | 674 (570.0–858.0) | 0.5051 |
| Xc (Ω) | 67.0 * (12.3–99.0) | 70.0 (53.0–90.7) | 0.1812 |
| Fat mass (%) | 27.4 ± 4.6 | 27.5 ± 4.4 | 0.9274 |
| Fat-free mass (%) | 72.8 * (24.9–86.9) | 72.3 (62.5–85.2) | 0.9862 |
| Body cell mass (%) | 44.4 ± 6.5 | 45.9 ± 5.3 | 0.2338 |
| Muscle mass (%) | 40.7 (27.3–60.4) | 40.8 * (31.5–67.2) | 0.9227 |
| Water content (%) | 53.1 ± 3.4 | 53.1 ± 3.2 | 0.9567 |
| Extracellular water content (%) | 47.1 * (40.3–64.2) | 46.4 (38.3–55.2) | 0.0638 |
| Intracellular water content (%) | 52.9 * (35.8–59.7) | 53.6 (44.8–61.7) | 0.0448 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Głąbska, D.; Cackowska, K.; Guzek, D. Comparison of the Body Composition of Caucasian Young Normal Body Mass Women, Measured in the Follicular Phase, Depending on the Carbohydrate Diet Level. Medicina 2018, 54, 104. https://doi.org/10.3390/medicina54060104
Głąbska D, Cackowska K, Guzek D. Comparison of the Body Composition of Caucasian Young Normal Body Mass Women, Measured in the Follicular Phase, Depending on the Carbohydrate Diet Level. Medicina. 2018; 54(6):104. https://doi.org/10.3390/medicina54060104
Chicago/Turabian StyleGłąbska, Dominika, Karolina Cackowska, and Dominika Guzek. 2018. "Comparison of the Body Composition of Caucasian Young Normal Body Mass Women, Measured in the Follicular Phase, Depending on the Carbohydrate Diet Level" Medicina 54, no. 6: 104. https://doi.org/10.3390/medicina54060104
APA StyleGłąbska, D., Cackowska, K., & Guzek, D. (2018). Comparison of the Body Composition of Caucasian Young Normal Body Mass Women, Measured in the Follicular Phase, Depending on the Carbohydrate Diet Level. Medicina, 54(6), 104. https://doi.org/10.3390/medicina54060104