
Early Molecular Diagnosis and Comprehensive Treatment of Oral Cancer

 ,
, 
Abstract
1. Introduction
2. Molecular Basis of Oral Cancer
2.1. Genetic and Epigenetic Alterations
2.1.1. Clinical and Molecular Implications of TP53 Mutations in Oral Squamous Cell Carcinoma: Prognostic Significance, Therapeutic Resistance, and Immune Microenvironment Modulation
2.1.2. Implications of CDKN2A Alterations in Oral and Head and Neck Squamous Cell Carcinoma: Distinguishing Somatic Events from Hereditary Risk
2.1.3. EGFR Overexpression in Oral Cancer: Prognostic Significance, Genetic Variants, and Emerging Therapeutic Strategies
2.1.4. The Emerging Role of MicroRNAs as Diagnostic, Prognostic, and Therapeutic Biomarkers in Oral Squamous Cell Carcinoma
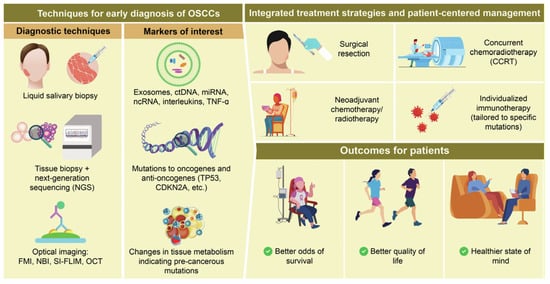
3. Early Molecular Diagnostic Approaches
3.1. Salivary and Blood-Based Extracellular Vesicles, Exosomal miRNAs, and Circulating Tumor DNA (ctDNA) as Emerging Non-Invasive Biomarkers for Early Detection, Prognosis, and Therapeutic Targeting in OSCC and HNSCC
3.2. Advances in Next-Generation Sequencing for Genetic Profiling, Diagnosis, and Prognosis in OSCC and HNSCC
3.3. Advancements in Optical Imaging for Early Detection, Surgical Guidance, and Diagnosis Optimization in HNSCC and OSCC
4. Integrative Treatment Strategies and Patient-Centered Management in Oral Squamous Cell Carcinoma
5. Discussion
6. Summary
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| OSCC | Oral Squamous Cell Carcinoma |
| GLOBOCAN | Global Cancer Observatory |
| HNSCC | Head and Neck Squamous Cell Carcinoma |
| OPMDs | Oral Potentially Malignant Disorders |
| EVs | Extracellular Vesicles |
| WMS | Whole Mouth Saliva |
| miRNAs | MicroRNAs |
| NGS | Next-Generation Sequencing |
| TP53 | Tumor Protein p53 |
| CDKN2A | Cyclin Dependent Kinase Inhibitor 2A |
| EGFR | Epidermal Growth Factor Receptor |
| PIK3CA | Phosphatidylinositol-4,5-Bisphosphate 3-Kinase Catalytic Subunit Alpha |
| NOTCH1 | Neurogenic locus notch homolog protein 1 |
| FFPE | Formalin-Fixed Paraffin-Embedded |
| SPTs | Second Primary Tumors |
| TME | Tumor Microenvironment |
| PD-L1 | Programmed Death-Ligand 1 |
| qRT-PCR | Quantitative Real-Time Polymerase Chain Reaction |
| FMI | Fluorescence Molecular Imaging |
| NBI | Narrow Band Imaging |
| OCT | Optical Coherence Tomography |
| SI-FLIM | Structured Illumination Fluorescence Lifetime Imaging Microscopy |
| FLIM | Fluorescence Lifetime Imaging Microscopy |
| US | Ultrasound |
| CM | Confocal Microscopy |
| CCRT | Concurrent Chemoradiotherapy |
| PORT | Postoperative Radiotherapy |
| AT | Adjuvant Therapy |
| CRT | Chemoradiotherapy |
| NACT | Neoadjuvant Chemotherapy |
| ICIs | Immune Checkpoint Inhibitors |
| OMCT | Oral Metronomic Chemotherapy |
| QOL | Quality of Life |
| TCGA | The Cancer Genome Atlas |
| AI | Artificial Intelligence |
| TIME | Tumor Immune Microenvironment |
| LVI | Lymphovascular Invasion |
| DHA | Dihydroartemisinin |
| EMT | Epithelial–Mesenchymal Transition |
| R/M HNSCC | Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma |
| OC | Oral Cancer |
| DEmiRs | Differentially Expressed miRNAs |
| DEGs | Differentially Expressed Genes |
| PPI | Protein–protein iInteraction |
| PNI | Perineural Invasion |
| ctDNA | Circulating Tumor DNA |
| cfRNA | Cell-Free RNA |
| PER1 | Directly Targeting Period 1 |
| PON2 | Paraoxonase-2 |
| PD-1 | Programmed Death-1 |
References
- Tranby, E.P.; Heaton, L.J.; Tomar, S.L.; Kelly, A.L.; Fager, G.L.; Backley, M.; Frantsve-Hawley, J. Oral Cancer Prevalence, Mortality, and Costs in Medicaid and Commercial Insurance Claims Data. Cancer Epidemiol. Biomark. Prev. 2022, 31, 1849–1857. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Xue, L.; Cheng, W.; Tang, J.; Ran, J.; Li, Y. Comprehensive survival analysis of oral squamous cell carcinoma patients undergoing initial radical surgery. BMC Oral. Health 2024, 24, 919. [Google Scholar] [CrossRef]
- Ravikumar, L.; Velmurugan, R. Innovations in early detection of oral cancer: Advancing diagnostic technologies and reducing global disparities. Oral. Oncol. Rep. 2024, 11, 100620. [Google Scholar] [CrossRef]
- Nagdeve, S.N.; Suganthan, B.; Ramasamy, R.P. Perspectives on the Application of Biosensors for the Early Detection of Oral Cancer. Sensors 2025, 25, 1459. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, M.; Khoushab, S.; Aghmiuni, M.H.; Anaraki, S.N.; Alimohammadi, M.; Taheriazam, A.; Farahani, N.; Entezari, M. Non-coding RNAs in oral cancer: Emerging biomarkers and therapeutic frontier. Heliyon 2024, 10, e40096. [Google Scholar] [CrossRef]
- Ravindran, S.; Ranganathan, S.; Karthikeyan, R.; Nandini, J.; Shanmugarathinam, A.; Kannan, S.K.; Prasad, K.D.; Marri, J.; Rajaganapathi, K. The role of molecular biomarkers in the diagnosis, prognosis, and treatment stratification of oral squamous cell carcinoma: A comprehensive review. J. Liq. Biopsy 2025, 7, 100285. [Google Scholar] [CrossRef]
- Pekarek, L.; Garrido-Gil, M.J.; Sanchez-Cendra, A.; Cassinello, J.; Pekarek, T.; Fraile-Martinez, O.; Garcia-Montero, C.; Lopez-Gonzalez, L.; Rios-Parra, A.; Alvarez-Mon, M.; et al. Emerging histological and serological biomarkers in oral squamous cell carcinoma: Applications in diagnosis, prognosis evaluation and personalized therapeutics (Review). Oncol. Rep. 2023, 50, 1–12. [Google Scholar] [CrossRef]
- Arabi, K.; Nazemi Salman, B.; Rahimzadeh-Bajgiran, F.; Moghbeli, M.; Moghadas, S.; Saburi, E. miRNAs in oral cancer; diagnostic and prognostic roles. Gene 2025, 951, 149382. [Google Scholar] [CrossRef]
- Park, Y.N.; Ryu, J.K.; Ju, Y. The Potential MicroRNA Diagnostic Biomarkers in Oral Squamous Cell Carcinoma of the Tongue. Curr. Issues Mol. Biol. 2024, 46, 6746–6756. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, Z.; Pu, J.J.; Zhong, J.; Khoo, U.S.; Su, Y.X.; Zhang, G. Proteogenomic characterisation of primary oral cancer unveils extracellular matrix remodelling and immunosuppressive microenvironment linked to lymph node metastasis. Clin. Transl. Med. 2025, 15, e70261. [Google Scholar] [CrossRef] [PubMed]
- Resurreccion, E.P.; Fong, K.W. The Integration of Metabolomics with Other Omics: Insights into Understanding Prostate Cancer. Metabolites 2022, 12, 488. [Google Scholar] [CrossRef]
- Kinane, D.F.; Gabert, J.; Xynopoulos, G.; Guzeldemir-Akcakanat, E. Strategic approaches in oral squamous cell carcinoma diagnostics using liquid biopsy. Periodontol 2000 2024, 96, 316–328. [Google Scholar] [CrossRef]
- Vinay, V.; Jodalli, P.; Chavan, M.S.; Buddhikot, C.S.; Luke, A.M.; Ingafou, M.S.H.; Reda, R.; Pawar, A.M.; Testarelli, L. Artificial Intelligence in Oral Cancer: A Comprehensive Scoping Review of Diagnostic and Prognostic Applications. Diagnostics 2025, 15, 280. [Google Scholar] [CrossRef]
- Prasad, M.; Sekar, R.; Priya, M.D.L.; Varma, S.R.; Karobari, M.I. A new perspective on diagnostic strategies concerning the potential of saliva-based miRNA signatures in oral cancer. Diagn. Pathol. 2024, 19, 147. [Google Scholar] [CrossRef] [PubMed]
- Balakittnen, J.; Ekanayake Weeramange, C.; Wallace, D.F.; Duijf, P.H.G.; Cristino, A.S.; Hartel, G.; Barrero, R.A.; Taheri, T.; Kenny, L.; Vasani, S.; et al. A novel saliva-based miRNA profile to diagnose and predict oral cancer. Int. J. Oral. Sci. 2024, 16, 14. [Google Scholar] [CrossRef]
- Patel, A.; Patel, S.; Patel, P.; Mandlik, D.; Patel, K.; Tanavde, V. Salivary Exosomal miRNA-1307-5p Predicts Disease Aggressiveness and Poor Prognosis in Oral Squamous Cell Carcinoma Patients. Int. J. Mol. Sci. 2022, 23, 10639. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Ping, F.; Fan, Z.; Zhang, C.; Deng, M.; Cheng, B.; Xia, J. Salivary exosomal miR-24-3p serves as a potential detective biomarker for oral squamous cell carcinoma screening. Biomed. Pharmacother. 2020, 121, 109553. [Google Scholar] [CrossRef]
- Bozyk, N.; Tang, K.D.; Zhang, X.; Batstone, M.; Kenny, L.; Vasani, S.; Punyadeera, C. Salivary exosomes as biomarkers for early diagnosis of oral squamous cell carcinoma. Oral. Oncol. Rep. 2023, 6, 100017. [Google Scholar] [CrossRef]
- Dongre, H.N.; Haave, H.; Fromreide, S.; Erland, F.A.; Moe, S.E.E.; Dhayalan, S.M.; Riis, R.K.; Sapkota, D.; Costea, D.E.; Aarstad, H.J.; et al. Targeted Next-Generation Sequencing of Cancer-Related Genes in a Norwegian Patient Cohort With Head and Neck Squamous Cell Carcinoma Reveals Novel Actionable Mutations and Correlations With Pathological Parameters. Front. Oncol. 2021, 11, 734134. [Google Scholar] [CrossRef]
- Liu, T.Y.; Lee, C.C.; Chen, Y.C.; Chang, Y.S.; Huang, H.Y.; Lee, Y.T.; Yen, J.C.; Chao, D.; Chang, J.G. Mutation Analysis of Second Primary Tumors in Oral Cancer in Taiwanese Patients through Next-Generation Sequencing. Diagnostics 2022, 12, 951. [Google Scholar] [CrossRef]
- Hinsdale, T.A.; Malik, B.H.; Cheng, S.; Benavides, O.R.; Giger, M.L.; Wright, J.M.; Patel, P.B.; Jo, J.A.; Maitland, K.C. Enhanced detection of oral dysplasia by structured illumination fluorescence lifetime imaging microscopy. Sci. Rep. 2021, 11, 4984. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Hayashi, Y.; Watanabe, K.; Yoshimi, R.; Hibi, H. Concurrent chemoradiotherapy with intravenous cisplatin and docetaxel for advanced oral cancer. Nagoya J. Med. Sci. 2019, 81, 407–414. [Google Scholar] [CrossRef]
- Vishwani, A.; Varghese, B.T.; Thomas, S.; Kumar, A.; Kaur, J.; Sharma, A. Neoadjuvant immunotherapy in advanced oral cancer: Emerging treatment paradigms. Oral. Oncol. Rep. 2024, 12, 100683. [Google Scholar] [CrossRef]
- Liu, X.H.; Wang, G.R.; Zhong, N.N.; Wang, W.Y.; Liu, B.; Li, Z.; Bu, L.L. Multi-omics in immunotherapy research for HNSCC: Present situation and future perspectives. NPJ Precis. Oncol. 2025, 9, 93. [Google Scholar] [CrossRef]
- Adorno-Farias, D.; Morales-Pison, S.; Gischkow-Rucatti, G.; Margarit, S.; Fernandez-Ramires, R. Genetic and epigenetic landscape of early-onset oral squamous cell carcinoma: Insights of genomic underserved and underrepresented populations. Genet. Mol. Biol. 2024, 47 (Suppl. S1), e20240036. [Google Scholar] [CrossRef]
- Jiang, X.; Ye, J.; Dong, Z.; Hu, S.; Xiao, M. Novel genetic alterations and their impact on target therapy response in head and neck squamous cell carcinoma. Cancer Manag. Res. 2019, 11, 1321–1336. [Google Scholar] [CrossRef]
- Zhou, G.; Liu, Z.; Myers, J.N. TP53 Mutations in Head and Neck Squamous Cell Carcinoma and Their Impact on Disease Progression and Treatment Response. J. Cell Biochem. 2016, 117, 2682–2692. [Google Scholar] [CrossRef] [PubMed]
- Raghavi, S.; Anbarasu, K. Unravelling the role of key genes in oral cancer progression: A comprehensive review. Oral. Oncol. Rep. 2024, 10, 100384. [Google Scholar] [CrossRef]
- Lakshmipriya, T.; Gopinath, S.C.B. Monitoring changes in the P53 gene mutation to diagnose oral cancer. Oral. Oncol. Rep. 2024, 10, 100513. [Google Scholar] [CrossRef]
- Hyodo, T.; Kuribayashi, N.; Fukumoto, C.; Komiyama, Y.; Shiraishi, R.; Kamimura, R.; Sawatani, Y.; Yaguchi, E.; Hasegawa, T.; Izumi, S.; et al. The mutational spectrum in whole exon of p53 in oral squamous cell carcinoma and its clinical implications. Sci. Rep. 2022, 12, 21695. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Xie, T.; Wang, B.; Wang, R.; Cai, Y.; Yuan, B.; Gleber-Netto, F.O.; Tian, X.; Rodriguez-Rosario, A.E.; Osman, A.A.; et al. Mutant p53 drives an immune cold tumor immune microenvironment in oral squamous cell carcinoma. Commun. Biol. 2022, 5, 757. [Google Scholar] [CrossRef] [PubMed]
- Giri, R.; Hota, S.K.; Senapati, U. Expression of TP53 in oral squamous cell carcinoma and its correlation with adverse histopathological features. J. Cancer Res. Ther. 2023, 19, 278–282. [Google Scholar] [CrossRef]
- Lin, T.Y.; Liu, K.Y.P.; Novack, R.; Mattu, P.S.; Ng, T.L.; Hoang, L.N.; Prisman, E.; Poh, C.F.; Ko, Y.C.K. Abnormal p53 Immunohistochemical Patterns Are Associated with Regional Lymph Node Metastasis in Oral Cavity Squamous Cell Carcinoma at Time of Surgery. Mod. Pathol. 2024, 37, 100614. [Google Scholar] [CrossRef]
- Jefferies, S.; Edwards, S.M.; Hamoudi, R.A.; A’Hern, R.; Foulkes, W.; Goldgar, D.; Eeles, R.; Collaborators, M.P.T. No germline mutations in CDKN2A (p16) in patients with squamous cell cancer of the head and neck and second primary tumours. Br. J. Cancer 2001, 85, 1383–1386. [Google Scholar] [CrossRef] [PubMed]
- Perez-Sayans, M.; Suarez-Penaranda, J.M.; Gayoso-Diz, P.; Barros-Angueira, F.; Gandara-Rey, J.M.; Garcia-Garcia, A. p16(INK4a)/CDKN2 expression and its relationship with oral squamous cell carcinoma is our current knowledge enough? Cancer Lett. 2011, 306, 134–141. [Google Scholar] [CrossRef]
- Jeong, A.R.; Forbes, K.; Orosco, R.K.; Cohen, E.E.W. Hereditary oral squamous cell carcinoma associated with CDKN2A germline mutation: A case report. J. Otolaryngol. Head. Neck Surg. 2022, 51, 5. [Google Scholar] [CrossRef]
- Shahnavaz, S.A.; Bradley, G.; Regezi, J.A.; Thakker, N.; Gao, L.; Hogg, D.; Jordan, R.C. Patterns of CDKN2A gene loss in sequential oral epithelial dysplasias and carcinomas. Cancer Res. 2001, 61, 2371–2375. [Google Scholar]
- Ribeiro, F.A.; Noguti, J.; Oshima, C.T.; Ribeiro, D.A. Effective targeting of the epidermal growth factor receptor (EGFR) for treating oral cancer: A promising approach. Anticancer. Res. 2014, 34, 1547–1552. [Google Scholar]
- Chen, I.H.; Chang, J.T.; Liao, C.T.; Wang, H.M.; Hsieh, L.L.; Cheng, A.J. Prognostic significance of EGFR and Her-2 in oral cavity cancer in betel quid prevalent area cancer prognosis. Br. J. Cancer 2003, 89, 681–686. [Google Scholar] [CrossRef]
- Civico-Ortega, J.L.; Gonzalez-Ruiz, I.; Ramos-Garcia, P.; Cruz-Granados, D.; Samayoa-Descamps, V.; Gonzalez-Moles, M.A. Prognostic and Clinicopathological Significance of Epidermal Growth Factor Receptor (EGFR) Expression in Oral Squamous Cell Carcinoma: Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2023, 24, 11888. [Google Scholar] [CrossRef] [PubMed]
- Laimer, K.; Spizzo, G.; Gastl, G.; Obrist, P.; Brunhuber, T.; Fong, D.; Barbieri, V.; Jank, S.; Doppler, W.; Rasse, M.; et al. High EGFR expression predicts poor prognosis in patients with squamous cell carcinoma of the oral cavity and oropharynx: A TMA-based immunohistochemical analysis. Oral. Oncol. 2007, 43, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.F.; Chien, H.T.; Chuang, W.Y.; Lai, C.H.; Cheng, S.D.; Liao, C.T.; Wang, H.M. Epidermal growth factor receptor intron-1 CA repeat polymorphism on protein expression and clinical outcome in Taiwanese oral squamous cell carcinoma. Sci. Rep. 2017, 7, 4963. [Google Scholar] [CrossRef] [PubMed]
- Rehmani, H.S.; Issaeva, N. EGFR in head and neck squamous cell carcinoma: Exploring possibilities of novel drug combinations. Ann. Transl. Med. 2020, 8, 813. [Google Scholar] [CrossRef]
- Wang, J.; Lv, N.; Lu, X.; Yuan, R.; Chen, Z.; Yu, J. Diagnostic and therapeutic role of microRNAs in oral cancer (Review). Oncol. Rep. 2021, 45, 58–64. [Google Scholar] [CrossRef]
- Ghafouri-Fard, S.; Gholipour, M.; Taheri, M.; Shirvani Farsani, Z. MicroRNA profile in the squamous cell carcinoma: Prognostic and diagnostic roles. Heliyon 2020, 6, e05436. [Google Scholar] [CrossRef]
- Rajan, C.; Roshan, V.G.D.; Khan, I.; Manasa, V.G.; Himal, I.; Kattoor, J.; Thomas, S.; Kondaiah, P.; Kannan, S. MiRNA expression profiling and emergence of new prognostic signature for oral squamous cell carcinoma. Sci. Rep. 2021, 11, 7298. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, S.; Wang, S.; Cao, T.; Fan, H. Decoding oral cancer: Insights from miRNA expression profiles and their regulatory targets. Front. Mol. Biosci. 2024, 11, 1521839. [Google Scholar] [CrossRef]
- Dioguardi, M.; Spirito, F.; Iacovelli, G.; Sovereto, D.; Laneve, E.; Laino, L.; Caloro, G.A.; Nabi, A.Q.; Ballini, A.; Lo Muzio, L.; et al. The Potential microRNA Prognostic Signature in HNSCCs: A Systematic Review. Noncoding RNA 2023, 9, 54. [Google Scholar] [CrossRef]
- Jakob, M.; Mattes, L.M.; Kuffer, S.; Unger, K.; Hess, J.; Bertlich, M.; Haubner, F.; Ihler, F.; Canis, M.; Weiss, B.G.; et al. MicroRNA expression patterns in oral squamous cell carcinoma: Hsa-mir-99b-3p and hsa-mir-100-5p as novel prognostic markers for oral cancer. Head. Neck 2019, 41, 3499–3515. [Google Scholar] [CrossRef]
- Lu, Z.; He, Q.; Liang, J.; Li, W.; Su, Q.; Chen, Z.; Wan, Q.; Zhou, X.; Cao, L.; Sun, J.; et al. miR-31-5p Is a Potential Circulating Biomarker and Therapeutic Target for Oral Cancer. Mol. Ther. Nucleic Acids 2019, 16, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.H.; Tu, H.F.; Wu, C.H.; Yang, C.C.; Chang, K.W. MicroRNA-21 promotes perineural invasion and impacts survival in patients with oral carcinoma. J. Chin. Med. Assoc. 2017, 80, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Burtyn, O.; Borikun, T.; Rossylna, O.; Kopchak, A.; Kravets, O. Clinical Significance of Salivary Mir-21, -155, and -375 in Patients with Squamous Cell Carcinoma of Oral Cavity. Exp. Oncol. 2024, 46, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Patel, S.; Patel, P.; Mandlik, D.; Patel, K.; Tanavde, V. Salivary exosomal miR-1307-5p predicts disease aggressiveness and poor prognosis in oral squamous cell carcinoma patients. bioRxiv 2022. [Google Scholar] [CrossRef]
- Yang, R.; Li, T.; Zhang, S.; Shui, C.; Ma, H.; Li, C. The effect of circulating tumor DNA on the prognosis of patients with head and neck squamous cell carcinoma: A systematic review and meta-analysis. BMC Cancer 2024, 24, 1434. [Google Scholar] [CrossRef]
- Xu, Q.; Li, X. Tumor-derived extracellular vesicles in the immune microenvironment of head and neck squamous cell carcinoma: Foe or future? J. Stomatol. Oral. Maxillofac. Surg. 2024, 125, 101738. [Google Scholar] [CrossRef]
- Cristaldi, M.; Mauceri, R.; Di Fede, O.; Giuliana, G.; Campisi, G.; Panzarella, V. Salivary Biomarkers for Oral Squamous Cell Carcinoma Diagnosis and Follow-Up: Current Status and Perspectives. Front. Physiol. 2019, 10, 1476. [Google Scholar] [CrossRef]
- AlAli, A.M.; Walsh, T.; Maranzano, M. CYFRA 21-1 and MMP-9 as salivary biomarkers for the detection of oral squamous cell carcinoma: A systematic review of diagnostic test accuracy. Int. J. Oral. Maxillofac. Surg. 2020, 49, 973–983. [Google Scholar] [CrossRef]
- Vats, R.; Yadav, P.; Bano, A.; Wadhwa, S.; Bhardwaj, R. Salivary biomarkers in non-invasive oral cancer diagnostics: A comprehensive review. J. Appl. Oral. Sci. 2024, 32, e20240151. [Google Scholar]
- Bastias, D.; Maturana, A.; Marin, C.; Martinez, R.; Niklander, S.E. Salivary Biomarkers for Oral Cancer Detection: An Exploratory Systematic Review. Int. J. Mol. Sci. 2024, 25, 2634. [Google Scholar] [CrossRef]
- Senevirathna, K.; Mahakapuge, T.A.N.; Jayawardana, N.U.; Rajapakse, J.; Gamage, C.U.; Seneviratne, B.; Perera, U.; Kanmodi, K.K.; Jayasinghe, R.D. Diagnostic potential of salivary IL-1beta, IL-8, SAT, S100P, and OAZ1 in oral squamous cell carcinoma, oral submucous fibrosis, and oral lichen planus based on findings from a Sri Lankan cohort. Sci. Rep. 2024, 14, 27226. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Xu, M.; Liu, M.; Peng, H. Comparison of saliva and blood derived cell free RNAs for detecting oral squamous cell carcinoma. Sci. Rep. 2025, 15, 4645. [Google Scholar] [CrossRef] [PubMed]
- Ghiyasimoghaddam, N.; Shayan, N.; Mirkatuli, H.A.; Baghbani, M.; Ameli, N.; Ashari, Z.; Mohtasham, N. Does circulating tumor DNA apply as a reliable biomarker for the diagnosis and prognosis of head and neck squamous cell carcinoma? Discov. Oncol. 2024, 15, 427. [Google Scholar] [CrossRef]
- Sanesi, L.; Mori, G.; Troiano, G.; Ballini, A.; Valzano, F.; Dioguardi, M.; Muzio, L.L.; Magalhaes, M.; Caponio, V.C.A. Salivary exosomal microRNA profile as biomonitoring tool for diagnosis and prognosis of patients with head and neck squamous cell carcinoma: A systematic review. Arch. Oral. Biol. 2024, 165, 106012. [Google Scholar] [CrossRef] [PubMed]
- Maheswari, T.N.U.; Venugopal, A.; Sureshbabu, N.M.; Ramani, P. Salivary micro RNA as a potential biomarker in oral potentially malignant disorders: A systematic review. Tzu Chi Med. J. 2018, 30, 55–60. [Google Scholar] [CrossRef]
- Gai, C.; Camussi, F.; Broccoletti, R.; Gambino, A.; Cabras, M.; Molinaro, L.; Carossa, S.; Camussi, G.; Arduino, P.G. Salivary extracellular vesicle-associated miRNAs as potential biomarkers in oral squamous cell carcinoma. BMC Cancer 2018, 18, 439. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, J.; Liu, S.; Yu, L.; Liu, S.; Li, M.; Jin, F. Extracellular vesicles in oral squamous cell carcinoma: Current progress and future prospect. Front. Bioeng. Biotechnol. 2023, 11, 1149662. [Google Scholar] [CrossRef]
- Wang, Q.; Sun, J.; Jiang, H.; Yu, M. Emerging roles of extracellular vesicles in oral and maxillofacial areas. Int. J. Oral. Sci. 2025, 17, 11. [Google Scholar] [CrossRef]
- Li, R.; Zhou, Y.; Zhang, M.; Xie, R.; Duan, N.; Liu, H.; Qin, Y.; Ma, J.; Li, Z.; Ye, P.; et al. Oral squamous cell carcinoma-derived EVs promote tumor progression by regulating inflammatory cytokines and the IL-17A-induced signaling pathway. Int. Immunopharmacol. 2023, 118, 110094. [Google Scholar] [CrossRef]
- Sasahira, T.; Kurihara-Shimomura, M.; Shimojjukoku, Y.; Shima, K.; Kirita, T. Searching for New Molecular Targets for Oral Squamous Cell Carcinoma with a View to Clinical Implementation of Precision Medicine. J. Pers. Med. 2022, 12, 413. [Google Scholar] [CrossRef]
- Kim, S.; Lee, J.W.; Park, Y.S. The Application of Next-Generation Sequencing to Define Factors Related to Oral Cancer and Discover Novel Biomarkers. Life 2020, 10, 228. [Google Scholar] [CrossRef] [PubMed]
- van Schaik, J.E.; Halmos, G.B.; Witjes, M.J.H.; Plaat, B.E.C. An overview of the current clinical status of optical imaging in head and neck cancer with a focus on Narrow Band imaging and fluorescence optical imaging. Oral. Oncol. 2021, 121, 105504. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, Z.; Zhang, C.; Shao, C.; Duan, Y.; Zheng, G.; Cai, Y.; Ge, M.; Xu, J. Recent advances of photodiagnosis and treatment for head and neck squamous cell carcinoma. Neoplasia 2025, 60, 101118. [Google Scholar] [CrossRef] [PubMed]
- de Wit, J.G.; van Schaik, J.E.; Voskuil, F.J.; Vonk, J.; de Visscher, S.; Schepman, K.P.; van der Laan, B.; Doff, J.J.; van der Vegt, B.; Plaat, B.E.C.; et al. Comparison of narrow band and fluorescence molecular imaging to improve intraoperative tumour margin assessment in oral cancer surgery. Oral. Oncol. 2022, 134, 106099. [Google Scholar] [CrossRef]
- Romano, A.; Di Stasio, D.; Petruzzi, M.; Fiori, F.; Lajolo, C.; Santarelli, A.; Lucchese, A.; Serpico, R.; Contaldo, M. Noninvasive Imaging Methods to Improve the Diagnosis of Oral Carcinoma and Its Precursors: State of the Art and Proposal of a Three-Step Diagnostic Process. Cancers 2021, 13, 2864. [Google Scholar] [CrossRef]
- Jang, J.Y.; Choi, N.; Jeong, H.S. Surgical Extent for Oral Cancer: Emphasis on a Cut-Off Value for the Resection Margin Status: A Narrative Literature Review. Cancers 2022, 14, 5702. [Google Scholar] [CrossRef]
- Chang, C.C.; Wu, Y.T.; Lu, H.H.; Cheng, Y.J.; Tsai, M.H. The role of postoperative radiotherapy or chemoradiation in pT1-2N1M0 oral squamous cell carcinoma. J. Formos. Med. Assoc. 2025, 124, 67–72. [Google Scholar] [CrossRef]
- Mrosk, F.; Doll, C.; Scheer, J.; Neumann, F.; Hofmann, E.; Kreutzer, K.; Voss, J.; Rubarth, K.; Beck, M.; Heiland, M.; et al. Oncologic Outcome in Advanced Oral Squamous Cell Carcinoma After Refusal of Recommended Adjuvant Therapy. JAMA Otolaryngol. Head. Neck Surg. 2023, 149, 1027–1033. [Google Scholar] [CrossRef]
- Dhawan, A. Adjunctive Therapy in Oral Cancer. In Oral and Maxillofacial Surgery for the Clinician; Bonanthaya, K., Panneerselvam, E., Manuel, S., Kumar, V.V., Rai, A., Eds.; Springer Nature: Singapore, 2021; pp. 1903–1913. [Google Scholar]
- Geiger, J.L.; Adelstein, D.J. Chemotherapy in the definitive management of oral cancers: Where do we stand today? Oral. Oncol. 2020, 102, 104584. [Google Scholar] [CrossRef]
- Malik, A.; Vishnoi, K.; Noronha, V.; Prabhash, K. A nuanced review of neoadjuvant therapies in oral cancer. Expert. Rev. Anticancer. Ther. 2025, 25, 1–17. [Google Scholar] [CrossRef]
- Kende, P.; Mathur, Y.; Varte, V.; Tayal, S.; Patyal, N.; Landge, J. The efficacy of neoadjuvant chemotherapy as compared to upfront surgery for the management of oral squamous cell carcinoma: A systematic review and meta-analysis. Int. J. Oral. Maxillofac. Surg. 2024, 53, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Rajendra, A.; Noronha, V.; Joshi, A.; Patil, V.M.; Menon, N.; Prabhash, K. Palliative chemotherapy in head and neck cancer: Balancing between beneficial and adverse effects. Expert. Rev. Anticancer. Ther. 2020, 20, 17–29. [Google Scholar] [CrossRef]
- Kumar, N.A.N.; Dikhit, P.S.; Jose, A.; Mehta, V.; Pai, A.; Kudva, A.; Rao, M. Oral Metronomic Chemotherapy in Advanced and Metastatic Oral Squamous Cell Carcinoma: A Need of the Hour. J. Maxillofac. Oral. Surg. 2024, 23, 793–800. [Google Scholar] [CrossRef]
- Bhutani, R.; Singh, R.; Mishra, A.; Baluni, P. The adverse impact of chemo-radiotherapy on the quality of life of oral cancer patients: A review. Oral. Oncol. Rep. 2024, 10, 100544. [Google Scholar] [CrossRef]
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral. Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Lingen, M.W.; Kalmar, J.R.; Karrison, T.; Speight, P.M. Critical evaluation of diagnostic aids for the detection of oral cancer. Oral. Oncol. 2008, 44, 10–22. [Google Scholar] [CrossRef]
- Leemans, C.R.; Snijders, P.J.F.; Brakenhoff, R.H. The molecular landscape of head and neck cancer. Nat. Rev. Cancer 2018, 18, 269–282. [Google Scholar] [CrossRef]
- Melo-Alvim, C.; Neves, M.E.; Santos, J.L.; Abrunhosa-Branquinho, A.N.; Barroso, T.; Costa, L.; Ribeiro, L. Radiotherapy, Chemotherapy and Immunotherapy-Current Practice and Future Perspectives for Recurrent/Metastatic Oral Cavity Squamous Cell Carcinoma. Diagnostics 2022, 13, 99. [Google Scholar] [CrossRef]
- Menditti, D.; Santagata, M.; Imola, G.; Staglianò, S.; Vitagliano, R.; Boschetti, C.E.; Inchingolo, A.M. Personalized Medicine in Oral Oncology: Imaging Methods and Biological Markers to Support Diagnosis of Oral Squamous Cell Carcinoma (OSCC): A Narrative Literature Review. J. Pers. Med. 2023, 13, 1397. [Google Scholar] [CrossRef]
- Muralidharan, S.; Nikalje, M.; Subramaniam, T.; Koshy, J.A.; Koshy, A.V.; Bangera, D. A Narrative Review on Oral Squamous Cell Carcinoma. J. Pharm. Bioallied Sci. 2025, 17, S204–S206. [Google Scholar] [CrossRef]
- Campagna, R.; Pozzi, V.; Salvucci, A.; Togni, L.; Mascitti, M.; Sartini, D.; Salvolini, E.; Santarelli, A.; Lo Muzio, L.; Emanuelli, M. Paraoxonase-2 expression in oral squamous cell carcinoma. Hum. Cell 2023, 36, 1211–1213. [Google Scholar] [CrossRef] [PubMed]
- Parween, F.; Gupta, R.D. Insights into the role of paraoxonase 2 in human pathophysiology. J. Biosci. 2021, 46, 4. [Google Scholar] [CrossRef]
- Kamal, M.V.; Prabhu, K.; Sharan, K.; Pai, A.; Chakrabarty, S.; Damerla, R.R.; Shetty, P.S.; Belle, V.S.; Rao, M.; Kumar, N.A.N. Investigation of the Molecular Mechanisms of Paraoxonase-2 Mediated Radiotherapy and Chemotherapy Resistance in Oral Squamous Cell Carcinoma. Clin. Transl. Sci. 2025, 18, e70201. [Google Scholar] [CrossRef] [PubMed]
- Ashwini, R.; Narayan, M.; Rajkumar, K. Diagnostic and prognostic markers of oral squamous cell carcinoma- a detailed review. Oral. Oncol. Rep. 2024, 10, 100321. [Google Scholar] [CrossRef]
- Mahajan, A.; Mohanty, S.; Ghosh, S.; Urs, A.B.; Khurana, N.; Gupta, S. Sarcomatoid Carcinoma of the Oral Cavity: A Diagnostic Dilemma. Case Rep. Dent. 2017, 2017, 7495695. [Google Scholar] [CrossRef]
- Harnischfeger, N.; Szabo, L.; Kretzschmar, K. Establishment and Characterization of Patient-Derived Oral Cancer Organoids; Methods in Molecular Biology; Springer Nature: Berlin/Heidelberg, Germany, 2025. [Google Scholar] [CrossRef]
- Adeola, H.A.; Bello, I.O.; Aruleba, R.T.; Francisco, N.M.; Adekiya, T.A.; Adefuye, A.O.; Ikwegbue, P.C.; Musaigwa, F. The Practicality of the Use of Liquid Biopsy in Early Diagnosis and Treatment Monitoring of Oral Cancer in Resource-Limited Settings. Cancers 2022, 14, 1139. [Google Scholar] [CrossRef]

{kind=link}
| Key Findings | Clinical Implications | References |
|---|---|---|
| TP53 mutations lead to treatment resistance and poor survival | May guide personalized treatment and prognosis | [28,29,30,31,32,33,34] |
| Immune evasion via cold tumor microenvironment (TME) | Poor ICI response | [32] |
| Associated with lymphovascular invasion and positive surgical margins | Biomarker for risk stratification | [33] |
| Key Findings | Clinical Implications | References |
|---|---|---|
| Germline mutations rare in sporadic cases | Routine testing not recommended broadly | [35] |
| Germline variants in young or familial cases | May justify targeted surveillance | [37] |
| Deletion of exon 1α linked to OSCC | Early genetic marker for progression | [38] |
| Key Findings | Clinical Implications | References |
|---|---|---|
| Overexpression correlates with nodal spread and poor survival | Prognostic marker | [39,40,41,42] |
| EGFR CA repeat polymorphism (SS genotype) increases risk | Risk stratification in specific populations | [43] |
| Limited efficacy of current EGFR-targeted therapies | Need for novel drug combinations | [44] |
| miRNAs | Expression Pattern | Clinical Application | References |
|---|---|---|---|
| miR-31 | Strong predictor of recurrence | Prognostic signature | [15,16] |
| miR-21 | Prognostic markers in European cohort | Patient stratification | [16,47,48] |
| miR-125a-5p | Associated with tumor size and nodal status | Prognostic and predictive biomarkers | [48] |
| miR-145 | Linked to chemoresistance and poor prognosis | Salivary exosomal biomarker | [48] |
| miR-223 | Upregulated | Involved in cell cycle regulation | [48] |
| miR-155 | Upregulated | Immune regulation; involved in tumor progression; reported in multiple studies | [48,53] |
| miR-196a, miR-1237 | Upregulated | Strong predictor of recurrence; prognostic signature | [47] |
| miR-1444, miR-204 | Downregulated | Strong predictor of recurrence; prognostic signature | [47] |
| miR-99b-3p, miR-100-5p | — (not specified) | Patient stratification in European cohort | [50] |
| miR-375 | Upregulated | Correlated with tumor size and nodal status; prognostic and predictive marker | [53] |
| miR-1307-5p | Upregulated | Associated with chemoresistance and poor prognosis; salivary exosomal biomarker | [54] |
| Panel (e.g., miR-31, miR-21, miR-133a) | Mixed patterns (up/down) | Early diagnosis of OC with high specificity and sensitivity | [15,16] |
| Biomarker Type | Specific Markers | Clinical Utility | References |
|---|---|---|---|
| Cytokines and proteins | IL-8, MMP-9, CYFRA21-1 | Early detection with high sensitivity | [58,59,60] |
| mRNA panel | IL-1β, IL-8, SAT, S100P, OAZ1 | 100% predictive accuracy for OSCC | [61] |
| cfRNA (saliva) | CLEC2B ↑, DAZL, F9, AC008735.2 ↓ | Non-invasive diagnostic tool | [62] |
| miRNA | Expression | Clinical Significance | References |
|---|---|---|---|
| miR-1307-5p ↑ | Poor prognosis, chemoresistance | Prognostic biomarker | [17] |
| miR-24-3p ↑ | Promotes proliferation via PER1 targeting | Diagnostic potential | [18] |
| miR-302b-3p, miR-517b-3p | Unique to OSCC patients | Diagnostic biomarkers | [66] |
| miR-412-3p, and miR-512-3p ↑ | Discriminative power in ROC analysis | Screening tools | [66] |
| Study/Authors | Focus | Key Findings | Clinical Significance | References |
|---|---|---|---|---|
| Pilot study on salivary exosomes | Early diagnosis | Exosomal proteins PSB7, AMER3, and LOXL2 identified in whole mouth saliva (WMS) samples; high diagnostic accuracy | Non-invasive detection of OSCC using salivary biomarkers | [19] |
| EV-based approaches in OSCC | Diagnosis, monitoring, therapy | EVs participate in tumor communication; reflect disease status | Less invasive alternative to biopsy; potential for real-time monitoring | [67,68] |
| miRNA profiling in salivary EVs | Diagnostic biomarkers | miR-302b-3p and miR-517b-3p uniquely expressed; miR-512-3p and miR-412-3p significantly upregulated | Promising non-invasive miRNA biomarkers for OSCC screening | [66] |
| Li et al. | Tumor progression mechanisms | OSCC-derived EVs increase IL-17A, IL-10, IL-1β, PD-L1; activate TRAF6 and c-FOS; inhibition via GW4869 reduces malignancy | EV modulation may serve as a therapeutic target; immune reprogramming potential | [69] |
| Study/Authors | Focus | Key Findings | Clinical Implications | References |
|---|---|---|---|---|
| General review on NGS in OSCC | Early diagnosis and therapy | Underutilization of NGS in OSCC; recurrent mutations in TP53, NOTCH1, PIK3CA; miR-21 dysregulation | Supports precision medicine, miRNA biomarker discovery, and targeted therapies | [70,71] |
| Dongre et al. | Custom NGS panel in FFPE HNSCC samples | Reliable mutation detection in samples preserved up to 17 years; TP53, FAT1, FLG (HPV−), FGFR3 (HPV+); mutations correlated with poor differentiation and survival | Enables retrospective analysis, correlates mutation burden with outcomes, confirms TCGA data | [20] |
| Taiwanese cohort study | Differentiation between recurrence and second primary tumors | NGS identified unique mutations in SYNE1, TP53, CDKN2A; reclassified misdiagnosed recurrences | Improves diagnostic accuracy, guides individualized treatment, refines classification | [21] |
| Study/Authors | Technology | Key Findings | Clinical Implications | References |
|---|---|---|---|---|
| General review on optical imaging in HNSCC | Fluorescence, NBI, Raman, OCT, HSI, PAI | Imaging techniques offer real-time, non-invasive solutions for early detection and intraoperative guidance | Enhances diagnosis, reduces surgical margin errors, improves outcomes | [72,73] |
| FMI vs. NBI in OSCC surgery | Fluorescence Molecular Imaging (FMI), Narrow-Band Imaging (NBI) | FMI superior in submucosal extension detection; NBI cost-effective for early-stage lesions | Improves tumor margin delineation and surgical planning | [74] |
| SI-FLIM in oral dysplasia | SI-FLIM | Enhanced depth-resolved NADH fluorescence; better differentiation of mild dysplasia from normal tissue | Promising for early OSCC detection with higher diagnostic accuracy | [22] |
| Romano et al. | Toluidine blue, Lugol’s iodine, Autofluorescence, NBI, OCT, Ultrasound, Confocal Microscopy | Proposes 3-step diagnostic model integrating multiple non-invasive tools | Reduces biopsy reliance, improves early diagnosis and patient compliance | [75] |
| Therapeutic Approach | Key Findings | Clinical Implications | References |
|---|---|---|---|
| Surgical Resection | Margin width should be adjusted by tumor stage; narrower margins may suffice in early-stage OSCC; wider margins are necessary in advanced stages due to microscopic spread. | Personalized margin criteria may reduce recurrence without excessive tissue sacrifice. | [76] |
| CCRT vs. PORT | CCRT improved survival in pT2N1 OSCC compared to PORT; no benefit seen in pT1 cases. | CCRT may be preferred for selected advanced-stage OSCC, while PORT suffices in early-stage disease. | [77] |
| CCRT (cisplatin + docetaxel) | Safe and effective with response rate comparable to standard regimens; lower incidence of high-grade toxicity. | A feasible alternative to conventional CCRT in advanced OSCC. | [23] |
| Refusal of AT | AT refusal associated with 34% higher recurrence and poorer recurrence-free and overall survival. | Highlights importance of AT in advanced OSCC; aids clinician counseling. | [78] |
| Adjuvant Radiotherapy | Indicated in cases with positive margins or nodal metastasis. | Essential for locoregional control in high-risk patients. | [79] |
| NACT | May reduce tumor size and margin positivity, but lacks survival benefit. | Considered for facilitating conservative surgery; not a survival-enhancing intervention. | [80,81,82] |
| Neoadjuvant Immunotherapy (ICIs) | Promising results in shrinking tumors and converting inoperable cases to respectable. | Represents a novel preoperative strategy in selected cases. | [24] |
| R/M HNSCC Treatment | Limited survival gains; OMCT offers a low-toxicity, cost-effective option. | Suitable for frail patients; emphasizes QOL over aggressive regimens. | [83,84] |
| Personalized Chemotherapy/Multi-omics | Enables molecular stratification and therapeutic tailoring. | Advances precision oncology in HNSCC. | [25] |
| CRT-related Toxicities | Physiology: mucositis, dysphagia, nausea; Psychology: depression, anxiety. | Necessitates holistic management and supportive care integration. | [85] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, P.-C.; Huang, J.-H.; Tsai, C.-C.; Lin, Y.-H.; Kuo, C.-Y. Early Molecular Diagnosis and Comprehensive Treatment of Oral Cancer. Curr. Issues Mol. Biol. 2025, 47, 452. https://doi.org/10.3390/cimb47060452
Hsu P-C, Huang J-H, Tsai C-C, Lin Y-H, Kuo C-Y. Early Molecular Diagnosis and Comprehensive Treatment of Oral Cancer. Current Issues in Molecular Biology. 2025; 47(6):452. https://doi.org/10.3390/cimb47060452
Chicago/Turabian StyleHsu, Po-Chih, Jen-Hsuan Huang, Chung-Che Tsai, Ya-Hsuan Lin, and Chan-Yen Kuo. 2025. "Early Molecular Diagnosis and Comprehensive Treatment of Oral Cancer" Current Issues in Molecular Biology 47, no. 6: 452. https://doi.org/10.3390/cimb47060452
APA StyleHsu, P.-C., Huang, J.-H., Tsai, C.-C., Lin, Y.-H., & Kuo, C.-Y. (2025). Early Molecular Diagnosis and Comprehensive Treatment of Oral Cancer. Current Issues in Molecular Biology, 47(6), 452. https://doi.org/10.3390/cimb47060452