
Pathological Evidence for Residual SARS-CoV-2 in the Micrometastatic Niche of a Patient with Ovarian Cancer


Abstract
1. Introduction
2. Materials and Methods
2.1. Antibodies
2.2. Immunohistochemistry
2.3. Transmission Electron Microscopy
2.4. Statistical Analysis
2.5. Institutional Review Board Statement and Consent to Participate
3. Case Report
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.-Y.; Desai, A.; de Lima Lopes, G., Jr.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef] [PubMed]
- Moris, D.; Tsilimigras, D.I.; Schizas, D. Cancer and COVID-19. Lancet 2020, 396, 1066. [Google Scholar] [CrossRef] [PubMed]
- Kudo, K.; Ichihara, E. COVID-19 Pneumonia. Gan Kagaku Ryoho 2020, 47, 1657–1661. [Google Scholar]
- Cesaro, S.; Giacchino, M.; Fioredda, F.; Barone, A.; Battisti, L.; Bezzio, S.; Frenos, S.; De Santis, R.; Livadiotti, S.; Marinello, S.; et al. Guidelines on vaccinations in paediatric haematology and oncology patients. Biomed. Res. Int. 2014, 2014, 707691. [Google Scholar] [CrossRef] [PubMed]
- Buske, C.; Dreyling, M.; Alvarez-Larrán, A.; Apperley, J.; Arcaini, L.; Besson, C.; Bullinger, L.; Corradini, P.; Della Porta, M.G.; Dimopoulos, M.; et al. Managing hematological cancer patients during the COVID-19 pandemic: An ESMO-EHA Interdisciplinary Expert Consensus. ESMO Open 2022, 7, 100403. [Google Scholar] [CrossRef] [PubMed]
- Zojer, N. SARS-CoV-2 vaccination in patients with solid tumors or hematological malignancies: Is the pandemic over for fully vaccinated patients? MEMO 2021, 14, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Goudsmit, A.; Cubilier, E.; Meert, A.-P.; Aftimos, P.; Stathopoulos, K.; Spilleboudt, C.; Loizidou, A. Factors associated with SARS-CoV-2 infection and outcome in patients with solid tumors or hematological malignancies: A single-center study. Support. Care Cancer 2021, 29, 6271–6278. [Google Scholar] [CrossRef] [PubMed]
- Shiozawa, Y.; Pedersen, E.A.; Havens, A.M.; Jung, Y.; Mishra, A.; Joseph, J.; Kim, J.K.; Patel, L.R.; Ying, C.; Ziegler, A.M.; et al. Human prostate cancer metastases target the hematopoietic stem cell niche to establish footholds in mouse bone marrow. J. Clin. Investig. 2011, 121, 1298–1312. [Google Scholar] [CrossRef] [PubMed]
- Malanchi, I.; Santamaria-Martínez, A.; Susanto, E.; Peng, H.; Lehr, H.A.; Delaloye, J.F.; Huelsken, J. Interactions between cancer stem cells and their niche govern metastatic colonization. Nature 2012, 481, 85–89. [Google Scholar] [CrossRef]
- Ombrato, L.; Nolan, E.; Kurelac, I.; Mavousian, A.; Bridgeman, V.L.; Heinze, I.; Chakravarty, P.; Horswell, S.; Gonzalez-Gualda, E.; Matacchione, G.; et al. Metastatic-niche labelling reveals parenchymal cells with stem features. Nature 2019, 572, 603–608. [Google Scholar] [CrossRef]
- Hayashi, T.; Sano, K.; Aburatani, H.; Yaegashi, N.; Konishi, I. Initialization of epithelial cells by tumor cells in a metastatic microenvironment. Oncogene 2020, 39, 2638–2640. [Google Scholar] [CrossRef] [PubMed]
- Salahudeen, A.A.; Choi, S.S.; Rustagi, A.; Zhu, J.; van Unen, V.; de la, O.S.M.; Flynn, R.A.; Margalef-Català, M.; Santos, A.J.M.; Ju, J.; et al. Progenitor identification and SARS-CoV-2 infection in human distal lung organoids. Nature 2020, 588, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Sano, K.; Konishi, I. Possibility of SARS-CoV-2 infection in metastatic microenvironment of cancer. Curr. Issues Mol. Biol. 2022, 44, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Ichikawa, M.; Konishi, I. Spontaneous myocarditis in mice predisposed to autoimmune disease: Including Vaccination-induced onset. Biomedicines 2022, 10, 1443. [Google Scholar] [CrossRef] [PubMed]
- Rotondo, J.C.; Martini, F.; Maritati, M.; Caselli, E.; Gallenga, C.E.; Guarino, M.; De Giorgio, R.; Mazziotta, C.; Tramarin, M.L.; Badiale, G.; et al. Advanced Molecular and Immunological Diagnostic Methods to Detect SARS-CoV-2 Infection. Microorganisms 2022, 10, 1193. [Google Scholar] [CrossRef]
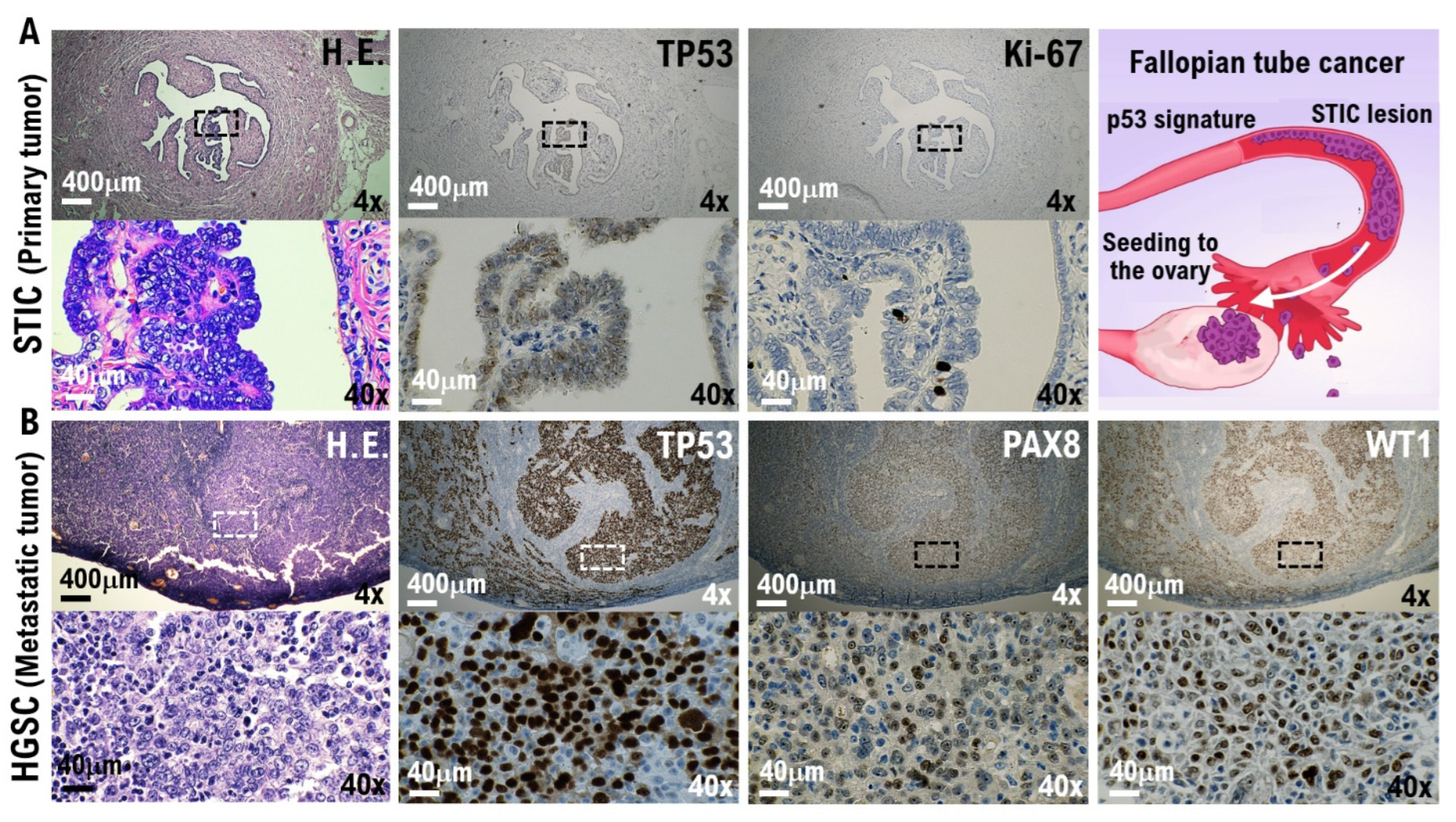
- Labidi-Galy, S.I.; Papp, E.; Hallberg, D.; Niknafs, N.; Adleff, V.; Noe, M.; Bhattacharya, R.; Novak, M.; Jones, S.; Phallen, J.; et al. High grade serous ovarian carcinomas originate in the fallopian tube. Nat. Commun. 2017, 8, 1093. [Google Scholar] [CrossRef] [PubMed]
- Ducie, J.; Dao, F.; Considine, M.; Olvera, N.; Shaw, P.A.; Kurman, R.J.; Shih, I.-M.; Soslow, R.A.; Cope, L.; Levine, D.A. Molecular analysis of high-grade serous ovarian carcinoma with and without associated serous tubal intra-epithelial carcinoma. Nat. Commun. 2017, 8, 990. [Google Scholar] [CrossRef] [PubMed]
- Konishi, I.; Abiko, K.; Hayashi, T.; Yamanoi, K.; Murakami, R.; Yamaguchi, K.; Hamanishi, J.; Baba, T.; Matsumura, N.; Mandai, M. Peritoneal dissemination of high-grade serous ovarian cancer: Pivotal roles of chromosomal instability and epigenetic dynamics. J. Gynecol. Oncol. 2022, 33, e83. [Google Scholar] [CrossRef] [PubMed]
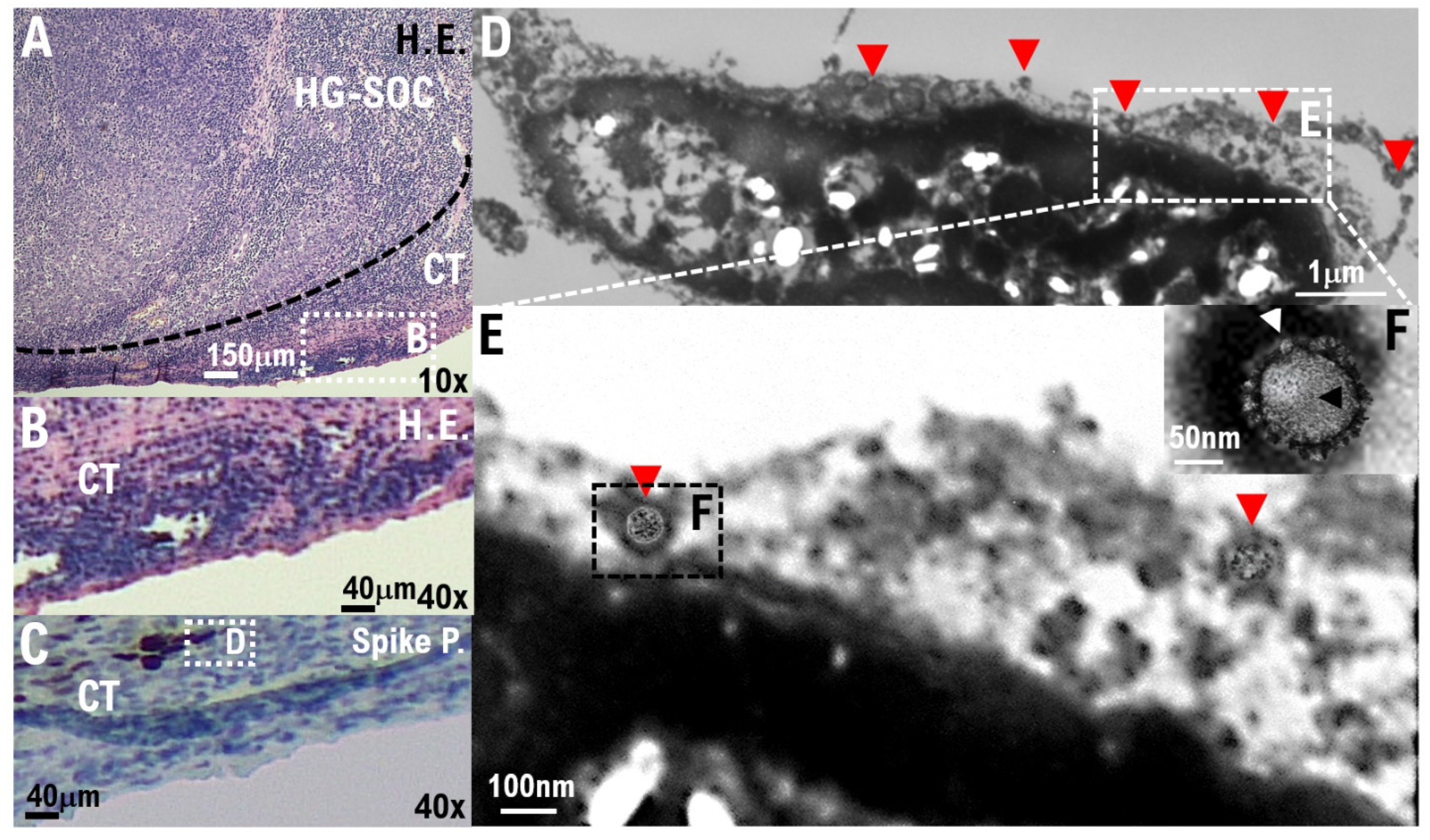
- Dittmayer, C.; Meinhardt, J.; Radbruch, H.; Radke, J.; Heppner, B.I.; Heppner, F.L.; Stenzel, W.; Holland, G.; Laue, M. Why misinterpretation of electron micrographs in SARS-CoV-2-infected tissue goes viral. Lancet 2020, 396, e64–e65. [Google Scholar] [CrossRef]
- Yao, X.H.; He, Z.C.; Li, T.Y.; Zhang, H.R.; Wang, Y.; Mou, H.; Guo, Q.; Yu, S.C.; Ding, Y.; Liu, X.; et al. Pathological evidence for residual SARS-CoV-2 in pulmonary tissues of a ready-for-discharge patient. Cell Res. 2020, 30, 541–543. [Google Scholar] [CrossRef] [PubMed]
- Torres, M.P.; Ponnusamy, M.P.; Lakshmanan, I.; Batra, S.K. Immunopathogenesis of ovarian cancer. Minerva Med. 2009, 100, 385–400. [Google Scholar]
- Yang, C.; Xia, B.R.; Zhang, Z.C.; Zhang, Y.J.; Lou, G.; Jin, W.L. Immunotherapy for Ovarian Cancer: Adjuvant, Combination, and Neoadjuvant. Front. Immunol. 2020, 11, 577869. [Google Scholar] [CrossRef]
- Santoiemma, P.P.; Powell, D.J., Jr. Tumor infiltrating lymphocytes in ovarian cancer. Cancer Biol. Ther. 2015, 16, 807–820. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; Aguilar-Company, J.; Ferrante, D.; Hanbury, G.; Bower, M.; Salazar, R.; Mirallas, O.; Sureda, A.; Plaja, A.; Cucurull, M.; et al. Outcomes of the SARS-CoV-2 omicron (B.1.1.529) variant outbreak among vaccinated and unvaccinated patients with cancer in Europe: Results from the retrospective, multicentre, OnCovid registry study. Lancet Oncol. 2022, 23, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Khan, Q.J.; Bivona, C.R.; Martin, G.A.; Zhang, J.; Liu, B.; He, J.; Li, K.H.; Nelson, M.; Williamson, S.; Doolittle, G.C.; et al. Evaluation of the Durability of the Immune Humoral Response to COVID-19 Vaccines in Patients with Cancer Undergoing Treatment or Who Received a Stem Cell Transplant. JAMA Oncol. 2022, 8, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; Tabernero, J.; Bower, M.; Scotti, L.; Patel, M.; Colomba, E.; Dolly, S.; Loizidou, A.; Chester, J.; Mukherjee, U.; et al. Prevalence and impact of COVID-19 sequelae on treatment and survival of patients with cancer who recovered from SARS-CoV-2 infection: Evidence from the OnCovid retrospective, multicentre registry study. Lancet Oncol. 2021, 22, 1669–1680. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient No. | Age Range | Age at Surgery (Years) | Histological Type | FIGO Stage | Grade | No. of Lung Metastatic Lesions | Pulmonary Metastatic Niche | Vital Status | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CD90* (%) | ACE2* (%) | ||||||||||
| 1 | 40s | 40–45 | HG serous | IVA | 3 | Single | 36.43 | 27.42 | Alive | ||
| 2 | 50s | 50–55 | HG serous | IVA | 3 | Single | 33.87 | 18.93 | Alive | ||
| 3 | 50s | 50–55 | HG serous | IVA | 3 | Multiple | 38.32 | 29.38 | Deceased | ||
| 4 | 40s | 45–50 | HG serous | IVB | 3 | Multiple | 32.67 | 28.05 | Alive | ||
| Patient no. | Age range | Age at surgery (years) | Histological type | FIGO stage | Grade | No. of metastatic lesions | Ovarian metastatic niche | Vital status | |||
| CD90* (%) | ACE2* (%) | ||||||||||
| 5 | 40s | 45–50 | HG serous | IIA | 2 | Single | 16.33 | 15.34 | Alive | ||
| Normal alveolar and bronchiolar areas. | |||||||||||
| Patient no. | Normal alveoli | Normal bronchioles | SARS-CoV-2a | COVID-19b | |||||||
| CD90* (%) | ACE2* (%) | CD90* (%) | ACE2* (%) | ||||||||
| 1 | 4.53 | 11.82 | 3.23 | 20.67 | Negative | Negative | |||||
| 2 | 3.91 | 12.57 | 3.18 | 21.46 | Negative | Negative | |||||
| 3 | 4.34 | 12.71 | 3.45 | 22.05 | Negative | Negative | |||||
| 4 | 4.08 | 13.43 | 2.98 | 21.92 | Negative | Negative | |||||
| 5c | NA | NA | NA | NA | Positive | Positive | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayashi, T.; Sano, K.; Yaegashi, N.; Konishi, I. Pathological Evidence for Residual SARS-CoV-2 in the Micrometastatic Niche of a Patient with Ovarian Cancer. Curr. Issues Mol. Biol. 2022, 44, 5879-5889. https://doi.org/10.3390/cimb44120400
Hayashi T, Sano K, Yaegashi N, Konishi I. Pathological Evidence for Residual SARS-CoV-2 in the Micrometastatic Niche of a Patient with Ovarian Cancer. Current Issues in Molecular Biology. 2022; 44(12):5879-5889. https://doi.org/10.3390/cimb44120400
Chicago/Turabian StyleHayashi, Takuma, Kenji Sano, Nobuo Yaegashi, and Ikuo Konishi. 2022. "Pathological Evidence for Residual SARS-CoV-2 in the Micrometastatic Niche of a Patient with Ovarian Cancer" Current Issues in Molecular Biology 44, no. 12: 5879-5889. https://doi.org/10.3390/cimb44120400
APA StyleHayashi, T., Sano, K., Yaegashi, N., & Konishi, I. (2022). Pathological Evidence for Residual SARS-CoV-2 in the Micrometastatic Niche of a Patient with Ovarian Cancer. Current Issues in Molecular Biology, 44(12), 5879-5889. https://doi.org/10.3390/cimb44120400