Efficacy of Aortic Valve Replacement through Full Sternotomy and Minimal Invasion (Ministernotomy)

Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
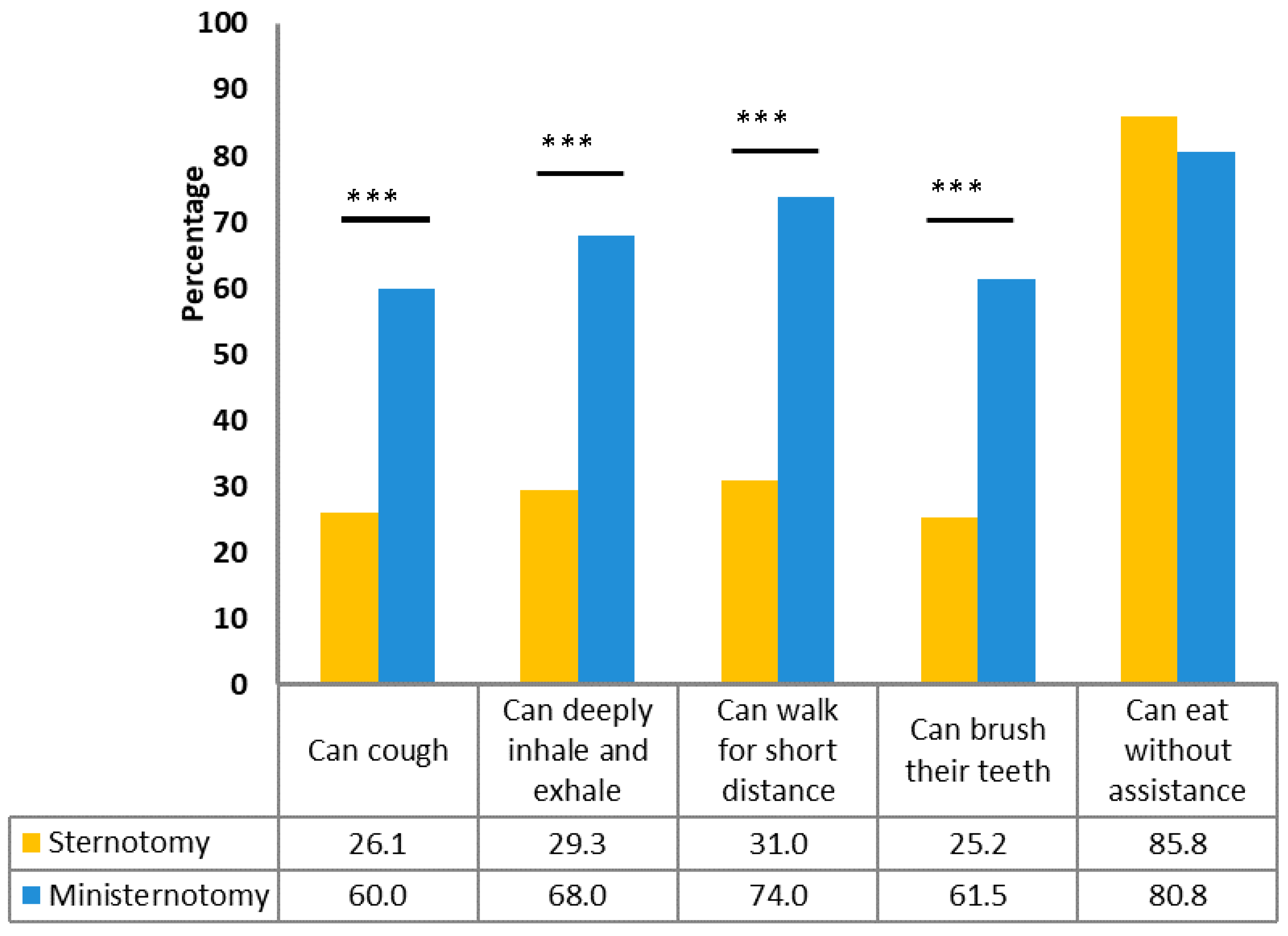
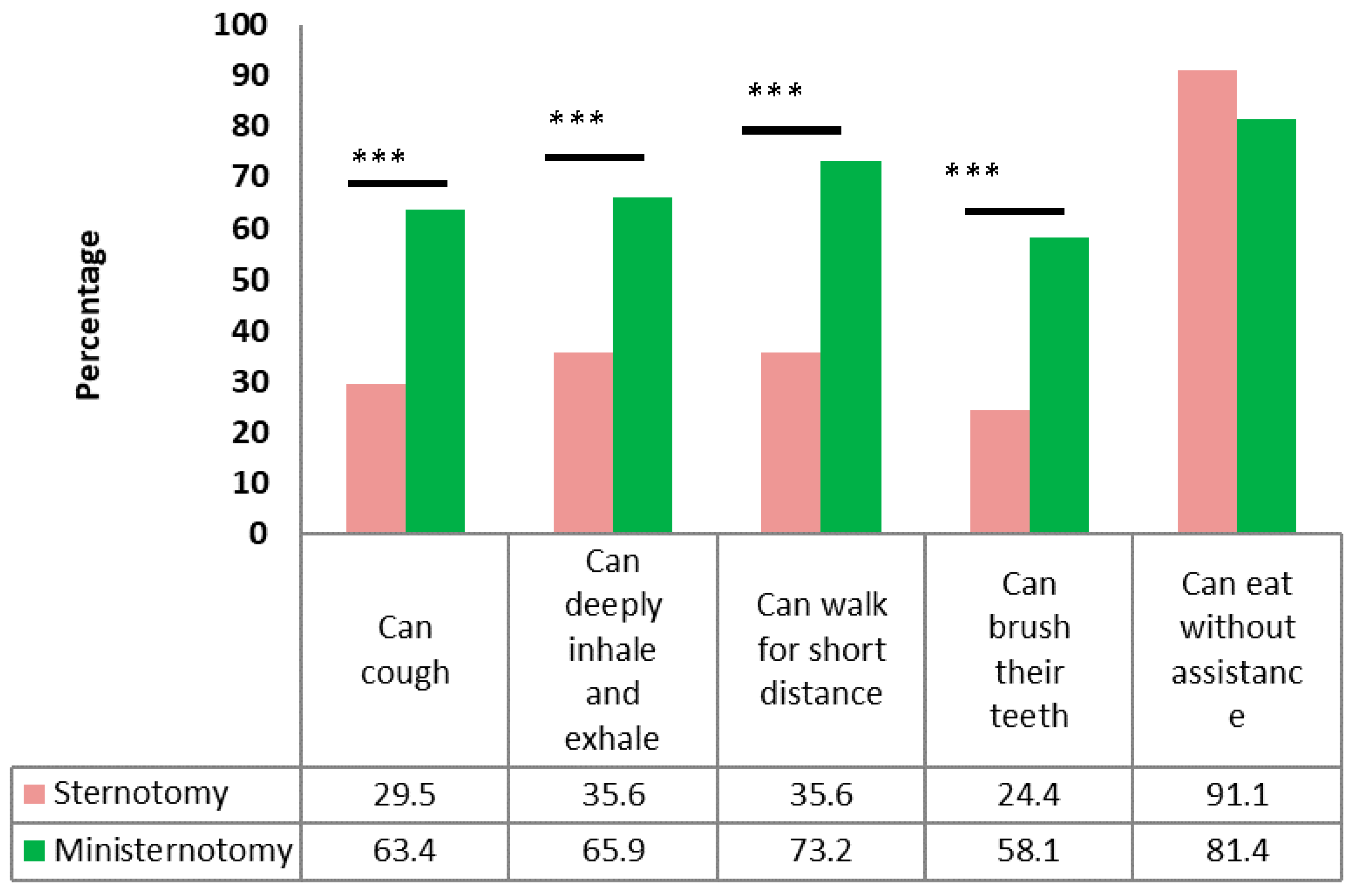
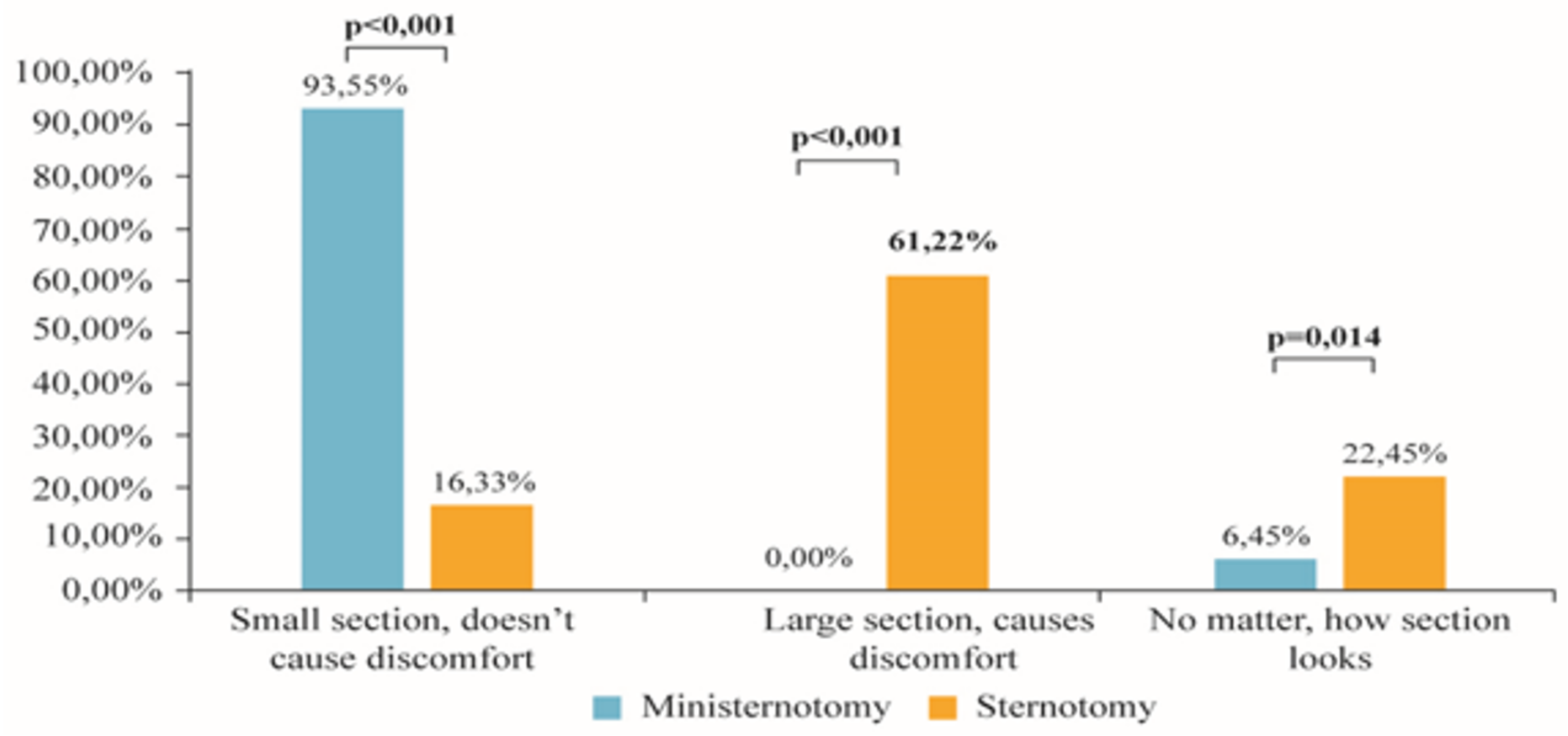
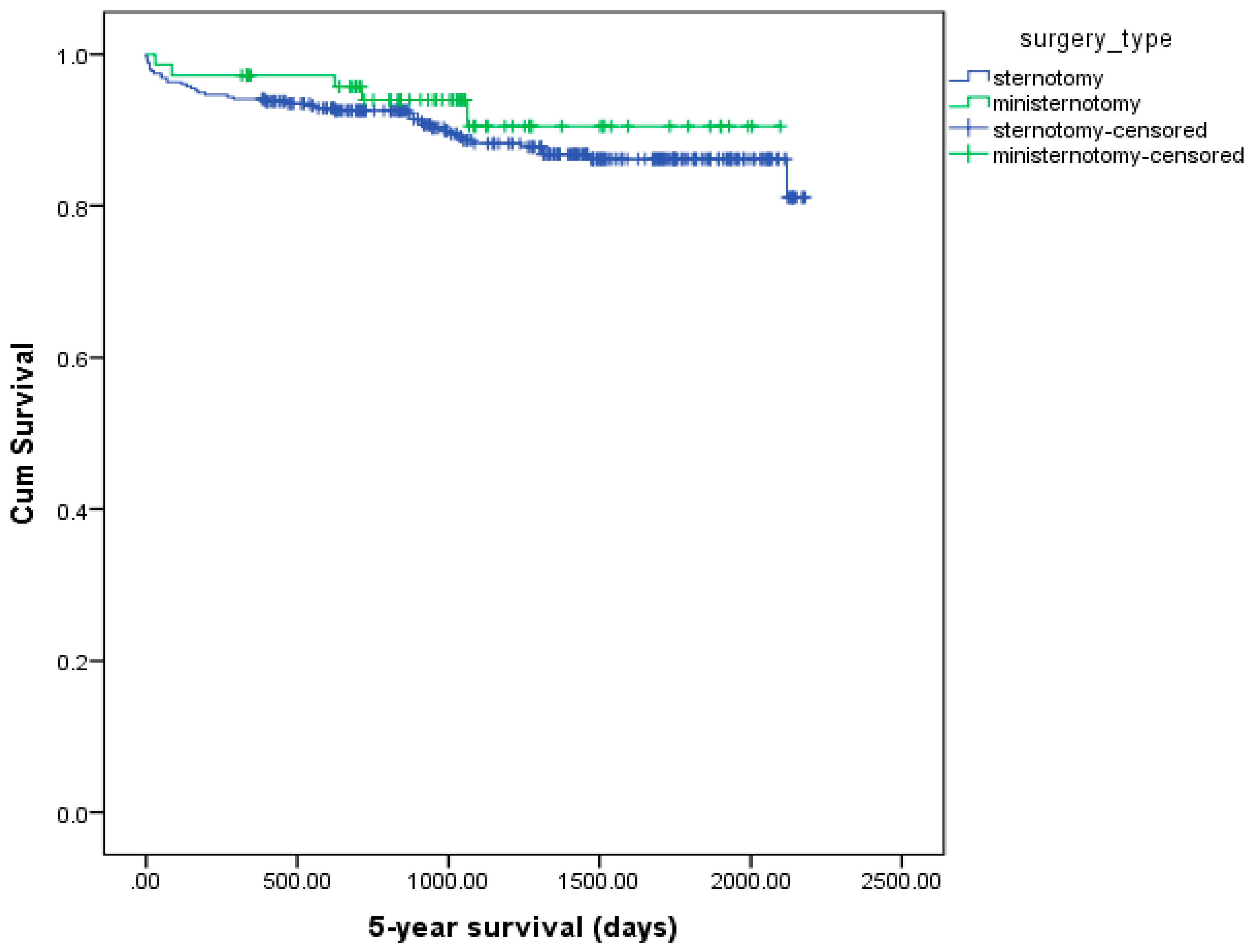
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ferreira, R.T.R.; Marchi, E. Aortic Valve Replacement: Treatment by Sternotomy versus Minimally Invasive Approach. Braz. J. Cardiovasc. Surg. 2016, 31, 422–427. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Foghsgaard, S.; Gazi, D.; Bach, K.; Hansen, H.; Schmidt, T.A.; Kjaergard, H.K. Minimally invasive aortic valve replacement reduces atelectasis in cardiac intensive care. Acute Card Care 2009, 11, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.L.; McKellar, S.H.; Sundt, T.M.; Schaff, H.V. Ministernotomy versus conventional sternotomy for aortic valve replacement: A systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2009, 137, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Skripochnik, E.; Michler, R.E.; Hentschel, V.; Neragi-Miandoab, S. The Efficacy and Outcome of Ministernotomy Compared to Those of Standard Sternotomy for Aortic Valve Replacement. ISRN Minim. Invasive Surg. 2014, 2014, 254084. [Google Scholar] [CrossRef]
- Raja, S.G.; Benedetto, U.; Amrani, M. Aortic valve replacement through J-shaped partial upper sternotomy. J. Thorac. Dis. 2013, 5, S662–S668. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarczyk, M.; Szałański, P.; Zembala, M.; Filipiak, K.; Karolak, W.; Wojarski, J.; Garbacz, M.; Kaczmarczyk, A.; Kwiecień, A.; Zembala, M. Minimally invasive aortic valve replacement–pros and cons of keyhole aortic surgery. Kardiochir. I Torakochir. Pol. 2015, 12, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Neely, R.C.; Boskovski, M.T.; Gosev, I.; Kaneko, T.; McGurk, S.; Leacche, M.; Cohn, L.H.; Division of Cardiac Surgery; The Brigham and Women’s Hospital; Harvard Medical School. Minimally invasive aortic valve replacement versus aortic valve replacement through full sternotomy: The Brigham and Women’s Hospital experience. Ann. Cardiothorac. Surg. 2015, 4, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Mahesh, B.; Navaratnarajah, M.; Mensah, K.; Ilsley, C.; Amrani, M. Mini-sternotomy aortic valve replacement: Is it safe and effective? Comparison with standard techniques. J. Heart Valve Dis. 2011, 20, 650–656. [Google Scholar] [PubMed]
- Glauber, M.; Ferrarini, M.; Miceli, A. Minimally invasive aortic valve surgery: State of the art and future directions. Ann. Cardiothorac. Surg. 2015, 4, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Gilmanov, D.; Solinas, M.; Farneti, P.A.; Cerillo, A.G.; Kallushi, E.; Santarelli, F.; Glauber, M.; Department of Adult Cardiac Surgery; Gabriele Monasterio Tuscany Foundation; Pasquinucci Heart hospital. Minimally invasive aortic valve replacement: 12-year single center experience. Ann. Cardiothorac. Surg. 2015, 4, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Shehada, S.E.; Öztürk, Ö.; Wottke, M.; Lange, R. Propensity score analysis of outcomes following minimal access versus conventional aortic valve replacement. Eur. J. Cardiothorac. Surg. 2016, 49, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Amr, M.A. Evaluation of feasibility and outcome of isolated aortic valve replacement surgery through j-shaped upper ministernotomy: A comparative study versus full sternotomy. J. Egypt. Soc. Cardiothorac. Surg. 2016, 24, 123–130. [Google Scholar] [CrossRef]
- Mikus, E.; Calvi, S.; Tripodi, A.; Lamarra, M.; Del Giglio, M. Upper ‘J’ ministernotomy versus full sternotomy: An easier approach for aortic valve reoperation. J. Heart Valve Dis. 2013, 22, 295–300. [Google Scholar] [PubMed]
- Lim, J.Y.; Deo, S.V.; Altarabsheh, S.E.; Jung, S.H.; Erwin, P.J.; Markowitz, A.H.; Park, S.J. Conventional versus minimally invasive aortic valve replacement: Pooled analysis of Propensity-Matched Data. J. Card Surg. 2015, 30, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Fudulu, D.; Lewis, H.; Benedetto, U.; Caputo, M.; Angelini, G.; Vohra, H.A. Minimally invasive aortic valve replacement in high risk patient groups. J. Thorac. Dis. 2017, 9, 1672–1696. [Google Scholar] [CrossRef] [PubMed]
- Sharony, R.; Grossi, E.A.; Saunders, P.C.; Schwartz, C.F.; Ribakove, G.H.; Culliford, A.T.; Ursomanno, P.; Baumann, F.G.; Galloway, A.C.; Colvin, S.B. Minimally invasive aortic valve surgery in the elderly: A case-control study. Circulation 2003, 8, II-43-7. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Byrne, J.G.; Adams, D.H.; Couper, G.S.; Rizzo, R.J.; Cohn, L.H.; Aranki, S.F. Minimally-invasive aortic root replacement. Heart Surg Forum 1999, 2, 326–329. [Google Scholar] [PubMed]
- Tabata, M.; Khalpey, Z.; Shekar, P.S.; Cohn, L.H. Reoperative minimal access aortic valve surgery: Minimal mediastinal dissection and minimal injury risk. J. Thorac. Cardiovasc. Surg. 2008, 136, 1564–1568. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Totaro, P.; Carlini, S.; Pozzi, M.; Pagani, F.; Zattera, G.; D’armini, A.M.; Vigano, M. Minimally invasive approach for complex cardiac surgery procedures. Ann. Thorac. Surg. 2009, 88, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Merk, D.R.; Lehmann, S.; Holzhey, D.M.; Dohmen, P.; Candolfi, P.; Misfeld, M.; Mohr, F.W.; Borger, M.A. Minimal invasive aortic valve replacement surgery is associated with improved survival: A propensity-matched comparison. Eur. J. Cardiothorac. Surg. 2015, 47, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, A.; Sjatskig, J.; van Boven, W.J.; Waanders, F.G.; Kelder, J.C.; Sonker, U.; Kloppenburg, G.T. J-shaped versus median sternotomy for aortic valve replacement with minimal extracorporeal circuit. Scand. Cardiovasc. J. 2011, 45, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Skripochnik, E.; Friedman, P.; Michler, R.E.; Neragi-Miandoab, S. The outcome of surgical management of type A aortic dissection. Asian Cardiovasc. Thorac. Ann. 2014, 22, 687–693. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicator | Overall Cohort | Propensity Score Matched Cohort | ||||
|---|---|---|---|---|---|---|
| Mini-Sternotomy n = 70 | Full Sternotomy n = 356 | p | Mini-Sternotomy n = 70 | Full Sternotomy n = 70 | p | |
| Age, mean ± SD, years | 60.8 ± 11.6 | 63.3 ± 13.2 | 0.155 | 60.8 ± 11.6 | 61.4 ± 11.9 | 0.155 |
| Male, n (%) | 42 (60.0) | 193 (54.2) | 0.384 | 42 (60) | 42 (60) | 1.000 |
| Height, mean ± SD, cm | 170.8 ± 10.0 | 169.3 ± 10.2 | 0.247 | 170.8 ± 10.0 | 170.1 ± 9.0 | 0.247 |
| Body weight, mean ± SD, kg | 82.3 ± 1.8 | 82.6 ± 1.8 | 0.886 | 82.3 ± 1.8 | 81.0 ± 1.6 | 0.886 |
| BMI, mean ± SD, kg/m2 | 27.7 ± 4.4 | 28.8 ± 5.6 | 0.656 | 27.7 ± 4.4 | 27.9 ± 4.5 | 0.536 |
| Diagnosis, n (%) | ||||||
| Aortic stenosis | 51 (72.9) | 267 (75.2) | 0.822 | 51 (72.9) | 45 (64.3) | 0.754 |
| Aortic regurgitation | 12 (17.1) | 50 (14.1) | 0.502 | 12 (17.1) | 13 (18.6) | 0.825 |
| Combined | 7 (10.0) | 38 (10.7) | 0.763 | 7 (10.0) | 12 (17.1) | 0.217 |
| Etiology of the disease, n (%) | ||||||
| Senile degeneration | 53 (75.71) | 283 (80.4) | 0.350 | 53 (75.71) | 53 (75.71) | 1.000 |
| Annular expansion | 13 (18.6) | 47(13.4) | 0.238 | 13 (18.6) | 12 (17.14) | 0.825 |
| Mitral valve | 1 (1.4) | 0 (0.0) | 0.024 | 1 (1.4) | 0 (0.0) | 0.316 |
| Infective endocarditis | 3 (4.3) | 22 (6.3) | 0.538 | 3 (4.3) | 5 (7.14) | 0.466 |
| EuroSCORE II | ||||||
| <1%, n (%) | 24 (34.3) | 99 (27.8) | 0.253 | 24 (34.3) | 20 (28.6) | 0.466 |
| 1–3%, n (%) | 44 (62.9) | 201 (56.5) | 0.344 | 44 (62.9) | 42 (60.0) | 0.728 |
| >3%, n (%) | 2 (2.9) | 56 (15.7) | 0.004 | 2 (2.9) | 8 (11.4) | 0.049 |
| NYHA functional class, n (%) | ||||||
| II | 12 (17.14) | 41 (11.5) | 0.192 | 12 (17.14) | 6 (8.6) | 0.130 |
| III | 57 (81.43) | 301 (84.6) | 0.514 | 57 (81.43) | 64 (91.4) | 0.084 |
| IV | 1 (1.4) | 14 (3.9) | 0.299 | 1 (1.4) | 0 (0.0) | 0.316 |
| Creatinine clearance (mL/min) | ||||||
| <50, n (%) | 41 (58.6) | 3 (0.8) | 0.144 | 41 (58.6) | 36 (51.4) | 0.396 |
| 50–85, n (%) | 27 (38.6) | 196 (55.4) | 0.075 | 27 (38.6) | 31 (44.3) | 0.493 |
| >85, n (%) | 2 (2.86) | 155 (43.8) | 0.098 | 2 (2.86) | 3 (4.3) | 0.649 |
| Diabetes mellitus, n (%) | 11 (15.7) | 5 (7.1) | 0.111 | 11 (15.7) | 5 (7.1) | 0.111 |
| COPD, n (%) | 4 (5.7) | 0 (0.0) | 0.042 | 4 (5.7) | 0 (0.0) | 0.042 |
| Hypertension, n (%) | 22 (31.4) | 57 (16.1) | 0.003 | 22 (31.4) | 10 (16.0) | 0.016 |
| Stroke, n (%) | 0 (0.0) | 16 (4.5) | 0.086 | 0 (0.0) | 2 (2.9) | 0.154 |
| Coronary artery disease, n (%) | 3 (4.3) | 12 (3.4) | 0.723 | 3 (4.3) | 1 (1.4) | 0.310 |
| Renal failure, n (%) | 2 (2.9) | 1 (1.4) | 0.5590.000 | 2 (2.9) | 1 (1.4) | 0.559 |
| Pacemaker, n (%) | 5 (7.1) | 16 (4.5) | 1.000 | 5 (7.1) | 2 (2.9) | 0.245 |
| LVEF %, n (%) | ||||||
| <30% | 0 (0.0) | 0 (0.0) | ND | 0 (0.0) | 0 (0.0) | ND |
| 30–49% | 16 (22.9) | 11 (15.7) | 0.580 | 16 (22.9) | 11 (15.7) | 0.284 |
| ≥50% | 54 (77.1) | 59 (84.3) | 0.826 | 54 (77.1) | 59 (84.3) | 0.284 |
| Indicator | Overall Cohort | Propensity Score Matched Cohort | ||||
|---|---|---|---|---|---|---|
| Full Sternotomy n = 356 | Mini-Sternotomy n = 70 | p | Full Sternotomy n = 70 | Mini-Sternotomy n = 70 | p | |
| Surgery duration, mean ± standard deviation (SD), min | 246.7 ± 74.2 | 263.5 ± 62.0 | 0.037 | 256.9 ± 79.7 | 263.5 ± 62.0 | 0.856 |
| Aortic cross-clamping time, mean ± SD, min | 79.9 ± 24.8 | 88.7 ± 20.7 | <0.001 | 80.3 ± 24.6 | 88.7 ± 20.7 | 0.007 |
| Cardiopulmonary bypass time, mean ± SD, min | 132.7 ± 44.5 | 144.0 ± 29.9 | 0.026 | 132.9 ± 44.9 | 144.0 ± 29.9 | 0.049 |
| Repeated cardioplegia, n (%) | 11 (3.1) | 0 (0.0) | 0.224 | 3(4.3) | 0 (0.0) | 0.080 |
| Valve type, n (%) | ||||||
| Biological | 163 (45.8) | 60 (85.7) | <0.001 | 24 (34.3) | 60 (85.7) | <0.001 |
| Mechanical | 193 (54.2) | 10 (14.3) | <0.001 | 46 (65.7) | 10 (14.3) | <0.001 |
| Size of aortic valve prosthesis, n (%) | ||||||
| 19 mm | 1 (0.3) | 0 (0.0) | 0.657 | 0 (0.0) | 0 (0.0) | ND |
| 21 mm | 57 (16.0) | 4 (5.6) | 0.025 | 7 (10.0) | 4 (5.7) | 0.346 |
| 23 mm | 154 (43.3) | 34 (47.2) | 0.549 | 36 (51.4) | 33 (47.1) | 0.612 |
| 25 mm | 111 (31.2) | 30 (41.7) | 0.095 | 19 (27.1) | 29 (41.4) | 0.075 |
| 27 mm | 31 (8.7) | 4 (5.6) | 0.404 | 8 (11.4) | 4 (5.7) | 0.227 |
| 29 mm | 2 (0.6) | 0 (0.0) | 0.530 | 0 (0.0) | 0 (0.0) | ND |
| Indicator | Overall Cohort | Propensity Score Matched Cohort | ||||
|---|---|---|---|---|---|---|
| Full Sternotomy n = 356 | Mini-Sternotomy n = 70 | p | Full Sternotomy n = 70 | Mini-Sternotomy n = 70 | p | |
| Ventilation time, mean ± SD, h | 11.7 ± 17.0 | 9.7 ± 1.7 | 0.213 | 11.7 ± 1.4 | 9.7 ± 1.7 | <0.001 |
| Blood loss ≥1000 mL/24 h, n (%) | 27 (7.6) | 1 (1.4) | 0.069 | 2 (2.9) | 1 (1.4) | 0.559 |
| 24-h chest tube drainage, mean± SD, mL | 411.9 ± 294.6 | 256.2 ± 28.6 | <0.001 | 407.6 ± 40.37 | 256.2 ± 28.6 | <0.001 |
| Coagulopathy correction, n (%) | 87 (24.4) | 0 (0.0) | <0.001 | 14 (20.0) | 0 (0.0) | <0.001 |
| Blood product transfusion, n (%) Packed red blood cells Platelet concentrates Fresh frozen plasma | 78 (21.9) 7 (2.0) 29 (8.1) | 12 (17.1) 4 (5.7) 1 (1.4) | 0.265 0.096 0.041 | 15 (21.4) 1 (1.4) 5 (7.1) | 12 (17.1) 4 (5.7) 1 (1.4) | 0.520 0.172 0.095 |
| ICU stay, mean ± SD, h | 83.8 ± 124.8 | 68.97 ± 6.3 | 0.305 | 88.41 ± 20.62 | 68.97 ± 6.3 | 0.319 |
| Hospital stay, mean ± SD, days | 21.9 ± 18.2 | 18.3 ± 1.9 | 0.109 | 21.9 ± 1.9 | 18.3 ± 1.9 | 0.012 |
| Hospital stay after surgery, mean ± SD, days | 17.6 ± 16.9 | 13.06 ± 1.0 | 0.025 | 15.2 ± 1.5 | 13.06 ± 1.0 | 0.113 |
| 30-day mortality, n (%) | 13 (3.7) | 1 (1.4) | 0.022 | 0(0.0) | 1 (1.4) | 0.316 |
| Resternotomy, n (%) | 21 (6) | 0 (0.0) | <0.001 | 2(2.9) | 1 (1.4) | 0.559 |
| Endocarditis, n (%) | 18 (5.1) | 1 (1.4) | 0.384 | 5(7.1) | 1 (1.4) | 0.095 |
| Wound infection, n (%) | 19 (5.3) | 2 (2.9) | 0.645 | 2(2.9) | 2 (2.9) | 1,000 |
| Cardiac tamponade, n (%) | 15 (4.2) | 1 (1.4) | 0.489 | 1(1.4) | 1 (1.4) | 1.000 |
| Acute renal failure, n (%) | 28 (7.9) | 2 (2.9) | 0.067 | 1(1.4) | 2 (2.9) | 0.559 |
| Other actions, n (%) ECMO IABP | 2 (0.6) 16 (4.5) | 1 (1.4) 0 (0.0) | 0.108 0.054 | 0 (0.0) 0 (0.0) | 1 (1.4) 0 (0.0) | 0.428 |
| Cardiac rhythm at discharge New atrial fibrillation, n (%) New pacemaker, n (%) | 18 (5.1) 12 (3.4) | 3 (4.3) 3 (4.3) | 0.071 0.902 | 3 (4.3) 4 (5.71) | 3 (4.3) 3 (4.3) | 1.000 0.698 |
| Number of patients treated with: Catecholamine, n (%) Morphine, n (%) | 21 (30.0) 350 (98.31) | 4 (5.71) 63 (90.0) | <0.001 0.042 | 21(30.0) 69 (98.57) | 4 (5.71) 63 (90.0) | <0.001 0.029 |
| Morphine dose, mean ± SD, mg | 18.56 ± 17.08 | 8.33 ± 3.58 | <0.001 | 18.56 ± 17.08 | 8.33 ± 3.58 | <0.001 |
| LVEF% at discharge, n (%) <30% 30%–49% ≥50% | 7 (2.1) 49 (14.7) 278 (83.2) | 0 (0.0) 12 (17.4) 57 (82.6) | 0.732 0.427 0.428 | 0 (0.0) 13 (18.6) 57 (81.4) | 0 (0.0) 12 (17.4) 57 (82.6) | ND 0.856 0.856 |
| Variables | Relative Risk (RR) | 95% CI | p Value |
|---|---|---|---|
| Preop hypertension (no vs. yes) | 1.717 | 0.320–9.209 | 0.528 |
| Preop LVEF (30–49% vs. >50%) | 0.156 | 0.031–0.774 | 0.023 |
| Aortotomy (transverse vs. J-shaped) | 0.761 | 0.124–4.668 | 0.768 |
| Type of cardioplegia | |||
| (coronary ostium vs. both) | 1.326 | 0.156–11.301 | 0.796 |
| (retrograde vs. both) | 0.140 | 0.006–3.494 | 0.231 |
| Aortic valve type (biological vs. mechanical) | 1.059 | 0.154–7.303 | 0.953 |
| Coagulopathy correction (no vs. yes) | 7.412 | 1.046–52.508 | 0.045 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aliahmed, H.M.A.; Karalius, R.; Valaika, A.; Grebelis, A.; Semėnienė, P.; Čypienė, R. Efficacy of Aortic Valve Replacement through Full Sternotomy and Minimal Invasion (Ministernotomy). Medicina 2018, 54, 26. https://doi.org/10.3390/medicina54020026
Aliahmed HMA, Karalius R, Valaika A, Grebelis A, Semėnienė P, Čypienė R. Efficacy of Aortic Valve Replacement through Full Sternotomy and Minimal Invasion (Ministernotomy). Medicina. 2018; 54(2):26. https://doi.org/10.3390/medicina54020026
Chicago/Turabian StyleAliahmed, Hammad M. A., Rimantas Karalius, Arūnas Valaika, Arimantas Grebelis, Palmyra Semėnienė, and Rasa Čypienė. 2018. "Efficacy of Aortic Valve Replacement through Full Sternotomy and Minimal Invasion (Ministernotomy)" Medicina 54, no. 2: 26. https://doi.org/10.3390/medicina54020026
APA StyleAliahmed, H. M. A., Karalius, R., Valaika, A., Grebelis, A., Semėnienė, P., & Čypienė, R. (2018). Efficacy of Aortic Valve Replacement through Full Sternotomy and Minimal Invasion (Ministernotomy). Medicina, 54(2), 26. https://doi.org/10.3390/medicina54020026