
Hyperbaric Oxygen Therapy Adjuvant Chemotherapy and Radiotherapy through Inhibiting Stemness in Glioblastoma
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Cell Cultures and Treatment Conditions
2.2. Cell Viability Assay
2.3. Neurosphere Assay
2.4. Colony Formation Assay
2.5. Animal Model
2.6. Immunohistochemical Staining
2.7. Western Blot Assay
2.8. Statistical Analysis
3. Results
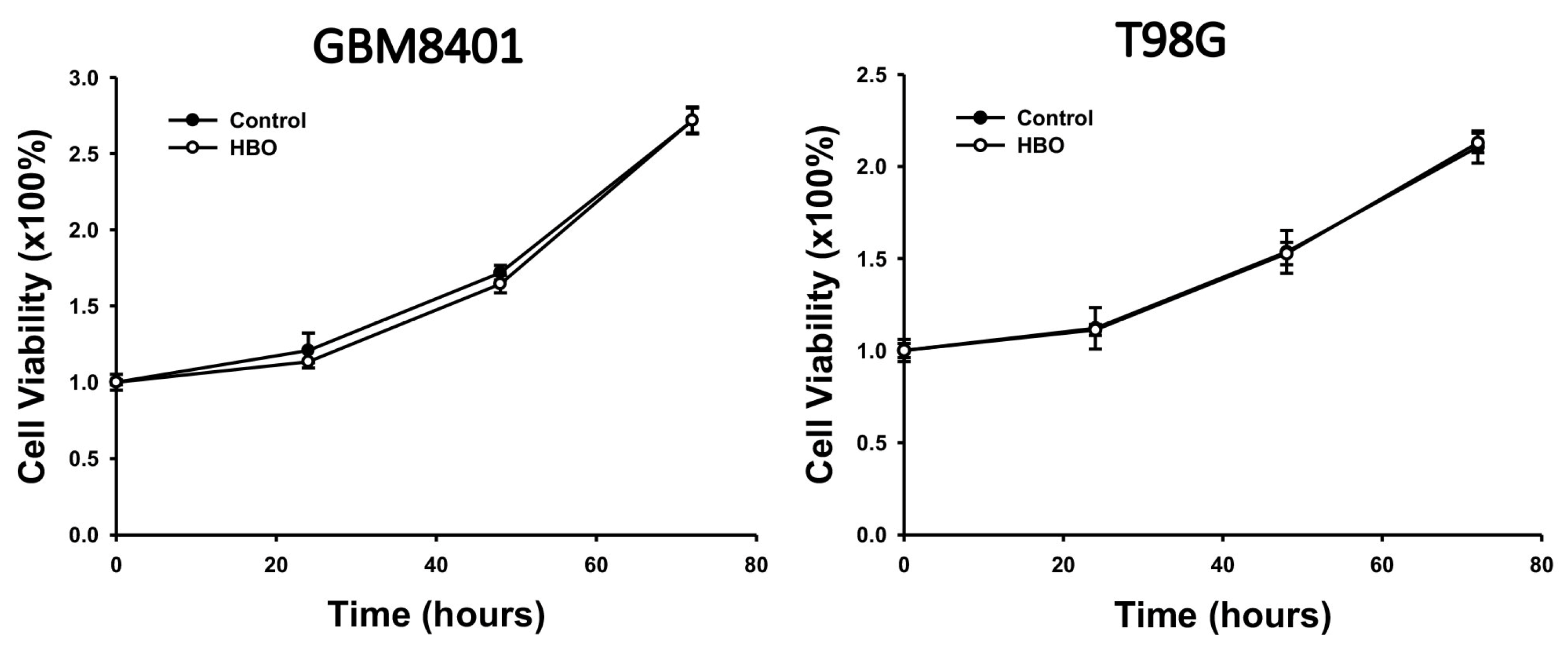
3.1. Effect of HBO Therapy on GBM Cell Viability In Vitro
3.2. Effect of HBO Therapy Combined with Chemotherapy or Radiotherapy In Vitro
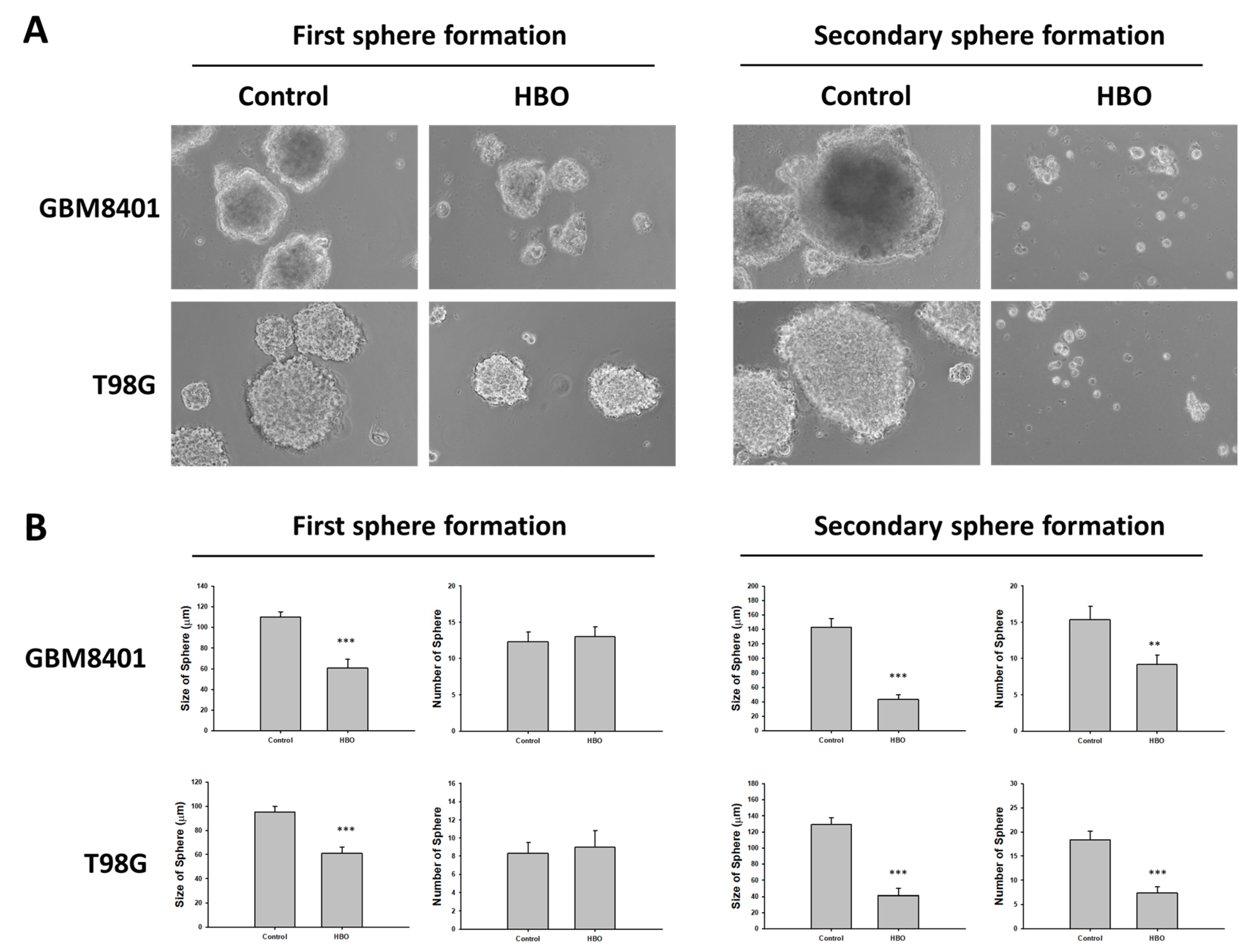
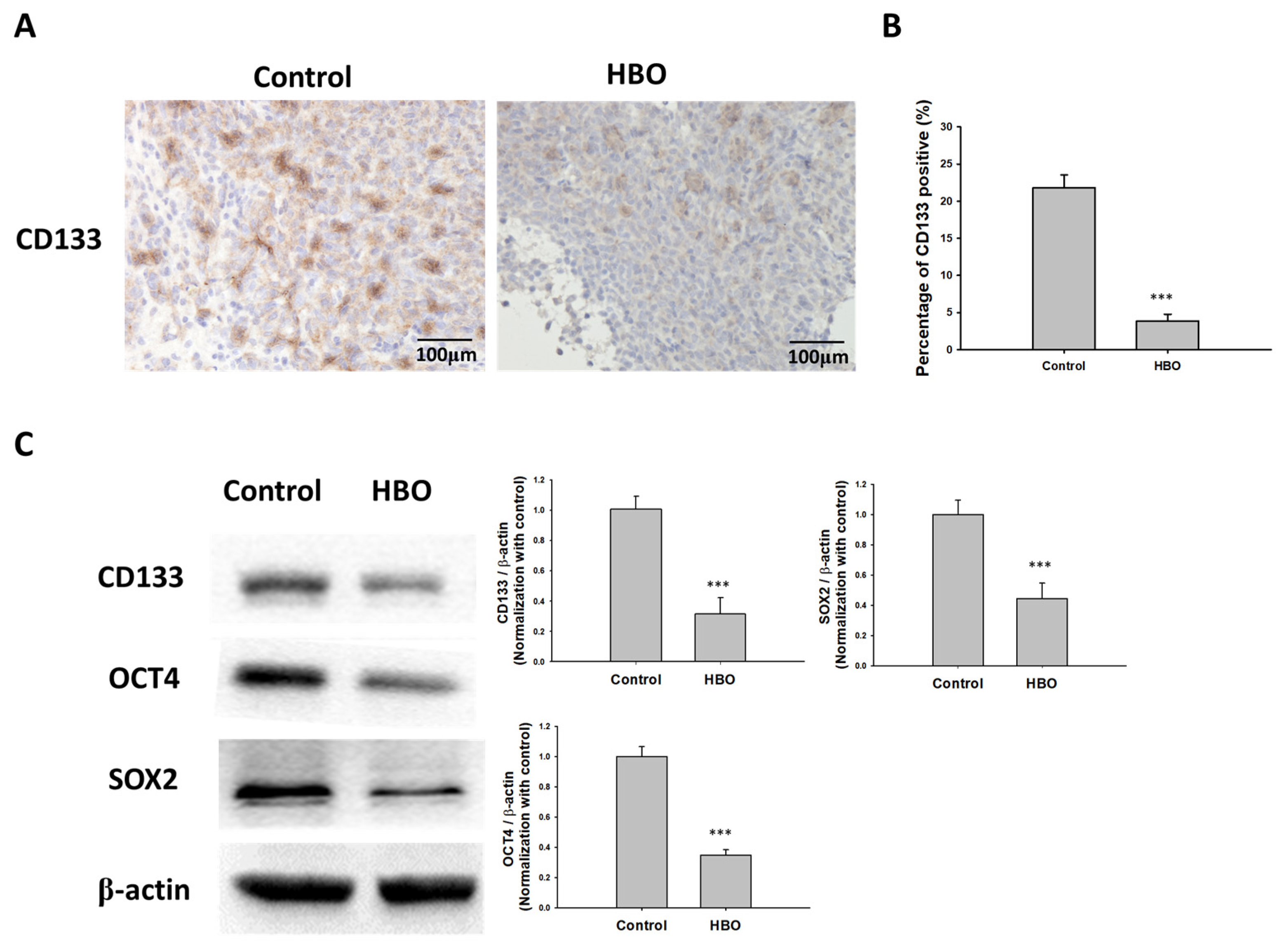
3.3. Effect of HBO Therapy on GBM Stemness In Vitro and In Vivo
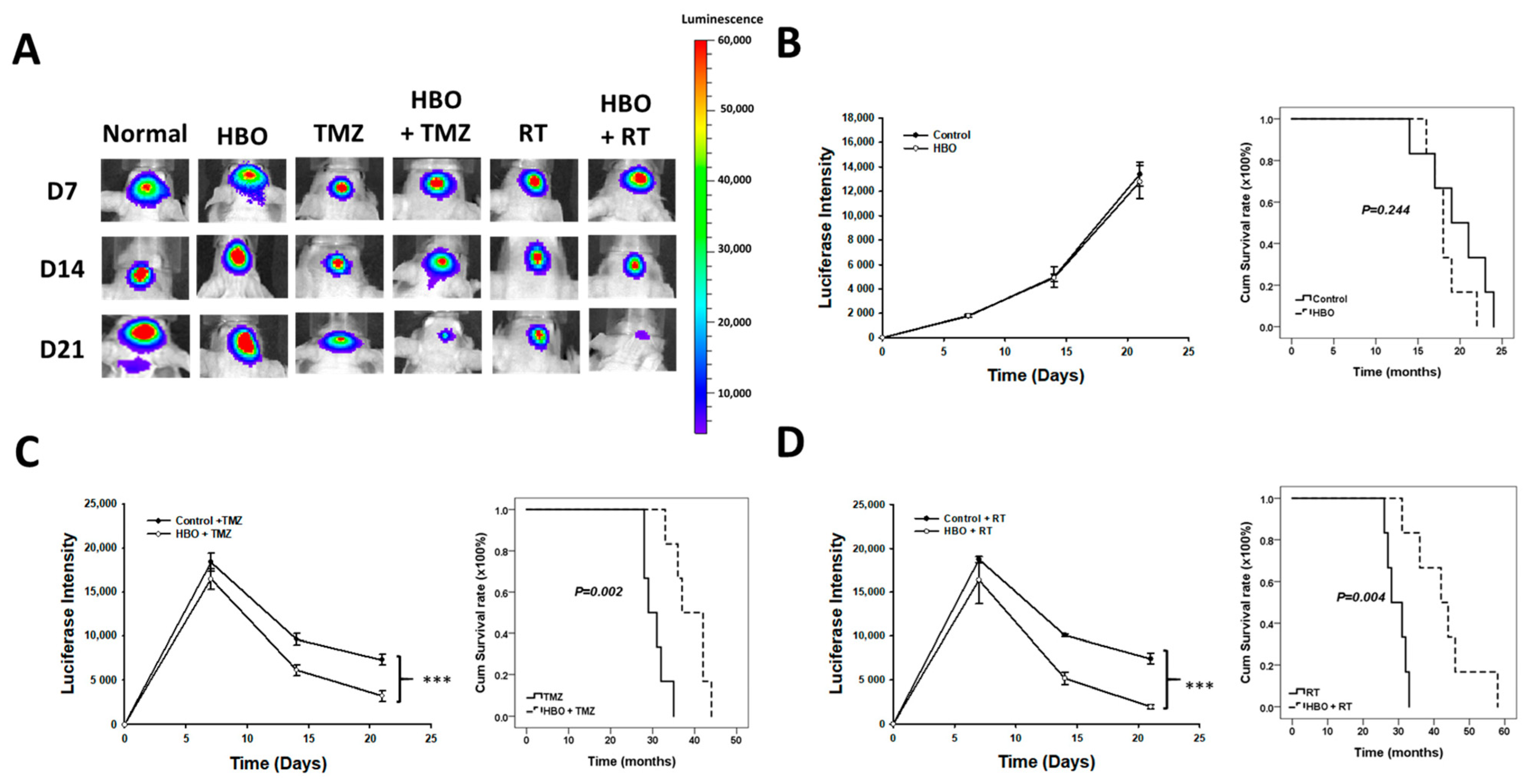
3.4. Effect of HBO Therapy Alone and Combined with Chemotherapy or Radiotherapy In Vivo
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thirant, C.; Bessette, B.; Varlet, P.; Puget, S.; Cadusseau, J.; Tavares, S.D.R.; Studler, J.-M.; Silvestre, D.C.; Susini, A.; Villa, C.; et al. Clinical relevance of tumor cells with stem-like properties in pediatric brain tumors. PLoS ONE 2011, 28, e16375. [Google Scholar] [CrossRef] [PubMed]
- Quader, S.; Kataoka, K.; Cabral, H. Nanomedicine for brain cancer. Adv. Drug Deliv. Rev. 2022, 182, 114115. [Google Scholar] [CrossRef] [PubMed]
- Bruno, F.; Pellerino, A.; Palmiero, R.; Bertero, L.; Mantovani, C.; Garbossa, D.; Soffietti, R.; Rudà, R. Glioblastoma in the Elderly: Review of Molecular and Therapeutic Aspects. Biomedicines 2022, 10, 644. [Google Scholar] [CrossRef] [PubMed]
- Butowski, N.A. Epidemiology and diagnosis of brain tumors. CONTINUUM Lifelong Learn. Neurol. 2015, 21, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Hanif, F.; Muzaffar, K.; Perveen, K.; Malhi, S.M.; Simjee, S.U. Glioblastoma Multiforme: A Review of its Epidemiology and Pathogenesis through Clinical Presentation and Treatment. Asian Pac. J. Cancer Prev. 2017, 1, 3–9. [Google Scholar]
- Francis, S.S.; Ostrom, Q.T.; Cote, D.J.; Smith, T.R.; Claus, E.; Barnholtz-Sloan, J.S. The Epidemiology of Central Nervous System Tumors. Hematol. Oncol. Clin. N. Am. 2022, 36, 23–42. [Google Scholar] [CrossRef] [PubMed]
- Elwatidy, S.M.; Albakr, A.A.; Al Towim, A.A.; Malik, S.H. Tumors of the lateral and third ventricle: Surgical management and outcome analysis in 42 cases. Neurosciences 2017, 22, 274–281. [Google Scholar] [CrossRef] [PubMed]
- McKinnon, C.; Nandhabalan, M.; Murray, S.A.; Plaha, P. Glioblastoma: Clinical presentation, diagnosis, and management. BMJ 2021, 14, n1560. [Google Scholar] [CrossRef]
- Nair, A.G.; Pathak, R.S.; Iyer, V.R.; Gandhi, R.A. Optic nerve glioma: An update. Int. Ophthalmol. 2014, 34, 999–1005. [Google Scholar] [CrossRef]
- Walker, D.A.; Aquilina, K.; Spoudeas, H.; Pilotto, C.; Gan, H.W.; Meijer, L. A new era for optic pathway glioma: A developmental brain tumor with life-long health consequences. Front. Pediatr. 2023, 11, 1038937. [Google Scholar] [CrossRef]
- Janjua, T.I.; Rewatkar, P.; Ahmed-Cox, A.; Saeed, I.; Mansfeld, F.M.; Kulshreshtha, R.; Kumeria, T.; Ziegler, D.S.; Kavallaris, M.; Mazzieri, R.; et al. Frontiers in the treatment of glioblastoma: Past, present and emerging. Adv. Drug Deliv. Rev. 2021, 171, 108–138. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Varn, F.S.; Park, S.-H.; Yoon, B.W.; Park, H.R.; Lee, C.; Verhaak, R.G.W.; Paek, S.H. Perspective of mesenchymal transformation in glioblastoma. Acta Neuropathol. Commun. 2021, 24, 50. [Google Scholar] [CrossRef] [PubMed]
- Jakovlevs, A.; Vanags, A.; Gardovskis, J.; Strumfa, I. Molecular classification of diffuse gliomas. Pol. J. Pathol. 2019, 70, 246–258. [Google Scholar] [CrossRef] [PubMed]
- You, J.-H.; Jiang, J.-L.; He, W.-B.; Ma, H.; Zhou, M.; Chen, X.-X.; Liu, Q.-L.; Huang, C. Addition of hyperbaric oxygen therapy versus usual care alone for inflammatory bowel disease: A systematic review and meta-analysis. Heliyon 2022, 8, e11007. [Google Scholar] [CrossRef]
- Sahni, T.; Singh, P.; John, M.J. Hyperbaric oxygen therapy: Current trends and applications. J. Assoc. Physicians India 2003, 51, 280–284. [Google Scholar] [PubMed]
- Sen, S.; Sen, S. Therapeutic effects of hyperbaric oxygen: Integrated review. Med. Gas Res. 2021, 11, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, S.; Vishwanath, G. Hyperbaric oxygen and wound healing. Indian J. Plast. Surg. 2012, 45, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Lam, G.; Fontaine, R.; Ross, F.L.; Chiu, E.S. Hyperbaric Oxygen Therapy: Exploring the Clinical Evidence. Adv. Skin Wound Care 2017, 30, 181–190. [Google Scholar] [CrossRef]
- Tejada, S.; Batle, J.M.; Ferrer, M.D.; Busquets-Cortés, C.; Monserrat-Mesquida, M.; Nabavi, S.M.; Bibiloni, M.D.M.; Pons, A.; Sureda, A. Therapeutic Effects of Hyperbaric Oxygen in the Process of Wound Healing. Curr. Pharm. Des. 2019, 25, 1682–1693. [Google Scholar] [CrossRef]
- Gottfried, I.; Schottlender, N.; Ashery, U. Hyperbaric Oxygen Treatment-From Mechanisms to Cognitive Improvement. Biomolecules 2021, 15, 1520. [Google Scholar] [CrossRef]
- Levitan, D.M.; Hitt, M.; Geiser, D.R.; Lyman, R. Rationale for hyperbaric oxygen therapy in traumatic injury and wound care in small animal veterinary practice. J. Small Anim. Pract. 2021, 62, 719–729. [Google Scholar] [CrossRef] [PubMed]
- Eve, D.J.; Steele, M.R.; Sanberg, P.R.; Borlongan, C.V. Hyperbaric oxygen therapy as a potential treatment for post-traumatic stress disorder associated with traumatic brain injury. Neuropsychiatr. Dis. Treat. 2016, 12, 2689–2705. [Google Scholar] [CrossRef]
- Fischer, I.; Barak, B. Molecular and Therapeutic Aspects of Hyperbaric Oxygen Therapy in Neurological Conditions. Biomolecules 2020, 10, 1247. [Google Scholar] [CrossRef] [PubMed]
- Moen, I.; Stuhr, L.E. Hyperbaric oxygen therapy and cancer—A review. Target Oncol 2012, 7, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Stepien, K.; Ostrowski, R.P.; Matyja, E. Hyperbaric oxygen as an adjunctive therapy in treatment of malignancies, including brain tumours. Med. Oncol. 2016, 33, 101. [Google Scholar] [CrossRef]
- Fernández, E.; Morillo, V.; Salvador, M.; Santafé, A.; Beato, I.; Rodríguez, M.; Ferrer, C. Hyperbaric oxygen and radiation therapy: A review. Clin. Transl. Oncol. 2021, 23, 1047–1053. [Google Scholar] [CrossRef]
- Friedman, G.K.; Gillespie, G.Y. Cancer Stem Cells and Pediatric Solid Tumors. Cancers 2011, 3, 298–318. [Google Scholar] [CrossRef] [PubMed]
- Ajani, J.A.; Song, S.; Hochster, H.S.; Steinberg, I.B. Cancer Stem Cells: The Promise and the Potential. Semin. Oncol. 2015, 42, S3–S17. [Google Scholar] [CrossRef] [PubMed]
- Ciurea, M.E.; Georgescu, A.M.; Purcaru, S.O.; Artene, S.-A.; Emami, G.H.; Boldeanu, M.V.; Tache, D.E.; Dricu, A. Cancer stem cells: Biological functions and therapeutically targeting. Int. J. Mol. Sci. 2014, 15, 8169–8185. [Google Scholar] [CrossRef]
- Yang, M.; Liu, P.; Huang, P. Cancer stem cells, metabolism, and therapeutic significance. Tumour. Biol. 2016, 37, 5735–5742. [Google Scholar] [CrossRef]
- Yong, L.; Tang, S.; Yu, H.; Zhang, H.; Zhang, Y.; Wan, Y.; Cai, F. The role of hypoxia-inducible factor-1 alpha in multidrug-resistant breast cancer. Front. Oncol. 2022, 12, 964934. [Google Scholar] [CrossRef]
- Shi, Q.Y.; Zhang, S.J.; Liu, L.; Chen, Q.S.; Yu, L.N.; Zhang, F.J.; Yan, M. Sevoflurane promotes the expansion of glioma stem cells through activation of hypoxia-inducible factors in vitro. Br. J. Anaesth. 2015, 114, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Schoning, J.P.; Monteiro, M.; Gu, W. Drug resistance and cancer stem cells: The shared but distinct roles of hypoxia-inducible factors HIF1alpha and HIF2alpha. Clin. Exp. Pharmacol. Physiol. 2017, 44, 153–161. [Google Scholar] [CrossRef]
- Lu, Z.; Ma, J.; Liu, B.; Dai, C.; Xie, T.; Ma, X.; Li, M.; Dong, J.; Lan, Q.; Huang, Q. Hyperbaric oxygen therapy sensitizes nimustine treatment for glioma in mice. Cancer Med. 2016, 5, 3147–3155. [Google Scholar] [CrossRef]
- Song, K.; Chen, J.; Ding, J.; Xu, H.; Xu, H.; Qin, Z. Hyperbaric oxygen suppresses stemness-associated properties and Nanog and oncostatin M expression, but upregulates beta-catenin in orthotopic glioma models. J. Int. Med. Res. 2020, 48, 300060519872898. [Google Scholar] [PubMed]
- Daruwalla, J.; Christophi, C. Hyperbaric oxygen therapy for malignancy: A review. World J. Surg. 2006, 30, 2112–2131. [Google Scholar] [CrossRef] [PubMed]
- Ortega, M.A.; Fraile-Martinez, O.; García-Montero, C.; Callejón-Peláez, E.; Sáez, M.A.; Álvarez-Mon, M.A.; García-Honduvilla, N.; Monserrat, J.; Álvarez-Mon, M.; Bujan, J.; et al. A General Overview on the Hyperbaric Oxygen Therapy: Applications, Mechanisms and Translational Opportunities. Medicina 2021, 24, 864. [Google Scholar] [CrossRef]
- Graham, K.; Unger, E. Overcoming tumor hypoxia as a barrier to radiotherapy, chemotherapy and immunotherapy in cancer treatment. Int. J. Nanomed. 2018, 13, 6049–6058. [Google Scholar] [CrossRef]
- Huang, L.; Boling, W.; Zhang, J.H. Hyperbaric oxygen therapy as adjunctive strategy in treatment of glioblastoma multiforme. Med. Gas Res. 2018, 8, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Heyboer, M.; Sharma, D.; Santiago, W.; McCulloch, N. Hyperbaric Oxygen Therapy: Side Effects Defined and Quantified. Adv. Wound Care 2017, 6, 210–224. [Google Scholar] [CrossRef]
- Janssen, H.L.; Haustermans, K.M.; Balm, A.J.; Begg, A.C. Hypoxia in head and neck cancer: How much, how important? Head Neck 2005, 27, 622–638. [Google Scholar] [CrossRef] [PubMed]
- Dauwe, P.B.; Pulikkottil, B.J.; Lavery, L.; Stuzin, J.M.; Rohrich, R.J. Does hyperbaric oxygen therapy work in facilitating acute wound healing: A systematic review. Plast. Reconstr. Surg. 2014, 133, 208e–215e. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuen, C.-M.; Tsai, H.-P.; Tseng, T.-T.; Tseng, Y.-L.; Lieu, A.-S.; Kwan, A.-L.; Chang, A.Y.W. Hyperbaric Oxygen Therapy Adjuvant Chemotherapy and Radiotherapy through Inhibiting Stemness in Glioblastoma. Curr. Issues Mol. Biol. 2023, 45, 8309-8320. https://doi.org/10.3390/cimb45100524
Yuen C-M, Tsai H-P, Tseng T-T, Tseng Y-L, Lieu A-S, Kwan A-L, Chang AYW. Hyperbaric Oxygen Therapy Adjuvant Chemotherapy and Radiotherapy through Inhibiting Stemness in Glioblastoma. Current Issues in Molecular Biology. 2023; 45(10):8309-8320. https://doi.org/10.3390/cimb45100524
Chicago/Turabian StyleYuen, Chun-Man, Hung-Pei Tsai, Tzu-Ting Tseng, Yu-Lung Tseng, Ann-Shung Lieu, Aij-Lie Kwan, and Alice Y. W. Chang. 2023. "Hyperbaric Oxygen Therapy Adjuvant Chemotherapy and Radiotherapy through Inhibiting Stemness in Glioblastoma" Current Issues in Molecular Biology 45, no. 10: 8309-8320. https://doi.org/10.3390/cimb45100524
APA StyleYuen, C.-M., Tsai, H.-P., Tseng, T.-T., Tseng, Y.-L., Lieu, A.-S., Kwan, A.-L., & Chang, A. Y. W. (2023). Hyperbaric Oxygen Therapy Adjuvant Chemotherapy and Radiotherapy through Inhibiting Stemness in Glioblastoma. Current Issues in Molecular Biology, 45(10), 8309-8320. https://doi.org/10.3390/cimb45100524