

Role of Single Nucleotide Polymorphism L55M in the Paraoxonase 1 Gene as a Risk and Prognostic Factor in Acute Coronary Syndrome


Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Control Individuals
2.2. Clinical Examination and Standard Laboratory Analyses
2.3. Isolation of Genomic DNA
2.4. PCR-RFLP Method of Genotyping for PON1 L55M (rs 854560)
2.5. Agarose Gel Electrophoresis
2.6. Statistical Analyses
3. Results
3.1. PON1 L55M SNP and the Risk for ACS
3.2. Associations of PON1 L55M SNP with Biochemical and Clinical Markers of Patients with ACS
3.3. PON1 L55M SNP and other Factors Influencing the Survival of the Patients with ACS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gaziano, T.A.; Bitton, A.; Anand, S.; Abrahams-Gessel, S.; Murphy, A. Growing Epidemic of Coronary Heart Disease in Low- and Middle-Income Countries. Curr. Probl. Cardiol. 2010, 35, 72–115. [Google Scholar] [CrossRef] [PubMed]
- Berliner, J.A.; Navab, M.; Fogelman, A.M.; Frank, J.S.; Demer, L.L.; Edwards, P.A.; Watson, A.D.; Lusis, A.J. Atherosclerosis: Basic Mechanisms. Oxidation, Inflammation, and Genetics. Circulation 1995, 91, 2488–2496. [Google Scholar] [CrossRef] [PubMed]
- Van Himbergen, T.M.; van Tits, L.J.; Roest, M.; Stalenhoef, A.F. The Story of Pon1: How an Organophosphate-Hydrolysing Enzyme Is Becoming a Player in Cardiovascular Medicine. Neth. J. Med. 2006, 64, 34–38. [Google Scholar] [PubMed]
- Soran, H.; Schofield, J.D.; Durrington, P.N. Antioxidant Properties of Hdl. Front. Pharmacol. 2015, 6, 222. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Lang, X.; Cui, S.; Zou, L.; Cao, J.; Wang, S.; Wu, X. Quantitative Assessment of the Influence of Paraoxonase 1 Activity and Coronary Heart Disease Risk. DNA Cell Biol. 2012, 31, 975–982. [Google Scholar] [CrossRef]
- Costa, L.G.; Vitalone, A.; Cole, T.B.; Furlong, C.E. Modulation of Paraoxonase (Pon1) Activity. Biochem. Pharmacol. 2005, 69, 541–550. [Google Scholar] [CrossRef]
- Primo-Parmo, S.L.; Sorenson, R.C.; Teiber, J.; La Du, B.N. The Human Serum Paraoxonase/Arylesterase Gene (Pon1) Is One Member of a Multigene Family. Genomics 1996, 33, 498–507. [Google Scholar] [CrossRef]
- Draganov, D.I.; La Du, B.N. Pharmacogenetics of Paraoxonases: A Brief Review. Naunyn Schmiedebergs Arch. Pharmacol. 2004, 369, 78–88. [Google Scholar] [CrossRef]
- Vlaykova, T.; Doneva-Basheva, K.; Emin, S.; Yordanova, K.; Tsoneva, V.; Zhelev, V.; Andreev, Z.; Arnaudova, Z.; Ilchev, P.; Valcheva, S.; et al. Role of the Serum Paraoxonase 1 in Acute Coronary Disease. Heart-Lung 2009, 15, 35–47. [Google Scholar]
- Mackness, M.I.; Mackness, B.; Durrington, P.N. Paraoxonase and Coronary Heart Disease. Atheroscler. Suppl. 2002, 3, 49–55. [Google Scholar] [CrossRef]
- Ahmed, Z.; Ravandi, A.; Maguire, G.F.; Emili, A.; Draganov, D.; La Du, B.N.; Kuksis, A.; Connelly, P.W. Multiple Substrates for Paraoxonase-1 During Oxidation of Phosphatidylcholine by Peroxynitrite. Biochem. Biophys. Res. Commun. 2002, 290, 391–396. [Google Scholar] [CrossRef]
- Abudayyak, M.; Boran, T.; Tukel, R.; Oztas, E.; Özhan, G. The Role of Pon1 Variants in Disease Susceptibility in a Turkish Population. Glob. Med. Genet. 2020, 7, 41–46. [Google Scholar] [CrossRef]
- Ponce-Ruiz, N.; Murillo-González, F.E.; Rojas-García, A.E.; Mackness, M.; Bernal-Hernández, Y.Y.; Barrón-Vivanco, B.S.; González-Arias, C.A.; Medina-Díaz, I.M. Transcriptional Regulation of Human Paraoxonase 1 by Nuclear Receptors. Chem. Biol. Interact. 2017, 268, 77–84. [Google Scholar] [CrossRef]
- Zuin, M.; Trentini, A.; Marsillach, J.; D’Amuri, A.; Bosi, C.; Roncon, L.; Passaro, A.; Zuliani, G.; Mackness, M.; Cervellati, C. Paraoxonase-1 (Pon-1) Arylesterase Activity Levels in Patients with Coronary Artery Disease: A Meta-Analysis. Dis. Markers 2022, 2022, 4264314. [Google Scholar] [CrossRef]
- Ko, Y.L.; Ko, Y.S.; Wang, S.M.; Hsu, L.A.; Chang, C.J.; Chu, P.H.; Cheng, N.J.; Chen, W.J.; Chiang, C.W.; Lee, Y.S. The Gln-Arg 191 Polymorphism of the Human Paraoxonase Gene Is Not Associated with the Risk of Coronary Artery Disease among Chinese in Taiwan. Atherosclerosis 1998, 141, 259–264. [Google Scholar] [CrossRef]
- Arca, M.; Ombres, D.; Montali, A.; Campagna, F.; Mangieri, E.; Tanzilli, G.; Campa, P.P.; Ricci, G.; Verna, R.; Pannitteri, G. Pon1 L55m Polymorphism Is Not a Predictor of Coronary Atherosclerosis Either Alone or in Combination with Q192r Polymorphism in an Italian Population. Eur. J. Clin. Investig. 2002, 32, 9–15. [Google Scholar] [CrossRef]
- Wheeler, J.G.; Keavney, B.D.; Watkins, H.; Collins, R.; Danesh, J. Four Paraoxonase Gene Polymorphisms in 11212 Cases of Coronary Heart Disease and 12786 Controls: Meta-Analysis of 43 Studies. Lancet 2004, 363, 689–695. [Google Scholar] [CrossRef]
- Agrawal, S.; Tripathi, G.; Prajnya, R.; Sinha, N.; Gilmour, A.; Bush, L.; Mastana, S. Paraoxonase 1 Gene Polymorphisms Contribute to Coronary Artery Disease Risk among North Indians. Indian J. Med. Sci. 2009, 63, 335–344. [Google Scholar]
- Gupta, N.; Singh, S.; Maturu, V.N.; Sharma, Y.P.; Gill, K.D. Paraoxonase 1 (Pon1) Polymorphisms, Haplotypes and Activity in Predicting Cad Risk in North-West Indian Punjabis. PLoS ONE 2011, 6, e17805. [Google Scholar] [CrossRef]
- Hernández-Díaz, Y.; Tovilla-Zárate, C.A.; Juárez-Rojop, I.E.; González-Castro, T.B.; Rodríguez-Pérez, C.; López-Narváez, M.L.; Rodríguez-Pérez, J.M.; Cámara-Álvarez, J.F. Effects of Paraoxonase 1 Gene Polymorphisms on Heart Diseases: Systematic Review and Meta-Analysis of 64 Case-Control Studies. Medicine 2016, 95, e5298. [Google Scholar] [CrossRef]
- Chen, H.; Ding, S.; Zhou, M.; Wu, X.; Liu, X.; Liu, J.; Wu, Y.; Liu, D. Pon1 L55m and Q192r Gene Polymorphisms and Cad Risks in Patients with Hyperlipidemia: Clinical Study of Possible Associations. Herz 2018, 43, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Yun, Y.; Chen, H.; Yang, G.; Jiang, Y.; Pan, Y.; Yuan, S.; Huang, J.; Su, L.; Wu, Y.; et al. Association of Pon-1 Polymorphism with Susceptibility to and Severity of Ischemic Stroke in the Chinese Population. Pers. Med. 2022, 19, 219–228. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.outcomes-umassmed.org/grace/acs_risk2/index.html (accessed on 1 November 2022).
- Kumar, D.; Ashok, A.; Saghir, T.; Khan, N.; Solangi, B.A.; Ahmed, T.; Karim, M.; Abid, K.; Bai, R.; Kumari, R.; et al. Prognostic value of GRACE score for in-hospital and 6 months outcomes after non-ST elevation acute coronary syndrome. Egypt Heart J. 2021, 73, 22. [Google Scholar] [CrossRef]
- Tacheva, T.; Zienolddiny, S.; Dimov, D.; Vlaykova, D.; Vlaykova, T. The Leukocyte Telomere Length, Single Nucleotide Polymorphisms near Terc Gene and Risk of Copd. PeerJ 2021, 9, e12190. [Google Scholar] [CrossRef]
- Suehiro, T.; Ikeda, Y.; Shiinoki, T.; Inoue, M.; Kumon, Y.; Itahara, T.; Hashimoto, K. Serum Paraoxonase (Pon1) Concentration in Patients Undergoing Hemodialysis. J. Atheroscler. Thromb. 2002, 9, 133–138. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. Acc/Aha Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar]
- Ji, J.; Pan, E.; Li, J.; Chen, J.; Cao, J.; Sun, D.; Lu, X.; Chen, S.; Gu, D.; Duan, X.; et al. Classical Risk Factors of Cardiovascular Disease among Chinese Male Steel Workers: A Prospective Cohort Study for 20 Years. BMC Public Health 2011, 11, 497. [Google Scholar] [CrossRef]
- El Hadri, K.; Smith, R.; Duplus, E.; El Amri, C. Inflammation, Oxidative Stress, Senescence in Atherosclerosis: Thioredoxine-1 as an Emerging Therapeutic Target. Int. J. Mol. Sci. 2021, 23, 77. [Google Scholar] [CrossRef]
- Bounafaa, A.; Berrougui, H.; Ghalim, N.; Nasser, B.; Bagri, A.; Moujahid, A.; Ikhlef, S.; Camponova, P.; Yamoul, N.; Simo, O.K.; et al. Association between Paraoxonase 1 (Pon1) Polymorphisms and the Risk of Acute Coronary Syndrome in a North African Population. PLoS ONE 2015, 10, e0133719. [Google Scholar] [CrossRef]
- Aviram, M.; Rosenblat, M. Paraoxonases 1, 2, and 3, Oxidative Stress, and Macrophage Foam Cell Formation During Atherosclerosis Development. Free Radic. Biol. Med. 2004, 37, 1304–1316. [Google Scholar] [CrossRef]
- Garin, M.C.; James, R.W.; Dussoix, P.; Blanche, H.; Passa, P.; Froguel, P.; Ruiz, J. Paraoxonase Polymorphism Met-Leu54 Is Associated with Modified Serum Concentrations of the Enzyme. A Possible Link between the Paraoxonase Gene and Increased Risk of Cardiovascular Disease in Diabetes. J. Clin. Investig. 1997, 99, 62–66. [Google Scholar] [CrossRef]
- Kallel, A.; Sediri, Y.; SbaΓЇ, M.H.; Mourali, M.S.; Feki, M.; Elasmi, M.; Taieb, S.H.; Sanhaji, H.; Souheil, O.; Mechmeche, R.; et al. The Paraoxonase L55m and Q192r Gene Polymorphisms and Myocardial Infarction in a Tunisian Population. Clin. Biochem. 2010, 43, 1461–1463. [Google Scholar] [CrossRef]
- Grzegorzewska, A.E.; Ostromecka, K.; Swiderska, M.K.; Adamska, P.; Mostowska, A.; Jagodzinski, P.P. Paraoxonase 1 Gene Variants Concerning Cardiovascular Mortality in Conventional Cigarette Smokers and Non-Smokers Treated with Hemodialysis. Sci. Rep. 2021, 11, 19467. [Google Scholar] [CrossRef]
- Bachar, A.; Benmessaoud, F.A.; Diatta, A.; Fadoum, H.; Haroun, A.E.; Oukerraj, L.; Cherti, M. Predictive factors of heart failure in acute coronary syndrome: Institutional cross-sectional study. Ann. Med. Surg. 2022, 81, 104332. [Google Scholar] [CrossRef]
- Pramudyo, M.; Bijaksana, T.L.; Yahya, A.F.; Putra, I.C.S. Novel scoring system based on clinical examination for prediction of in-hospital mortality in acute coronary syndrome patients: A retrospective cohort study. Open Heart 2022, 9, e002095. [Google Scholar] [CrossRef]
- Pramudyo, M.; Yahya, A.F.; Martanto, E.; Tiksnadi, B.B.; Karwiky, G.; Rafidhinar, R.; Putri, G.N.I. Predictors of In-Hospital Mortality in Patients with Acute Coronary Syndrome in Hasan Sadikin Hospital, Bandung, Indonesia: A Retrospective Cohort Study. Acta Med. Indones. 2022, 54, 379–388. [Google Scholar]



{kind=link}
{kind=link}
| Indicators | Patients N (%) | Controls N (%) | p-Value |
|---|---|---|---|
| 77 | 122 | ||
| Sex | 0.006 | ||
| Males | 49 (63.6) | 53 (43.4) | |
| Females | 28 (36.4) | 69 (56.6) | |
| Age (years) | <0.0001 | ||
| Mean ± SEM | 64.53 ± 1.36 | 56.99 ± 1.17 | |
| BMI (kg/m2) | 0.618 | ||
| Mean ± SEM | 27.13 ± 0.52 | 26.81 ± 0.39 | |
| BMI | (77) | (101) | 0.504 |
| Normal | 21 (27.3) | 34 (33.7) | |
| Overweight | 41 (53.2) | 45 (44.6) | |
| Obese | 15 (19.5) | 22 (21.8) | |
| Smoking habits | (77) | (111) | 0.636 |
| Non-smokers | 46 (59.7) | 72 (64.9) | |
| Ex-smoker | 6 (7.8) | 10 (9.0) | |
| Current smokers | 25 (32.5) | 29 926.1) | |
| Total cholesterol (TC) (mmol/L) Mean ± SEM | 5.70 ± 0.23 | 5.02 ± 0.47 | 0.220 |
| HDL-cholesterol (mmol/L) Mean ± SEM | 1.78 ± 0.04 | 1.86 ± 0.23 | 0.934 |
| LDL-cholesterol (mmol/L) Mean ± SEM | 3.32 ± 0.20 | 2.42 ± 0.46 | 0.071 |
| Triglycerides (TG) (mmol/L)Mean ± SEM | 1.33 ± 0.11 | 1.14 ± 0.22 | 0.507 |
| Creatinine (µmol/L) Mean ± SEM | 100.56 ± 3.53 | NA | |
| GFR (mL/min/1.73 m2) Mean ± SEM | 69.06 ± 2.63 | NA | |
| Troponin (ng/mL) Mean ± SEM | 13.63 ± 10.64 | NA | |
| CPK (U/L) Mean ± SEM | 665.26 ± 111.16 | NA | |
| CPK-MB (U/L) Mean ± SEM | 93.09 ± 15.44 | NA | |
| LVEF | (77) | NA | |
| ≤29% | 5 (6.5) | ||
| 30–39% | 2 (2.6) | ||
| 40–49% | 29 (37.7) | ||
| ≥50% | 41 (53.2) | ||
| Diabetes | (77) | NA | |
| No | 53 (68.8) | ||
| D2T | 15 (19.5) | ||
| D1T | 6 (7.8) | ||
| Glucose intolerance | 3 (3.9) | ||
| Diagnosis | (77) | ||
| STEMI | 53 (68.8) | ||
| UA | 10 (13.0) | ||
| NSTEMI | 14 (18.2) | ||
| Blood vessels affected | (74) | NA | |
| none | 6 (8.1) | ||
| one vessel | 26 (35.1) | ||
| two vessels | 15 (20.3) | ||
| three vessels | 27 (36.5) | ||
| GRACE score | NA | ||
| Mean ± SEM | 120.95 ± 3.86 | ||
| GRACE score–short period risk | NA | ||
| Low risk (≤108) | 26 (33.8) | ||
| Moderate risk (109–139) | 31 (40.2) | ||
| High risk ≥140 | 20 (26.0) | ||
| GRACE score–long period risk | NA | ||
| Low risk (≤88) | 12 (15.6) | ||
| Moderate risk (89–117) | 26 (33.8) | ||
| High risk (≥118) | 39 (50.6) | ||
| 1–year survival | |||
| Alive | 57 (74.0) | ||
| Dead | 20 (26.0) | ||
| 5–year survival | |||
| Alive | 49 (63.3) | ||
| Dead | 28 (36.4) | ||
| 9–year survival | |||
| Alive | 39 (50.6) | ||
| Dead | 38 (49.4) |
| Primers | Annealing Temperature | Restrictase | PCRand Allele-Specific Products |
|---|---|---|---|
| L55MF (5′- GAA GAG TGA TGT ATA GCC CCA G-3′) L55MR (5′- ACT CAC AGA GCT AAT GAA AGC CA-3′), | 55 °C | NlaIII (37 °C) | PCR product–169 bp L allele–169 bp M allele–127 + 42 bp (not visible). |
| L55M SNP in PON1 | Patients | Controls | OR (95% CI), p-Value | OR (95% CI), p-Value | ||
|---|---|---|---|---|---|---|
| N | Frequency | N | Frequency | (After Adjustment for Sex and Age) | ||
| n = 77 | (%) | n = 122 | (%) | |||
| Genotype distribution | ||||||
| LL | 28 | 36.4 | 69 | 56.6 | 1.0 (referent) | |
| LM | 39 | 50.6 | 42 | 34.4 | 2.288 (1.233–4.248), p = 0.009 | 2.390 (1.230–4.643), p = 0.010 |
| MM | 10 | 13 | 11 | 9 | 2.240 (0.856–5.865), p = 0.100 | 2.275 (0.973–7.782), p = 0.056 |
| LM + MM | 49 | 63.6 | 53 | 43.4 | 2.278 (1.268–4.095), p = 0.006 | 2.457 (1.306–4.622), p = 0.005 |
| Allele distribution | ||||||
| 55L | 104 | 62.7 | 180 | 73.8 | 1.0 (referent) | |
| 55M | 62 | 37.3 | 64 | 26.2 | 1.677 (1.098–2.561), p = 0.017 | |
| Patients | Controls | OR (95% CI), p-Value | OR (95% CI), p-Value (After Adjustment for Sex and Age) | |||
|---|---|---|---|---|---|---|
| N | Frequency | N | Frequency | |||
| (%) | (%) | |||||
| Genotype distribution–patients with STEMI | ||||||
| n = 53 | n = 122 | |||||
| LL | 17 | 32.1 | 69 | 56.6 | 1.0 (referent) | |
| LM | 29 | 54.7 | 42 | 34.4 | 2.803 (1.376–5.706), p = 0.005 | 2.750(1.304–5.798), p = 0.008 |
| MM | 7 | 13.2 | 11 | 9 | 2.583(0.872–7.652), p = 0.087 | 3.029 (0.950–9.658), p = 0.061 |
| LM + MM | 36 | 67.9 | 53 | 43.4 | 2.757 (1.398–5.436), p = 0.003 | 2.801(1.372–5.718), p = 0.005 |
| Genotype distribution–patients with UA | ||||||
| n = 10 | (%) | n = 122 | (%) | |||
| LL | 4 | 40 | 69 | 56.6 | 1.0 (referent) | |
| LM | 4 | 40 | 42 | 34.4 | 1.643 (0.390–6.920), p = 0.499 | 1.834(0.419–8.029), p = 0.421 |
| MM | 2 | 20 | 11 | 9 | 3.136 (0.512–19.22), p = 0.216 | 4.967 (0.713–34.63), p = 0.106 |
| LM + MM | 6 | 60 | 53 | 43.4 | 1.953 (0.542–7.273), p = 0.318 | 2.295(0.590–8.927), p = 0.231 |
| Genotype distribution–patients with NSTEMI | ||||||
| n = 14 | (%) | n = 122 | (%) | |||
| LL | 7 | 50 | 69 | 56.6 | 1.0 (referent) | |
| LM | 6 | 42.9 | 42 | 34.4 | 1.408 (0.443–4.474), p = 0.562 | 1.597 (0.462–5.527), p = 0.460 |
| MM | 1 | 7.1 | 11 | 9 | 0.896(0.100–8.005), p = 0.922 | 2.301 (0.214–24.80), p = 0.492 |
| LM + MM | 7 | 50 | 53 | 43.4 | 1.302(0.430–3.939), p = 0.640 | 1.670 (0.505–5.523), p = 0.400 |
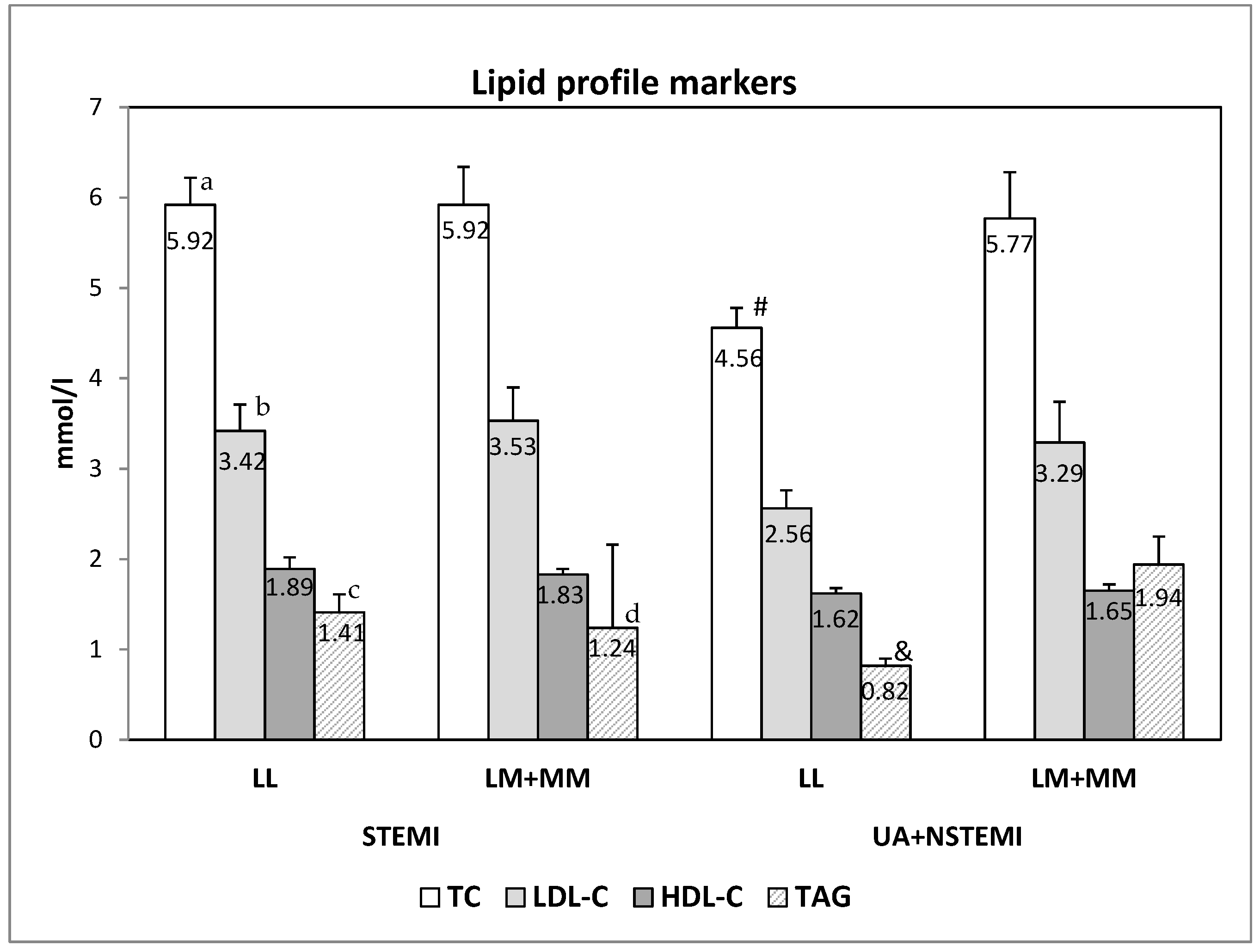
| Indicators | STEMI | LL | NSTEACS (UA + NSTEMI) | LM + MM | ||||
|---|---|---|---|---|---|---|---|---|
| LL (n = 17) | LL_LM (n = 36) | p-Value (LL vs. LM + MM) | p-Value– (STEMI vs. UA + NSTEMI) | LL (n = 11) | LL_LM (n = 13) | p-Value (LL vs. LM + MM) | p-Value– (STEMI vs. UA + NSTEMI) | |
| TC (mmol/L) Mean ± SEM | 5.92 ± 0.30 | 5.92 ± 0.43 | 0.112 | 0.005 | 4.56 ± 0.22 | 5.77 ± 0.51 | 0.022 | 0.919 |
| LDL-C (mmol/L) Mean ± SEM | 3.42 ± 0.29 | 3.53 ± 0.37 | 0.265 | 0.042 | 2.56 ± 0.21 | 3.29 ± 0.45 | 0.106 | 0.768 |
| HDL-C (mmol/L) Mean ± SEM | 1.89 ± 0.13 | 1.83 ± 0.06 | 0.864 | 0.208 | 1.62 ± 0.06 | 1.65 ± 0.08 | 0.955 | 0.113 |
| TAG (mmol/L) Mean ± SEM | 1.41 ± 0.20 | 1.24 ± 0.16 | 0.299 | 0.029 | 0.82 ± 0.08 | 1.94 ± 0.31 | 0.015 | 0.034 |
| Creatinine (µmol/L) Mean ± SEM | 100.24 ± 5.54 | 102.54 ± 5.40 | 0.614 | 0.578 | 87.36 ± 6.61 | 106.63 ± 8.05 | 0.072 | 0.511 |
| GFR (ml/min/1.73 m2) Mean ± SEM | 64 ± 5.54 | 69.97 ± 4.05 | 0.620 | 0.134 | 77.10 ± 6.80 | 65.50 ± 5.70 | 0.361 | 0.483 |
| Survival Periods | STEMI N (%) | NSTEACS N (%) | p Value (STEMI vs. NSTEACS) |
|---|---|---|---|
| 1 year survival Alive Dead | 38 (71.7) 15 (28.3) | 22 (91.7) 2 (8.3) | 0.050 |
| 5-year survival | |||
| Alive Dead | 32 (60.4) 21 (39.6) | 17 (70.8) 7 (29.2) | 0.377 |
| 9-year survival | |||
| Alive Dead | 26 (49.1) 27 (50.9) | 13 (54.2) 11 (45.8) | 0.678 |
| The Whole Group with ACS | STEMI | NSTEACS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Factor (N) | p-Value | HR | CI (95%) | p-Value | HR | CI (95%) | p-Value | HR | CI (95%) |
| Age | 0.003 | 0.006 | 0.440 | ||||||
| <60 years | 1 | 1 | 1 | ||||||
| ≥60 years | 4.82 | 1.70–13.70 | 4.57 | 1.56–13.43 | 103.73 | 0.001–1351 | |||
| GFR | 0.027 | 0.202 | 0.456 | ||||||
| ≥60 mL/min/1.73m2 | 1 | 1 | 1 | ||||||
| ≤60 mL/min/1.73m2 | 3.07 | 1.14–8.32 | 1.96 | 0.70–5.51 | 304.56 | 0.000–1036 | |||
| Previous incidence of infarction | 0.161 | 1 1.98 | 0.76–5.12 | 0.020 | 1 3.34 | 1.21–9.26 | 0.832 | 1 0.74 | 0.05–11.86 |
| No | |||||||||
| Yes | |||||||||
| Cardiogenic shock | 0.002 | 0.006 | NA | ||||||
| No | 1 | 1 | |||||||
| Yes | 7.73 | 2.17–27.56 | 6.17 | 1.70–22.35 | |||||
| Lung edema | 0.026 | 0.016 | 0.884 | ||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 4.15 | 1.19–14.53 | 4.80 | 1.34–17.29 | 0.047 | 0.000–8242 | |||
| Cardiac asthma | 0.008 | 0.043 | NA | ||||||
| No | 1 | 1 | |||||||
| Yes | 3.91 | 1.42–10.79 | 2.99 | 1.04–8.65 | |||||
| ST-segment elevation | 0.025 | 0.335 | NA | ||||||
| No | 1 | 1 | |||||||
| Yes | 5.41 | 1.24–23.66 | 24.99 | 0.04–1724 | |||||
| Cardiac arrest | 0.007 | 0.002 | 0.884 | ||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 5.58 | 1.59–19.63 | 7.94 | 2.18–28.91 | 0.047 | 0.000–8242 | |||
| LVEF | 0.011 | 0.030 | 0.545 | ||||||
| ≥50 | 1 | 1 | 1 | ||||||
| <50 | 4.32 | 1.41–13.26 | 4.08 | 1.15–14.49 | 2.36 | 0.15–37.68 | |||
| Affected blood vessels 1 or 2 3 (TVD) | 0.031 | 1 2.89 | 1.10–7.61 | 0.007 | 1 4.19 | 1.48–11.80 | 0.992 | 1 1.15 | 0.07–18.38 |
| AV block | 0.001 | 0.005 | NA | ||||||
| No | 1 | 1 | |||||||
| Yes | 8.07 | 2.25–28.93 | 6.49 | 1.78–23.69 | |||||
| CAD | 0.131 | 0.056 | 0.658 | ||||||
| <50 | 1 | 1 | 1 | ||||||
| ≥50 | 2.37 | 0.77–7.27 | 3.43 | 0.97–12.17 | 0.54 | 0.03–8.56 | |||
| PON1 L55M SNP | 0.555 | 0.51–3.52 | 0.789 | 0.40–3.39 | 0.451 | 82.72 1 | 0.001–8050 | ||
| LL | 1.34 | 1.16 | |||||||
| LM + MM | 1 | 1 | |||||||
| 1 Year’s Period | 5 Years’ Period | 9 Years’ Period | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Factor (N) | p-Value | HR | CI (95%) | p-Value | HR | CI (95%) | p-Value | HR | CI (95%) |
| Age | 0.093 | 0.237 | 0.117 | ||||||
| <60 years | 1 | 1 | 1 | ||||||
| ≥60 years | 3.60 | 0.81–16.09 | 1.18 | 0.68–4.86 | 1.97 | 0.84–4.60 | |||
| GFR | 0.776 | 0.310 | 0.750 | ||||||
| ≥60 mL/min/1.73m2 | 1 | 1 | 1 | ||||||
| ≤60 mL/min/1.73m2 | 0.78 | 0.77–4.75 | 2.24 | 0.47–10.67 | 0.85 | 0.31–2.35 | |||
| Previous incidence of infarction No Yes | 0.528 | 1 1.60 | 0.37–6.95 | 0.092 | 1 2.24 | 0.88–5.72 | 0.006 | 1 3.15 | 1.39–7.14 |
| Cardiogenic shock | 0.015 | 0.013 | 0.040 | ||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 62.80 | 2.20–1790 | 16.31 | 1.81–146.81 | 8.10 | 1.10–59.61 | |||
| Lung edema | 0.265 | 0.412 | 0.685 | ||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 3.50 | 0.39–31.84 | 1.86 | 0.42–8.18 | 1.34 | 0.33–5.53 | |||
| Cardiac asthma | 0.146 | 0.132 | 0.646 | ||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 4.11 | 0.61–27.77 | 2.74 | 0.74–10.14 | 1.33 | 0.40–4.41 | |||
| ST-segment elevation | 0.296 | 0.450 | 0.135 | ||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 2.96 | 0.39–22.72 | 1.58 | 0.48–5.19 | 2.26 | 0.78–6.54 | |||
| Cardiac arrest | 0.291 | 0.297 | 0.580 | ||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 3.85 | 0.31–50.00 | 2.56 | 0.44–14.71 | 1.52 | 0.34–6.80 | |||
| LVEF | 0.424 | 0.261 | 0.240 | ||||||
| ≥50 | 1 | 1 | 1 | ||||||
| <50 | 1.81 | 0.42–7.69 | 1.77 | 0.65–7.77 | 1.66 | 0.71–3.82 | |||
| Affected blood vessels | 0.056 | 0.027 | 0.009 | ||||||
| 1 or 2 | 1 | 1 | 1 | ||||||
| 3 (TVD) | 6.90 | 0.96–49.79 | 4.61 | 1.19–17.87 | 4.91 | 1.49–16.20 | |||
| AV block | 0.018 | 0.039 | 0.209 | ||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 14.53 | 1.58–133.59 | 6.11 | 1.09–34.14 | 2.79 | 0.57–13.66 | |||
| CAD | 0.149 | 0.230 | 0.226 | ||||||
| <50 | 1 | 1 | 1 | ||||||
| ≥50 | 5.82 | 0.53–63.50 | 2.54 | 0.55–11.68 | 2.20 | 0.62–7.86 | |||
| PON1 L55M SNP | 0.310 | 0.55–6.25 | 0.916 | 0.41–2.72 | 0.958 | 0.46–2.28 | |||
| LL | 1.87 | 1.05 | 1.02 | ||||||
| LM + MM | 1 | 1 | 1 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doneva-Basheva, K.I.; Gospodinov, K.; Tacheva, T.; Dimov, D.; Vlaykova, T.I. Role of Single Nucleotide Polymorphism L55M in the Paraoxonase 1 Gene as a Risk and Prognostic Factor in Acute Coronary Syndrome. Curr. Issues Mol. Biol. 2022, 44, 5915-5932. https://doi.org/10.3390/cimb44120403
Doneva-Basheva KI, Gospodinov K, Tacheva T, Dimov D, Vlaykova TI. Role of Single Nucleotide Polymorphism L55M in the Paraoxonase 1 Gene as a Risk and Prognostic Factor in Acute Coronary Syndrome. Current Issues in Molecular Biology. 2022; 44(12):5915-5932. https://doi.org/10.3390/cimb44120403
Chicago/Turabian StyleDoneva-Basheva, Krastina I., Konstantin Gospodinov, Tanya Tacheva, Dimo Dimov, and Tatyana I. Vlaykova. 2022. "Role of Single Nucleotide Polymorphism L55M in the Paraoxonase 1 Gene as a Risk and Prognostic Factor in Acute Coronary Syndrome" Current Issues in Molecular Biology 44, no. 12: 5915-5932. https://doi.org/10.3390/cimb44120403
APA StyleDoneva-Basheva, K. I., Gospodinov, K., Tacheva, T., Dimov, D., & Vlaykova, T. I. (2022). Role of Single Nucleotide Polymorphism L55M in the Paraoxonase 1 Gene as a Risk and Prognostic Factor in Acute Coronary Syndrome. Current Issues in Molecular Biology, 44(12), 5915-5932. https://doi.org/10.3390/cimb44120403