

Neuroprotective Effect of Methylene Blue in a Rat Model of Traumatic Optic Neuropathy
 , , , ,
, , , ,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
2.1. Surgery and Treatment Groups
2.2. Methylene Blue Restores Electroretinogram Patterns
2.2.1. Scotopic Full Field Electroretinography
2.2.2. Scotopic Oscillatory Potentials
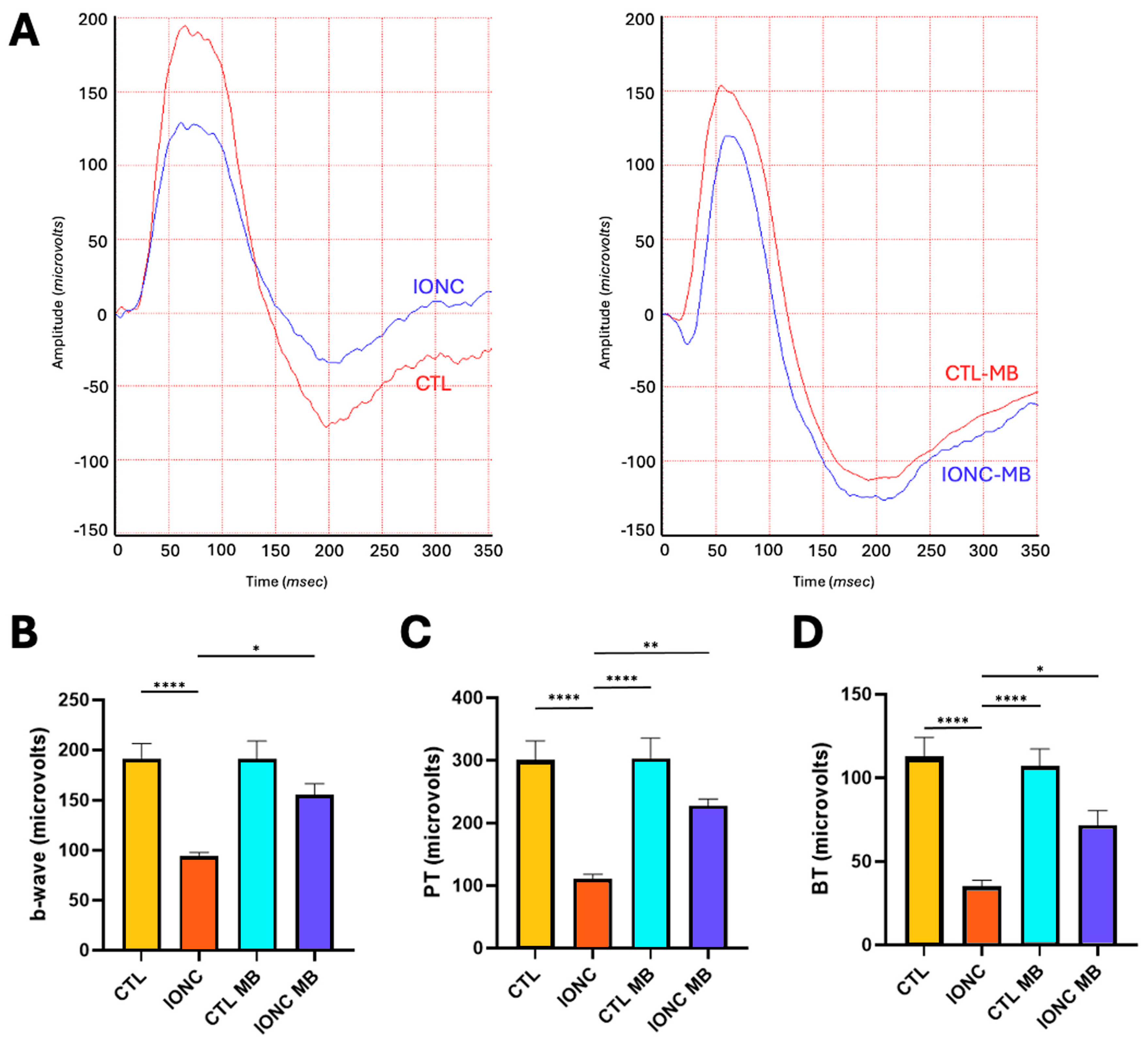
2.2.3. Photopic Full Field Electroretinography
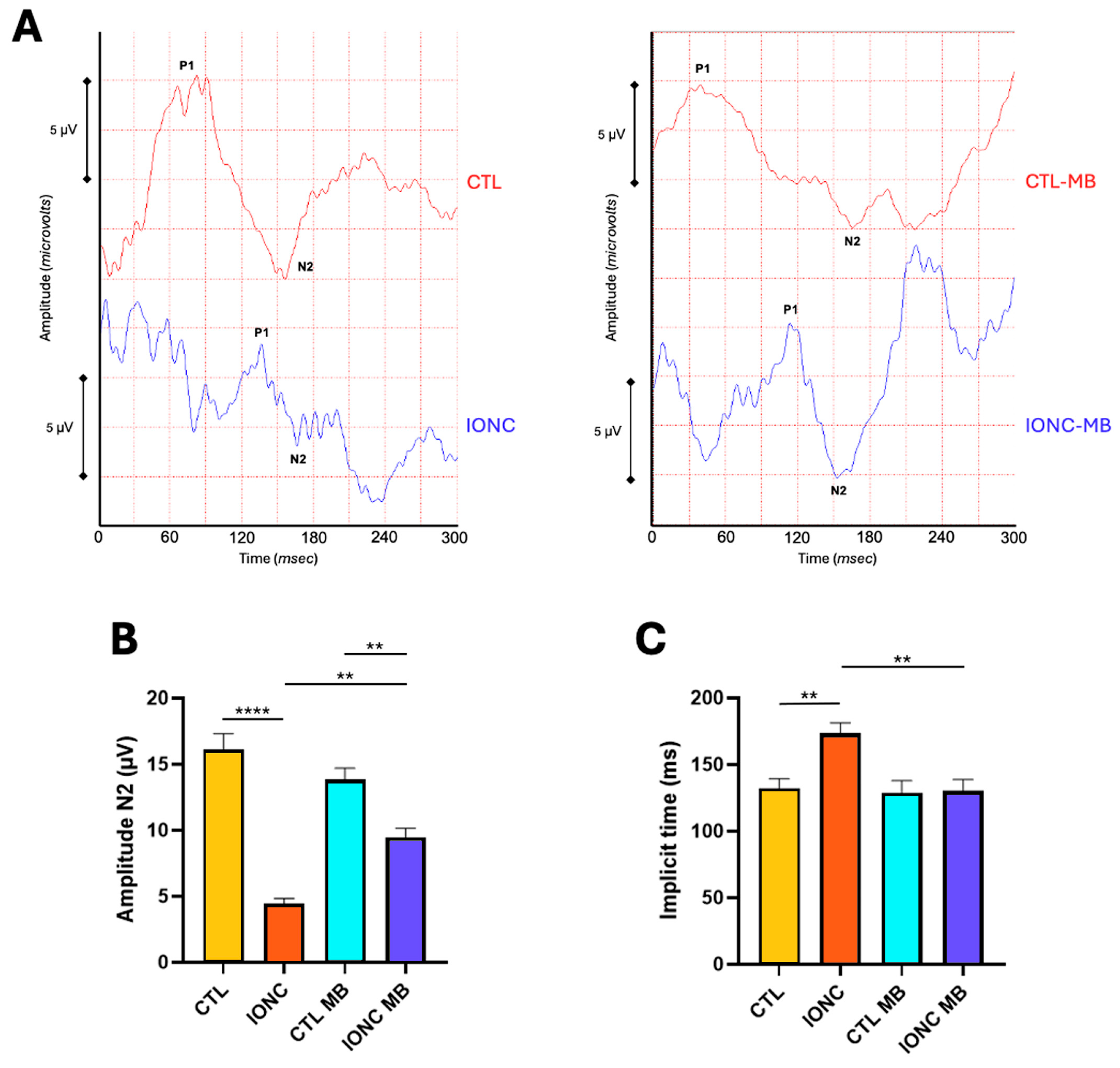
2.2.4. Pattern Electroretinography
2.3. Methylene Blue Prevents IONC-Induced Cell Death in the Ganglion Cell Layer
3. Discussion
4. Materials and Methods
4.1. Traumatic Neuropathy Model Through Intraorbital Optic Nerve Crush (IONC)
4.2. Scotopic Full-Field Electroretinography (scERG) and Scotopic Oscillatory Potentials (OP)
4.3. Photopic Full Field Electroretinography (phERG)
4.4. Pattern Electroretinography (PERG)
4.5. Histology and Morphological Evaluation
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| BDNF | Brain-derived neurotrophic factor |
| BT | Baseline-to-trough |
| cAMP | Cyclic adenosine monophosphate |
| CTL | Control |
| ERG | Electroretinogram |
| INL | Inner nuclear layer |
| IONC | Intraorbital nerve crush |
| GCL | Ganglion cell layer |
| MB | Methylene blue |
| NO | Nitric oxide |
| NOS | Nitric oxide synthase |
| ONL | Outer nuclear layer |
| OP | Oscillatory potentials |
| PBS | Phosphate buffered saline |
| PERG | Pattern electroretinography |
| phERG | Photopic electroretinography |
| PhNR | Photopic negative response |
| PT | Peak-to-trough |
| RGC | Retinal ganglion cells |
| scERG | Scotopic electroretinogram |
| TON | Traumatic optic neuropathy |
References
- Singman, E.L.; Daphalapurkar, N.; White, H.; Nguyen, T.D.; Panghat, L.; Chang, J.; McCulley, T. Indirect traumatic optic neuropathy. Mil. Med. Res. 2016, 3, 2. [Google Scholar] [CrossRef] [PubMed]
- Miller, N.R. Traumatic Optic Neuropathy. J. Neurol. Surg. Part B Skull Base 2021, 82, 107–115. [Google Scholar]
- Yu-Wai-Man, P. Traumatic optic neuropathy-Clinical features and management issues. Taiwan J. Ophthalmol. 2015, 5, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Sarkies, N. Traumatic optic neuropathy. Eye 2004, 18, 1122–1125. [Google Scholar] [CrossRef]
- Lee, V.; Ford, R.L.; Xing, W.; Bunce, C.; Foot, B. Surveillance of traumatic optic neuropathy in the UK. Eye 2010, 24, 240–250. [Google Scholar] [CrossRef]
- Ford, R.L.; Lee, V.; Xing, W.; Bunce, C. A 2-year prospective surveillance of pediatric traumatic optic neuropathy in the United Kingdom. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2012, 16, 413–417. [Google Scholar] [CrossRef]
- Cass, S.P. Ocular injuries in sports. Curr. Sports Med. Rep. 2012, 11, 11–15. [Google Scholar] [CrossRef]
- Matschke, J.; Herrmann, B.; Sperhake, J.; Korber, F.; Bajanowski, T.; Glatzel, M. Shaken baby syndrome: A common variant of non-accidental head injury in infants. Dtsch. Arztebl. Int. 2009, 106, 211–217. [Google Scholar]
- Blanch, R.J.; Joseph, I.J.; Cockerham, K. Traumatic optic neuropathy management: A systematic review. Eye 2024, 38, 2312–2318. [Google Scholar] [CrossRef]
- Phillips, B.N.; Chun, D.W.; Colyer, M. Closed globe macular injuries after blasts in combat. Retina 2013, 33, 371–379. [Google Scholar] [CrossRef]
- Goodrich, G.L.; Flyg, H.M.; Kirby, J.E.; Chang, C.Y.; Martinsen, G.L. Mechanisms of TBI and visual consequences in military and veteran populations. Optom. Vis. Sci. 2013, 90, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Selhorst, J.B.; Chen, Y. The optic nerve. Semin. Neurol. 2009, 29, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Wladis, E.J.; Aakalu, V.K.; Sobel, R.K.; McCulley, T.J.; Foster, J.A.; Tao, J.P.; Freitag, S.K.; Yen, M.T. Interventions for Indirect Traumatic Optic Neuropathy: A Report by the American Academy of Ophthalmology. Ophthalmology 2021, 128, 928–937. [Google Scholar] [CrossRef] [PubMed]
- Morgan-Warren, P.J.; Berry, M.; Ahmed, Z.; Scott, R.A.; Logan, A. Exploiting mTOR signaling: A novel translatable treatment strategy for traumatic optic neuropathy? Investig. Ophthalmol. Vis. Sci. 2013, 54, 6903–6916. [Google Scholar] [CrossRef]
- Mesentier-Louro, L.A.; Teixeira-Pinheiro, L.C.; Gubert, F.; Vasques, J.F.; Silva-Junior, A.J.; Chimeli-Ormonde, L.; Nascimento-Dos-Santos, G.; Mendez-Otero, R.; Santiago, M.F. Long-term neuronal survival, regeneration, and transient target reconnection after optic nerve crush and mesenchymal stem cell transplantation. Stem Cell Res. Ther. 2019, 10, 121. [Google Scholar] [CrossRef] [PubMed]
- Mysona, B.A.; Zhao, J.; Bollinger, K.E. Role of BDNF/TrkB pathway in the visual system: Therapeutic implications for glaucoma. Expert. Rev. Ophthalmol. 2017, 12, 69–81. [Google Scholar] [CrossRef]
- Nascimento-Dos-Santos, G.; Teixeira-Pinheiro, L.C.; da Silva-Junior, A.J.; Carvalho, L.R.P.; Mesentier-Louro, L.A.; Hauswirth, W.W.; Mendez-Otero, R.; Santiago, M.F.; Petrs-Silva, H. Effects of a combinatorial treatment with gene and cell therapy on retinal ganglion cell survival and axonal outgrowth after optic nerve injury. Gene Ther. 2020, 27, 27–39. [Google Scholar] [CrossRef]
- Liu, D.; Webber, H.C.; Bian, F.; Xu, Y.; Prakash, M.; Feng, X.; Yang, M.; Yang, H.; You, I.J.; Li, L.; et al. Optineurin-facilitated axonal mitochondria delivery promotes neuroprotection and axon regeneration. Nat. Commun. 2025, 16, 1789. [Google Scholar] [CrossRef]
- Lukomska, A.; Frost, M.P.; Theune, W.C.; Xing, J.; Gupta, M.; Trakhtenberg, E.F. Nfe2l3 promotes neuroprotection and long-distance axon regeneration after injury in vivo. Exp. Neurol. 2024, 375, 114741. [Google Scholar] [CrossRef]
- Li, Q.; Feng, P.; Lin, S.; Xu, Z.; Zhao, J.; Chen, Z.; Luo, Z.; Tao, Y.; Chen, S.; Wang, P. Crocetin confers neuroprotection and is anti-inflammatory in rats with induced glaucoma. Mol. Biol. Rep. 2023, 50, 1321–1331. [Google Scholar] [CrossRef]
- Mackiewicz, J.; Tomczak, J.; Lisek, M.; Sakowicz, A.; Guo, F.; Boczek, T. NFATc4 Knockout Promotes Neuroprotection and Retinal Ganglion Cell Regeneration After Optic Nerve Injury. Mol. Neurobiol. 2024, 61, 9383–9401. [Google Scholar] [CrossRef] [PubMed]
- Namekata, K.; Noro, T.; Nishijima, E.; Sotozono, A.; Guo, X.; Harada, C.; Shinozaki, Y.; Mitamura, Y.; Nakano, T.; Harada, T. Drug combination of topical ripasudil and brimonidine enhances neuroprotection in a mouse model of optic nerve injury. J. Pharmacol. Sci. 2024, 154, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Rey-Funes, M.; Larrayoz, I.M.; Contartese, D.S.; Solino, M.; Sarotto, A.; Bustelo, M.; Bruno, M.; Dorfman, V.B.; Loidl, C.F.; Martinez, A. Hypothermia Prevents Retinal Damage Generated by Optic Nerve Trauma in the Rat. Sci. Rep. 2017, 7, 6966. [Google Scholar] [CrossRef]
- Contartese, D.S.; Rey-Funes, M.; Pelaez, R.; Solino, M.; Fernandez, J.C.; Nakamura, R.; Ciranna, N.S.; Sarotto, A.; Dorfman, V.B.; Lopez-Costa, J.J.; et al. A hypothermia mimetic molecule (zr17-2) reduces ganglion cell death and electroretinogram distortion in a rat model of intraorbital optic nerve crush (IONC). Front. Pharmacol. 2023, 14, 1112318. [Google Scholar] [CrossRef] [PubMed]
- Atamna, H.; Nguyen, A.; Schultz, C.; Boyle, K.; Newberry, J.; Kato, H.; Ames, B.N. Methylene blue delays cellular senescence and enhances key mitochondrial biochemical pathways. FASEB J. 2008, 22, 703–712. [Google Scholar] [CrossRef]
- Mayer, B.; Brunner, F.; Schmidt, K. Inhibition of nitric oxide synthesis by methylene blue. Biochem. Pharmacol. 1993, 45, 367–374. [Google Scholar] [CrossRef]
- Volke, V.; Wegener, G.; Vasar, E.; Rosenberg, R. Methylene blue inhibits hippocampal nitric oxide synthase activity in vivo. Brain Res. 1999, 826, 303–305. [Google Scholar] [CrossRef]
- Fernandez, J.C.; Pelaez, R.; Rey-Funes, M.; Solino, M.; Contartese, D.S.; Dorfman, V.B.; Lopez-Costa, J.J.; Larrayoz, I.M.; Loidl, C.F.; Martinez, A. Methylene Blue Prevents Retinal Damage Caused by Perinatal Asphyxia in the Rat. Front. Cell. Neurosci. 2020, 14, 157. [Google Scholar] [CrossRef]
- Rey-Funes, M.; Larrayoz, I.M.; Fernandez, J.C.; Contartese, D.S.; Rolon, F.; Inserra, P.I.; Martinez-Murillo, R.; Lopez-Costa, J.J.; Dorfman, V.B.; Martinez, A.; et al. Methylene blue prevents retinal damage in an experimental model of ischemic proliferative retinopathy. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2016, 310, R1011–R1019. [Google Scholar] [CrossRef]
- Nakamura, R.; Ciranna, N.S.; Fernandez, J.C.; Pelaez, R.; Perez-Sala, A.; Bobadilla, M.; Lopez-Costa, J.J.; Loidl, C.F.; Martinez, A.; Rey-Funes, M. Methylene Blue Reduces Electroretinogram Distortion and Ganglion Cell Death in a Rat Model of Glaucoma. Biomedicines 2024, 12, 1983. [Google Scholar] [CrossRef]
- Hosseini Siyanaki, M.R.A.M.; Lucke-Wold, B. Traumatic optic neuropathy: Update on management. Encyclopedia 2023, 3, 88–101. [Google Scholar] [CrossRef]
- Klocker, N.; Cellerino, A.; Bahr, M. Free radical scavenging and inhibition of nitric oxide synthase potentiates the neurotrophic effects of brain-derived neurotrophic factor on axotomized retinal ganglion cells In vivo. J. Neurosci. 1998, 18, 1038–1046. [Google Scholar] [CrossRef]
- Osborne, N.N.; Chidlow, G.; Layton, C.J.; Wood, J.P.; Casson, R.J.; Melena, J. Optic nerve and neuroprotection strategies. Eye 2004, 18, 1075–1084. [Google Scholar] [CrossRef] [PubMed]
- Hetzer, S.M.; Shalosky, E.M.; Torrens, J.N.; Evanson, N.K. Chronic Histological Outcomes of Indirect Traumatic Optic Neuropathy in Adolescent Mice: Persistent Degeneration and Temporally Regulated Glial Responses. Cells 2021, 10, 3343. [Google Scholar] [CrossRef]
- Au, N.P.B.; Ma, C.H.E. Neuroinflammation, Microglia and Implications for Retinal Ganglion Cell Survival and Axon Regeneration in Traumatic Optic Neuropathy. Front. Immunol. 2022, 13, 860070. [Google Scholar] [CrossRef] [PubMed]
- Burke, E.G.; Cansler, S.M.; Evanson, N.K. Indirect traumatic optic neuropathy: Modeling optic nerve injury in the context of closed head trauma. Neural Regen. Res. 2019, 14, 593–594. [Google Scholar]
- Cansler, S.M.; Evanson, N.K. Connecting endoplasmic reticulum and oxidative stress to retinal degeneration, TBI, and traumatic optic neuropathy. J. Neurosci. Res. 2020, 98, 571–574. [Google Scholar] [CrossRef]
- Hetzer, S.M.G.-C.F.; Day, D.; Bedolla, A.; Evanson, N.K. Traumatic Optic Neuropathy Is Associated with Visual Impairment, Neurodegeneration, and Endoplasmic Reticulum Stress in Adolescent Mice. Cells 2021, 10, 996. [Google Scholar] [CrossRef]
- You, Y.; Gupta, V.K.; Graham, S.L.; Klistorner, A. Anterograde degeneration along the visual pathway after optic nerve injury. PLoS ONE 2012, 7, e52061. [Google Scholar] [CrossRef]
- Hendrickson, A.; Warner, C.E.; Possin, D.; Huang, J.; Kwan, W.C.; Bourne, J.A. Retrograde transneuronal degeneration in the retina and lateral geniculate nucleus of the V1-lesioned marmoset monkey. Brain Struct. Funct. 2015, 220, 351–360. [Google Scholar] [CrossRef]
- Sung, J.Y.; Lee, H.M.; Lee, S.B.; Kim, K.N.; Lee, Y.H. Progression of optic atrophy in traumatic optic neuropathy: Retrograde neuronal degeneration in humans. Neurol. Sci. 2022, 43, 1351–1358. [Google Scholar] [CrossRef] [PubMed]
- Fujitani, T.; Inoue, K.; Takahashi, T.; Ikushima, K.; Asai, T. Indirect traumatic optic neuropathy--visual outcome of operative and nonoperative cases. Jpn. J. Ophthalmol. 1986, 30, 125–134. [Google Scholar] [PubMed]
- Yu-Wai-Man, P.; Griffiths, P.G. Steroids for traumatic optic neuropathy. Cochrane Database Syst. Rev. 2013, 2013, CD006032. [Google Scholar] [CrossRef]
- Kashkouli, M.B.; Yousefi, S.; Nojomi, M.; Sanjari, M.S.; Pakdel, F.; Entezari, M.; Etezad-Razavi, M.; Razeghinejad, M.R.; Esmaeli, M.; Shafiee, M.; et al. Traumatic optic neuropathy treatment trial (TONTT): Open label, phase 3, multicenter, semi-experimental trial. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 209–218. [Google Scholar] [CrossRef]
- Shirley Ding, S.L.; Leow, S.N.; Munisvaradass, R.; Koh, E.H.; Bastion, M.L.; Then, K.Y.; Kumar, S.; Mok, P.L. Revisiting the role of erythropoietin for treatment of ocular disorders. Eye 2016, 30, 1293–1309. [Google Scholar] [CrossRef]
- Kashkouli, M.B.; Pakdel, F.; Sanjari, M.S.; Haghighi, A.; Nojomi, M.; Homaee, M.H.; Heirati, A. Erythropoietin: A novel treatment for traumatic optic neuropathy-a pilot study. Graefes Arch. Clin. Exp. Ophthalmol. 2011, 249, 731–736. [Google Scholar] [CrossRef]
- Entezari, M.; Esmaeili, M.; Yaseri, M. A pilot study of the effect of intravenous erythropoetin on improvement of visual function in patients with recent indirect traumatic optic neuropathy. Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 1309–1313. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Sun, B.; Yu, Z.; An, J.; Liu, Q.; Ren, T. High dose erythropoietin promotes functional recovery of rats following facial nerve crush. J. Clin. Neurosci. 2009, 16, 554–556. [Google Scholar] [CrossRef]
- Heng, K.; Young, B.K.; Li, B.; Nies, A.D.; Xia, X.; Wen, R.R.; Dalal, R.; Bramblett, G.T.; Holt, A.W.; Cleland, J.M.; et al. BDNF and cAMP are neuroprotective in a porcine model of traumatic optic neuropathy. JCI Insight 2024, 9, e172935. [Google Scholar] [CrossRef]
- Henrich-Noack, P.; Voigt, N.; Prilloff, S.; Fedorov, A.; Sabel, B.A. Transcorneal electrical stimulation alters morphology and survival of retinal ganglion cells after optic nerve damage. Neurosci. Lett. 2013, 543, 1–6. [Google Scholar] [CrossRef]
- Kurimoto, T.; Oono, S.; Oku, H.; Tagami, Y.; Kashimoto, R.; Takata, M.; Okamoto, N.; Ikeda, T.; Mimura, O. Transcorneal electrical stimulation increases chorioretinal blood flow in normal human subjects. Clin. Ophthalmol. 2010, 4, 1441–1446. [Google Scholar] [CrossRef]
- Miyake, K.; Yoshida, M.; Inoue, Y.; Hata, Y. Neuroprotective effect of transcorneal electrical stimulation on the acute phase of optic nerve injury. Investig. Ophthalmol. Vis. Sci. 2007, 48, 2356–2361. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.O.; Lewander, W.J.; Woolf, A.D. Methemoglobinemia: Etiology, pharmacology, and clinical management. Ann. Emerg. Med. 1999, 34, 646–656. [Google Scholar] [CrossRef]
- Sparicio, D.; Landoni, G.; Zangrillo, A. Angiotensin-converting enzyme inhibitors predispose to hypotension refractory to norepinephrine but responsive to methylene blue. J. Thorac. Cardiovasc. Surg. 2004, 127, 608. [Google Scholar] [CrossRef]
- Landoni, G.; Pasin, L.; Di Prima, A.L.; Dossi, R.; Taddeo, D.; Zangrillo, A. Methylene blue: Between scylla (meta-analysis) and charybdis (propensity). J. Cardiothorac. Vasc. Anesth. 2014, 28, e12–e13. [Google Scholar] [CrossRef]
- Gokoffski, K.K.; Peng, M.; Alas, B.; Lam, P. Neuro-protection and neuro-regeneration of the optic nerve: Recent advances and future directions. Curr. Opin. Neurol. 2020, 33, 93–105. [Google Scholar] [CrossRef]
- Aslan, M.; Cort, A.; Yucel, I. Oxidative and nitrative stress markers in glaucoma. Free Radic. Biol. Med. 2008, 45, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.S.F.; Geisert, E.E. Commonalities of optic nerve injury and glaucoma-induced neurodegeneration: Insights from transcriptome-wide studies. Exp. Eye Res. 2021, 207, 108571. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, Y.; Hunt, D.M.; Carvalho, L.S. The origins of the full-field flash electroretinogram b-wave. Front. Mol. Neurosci. 2023, 16, 1153934. [Google Scholar] [CrossRef] [PubMed]
- Rey-Funes, M.; Contartese, D.S.; Pelaez, R.; Garcia-Sanmartin, J.; Narro-Iniguez, J.; Solino, M.; Fernandez, J.C.; Sarotto, A.; Ciranna, N.S.; Lopez-Costa, J.J.; et al. Hypothermic Shock Applied After Perinatal Asphyxia Prevents Retinal Damage in Rats. Front. Pharmacol. 2021, 12, 651599. [Google Scholar] [CrossRef] [PubMed]
- Rey-Funes, M.; Fernandez, J.C.; Pelaez, R.; Solino, M.; Contartese, D.S.; Ciranna, N.S.; Nakamura, R.; Sarotto, A.; Dorfman, V.B.; Zapico, J.M.; et al. A hypothermia mimetic molecule (zr17-2) reduces ganglion cell death, gliosis, and electroretinogram distortion in male rats subjected to perinatal asphyxia. Front. Pharmacol. 2023, 14, 1252184. [Google Scholar] [CrossRef]
- Wachtmeister, L. Oscillatory potentials in the retina: What do they reveal. Prog. Retin. Eye Res. 1998, 17, 485–521. [Google Scholar] [CrossRef]
- Liao, F.L.H.; Milla-Navarro, S.; Villa, P.; Germain, F. Origin of Retinal Oscillatory Potentials in the Mouse, a Tool to Specifically Locate Retinal Damage. Int. J. Mol. Sci. 2023, 24, 3126. [Google Scholar] [CrossRef]
- Luu, C.D.; Szental, J.A.; Lee, S.Y.; Lavanya, R.; Wong, T.Y. Correlation between retinal oscillatory potentials and retinal vascular caliber in type 2 diabetes. Investig. Ophthalmol. Vis. Sci. 2010, 51, 482–486. [Google Scholar] [CrossRef]
- Speros, P.; Price, J. Oscillatory potentials. History, techniques and potential use in the evaluation of disturbances of retinal circulation. Surv. Ophthalmol. 1981, 25, 237–252. [Google Scholar] [CrossRef]
- Frishman, L.; Sustar, M.; Kremers, J.; McAnany, J.J.; Sarossy, M.; Tzekov, R.; Viswanathan, S. ISCEV extended protocol for the photopic negative response (PhNR) of the full-field electroretinogram. Doc. Ophthalmol. 2018, 136, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Prencipe, M.; Perossini, T.; Brancoli, G.; Perossini, M. The photopic negative response (PhNR): Measurement approaches and utility in glaucoma. Int. Ophthalmol. 2020, 40, 3565–3576. [Google Scholar] [CrossRef] [PubMed]
- Jafarzadehpour, E.; Radinmehr, F.; Pakravan, M.; Mirzajani, A.; Yazdani, S. Pattern electroretinography in glaucoma suspects and early primary open angle glaucoma. J. Ophthalmic Vis. Res. 2013, 8, 199–206. [Google Scholar] [PubMed]
- Holder, G.E. Pattern electroretinography (PERG) and an integrated approach to visual pathway diagnosis. Prog. Retin. Eye Res. 2001, 20, 531–561. [Google Scholar] [CrossRef]
- World Health Organization. WHO Model List of Essential Medicines. 2017. Available online: http://apps.who.int/iris/bitstream/handle/10665/273826/EML-20-eng.pdf (accessed on 15 April 2025).
- Bewick, J.; Pfleiderer, A. The value and role of low dose methylene blue in the surgical management of hyperparathyroidism. Ann. R. Coll. Surg. Engl. 2014, 96, 526–529. [Google Scholar] [CrossRef]
- Rodrigo, J.; Fernandez, A.P.; Serrano, J.; Peinado, M.A.; Martinez, A. The role of free radicals in cerebral hypoxia and ischemia. Free Radic. Biol. Med. 2005, 39, 26–50. [Google Scholar] [CrossRef] [PubMed]
- Parrilla-Reverter, G.; Agudo, M.; Nadal-Nicolas, F.; Alarcon-Martinez, L.; Jimenez-Lopez, M.; Salinas-Navarro, M.; Sobrado-Calvo, P.; Bernal-Garro, J.M.; Villegas-Perez, M.P.; Vidal-Sanz, M. Time-course of the retinal nerve fibre layer degeneration after complete intra-orbital optic nerve transection or crush: A comparative study. Vis. Res. 2009, 49, 2808–2825. [Google Scholar] [CrossRef]
- Leyh, R.G.; Kofidis, T.; Struber, M.; Fischer, S.; Knobloch, K.; Wachsmann, B.; Hagl, C.; Simon, A.R.; Haverich, A. Methylene blue: The drug of choice for catecholamine-refractory vasoplegia after cardiopulmonary bypass? J. Thorac. Cardiovasc. Surg. 2003, 125, 1426–1431. [Google Scholar] [CrossRef] [PubMed]
- Shanmugam, G. Vasoplegic syndrome--the role of methylene blue. Eur. J. Cardiothorac. Surg. 2005, 28, 705–710. [Google Scholar] [CrossRef]
- Ginimuge, P.R.; Jyothi, S.D. Methylene blue: Revisited. J. Anaesthesiol. Clin. Pharmacol. 2010, 26, 517–520. [Google Scholar] [CrossRef]
- Peter, C.; Hongwan, D.; Kupfer, A.; Lauterburg, B.H. Pharmacokinetics and organ distribution of intravenous and oral methylene blue. Eur. J. Clin. Pharmacol. 2000, 56, 247–250. [Google Scholar] [CrossRef]
- Roth, S.; Dreixler, J.C.; Mathew, B.; Balyasnikova, I.; Mann, J.R.; Boddapati, V.; Xue, L.; Lesniak, M.S. Hypoxic-Preconditioned Bone Marrow Stem Cell Medium Significantly Improves Outcome After Retinal Ischemia in Rats. Investig. Ophthalmol. Vis. Sci. 2016, 57, 3522–3532. [Google Scholar] [CrossRef]
- Lani, R.; Dias, M.S.; Abreu, C.A.; Araujo, V.G.; Goncalo, T.; Nascimento-Dos-Santos, G.; Dantas, A.M.; Allodi, S.; Fiorani, M.; Petrs-Silva, H.; et al. A subacute model of glaucoma based on limbal plexus cautery in pigmented rats. Sci. Rep. 2019, 9, 16286. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shlomo, G.; Bakalash, S.; Lambrou, G.N.; Latour, E.; Dawson, W.W.; Schwartz, M.; Ofri, R. Pattern electroretinography in a rat model of ocular hypertension: Functional evidence for early detection of inner retinal damage. Exp. Eye Res. 2005, 81, 340–349. [Google Scholar] [CrossRef]
- Clark, M.E.; Kraft, T.W. Measuring rodent electroretinograms to assess retinal function. Methods Mol. Biol. 2012, 884, 265–276. [Google Scholar]
- Sasovetz, D. Ketamine hydrochloride: An effective general anesthetic for use in electroretinography. Ann. Ophthalmol. 1978, 10, 1510–1514. [Google Scholar] [PubMed]
- Gellrich, M.M.; Gellrich, N.C. Quantitative relations in the retinal ganglion cell layer of the rat: Neurons, glia and capillaries before and after optic nerve section. Graefes Arch. Clin. Exp. Ophthalmol. 1996, 234, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Xu, J.; Hauswirth, W.W.; DeVries, S.H. Genetically targeted binary labeling of retinal neurons. J. Neurosci. 2014, 34, 7845–7861. [Google Scholar] [CrossRef] [PubMed]
- Kolb, H.; Nelson, R.; Mariani, A. Amacrine cells, bipolar cells and ganglion cells of the cat retina: A Golgi study. Vis. Res. 1981, 21, 1081–1114. [Google Scholar] [CrossRef]
- Perry, V.H. Evidence for an amacrine cell system in the ganglion cell layer of the rat retina. Neuroscience 1981, 6, 931–944. [Google Scholar] [CrossRef]
- Hayes, B.P. Cell populations of the ganglion cell layer: Displaced amacrine and matching amacrine cells in the pigeon retina. Exp. Brain Res. 1984, 56, 565–573. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciranna, N.S.; Nakamura, R.; Peláez, R.; Pérez-Sala, Á.; Sarrión, P.; Fernández, J.C.; Paganelli, A.; Aranalde, A.P.; Ruiz, U.P.; López-Costa, J.J.; et al. Neuroprotective Effect of Methylene Blue in a Rat Model of Traumatic Optic Neuropathy. Pharmaceuticals 2025, 18, 920. https://doi.org/10.3390/ph18060920
Ciranna NS, Nakamura R, Peláez R, Pérez-Sala Á, Sarrión P, Fernández JC, Paganelli A, Aranalde AP, Ruiz UP, López-Costa JJ, et al. Neuroprotective Effect of Methylene Blue in a Rat Model of Traumatic Optic Neuropathy. Pharmaceuticals. 2025; 18(6):920. https://doi.org/10.3390/ph18060920
Chicago/Turabian StyleCiranna, Nicolás S., Ronan Nakamura, Rafael Peláez, Álvaro Pérez-Sala, Patricia Sarrión, Juan C. Fernández, Alejandra Paganelli, Agustín P. Aranalde, Ulises P. Ruiz, Juan J. López-Costa, and et al. 2025. "Neuroprotective Effect of Methylene Blue in a Rat Model of Traumatic Optic Neuropathy" Pharmaceuticals 18, no. 6: 920. https://doi.org/10.3390/ph18060920
APA StyleCiranna, N. S., Nakamura, R., Peláez, R., Pérez-Sala, Á., Sarrión, P., Fernández, J. C., Paganelli, A., Aranalde, A. P., Ruiz, U. P., López-Costa, J. J., Loidl, C. F., Martínez, A., & Rey-Funes, M. (2025). Neuroprotective Effect of Methylene Blue in a Rat Model of Traumatic Optic Neuropathy. Pharmaceuticals, 18(6), 920. https://doi.org/10.3390/ph18060920