
PLGA Implants for Controlled Drug Delivery and Regenerative Medicine: Advances, Challenges, and Clinical Potential


Abstract
1. Introduction
2. Essential Materials for PLGA Implant Design
2.1. PLGA as a Base Polymer
2.2. Therapeutic Agents Delivered via PLGA
2.3. Additives, Nanocarriers, and Structural Enhancements
2.4. Solvents and Processing Aids
3. Key Properties of PLGA Implants for Medical Applications
3.1. Controlled Release Kinetics
3.2. Porosity and Morphology
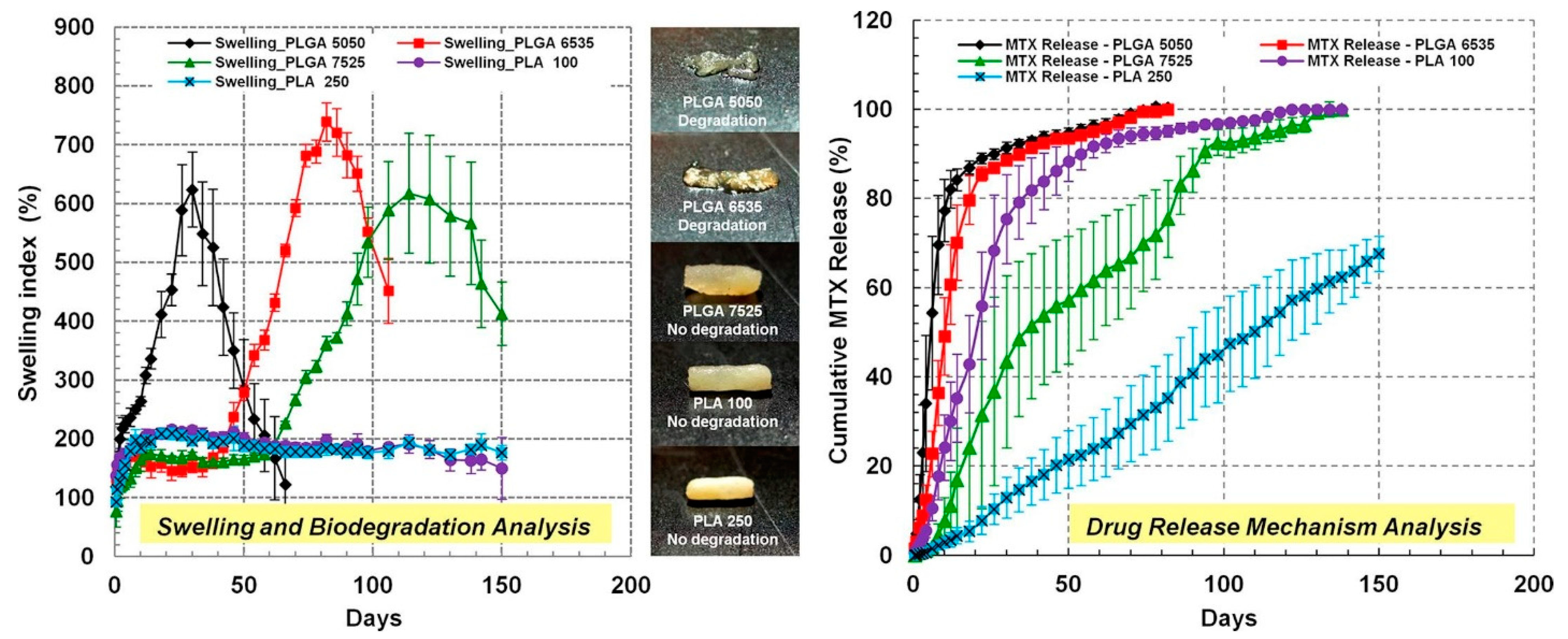
3.3. Swelling and Degradation Behavior
3.4. Thermal and Mechanical Stability
3.5. Biocompatibility and Reduced Inflammation
3.6. Multifunctionality and Enhanced Therapeutic Outcomes
4. Fabrication Techniques for Tailored PLGA Implants
4.1. Solvent-Based Fabrication Techniques
4.2. Hot Melt Extrusion (HME) for Controlled Release
4.3. In Situ Forming and Injectable Implants
4.4. Advanced 3D Printing Techniques
4.5. Microspheres, Nanoparticles, and Scaffold Fabrication
4.6. Surface Engineering and Hybrid Systems
4.7. Real-Time Monitoring and Structural Optimization
5. Testing and Validation of PLGA Implants
5.1. Drug Release and Kinetics
5.2. Material Properties and Fabrication
5.3. Degradation and Stability Studies
5.4. Biocompatibility and Toxicity
5.5. Application-Specific Evaluations and Therapeutic Performance
5.6. Imaging and Monitoring Techniques
5.7. Statistical and Computational Approaches
6. Tailored Therapeutic Effects of PLGA Implants
6.1. Exogenous Stimuli
6.2. Endogenous Stimuli
7. Applications and Benefits of PLGA-Based Implants
7.1. Sustained and Controlled Drug Release
7.2. Localized and Minimally Invasive Drug Delivery
7.3. Mitigation of Burst Release and Drug Stability
7.4. Advances in Regenerative Medicine
7.5. Specialized Applications
7.6. Enhancing Biocompatibility and Safety
8. Customization of Implants for Individual Patients
8.1. Personalized Medicine Factors: Age, Gender, Health, and Defect Characteristics
8.2. Biomimetic Design: Scaffold Rigidity, Pore Size, and Implant Shape
8.3. Biomechanical and Environmental Influences on Custom Regeneration
8.4. Advanced Technologies for Personalized PLGA Implants
8.5. Integration of Functionalized Nanoparticles for Patient-Specific Needs
9. Challenges in the Development of PLGA Implants
9.1. Challenges in Drug Release Consistency and Predictability
9.2. Manufacturing Complexity and Cost Barriers
9.3. Limitations in Bone Regeneration and Tissue Engineering
9.4. Inflammatory Reactions and Biocompatibility Issues
9.5. Structural and Mechanical Limitations of PLGA Implants
10. Opportunities and Future Directions in PLGA Implant Research
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ayoub, M.M.; Jasti, B.; Elantouny, N.G.; Elnahas, H.; Ghazy, F.E. Comparative Study of PLGA in-situ Implant and Nanoparticle Formulations of Entecavir; in-vitro and in-vivo evaluation. J. Drug Deliv. Sci. Technol. 2020, 56, 101585. [Google Scholar] [CrossRef]
- Ulianova, Y.; Ermolenko, Y.; Tkachenko, S.; Trukhan, V.; Morozov, A.; Gelperina, S. Tuning the release rate of rilpivirine from PLGA-based in situ forming implants. Polym. Bull. 2022, 80, 11401–11420. [Google Scholar] [CrossRef]
- Wang, F.; Lee, T.; Wang, C.H. PEG modulated release of etanidazole from implantable PLGA/PDLA discs. Biomaterials 2002, 23, 3555–3566. [Google Scholar] [CrossRef] [PubMed]
- Bassand, C.; Benabed, L.; Verin, J.; Danede, F.; Lefol, L.A.; Willart, J.F.; Siepmann, F.; Siepmann, J. Hot melt extruded PLGA implants loaded with ibuprofen: How heat exposure alters the physical drug state. J. Drug. Deliv. Sci. Technol. 2022, 73, 103432. [Google Scholar] [CrossRef]
- Solorio, L.; Olear, A.M.; Hamilton, J.I.; Patel, R.B.; Beiswenger, A.C.; Wallace, J.E.; Zhou, H.; Exner, A.A. Noninvasive characterization of the effect of varying PLGA molecular weight blends on in situ forming implant behavior using ultrasound imaging. Theranostics 2012, 2, 1064–1077. [Google Scholar] [CrossRef]
- Amini-Fazl, M.S. Biodegradation study of PLGA as an injectable in situ depot-forming implant for controlled release of paclitaxel. Polym. Bull. 2021, 79, 2763–2776. [Google Scholar] [CrossRef]
- Wang, X.; Wang, L.; Qi, F.; Zhao, J. The effect of a single injection of uniform-sized insulin-loaded PLGA microspheres on peri-implant bone formation. RSC Adv. 2018, 8, 40417–40425. [Google Scholar] [CrossRef]
- Bassand, C.; Freitag, J.; Benabed, L.; Verin, J.; Siepmann, F.; Siepmann, J. PLGA implants for controlled drug release: Impact of the diameter. Eur. J. Pharm. Biopharm. 2022, 177, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Shafiee, K.; Bazraei, S.; Mashak, A.; Mobedi, H. The Impact of Temperature on the Formation, Release Mechanism, and Degradation of PLGA-based In-Situ Forming Implants. J. Polym. Environ. 2024, 32, 3591–3608. [Google Scholar] [CrossRef]
- Hamoudi-Ben Yelles, M.C.; Tran Tan, V.; Danede, F.; Willart, J.F.; Siepmann, J. PLGA implants: How Poloxamer/PEO addition slows down or accelerates polymer degradation and drug release. J. Control. Release 2017, 253, 19–29. [Google Scholar] [CrossRef]
- Duque, L.; Korber, M.; Bodmeier, R. Improving release completeness from PLGA-based implants for the acid-labile model protein ovalbumin. Int. J. Pharm. 2018, 538, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, M.; Mobedi, H.; Behnamghader, A. In situ-forming PLGA implants loaded with leuprolide acetate/β-cyclodextrin complexes: Mathematical modelling and degradation. J. Microencapsul. 2016, 33, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Ranganath, S.H.; Kee, I.; Krantz, W.B.; Chow, P.K.; Wang, C.H. Hydrogel matrix entrapping PLGA-paclitaxel microspheres: Drug delivery with near zero-order release and implantability advantages for malignant brain tumour chemotherapy. Pharm. Res. 2009, 26, 2101–2114. [Google Scholar] [CrossRef] [PubMed]
- Thorfve, A.; Bergstrand, A.; Ekstrom, K.; Lindahl, A.; Thomsen, P.; Larsson, A.; Tengvall, P. Gene expression profiling of peri-implant healing of PLGA-Li+ implants suggests an activated Wnt signaling pathway in vivo. PLoS ONE 2014, 9, e102597. [Google Scholar] [CrossRef]
- Ibrahim, T.M.; El-Megrab, N.A.; El-Nahas, H.M. An overview of PLGA in-situ forming implants based on solvent exchange technique: Effect of formulation components and characterization. Pharm. Dev. Technol. 2021, 26, 709–728. [Google Scholar] [CrossRef]
- Saraf, I.; Kushwah, V.; Alva, C.; Koutsamanis, I.; Rattenberger, J.; Schroettner, H.; Mayrhofer, C.; Modhave, D.; Braun, M.; Werner, B.; et al. Influence of PLGA End Groups on the Release Profile of Dexamethasone from Ocular Implants. Mol. Pharm. 2023, 20, 1307–1322. [Google Scholar] [CrossRef]
- Bassand, C.; Benabed, L.; Charlon, S.; Verin, J.; Freitag, J.; Siepmann, F.; Soulestin, J.; Siepmann, J. 3D printed PLGA implants: APF DDM vs. FDM. J. Control. Release 2023, 353, 864–874. [Google Scholar] [CrossRef]
- Schadlich, A.; Kempe, S.; Mader, K. Non-invasive in vivo characterization of microclimate pH inside in situ forming PLGA implants using multispectral fluorescence imaging. J. Control. Release 2014, 179, 52–62. [Google Scholar] [CrossRef]
- Yang, F.; Stahnke, R.; Lawal, K.; Mahnen, C.; Duffy, P.; Xu, S.; Durig, T. Development of poly (lactic-co-glycolic acid) (PLGA) based implants using hot melt extrusion (HME) for sustained release of drugs: The impacts of PLGA’s material characteristics. Int. J. Pharm. 2024, 663, 124556. [Google Scholar] [CrossRef]
- Wang, X.; Bao, Q.; Wang, R.; Kwok, O.; Maurus, K.; Wang, Y.; Qin, B.; Burgess, D.J. In situ forming risperidone implants: Effect of PLGA attributes on product performance. J. Control. Release 2023, 361, 777–791. [Google Scholar] [CrossRef]
- Lehner, E.; Liebau, A.; Menzel, M.; Schmelzer, C.E.H.; Knolle, W.; Scheffler, J.; Binder, W.H.; Plontke, S.K.; Mäder, K. Characterization of PLGA versus PEG-PLGA intracochlear drug delivery implants: Degradation kinetics, morphological changes, and pH alterations. J. Drug Deliv. Sci. Technol. 2024, 99, 105972. [Google Scholar] [CrossRef]
- Bode, C.; Kranz, H.; Fivez, A.; Siepmann, F.; Siepmann, J. Often neglected: PLGA/PLA swelling orchestrates drug release: HME implants. J. Control. Release 2019, 306, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Bode, C.; Kranz, H.; Kruszka, A.; Siepmann, F.; Siepmann, J. In-situ forming PLGA implants: How additives affect swelling and drug release. J. Drug Deliv. Sci. Technol. 2019, 53, 10. [Google Scholar] [CrossRef]
- Vesna Milacic, V.M.; Schwendeman, S.P. Lysozyme release and polymer erosion behavior of injectable implants prepared from PLGA-PEG block copolymers and PLGA/PLGA-PEG blends. Pharm. Res. 2014, 31, 436–448. [Google Scholar] [CrossRef]
- Bassand, C.; Verin, J.; Lamatsch, M.; Siepmann, F.; Siepmann, J. How agarose gels surrounding PLGA implants limit swelling and slow down drug release. J. Control. Release 2022, 343, 255–266. [Google Scholar] [CrossRef]
- Gao, L.; Li, Q.; Zhang, J.; Huang, Y.; Deng, L.; Li, C.; Tai, G.; Ruan, B. Local penetration of doxorubicin via intrahepatic implantation of PLGA based doxorubicin-loaded implants. Drug Deliv. 2019, 26, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- KadioĞLu, Y.; AtİLa, A.; Vural, İ.; ÇEtİN, M. Preparation and characterization of anticancer drug-loaded implantable PLGA microparticles. Turk. J. Chem. 2010, 34, 509–516. [Google Scholar] [CrossRef]
- Zheng, L.; Wang, L.; Qin, J.; Sun, X.L.; Yang, T.T.; Ni, Y.X.; Zhou, Y.M. New Biodegradable Implant Material Containing Hydrogel with Growth Factors of Lyophilized PRF in Combination with an nHA/PLGA Scaffold. J. Hard Tissue Biol. 2015, 24, 54–60. [Google Scholar] [CrossRef]
- Kazek-Kesik, A.; Nosol, A.; Plonka, J.; Smiga-Matuszowicz, M.; Golda-Cepa, M.; Krok-Borkowicz, M.; Brzychczy-Wloch, M.; Pamula, E.; Simka, W. PLGA-amoxicillin-loaded layer formed on anodized Ti alloy as a hybrid material for dental implant applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 94, 998–1008. [Google Scholar] [CrossRef]
- Ghaffari, A.A.; Matter, B.A.; Hartman, R.R.; Bourne, D.W.A.; Wang, Y.; Choi, S.; Kompella, U.B. Hot-Melt Extrusion-Based Dexamethasone-PLGA Implants: Physicochemical, Physicomechanical, and Surface Morphological Properties and In Vitro Release Corrected for Drug Degradation. Pharmaceutics 2024, 16, 895. [Google Scholar] [CrossRef]
- Kasinathan, N.; Amirthalingam, M.; Reddy, N.D.; Vanthi, M.B.; Volety, S.M.; Rao, J.V. Polycaprolactone-based in situ implant containing curcumin-PLGA nanoparticles prepared using the multivariate technique. Artif. Cells Nanomed. Biotechnol. 2016, 44, 1520–1528. [Google Scholar] [CrossRef] [PubMed]
- Won, J.Y.; Park, C.Y.; Bae, J.H.; Ahn, G.; Kim, C.; Lim, D.H.; Cho, D.W.; Yun, W.S.; Shim, J.H.; Huh, J.B. Evaluation of 3D printed PCL/PLGA/β-TCP versus collagen membranes for guided bone regeneration in a beagle implant model. Biomed. Mater. 2016, 11, 055013. [Google Scholar] [CrossRef] [PubMed]
- Lehner, E.; Gundel, D.; Liebau, A.; Plontke, S.; Mader, K. Intracochlear PLGA based implants for dexamethasone release: Challenges and solutions. Int. J. Pharm. X 2019, 1, 100015. [Google Scholar] [CrossRef] [PubMed]
- Bible, E.; Qutachi, O.; Chau, D.Y.; Alexander, M.R.; Shakesheff, K.M.; Modo, M. Neo-vascularization of the stroke cavity by implantation of human neural stem cells on VEGF-releasing PLGA microparticles. Biomaterials 2012, 33, 7435–7446. [Google Scholar] [CrossRef]
- Sun, S.; Zhang, Y.; Zeng, D.; Zhang, S.; Zhang, F.; Yu, W. PLGA film/Titanium nanotubues as a sustained growth factor releasing system for dental implants. J. Mater. Sci. Mater. Med. 2018, 29, 141. [Google Scholar] [CrossRef]
- Zou, G.K.; Song, Y.L.; Zhou, W.; Yu, M.; Liang, L.H.; Sun, D.C.; Li, D.H.; Deng, Z.X.; Zhu, W.Z. Effects of local delivery of bFGF from PLGA microspheres on osseointegration around implants in diabetic rats. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 284–289. [Google Scholar] [CrossRef]
- Resende, A.F.C.; Pereira, A.F.; Moreira, T.P.; Patricio, P.S.O.; Fialho, S.L.; Cunha, G.M.F.; Silva-Cunha, A.; Magalhaes, J.T.; Silva, G.R. PLGA Implants containing vancomycin and dexamethasone: Development, characterization and bactericidal effects. Pharmazie 2016, 71, 439–446. [Google Scholar] [CrossRef]
- Soares, D.C.F.; de Paula Oliveira, D.C.; Barcelos, L.S.; Barbosa, A.S.; Vieira, L.C.; Townsend, D.M.; Rubello, D.; de Barros, A.L.B.; Duarte, L.P.; Silva-Cunha, A. Antiangiogenic activity of PLGA-Lupeol implants for potential intravitreal applications. Biomed. Pharmacother. 2017, 92, 394–402. [Google Scholar] [CrossRef]
- Toledo, C.R.; Pereira, V.V.; Andrade, G.F.; Silva-Cunha, A. PLGA-corosolic acid implants for potential application in ocular neovascularization diseases. Braz. J. Pharm. Sci. 2020, 56, e18484. [Google Scholar] [CrossRef]
- Hickey, T.; Kreutzer, D.; Burgess, D.J.; Moussy, F. Dexamethasone/PLGA microspheres for continuous delivery of an anti-inflammatory drug for implantable medical devices. Biomaterials 2002, 23, 1649–1656. [Google Scholar] [CrossRef]
- Do, M.P.; Neut, C.; Metz, H.; Delcourt, E.; Siepmann, J.; Mader, K.; Siepmann, F. Mechanistic analysis of PLGA/HPMC-based in-situ forming implants for periodontitis treatment. Eur. J. Pharm. Biopharm. 2015, 94, 273–283. [Google Scholar] [CrossRef]
- Carlier, E.; Marquette, S.; Peerboom, C.; Amighi, K.; Goole, J. Development of mAb-loaded 3D-printed (FDM) implantable devices based on PLGA. Int. J. Pharm. 2021, 597, 120337. [Google Scholar] [CrossRef] [PubMed]
- Maged, A.; Mabrouk, M.; Nour El-Din, H.T.; Osama, L.; Badr-Eldin, S.M.; Mahmoud, A.A. PLGA and PDMS-based in situ forming implants loaded with rosuvastatin and copper-selenium nanoparticles: A promising dual-effect formulation with augmented antimicrobial and cytotoxic activity in breast cancer cells. Front. Pharmacol. 2024, 15, 1397639. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Ren, S.; Zhang, X.; Yu, Y.; Liu, C.; Yang, J.; Miao, L. Safety and efficacy of PLGA(Ag-Fe3O4)-coated dental implants in inhibiting bacteria adherence and osteogenic inducement under a magnetic field. Int. J. Nanomed. 2018, 13, 3751–3762. [Google Scholar] [CrossRef]
- Geng, Z.; Dong, R.; Li, X.; Xu, X.; Chen, L.; Han, X.; Liu, D.; Liu, Y. Study on the Antibacterial Activity and Bone Inductivity of Nanosilver/PLGA-Coated TI-CU Implants. Int. J. Nanomed. 2024, 19, 6427–6447. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Tan, N.; Zhou, Y.; Wei, H.; Ren, S.; Yu, F.; Chen, H.; Jia, C.; Yang, G.; Song, Y. Delivery of antagomiR204-conjugated gold nanoparticles from PLGA sheets and its implication in promoting osseointegration of titanium implant in type 2 diabetes mellitus. Int. J. Nanomed. 2017, 12, 7089–7101. [Google Scholar] [CrossRef]
- Kefayat, A.; Vaezifar, S. Biodegradable PLGA implants containing doxorubicin-loaded chitosan nanoparticles for treatment of breast tumor-bearing mice. Int. J. Biol. Macromol. 2019, 136, 48–56. [Google Scholar] [CrossRef]
- Shi, S.; Song, S.; Liu, X.; Zhao, G.; Ding, F.; Zhao, W.; Zhang, S.; Song, Y.; Ma, W. Construction and performance of exendin-4-loaded chitosan-PLGA microspheres for enhancing implant osseointegration in type 2 diabetic rats. Drug Deliv. 2022, 29, 548–560. [Google Scholar] [CrossRef]
- Park, J.W.; Hwang, J.U.; Back, J.H.; Jang, S.W.; Kim, H.J.; Kim, P.S.; Shin, S.; Kim, T. High strength PLGA/Hydroxyapatite composites with tunable surface structure using PLGA direct grafting method for orthopedic implants. Compos. Part B Eng. 2019, 178, 107449. [Google Scholar] [CrossRef]
- Kim, M.S.; Ahn, H.H.; Shin, Y.N.; Cho, M.H.; Khang, G.; Lee, H.B. An in vivo study of the host tissue response to subcutaneous implantation of PLGA- and/or porcine small intestinal submucosa-based scaffolds. Biomaterials 2007, 28, 5137–5143. [Google Scholar] [CrossRef]
- Bai, H.Y.; Chen, G.A.; Mao, G.H.; Song, T.R.; Wang, Y.X. Three step derivation of cartilage like tissue from human embryonic stem cells by 2D-3D sequential culture in vitro and further implantation in vivo on alginate/PLGA scaffolds. J. Biomed. Mater. Res. A 2010, 94, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Xin, L.; Xu, W.; Yu, L.; Fan, S.; Wang, W.; Yu, F.; Wang, Z. Effects of annulus defects and implantation of poly(lactic-co-glycolic acid) (PLGA)/fibrin gel scaffolds on nerves ingrowth in a rabbit model of annular injury disc degeneration. J. Orthop. Surg. Res. 2017, 12, 73. [Google Scholar] [CrossRef] [PubMed]
- Eliaz, R.E.; Kost, J. Characterization of a polymeric PLGA-injectable implant delivery system for the controlled release of proteins. J. Biomed. Mater. Res. 2000, 50, 388–396. [Google Scholar] [CrossRef]
- Bode, C.; Kranz, H.; Siepmann, F.; Siepmann, J. In-situ forming PLGA implants for intraocular dexamethasone delivery. Int. J. Pharm. 2018, 548, 337–348. [Google Scholar] [CrossRef]
- Ibrahim, T.M.; El-Megrab, N.A.; El-Nahas, H.M. Optimization of injectable PLGA in-situ forming implants of anti-psychotic risperidone via Box-Behnken Design. J. Drug Deliv. Sci. Technol. 2020, 58, 101803. [Google Scholar] [CrossRef]
- Kamali, H.; Khodaverdi, E.; Hadizadeh, F.; Yazdian-Robati, R.; Haghbin, A.; Zohuri, G. An in-situ forming implant formulation of naltrexone with minimum initial burst release using mixture of PLGA copolymers and ethyl heptanoate as an additive: In-vitro, ex-vivo, and in-vivo release evaluation. J. Drug Deliv. Sci. Technol. 2018, 47, 95–105. [Google Scholar] [CrossRef]
- Bakhshi, R.; Vasheghani-Farahani, E.; Mobedi, H.; Jamshidi, A.; Khakpour, M. The effect of additives on naltrexone hydrochloride release and solvent removal rate from an injectable in situ forming PLGA implant. Polym. Adv. Technol. 2006, 17, 354–359. [Google Scholar] [CrossRef]
- Ramos, F.; Willart, J.F.; Neut, C.; Agossa, K.; Siepmann, J.; Siepmann, F. In-situ forming PLGA implants: Towards less toxic solvents. Int. J. Pharm. 2024, 657, 124121. [Google Scholar] [CrossRef]
- Bassand, C.; Siepmann, F.; Benabed, L.; Verin, J.; Freitag, J.; Charlon, S.; Soulestin, J.; Siepmann, J. 3D printed PLGA implants: How the filling density affects drug release. J. Control. Release 2023, 363, 1–11. [Google Scholar] [CrossRef]
- Riggin, C.N.; Qu, F.; Kim, D.H.; Huegel, J.; Steinberg, D.R.; Kuntz, A.F.; Soslowsky, L.J.; Mauck, R.L.; Bernstein, J. Electrospun PLGA Nanofiber Scaffolds Release Ibuprofen Faster and Degrade Slower After In Vivo Implantation. Ann. Biomed. Eng. 2017, 45, 2348–2359. [Google Scholar] [CrossRef]
- Elias-Al-Mamun, M.; Khan, H.A.; Dewan, I.; Jalil, R.U. In vitro study on tamsulosin release kinetics from biodegradable PLGA in situ implants. Pak. J. Pharm. Sci. 2009, 22, 360–367. [Google Scholar] [PubMed]
- Yu, Y.; Ngo, H.V.; Jin, G.; Tran, P.H.L.; Tran, T.T.D.; Nguyen, V.H.; Park, C.; Lee, B.J. Double-Controlled Release of Poorly Water-Soluble Paliperidone Palmitate from Self-Assembled Albumin-Oleic Acid Nanoparticles in PLGA in situ Forming Implant. Int. J. Nanomed. 2021, 16, 2819–2831. [Google Scholar] [CrossRef]
- Desai, K.G.; Olsen, K.F.; Mallery, S.R.; Stoner, G.D.; Schwendeman, S.P. Formulation and in vitro-in vivo evaluation of black raspberry extract-loaded PLGA/PLA injectable millicylindrical implants for sustained delivery of chemopreventive anthocyanins. Pharm. Res. 2010, 27, 628–643. [Google Scholar] [CrossRef] [PubMed]
- Enayati, M.; Mobedi, H.; Hojjati-Emami, S.; Mirzadeh, H.; Jafari-Nodoushan, M. In situ forming PLGA implant for 90 days controlled release of leuprolide acetate for treatment of prostate cancer. Polym. Adv. Technol. 2017, 28, 867–875. [Google Scholar] [CrossRef]
- Kokovic, V.; Todorovic, L. Preimplantation filling of tooth socket with β-tricalcium phosphate/polylactic-polyglycolic acid (β-TCP/PLGA) root analogue: Clinical and histological analysis in a patient. Vojnosanit. Pregl. 2011, 68, 366–371. [Google Scholar] [CrossRef]
- Prosolov, K.A.; Komarova, E.G.; Kazantseva, E.A.; Luginin, N.A.; Kashin, A.D.; Uvarkin, P.V.; Sharkeev, Y.P. Enhanced Corrosion Resistance and Mechanical Durability of the Composite PLGA/CaP/Ti Scaffolds for Orthopedic Implants. Polymers 2024, 16, 826. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Li, S.; Yin, Y.; Guo, J.; Chen, W.; Hou, Z.; Zhang, Y. Open-Wedge HTO with Absorbable β-TCP/PLGA Spacer Implantation and Proximal Fibular Osteotomy for Medial Compartmental Knee Osteoarthritis: New Technique Presentation. J. Investig. Surg. 2021, 34, 653–661. [Google Scholar] [CrossRef]
- Wachowiak, S.; Danede, F.; Willart, J.F.; Siepmann, F.; Siepmann, J.; Hamoudi, M. PLGA implants for controlled dexamethasone delivery: Impact of the polymer chemistry. J. Drug Deliv. Sci. Technol. 2023, 86, 104648. [Google Scholar] [CrossRef]
- Hickey, T.; Kreutzer, D.; Burgess, D.J.; Moussy, F. In vivo evaluation of a dexamethasone/PLGA microsphere system designed to suppress the inflammatory tissue response to implantable medical devices. J. Biomed. Mater. Res. 2002, 61, 180–187. [Google Scholar] [CrossRef]
- Gosau, M.; Muller, B.W. Release of gentamicin sulphate from biodegradable PLGA-implants produced by hot melt extrusion. Pharmazie 2010, 65, 487–492. [Google Scholar] [CrossRef]
- Ahmadi, H.; Haddadi-Asl, V.; Mohammadloo, H.E. Advancing anticorrosion and antibacterial performance of mg AZ31 implants using novel pH-responsive polymeric surfactant for preparing PLGA nanoparticles. Surf. Coat. Technol. 2024, 482, 130738. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, F.; Zheng, K.; Deng, L.; Yang, L.; Zhang, N.; Xu, C.; Ran, H.; Wang, Z.; Wang, Z.; et al. Injectable PLGA/Fe3O4 implants carrying cisplatin for synergistic magnetic hyperthermal ablation of rabbit VX2 tumor. PLoS ONE 2017, 12, e0177049. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Meisner, D.; Kwong, E.; Wu, X.Y.; Johnston, M.R. A novel trans-lymphatic drug delivery system: Implantable gelatin sponge impregnated with PLGA-paclitaxel microspheres. Biomaterials 2007, 28, 3236–3244. [Google Scholar] [CrossRef]
- Gao, W.; Zheng, Y.; Wang, R.; Chen, H.; Cai, X.; Lu, G.; Chu, L.; Xu, C.; Zhang, N.; Wang, Z.; et al. A smart, phase transitional and injectable DOX/PLGA-Fe implant for magnetic-hyperthermia-induced synergistic tumor eradication. Acta Biomater. 2016, 29, 298–306. [Google Scholar] [CrossRef]
- Zhao, X.; Zhang, S.; Yang, G.; Zhou, Z.; Gao, Y. Exploring Trehalose on the Release of Levonorgestrel from Implantable PLGA Microneedles. Polymers 2020, 12, 59. [Google Scholar] [CrossRef] [PubMed]
- Manna, S.; Donnell, A.M.; Kaval, N.; Al-Rjoub, M.F.; Augsburger, J.J.; Banerjee, R.K. Improved design and characterization of PLGA/PLA-coated Chitosan based micro-implants for controlled release of hydrophilic drugs. Int. J. Pharm. 2018, 547, 122–132. [Google Scholar] [CrossRef]
- Holmkvist, A.D.; Agorelius, J.; Forni, M.; Nilsson, U.J.; Linsmeier, C.E.; Schouenborg, J. Local delivery of minocycline-loaded PLGA nanoparticles from gelatin-coated neural implants attenuates acute brain tissue responses in mice. J. Nanobiotechnol. 2020, 18, 27. [Google Scholar] [CrossRef]
- Chang, N.J.; Lin, C.C.; Shie, M.Y.; Yeh, M.L.; Li, C.F.; Liang, P.I.; Lee, K.W.; Shen, P.H.; Chu, C.J. Positive effects of cell-free porous PLGA implants and early loading exercise on hyaline cartilage regeneration in rabbits. Acta Biomater. 2015, 28, 128–137. [Google Scholar] [CrossRef]
- Herran, E.; Perez-Gonzalez, R.; Igartua, M.; Pedraz, J.L.; Carro, E.; Hernandez, R.M. Enhanced Hippocampal Neurogenesis in APP/Ps1 Mouse Model of Alzheimer’s Disease After Implantation of VEGF-loaded PLGA Nanospheres. Curr. Alzheimer Res. 2015, 12, 932–940. [Google Scholar] [CrossRef]
- Bode, C.; Kranz, H.; Siepmann, F.; Siepmann, J. Coloring of PLGA implants to better understand the underlying drug release mechanisms. Int. J. Pharm. 2019, 569, 118563. [Google Scholar] [CrossRef]
- Agossa, K.; Lizambard, M.; Rongthong, T.; Delcourt-Debruyne, E.; Siepmann, J.; Siepmann, F. Physical key properties of antibiotic-free, PLGA/HPMC-based in-situ forming implants for local periodontitis treatment. Int. J. Pharm. 2017, 521, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Park, P.I.; Makoid, M.; Jonnalagadda, S. The design of flexible ciprofloxacin-loaded PLGA implants using a reversed phase separation/coacervation method. Eur. J. Pharm. Biopharm. 2011, 77, 233–239. [Google Scholar] [CrossRef]
- Jain, R.A.; Rhodes, C.T.; Railkar, A.M.; Malick, A.W.; Shah, N.H. Comparison of various injectable protein-loaded biodegradable poly(lactide-co-glycolide) (PLGA) devices: In-situ-formed implant versus in-situ-formed microspheres versus isolated microspheres. Pharm. Dev. Technol. 2000, 5, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Fassihi, R. Release rate determination from in situ gel forming PLGA implant: A novel ‘shape-controlled basket in tube’ method. J. Pharm. Pharmacol. 2020, 72, 1038–1048. [Google Scholar] [CrossRef] [PubMed]
- Ghalanbor, Z.; Korber, M.; Bodmeier, R. Interdependency of protein-release completeness and polymer degradation in PLGA-based implants. Eur. J. Pharm. Biopharm. 2013, 85, 624–630. [Google Scholar] [CrossRef]
- Kim, M.S.; Seo, K.S.; Hyun, H.; Kim, S.K.; Khang, G.; Lee, H.B. Sustained release of bovine serum albumin using implantable wafers prepared by MPEG-PLGA diblock copolymers. Int. J. Pharm. 2005, 304, 165–177. [Google Scholar] [CrossRef]
- Karp, F.; Turino, L.N.; Helbling, I.M.; Islan, G.A.; Luna, J.A.; Estenoz, D.A. In situ Formed Implants, Based on PLGA and Eudragit Blends, for Novel Florfenicol Controlled Release Formulations. J. Pharm. Sci. 2021, 110, 1270–1278. [Google Scholar] [CrossRef]
- Astaneh, R.; Erfan, M.; Barzin, J.; Mobedi, H.; Moghimi, H. Effects of Ethyl Benzoate on Performance, Morphology, and Erosion of PLGA Implants Formed In Situ. Adv. Polym. Technol. 2008, 27, 17–26. [Google Scholar] [CrossRef]
- Darlot, F.; Villard, P.; Salam, L.A.; Rousseau, L.; Piret, G. Glial scarring around intra-cortical MEA implants with flexible and free microwires inserted using biodegradable PLGA needles. Front. Bioeng. Biotechnol. 2024, 12, 1408088. [Google Scholar] [CrossRef]
- Lee, J.H.; Moon, S.K.; Kim, K.M.; Kim, K.N. Modification of TiO2 nanotube surfaces by electro-spray deposition of amoxicillin combined with PLGA for bactericidal effects at surgical implantation sites. Acta Odontol. Scand. 2013, 71, 168–174. [Google Scholar] [CrossRef]
- Noothongkaew, S.; Ariyachaokun, K.; Pansri, S. Enhanced bioactivity and antibacterial properties of anodized ZrO2 implant coatings via optimized nanoscale morphology and timed antibiotic release through PLGA overcoat. Ceram. Int. 2021, 47, 33775–33787. [Google Scholar] [CrossRef]
- Thalhauser, S.; Peterhoff, D.; Wagner, R.; Breunig, M. Silica particles incorporated into PLGA-based in situ-forming implants exploit the dual advantage of sustained release and particulate delivery. Eur. J. Pharm. Biopharm. 2020, 156, 1–10. [Google Scholar] [CrossRef]
- Kempe, S.; Metz, H.; Pereira, P.G.; Mader, K. Non-invasive in vivo evaluation of in situ forming PLGA implants by benchtop magnetic resonance imaging (BT-MRI) and EPR spectroscopy. Eur. J. Pharm. Biopharm. 2010, 74, 102–108. [Google Scholar] [CrossRef] [PubMed]
- van de Ven, C.; Bakker, N.E.C.; Link, D.P.; Geven, E.J.W.; Gossen, J.A. Sustained release of ancillary amounts of testosterone and alendronate from PLGA coated pericard membranes and implants to improve bone healing. PLoS ONE 2021, 16, e0251864. [Google Scholar] [CrossRef]
- Penk, A.; Forster, Y.; Scheidt, H.A.; Nimptsch, A.; Hacker, M.C.; Schulz-Siegmund, M.; Ahnert, P.; Schiller, J.; Rammelt, S.; Huster, D. The pore size of PLGA bone implants determines the de novo formation of bone tissue in tibial head defects in rats. Magn. Reson. Med. 2013, 70, 925–935. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.L.; Chen, Y.F.; Lu, W.J.; Zhang, Q.; Gao, S.; Sun, L.F.; Chen, S.Q.; Hu, R.F. A biodegradable long-term contraceptive implant with steady levonorgestrel release based on PLGA microspheres embedded in PCL-coated implant. J. Drug Deliv. Sci. Technol. 2022, 67, 102955. [Google Scholar] [CrossRef]
- Eawsakul, K.; Tancharoen, S.; Nasongkla, N. Combination of dip coating of BMP-2 and spray coating of PLGA on dental implants for osseointegration. J. Drug Deliv. Sci. Technol. 2021, 61, 102296. [Google Scholar] [CrossRef]
- Boimvaser, S.; Mariano, R.N.; Turino, L.N.; Vega, J.R. In vitro bulk/surface erosion pattern of PLGA implant in physiological conditions: A study based on auxiliary microsphere systems. Polym. Bull. 2016, 73, 209–227. [Google Scholar] [CrossRef]
- Kulkova, J.; Moritz, N.; Suokas, E.O.; Strandberg, N.; Leino, K.A.; Laitio, T.T.; Aro, H.T. Osteointegration of PLGA implants with nanostructured or microsized β-TCP particles in a minipig model. J. Mech. Behav. Biomed. Mater. 2014, 40, 190–200. [Google Scholar] [CrossRef]
- Bassand, C.; Benabed, L.; Freitag, J.; Verin, J.; Siepmann, F.; Siepmann, J. How bulk fluid renewal can affect in vitro drug release from PLGA implants: Importance of the experimental set-up. Int. J. Pharm. X 2022, 4, 100131. [Google Scholar] [CrossRef]
- Astaneh, R.; Erfan, M.; Moghimi, H.; Mobedi, H. Changes in morphology of in situ forming PLGA implant prepared by different polymer molecular weight and its effect on release behavior. J. Pharm. Sci. 2009, 98, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.B.; Park, C.H.; Park, K.; Chung, D.J.; Han, D.K. Biodegradable PLGA Polymer Coating on Biomedical Metal Implants Using Electrospraying. Polymer-Korea 2009, 33, 620–624. [Google Scholar]
- Golda-Cepa, M.; Chorylek, A.; Chytrosz, P.; Brzychczy-Wloch, M.; Jaworska, J.; Kasperczyk, J.; Hakkarainen, M.; Engvall, K.; Kotarba, A. Multifunctional PLGA/Parylene C Coating for Implant Materials: An Integral Approach for Biointerface Optimization. ACS Appl. Mater. Interfaces 2016, 8, 22093–22105. [Google Scholar] [CrossRef] [PubMed]
- Cosse, A.; Konig, C.; Lamprecht, A.; Wagner, K.G. Hot Melt Extrusion for Sustained Protein Release: Matrix Erosion and In Vitro Release of PLGA-Based Implants. AAPS PharmSciTech 2017, 18, 15–26. [Google Scholar] [CrossRef]
- Youssef, S.H.; Kim, S.; Khetan, R.; Afinjuomo, F.; Song, Y.M.; Garg, S. The development of 5-fluorouracil biodegradable implants: A comparative study of PCL/PLGA blends. J. Drug Deliv. Sci. Technol. 2023, 81, 104300. [Google Scholar] [CrossRef]
- Annaji, M.; Mita, N.; Poudel, I.; Boddu, S.H.S.; Fasina, O.; Babu, R.J. Three-Dimensional Printing of Drug-Eluting Implantable PLGA Scaffolds for Bone Regeneration. Bioengineering 2024, 11, 259. [Google Scholar] [CrossRef]
- Zhang, Z.; Ekanem, E.E.; Nakajima, M.; Bolognesi, G.; Vladisavljevic, G.T. Monodispersed Sirolimus-Loaded PLGA Microspheres with a Controlled Degree of Drug-Polymer Phase Separation for Drug-Coated Implantable Medical Devices and Subcutaneous Injection. ACS Appl. Bio Mater. 2022, 5, 3766–3777. [Google Scholar] [CrossRef]
- Bisht, R.; Jaiswal, J.K.; Oliver, V.F.; Eurtivong, C.; Reynisson, J.; Rupenthal, I.D. Preparation and evaluation of PLGA nanoparticle-loaded biodegradable light-responsive injectable implants as a promising platform for intravitreal drug delivery. J. Drug Deliv. Sci. Technol. 2017, 40, 142–156. [Google Scholar] [CrossRef]
- He, M.; Yang, G.; Zhao, X.; Zhang, S.; Gao, Y. Intradermal Implantable PLGA Microneedles for Etonogestrel Sustained Release. J. Pharm. Sci. 2020, 109, 1958–1966. [Google Scholar] [CrossRef]
- Santovena, A.; Alvarez-Lorenzo, C.; Concheiro, A.; Llabres, M.; Farina, J.B. Rheological properties of PLGA film-based implants: Correlation with polymer degradation and SPf66 antimalaric synthetic peptide release. Biomaterials 2004, 25, 925–931. [Google Scholar] [CrossRef]
- Kobielarz, M.; Tomanik, M.; Mroczkowska, K.; Szustakiewicz, K.; Oryszczak, M.; Mazur, A.; Antończak, A.; Filipiak, J. Laser-modified PLGA for implants: In vitro degradation and mechanical properties. Acta Bioeng. Biomech. 2020, 22, 179–192. [Google Scholar] [CrossRef] [PubMed]
- Fernandes-Cunha, G.M.; Fialho, S.L.; da Silva, G.R.; Silva-Cunha, A.; Zhao, M.; Behar-Cohen, F. Ocular safety of Intravitreal Clindamycin Hydrochloride Released by PLGA Implants. Pharm. Res. 2017, 34, 1083–1092. [Google Scholar] [CrossRef]
- Li, W.F.; Wang, X.P.; Wang, K.; Chen, T.N.; Chen, X.; Niu, X.F. A Novel of Biodegradable Implants Based on PLGA for Control Delivery of Cisplatin. Int. J. Polym. Mater. Polym. Biomater. 2014, 63, 368–373. [Google Scholar] [CrossRef]
- Li, Z.; Mu, H.; Weng Larsen, S.; Jensen, H.; Ostergaard, J. An in vitro gel-based system for characterizing and predicting the long-term performance of PLGA in situ forming implants. Int. J. Pharm. 2021, 609, 121183. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.H.; Railkar, A.S.; Chen, F.C.; Tarantino, R.; Kumar, S.; Murjani, M.; Palmer, D.; Infeld, M.H.; Malick, A.W. A Biodegradable Injectable Implant for Delivering Micromolecules and Macromolecules Using Poly(lactic-co-glycolic) Acid (PLGA) Copolymers. J. Control. Release 1993, 27, 139–147. [Google Scholar] [CrossRef]
- Wang, Y.; Gu, B.; Burgess, D.J. Microspheres prepared with PLGA blends for delivery of dexamethasone for implantable medical devices. Pharm. Res. 2014, 31, 373–381. [Google Scholar] [CrossRef]
- Dong, S.; Wang, S.; Zheng, C.; Liang, W.; Huang, Y. An in situ-forming, solid lipid/PLGA hybrid implant for long-acting antipsychotics. Soft Matter 2011, 7, 5873–5878. [Google Scholar] [CrossRef]
- Xin, L.; Zhang, C.; Zhong, F.; Fan, S.; Wang, W.; Wang, Z. Minimal invasive annulotomy for induction of disc degeneration and implantation of poly (lactic-co-glycolic acid) (PLGA) plugs for annular repair in a rabbit model. Eur. J. Med. Res. 2016, 21, 7. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.Q.; Liu, Q.; Wang, D.W.; Xie, T.; Guo, T.L.; Duan, K.; Weng, J. Room-temperature attachment of PLGA microspheres to titanium surfaces for implant-based drug release. Appl. Surf. Sci. 2014, 309, 112–118. [Google Scholar] [CrossRef]
- Yang, R.; Chen, T.N.; Chen, H.L.; Wang, W.J. Microfabrication of biodegradable (PLGA) honeycomb-structures and potential applications in implantable drug delivery. Sens. Actuator B Chem. 2005, 106, 506–511. [Google Scholar] [CrossRef]
- Dorta, M.J.; Santovena, A.; Llabres, M.; Farina, J.B. Potential applications of PLGA film-implants in modulating in vitro drugs release. Int. J. Pharm. 2002, 248, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Dorta, M.J.; Oliva, A.; Munguia, O.; Llabres, M.; Farina, J.B. In-vitro release of fluoropyrimidines from PLGA film implants. J. Pharm. Pharmacol. 2002, 54, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Manna, S.; Donnell, A.M.; Faraj, R.Q.C.; Riemann, B.I.; Riemann, C.D.; Augsburger, J.J.; Correa, Z.M.; Banerjee, R.K. Pharmacokinetics and Toxicity Evaluation of a PLGA and Chitosan-Based Micro-Implant for Sustained Release of Methotrexate in Rabbit Vitreous. Pharmaceutics 2021, 13, 1227. [Google Scholar] [CrossRef]
- Ramchandani, M.; Robinson, D. In vitro and in vivo release of ciprofloxacin from PLGA 50:50 implants. J. Control. Release 1998, 54, 167–175. [Google Scholar] [CrossRef]
- Fernandes-Cunha, G.M.; Rezende, C.M.; Mussel, W.N.; da Silva, G.R.; Gomes, E.C.d.L.; Yoshida, M.I.; Fialho, S.L.; Goes, A.M.; Gomes, D.A.; de Almeida Vitor, R.W.; et al. Anti-Toxoplasma activity and impact evaluation of lyophilization, hot molding process, and gamma-irradiation techniques on CLH-PLGA intravitreal implants. J. Mater. Sci. Mater. Med. 2016, 27, 10. [Google Scholar] [CrossRef] [PubMed]
- Tavares, H.S.; Cardoso, J.F.; Almeida, T.C.; Marques, M.B.F.; Mussel, W.N.; Lopes, M.C.P.; Orefice, R.L.; Andrade, S.N.; Varotti, F.P.; Silva, G.N.; et al. Spiramyin-loaded PLGA implants for the treatment of ocular toxoplasmosis: Development, characterization, biocompatibility, and anti-toxoplasma activity. Pharmazie 2021, 76, 68–76. [Google Scholar] [CrossRef]
- Kamali, H.; Khodaverdi, E.; Hadizadeh, F.; Mohajeri, S.A.; Nazari, A.; Jafarian, A.H. Comparison of in-situ forming composite using PLGA-PEG-PLGA with in-situ forming implant using PLGA: In-vitro, ex-vivo, and in-vivo evaluation of naltrexone release. J. Drug Deliv. Sci. Technol. 2019, 50, 188–200. [Google Scholar] [CrossRef]
- Gilchrist, S.E.; Lange, D.; Letchford, K.; Bach, H.; Fazli, L.; Burt, H.M. Fusidic acid and rifampicin co-loaded PLGA nanofibers for the prevention of orthopedic implant associated infections. J. Control. Release 2013, 170, 64–73. [Google Scholar] [CrossRef]
- Newby, S.D.; Forsynth, C.; Bow, A.J.; Bourdo, S.E.; Hung, M.; Cheever, J.; Moffat, R.; Gross, A.J.; Licari, F.W.; Dhar, M.S. Xenogenic Implantation of Human Mesenchymal Stromal Cells Using a Novel 3D-Printed Scaffold of PLGA and Graphene Leads to a Significant Increase in Bone Mineralization in a Rat Segmental Femoral Bone Defect. Nanomaterials 2023, 13, 1149. [Google Scholar] [CrossRef]
- Ju, Y.M.; Yu, B.; West, L.; Moussy, Y.; Moussy, F. A dexamethasone-loaded PLGA microspheres/collagen scaffold composite for implantable glucose sensors. J. Biomed. Mater. Res. A 2010, 93, 200–210. [Google Scholar] [CrossRef]
- Ranganath, S.H.; Fu, Y.; Arifin, D.Y.; Kee, I.; Zheng, L.; Lee, H.S.; Chow, P.K.; Wang, C.H. The use of submicron/nanoscale PLGA implants to deliver paclitaxel with enhanced pharmacokinetics and therapeutic efficacy in intracranial glioblastoma in mice. Biomaterials 2010, 31, 5199–5207. [Google Scholar] [CrossRef]
- Razzaghi, M.; Kasiri-Asgarani, M.; Bakhsheshi-Rad, H.R.; Ghayour, H. In vitro bioactivity and corrosion of PLGA/hardystonite composite-coated magnesium-based nanocomposite for implant applications. Int. J. Miner. Metall. Mater. 2020, 28, 168–178. [Google Scholar] [CrossRef]
- Komarova, E.G.; Senkina, E.I.; Lozhkomoev, A.S.; Kazantseva, E.A.; Prosolov, K.A.; Kazantsev, S.O.; Akimova, E.B.; Tolkacheva, T.; Khimich, M.A.; Sharkeev, Y.P. Controlled anticancer 5-Fluorouracil release from functionalized 5-FU/PLGA/CaP coating on titanium implants: Characterization, in vitro drug delivery and cytotoxicity. Mater. Today Commun. 2024, 39, 109332. [Google Scholar] [CrossRef]
- Kamali, H.; Khodaverdi, E.; Hadizadeh, F.; Mohajeri, S.A.; Kamali, Y.; Jafarian, A.H. In-vitro, ex-vivo, and in-vivo release evaluation of in situ forming buprenorphine implants using mixture of PLGA copolymers and additives. Int. J. Polym. Mater. Polym. Biomater. 2018, 68, 965–977. [Google Scholar] [CrossRef]
- Shen, J.; Burgess, D.J. Accelerated in vitro release testing of implantable PLGA microsphere/PVA hydrogel composite coatings. Int. J. Pharm. 2012, 422, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Milosevic, M.; Stojanovic, D.; Simic, V.; Milicevic, B.; Radisavljevic, A.; Uskokovic, P.; Kojic, M. A Computational Model for Drug Release from PLGA Implant. Materials 2018, 11, 2416. [Google Scholar] [CrossRef] [PubMed]
- Souza, M.C.; Fialho, S.L.; Souza, P.A.; Fulgencio, G.O.; Da Silva, G.R.; Silva-Cunha, A. Tacrolimus-loaded PLGA implants: In vivo release and ocular toxicity. Curr. Eye Res. 2014, 39, 99–102. [Google Scholar] [CrossRef]
- Ahmed, O.A.; Zidan, A.S.; Khayat, M. Mechanistic analysis of Zein nanoparticles/PLGA triblock in situ forming implants for glimepiride. Int. J. Nanomed. 2016, 11, 543–555. [Google Scholar] [CrossRef]
- Castro, M.A.d.; Cunha, G.M.F.; Andrade, G.F.; Yoshida, M.I.; Faria, A.L.d.; Silva-Cunha, A. Development and characterization of PLGA-Bupivacaine and PLGA-S75:R25 Bupivacaine (Novabupi®) biodegradable implants for postoperative pain. Braz. J. Pharm. Sci. 2022, 58, 10. [Google Scholar] [CrossRef]
- Costello, M.A.; Liu, J.; Kuehster, L.; Wang, Y.; Qin, B.; Xu, X.; Li, Q.; Smith, W.C.; Lynd, N.A.; Zhang, F. Role of PLGA Variability in Controlled Drug Release from Dexamethasone Intravitreal Implants. Mol. Pharm. 2023, 20, 6330–6344. [Google Scholar] [CrossRef]
- Patrick, C.W., Jr.; Zheng, B.; Johnston, C.; Reece, G.P. Long-term implantation of preadipocyte-seeded PLGA scaffolds. Tissue Eng. 2002, 8, 283–293. [Google Scholar] [CrossRef]
- Wang, X.; Qi, F.; Xing, H.; Zhang, X.; Lu, C.; Zheng, J.; Ren, X. Uniform-sized insulin-loaded PLGA microspheres for improved early-stage peri-implant bone regeneration. Drug Deliv. 2019, 26, 1178–1190. [Google Scholar] [CrossRef]
- Sendil, D.; Bonney, I.M.; Carr, D.B.; Lipkowski, A.W.; Wise, D.L.; Hasirci, V. Antinociceptive effects of hydromorphone, bupivacaine and biphalin released from PLGA polymer after intrathecal implantation in rats. Biomaterials 2003, 24, 1969–1976. [Google Scholar] [CrossRef] [PubMed]
- Krucinska, I.; Zywicka, B.; Komisarczyk, A.; Szymonowicz, M.; Kowalska, S.; Zaczynska, E.; Struszczyk, M.; Czarny, A.; Jadczyk, P.; Uminska-Wasiluk, B.; et al. Biological Properties of Low-Toxicity PLGA and PLGA/PHB Fibrous Nanocomposite Implants for Osseous Tissue Regeneration. Part I: Evaluation of Potential Biotoxicity. Molecules 2017, 22, 2092. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Yuan, Z.; Kao, W.; Miller, D.; Li, S.K.; Park, Y.C. Size-Exclusive Nanoporous Biodegradable PLGA Capsules for Drug Delivery Implants and In Vivo Stability in the Posterior Segment. ACS Appl. Bio Mater. 2020, 3, 1722–1729. [Google Scholar] [CrossRef]
- Bhardwaj, U.; Sura, R.; Papadimitrakopoulos, F.; Burgess, D.J. PLGA/PVA hydrogel composites for long-term inflammation control following s.c. implantation. Int. J. Pharm. 2010, 384, 78–86. [Google Scholar] [CrossRef]
- Link, D.P.; van den Dolder, J.; Jurgens, W.J.; Wolke, J.G.; Jansen, J.A. Mechanical evaluation of implanted calcium phosphate cement incorporated with PLGA microparticles. Biomaterials 2006, 27, 4941–4947. [Google Scholar] [CrossRef]
- Chang, N.J.; Lin, C.C.; Li, C.F.; Wang, D.A.; Issariyaku, N.; Yeh, M.L. The combined effects of continuous passive motion treatment and acellular PLGA implants on osteochondral regeneration in the rabbit. Biomaterials 2012, 33, 3153–3163. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.C.; Chu, C.J.; Chou, P.H.; Liang, C.H.; Liang, P.I.; Chang, N.J. Beneficial Therapeutic Approach of Acellular PLGA Implants Coupled With Rehabilitation Exercise for Osteochondral Repair: A Proof of Concept Study in a Minipig Model. Am. J. Sports Med. 2020, 48, 2796–2807. [Google Scholar] [CrossRef]
- Stefani, R.M.; Lee, A.J.; Tan, A.R.; Halder, S.S.; Hu, Y.; Guo, X.E.; Stoker, A.M.; Ateshian, G.A.; Marra, K.G.; Cook, J.L.; et al. Sustained low-dose dexamethasone delivery via a PLGA microsphere-embedded agarose implant for enhanced osteochondral repair. Acta Biomater. 2020, 102, 326–340. [Google Scholar] [CrossRef]
- Wen, Y.; Yu, S.; Wu, Y.; Ju, R.; Wang, H.; Liu, Y.; Wang, Y.; Xu, Q. Spinal cord injury repair by implantation of structured hyaluronic acid scaffold with PLGA microspheres in the rat. Cell Tissue Res. 2016, 364, 17–28. [Google Scholar] [CrossRef]
- Nair, P.N.R.; Schug, J. Observations on healing of human tooth extraction sockets implanted with bioabsorbable polylactic-polyglycolic acids (PLGA) copolymer root replicas: A clinical, radiographic, and histologic follow-up report of 8 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 97, 559–569. [Google Scholar] [CrossRef]
- Landes, C.A.; Ballon, A.; Roth, C. Maxillary and mandibular osteosyntheses with PLGA and P(L/DL)LA implants: A 5-year inpatient biocompatibility and degradation experience. Plast. Reconstr. Surg. 2006, 117, 2347–2360. [Google Scholar] [CrossRef] [PubMed]
- Hild, N.; Tawakoli, P.N.; Halter, J.G.; Sauer, B.; Buchalla, W.; Stark, W.J.; Mohn, D. pH-dependent antibacterial effects on oral microorganisms through pure PLGA implants and composites with nanosized bioactive glass. Acta Biomater. 2013, 9, 9118–9125. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Hu, M.; Liu, W.; Hou, N.; Yin, K.; Shen, C.; Shang, Q. Fabrication of PLGA in situ forming implants and study on their correlation of in vitro release profiles with in vivo performances. J. Biomater. Sci. Polym. Ed. 2021, 32, 994–1008. [Google Scholar] [CrossRef] [PubMed]
- Gomaa, E.; Eissa, N.G.; Ibrahim, T.M.; El-Bassossy, H.M.; El-Nahas, H.M.; Ayoub, M.M. Development of depot PLGA-based in-situ implant of Linagliptin: Sustained release and glycemic control. Saudi. Pharm. J 2023, 31, 499–509. [Google Scholar] [CrossRef]
- Han, I.B.; Thakor, D.K.; Ropper, A.E.; Yu, D.; Wang, L.; Kabatas, S.; Zeng, X.; Kim, S.W.; Zafonte, R.D.; Teng, Y.D. Physical impacts of PLGA scaffolding on hMSCs: Recovery neurobiology insight for implant design to treat spinal cord injury. Exp. Neurol. 2019, 320, 112980. [Google Scholar] [CrossRef]
- Manaspon, C.; Hernandez, C.; Nittayacharn, P.; Jeganathan, S.; Nasongkla, N.; Exner, A.A. Increasing Distribution of Drugs Released from In Situ Forming PLGA Implants Using Therapeutic Ultrasound. Ann. Biomed. Eng. 2017, 45, 2879–2887. [Google Scholar] [CrossRef]
- Li, J.; Krupka, T.; Yao, J.; Wang, R.; Jiang, L.; Zhou, Y.; Zuo, G.; Wang, Z.; Dai, L.; Ren, J.; et al. Liquid-solid phase-inversion PLGA implant for the treatment of residual tumor tissue after HIFU ablation. PLoS ONE 2015, 10, e0117358. [Google Scholar] [CrossRef]
- Pas, J.; Rutz, A.L.; Quilichini, P.P.; Slezia, A.; Ghestem, A.; Kaszas, A.; Donahue, M.J.; Curto, V.F.; O’Connor, R.P.; Bernard, C.; et al. A bilayered PVA/PLGA-bioresorbable shuttle to improve the implantation of flexible neural probes. J. Neural Eng. 2018, 15, 065001. [Google Scholar] [CrossRef]
- He, P.; Xu, S.; Guo, Z.; Yuan, P.; Liu, Y.; Chen, Y.; Zhang, T.; Que, Y.; Hu, Y. Pharmacodynamics and pharmacokinetics of PLGA-based doxorubicin-loaded implants for tumor therapy. Drug Deliv. 2022, 29, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Li, C.; Zhou, J. Effective sustained release of 5-FU-loaded PLGA implant for improving therapeutic index of 5-FU in colon tumor. Int. J. Pharm. 2018, 550, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Yao, C.; Zhang, Q.; Li, J.; She, P.; Kong, F.; Du, Y.; Zhang, F. Implantable zoledronate-PLGA microcapsules ameliorate alveolar bone loss, gingival inflammation and oxidative stress in an experimental periodontitis rat model. J. Biomater. Appl. 2021, 35, 569–578. [Google Scholar] [CrossRef]
- Parent, M.; Nouvel, C.; Koerber, M.; Sapin, A.; Maincent, P.; Boudier, A. PLGA in situ implants formed by phase inversion: Critical physicochemical parameters to modulate drug release. J. Control. Release 2013, 172, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; He, J.; Olson, J.J.; Lu, D.R. Carboplatin-Loaded PLGA Microspheres for Intracerebral Implantation: In Vivo Characterization. Drug Deliv. 1997, 4, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Dsa, J.; Bekal, A.; Goswami, M. Microfabrication and Characterization of Chemically Actuated Implantable PLGA Reservoir-based Device for Controlled Drug Delivery. IETE J. Res. 2023, 70, 2941–2948. [Google Scholar] [CrossRef]
- Bakhrushina, E.O.; Sakharova, P.S.; Konogorova, P.D.; Pyzhov, V.S.; Kosenkova, S.I.; Bardakov, A.I.; Zubareva, I.M.; Krasnyuk, I.I.; Krasnyuk, I.I., Jr. Burst Release from In Situ Forming PLGA-Based Implants: 12 Effectors and Ways of Correction. Pharmaceutics 2024, 16, 115. [Google Scholar] [CrossRef]
- Santoveña, A.; Alvarez-Lorenzo, C.; Llabrés, M.; Concheiro, A.; Fariña, J.B. hGH release from directly compressed hGH-PLGA biodegradable implantable tablets: Influence of physicomechanical factors. Eur. Polym. J. 2009, 45, 2830–2838. [Google Scholar] [CrossRef]
- Amann, L.C.; Gandal, M.J.; Lin, R.; Liang, Y.; Siegel, S.J. In vitro-in vivo correlations of scalable PLGA-risperidone implants for the treatment of schizophrenia. Pharm. Res. 2010, 27, 1730–1737. [Google Scholar] [CrossRef]
- He, P.; Que, Y.K.; Li, S.; Chen, Y.; Xiao, L.Z.; Wang, H.M.; Guo, Z.H.; Wang, S.L.; Hu, Y. Enhanced anti-rheumatic efficacy of PLGA-based methotrexate-loaded implants in adjuvant-induced arthritis rat model. J. Drug Deliv. Sci. Technol. 2023, 88, 104939. [Google Scholar] [CrossRef]
- Zlomke, C.; Barth, M.; Mader, K. Polymer degradation induced drug precipitation in PLGA implants–Why less is sometimes more. Eur. J. Pharm. Biopharm. 2019, 139, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; He, L.; Pan, S.; Zhang, L.; Zhang, W.; Yi, H.; Niu, Y. Three-dimensional simulated microgravity culture improves the proliferation and odontogenic differentiation of dental pulp stem cell in PLGA scaffolds implanted in mice. Mol. Med. Rep. 2017, 15, 873–878. [Google Scholar] [CrossRef]
- Caminal, M.; Moll, X.; Codina, D.; Rabanal, R.M.; Morist, A.; Barrachina, J.; Garcia, F.; Pla, A.; Vives, J. Transitory improvement of articular cartilage characteristics after implantation of polylactide:polyglycolic acid (PLGA) scaffolds seeded with autologous mesenchymal stromal cells in a sheep model of critical-sized chondral defect. Biotechnol. Lett. 2014, 36, 2143–2153. [Google Scholar] [CrossRef] [PubMed]
- Onishi, H.; Takahashi, M.; Machida, Y. PLGA implant tablet of ketoprofen: Comparison of in vitro and in vivo releases. Biol. Pharm. Bull. 2005, 28, 2011–2015. [Google Scholar] [CrossRef]
- Rodriguez-Agirretxe, I.; Vega, S.C.; Rezola, R.; Vecino, E.; Mendicute, J.; Suarez-Cortes, T.; Acera, A. The PLGA implant as an antimitotic delivery system after experimental trabeculectomy. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5227–5235. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.J.; Bichara, D.A.; Zhao, X.; Randolph, M.A.; Gill, T.J. Implant-assisted meniscal repair in vivo using a chondrocyte-seeded flexible PLGA scaffold. J. Biomed. Mater. Res. A 2011, 99, 102–108. [Google Scholar] [CrossRef]
- Gad, H.A.; El-Nabarawi, M.A.; Abd El-Hady, S.S. Formulation and evaluation of PLA and PLGA in situ implants containing secnidazole and/or doxycycline for treatment of periodontitis. AAPS PharmSciTech 2008, 9, 878–884. [Google Scholar] [CrossRef]
- Lozza, I.; Martin-Sabroso, C.; Torres-Suarez, A.I.; Fraguas-Sanchez, A.I. In situ forming PLA and PLGA implants for the parenteral administration of Cannabidiol. Int. J. Pharm. 2024, 661, 124468. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PLGA and Additives in Implants | Expanded Patterns in Applications | Refs. |
|---|---|---|
| PLGA + Glycerol, Ethyl Heptanoate | Modifies implant morphology to reduce burst release and enhance mechanical stability; effective in opioid addiction treatment and antibiotic delivery systems. | [56,57,58] |
| PLGA + Ibuprofen | Widely used in pain relief and inflammation therapy, with hot melt extrusion and 3D printing methods enabling personalized and controlled release profiles. | [4,8,25,59,60] |
| PLGA + Dimethyl Sulfoxide (DMSO) | Facilitates in situ forming depot systems, reducing burst release for psychiatric and hormone therapies; supports rapid implant solidification. | [55,61] |
| PLGA + PEG | Enhances protein and peptide release by neutralizing acidic degradation; also used as a plasticizer in implants for flexibility and tailored degradation rates. | [3,21,23,40] |
| PLGA + Albumin–Oleic Acid Conjugates (AOC) | Double-controlled release systems for psychiatric drug delivery, reducing burst effects and enabling sustained release over weeks. | [62] |
| PLGA + β-Cyclodextrin (β-CD) | Improves peptide delivery by modulating polymer erosion and sustained drug release; effective in cancer and hormone therapies. | [12,42,63] |
| PLGA + Hydroxyapatite or β-TCP | Promotes bone regeneration by enhancing osteoconductivity; used in dental, orthopedic, and spine applications with sustained release for months. | [45,64,65,66,67] |
| PLGA + Poloxamer, PEO | Adjusts polymer swelling to control drug release; ideal for local anesthetic delivery with tunable degradation and erosion properties. | [10] |
| PLGA + Dexamethasone | A key agent in inflammation control, delivering sustained release in neural, ocular, and implantable medical devices for weeks to months. | [22,37,40,68,69] |
| PLGA + Antibiotics (e.g., Ciprofloxacin, Gentamicin) | Provides localized infection control in orthopedic and dental implants; coatings offer sustained antibacterial activity and biofilm prevention. | [44,45,70] |
| PLGA + Metal Nanoparticles (e.g., Ag, Fe3O4) | Combines antibacterial and bioactive properties for implant coatings; effective in reducing infections and promoting osseointegration. | [44,45,71] |
| PLGA + Paclitaxel, Doxorubicin (DOX) | Used in advanced chemotherapy delivery systems, integrating phase-specific release for targeted tumor reduction and minimal systemic toxicity. | [6,27,72,73,74] |
| PLGA + Trehalose, Chitosan | Enhances protein stability and biocompatibility; chitosan contributes to tissue integration in neural, ocular, and bone repair systems. | [48,75,76] |
| PLGA + Various Solvents (e.g., NMP, TEC, Ethanol) | Solvent systems influence implant morphology, burst release, and sustained delivery; commonly used in in situ forming implants and depot formulations. | [9,23,54,56,58] |
| PLGA + Alginate or Gelatin | Enhances structural support and drug retention for cartilage, neural, and bone regeneration; supports dual-release systems for complex treatments. | [51,73,77,78] |
| PLGA + VEGF or Growth Factors | Stimulates vascularization and tissue repair, particularly in stroke and regenerative therapies; biphasic release supports long-term recovery. | [28,34,36,79] |
| PLGA + Fluorescent Markers or Dyes | Enables real-time imaging and monitoring of drug release profiles and implant degradation in vivo, supporting formulation refinement. | [18,80] |
| PLGA + Excipients (e.g., HPMC, Stearic Acid) | Modulates release profiles by altering implant swelling and phase separation; effective in anti-inflammatory and antibiotic delivery systems. | [23,41,81] |
| Physicochemical Property | Expanded Observations and Patterns | Refs. |
|---|---|---|
| Entrapment Efficiency | High efficiency observed (47.03–95.34%) across multiple applications. Factors include polymer compatibility, drug hydrophilicity, and particle size. For proteins/peptides, additives like PEG improved encapsulation and preserved bioactivity. | [1,61,86,96,97] |
| Drug Release Kinetics | Bi-phasic, tri-phasic, and near-zero-order patterns linked to polymer degradation and diffusion mechanisms. Additives and solvent choices significantly modified release phases, enabling longer release durations (up to 6 months for some formulations). | [4,19,21,22,68] |
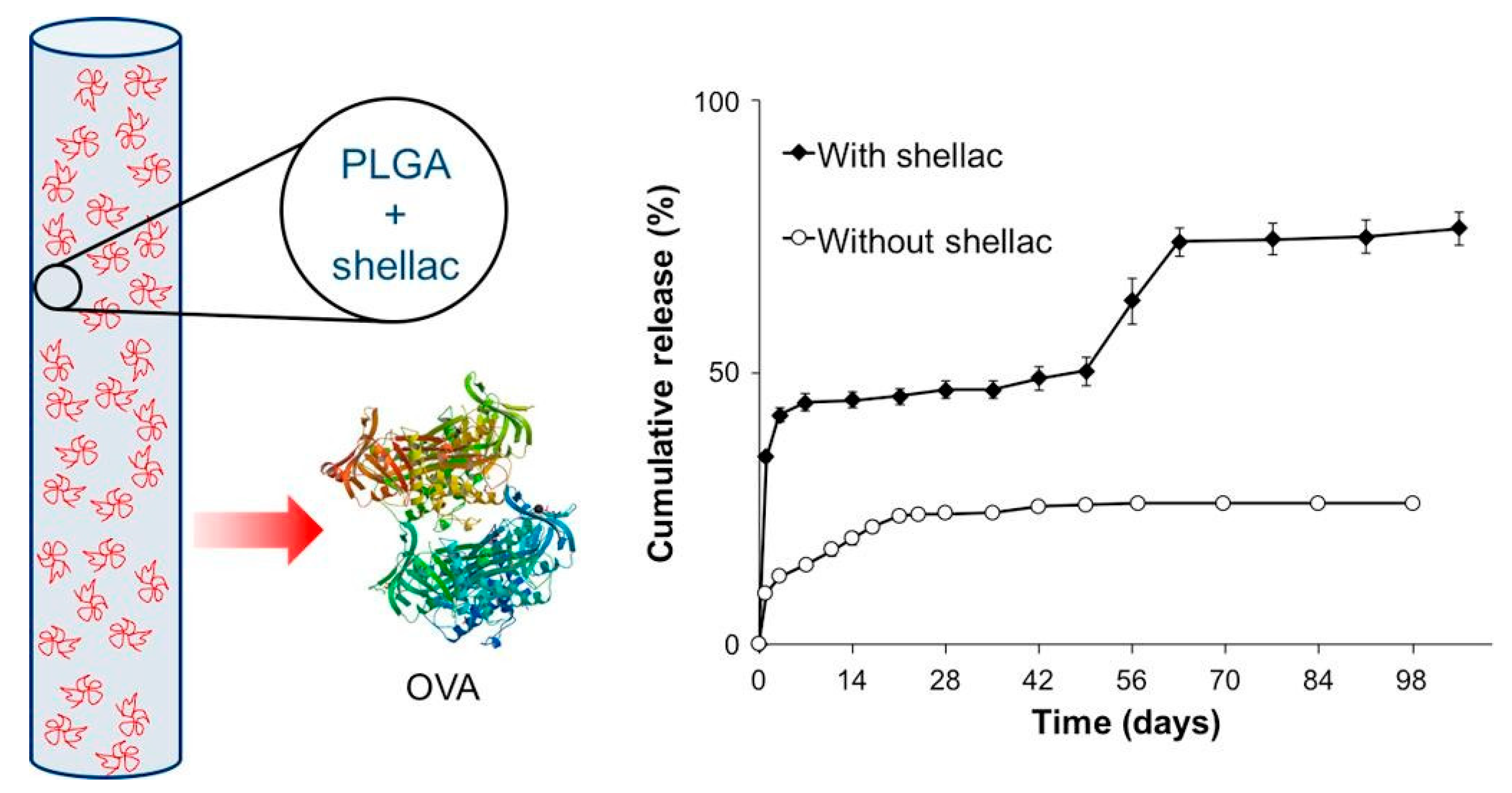
| Burst Release | Reduced burst release (<5%) achieved through techniques such as altering solvent miscibility, adding PEG, or modifying polymer end groups. Formulations with medium MW PLGA (e.g., 34 kDa) and additives like shellac showed effective burst suppression. | [3,12,23,83] |
| Swelling Behavior | Swelling increased implant size significantly (600–1700%), promoting drug release by enhancing water penetration. Hydrophobic additives reduced swelling effects, creating more controlled release profiles. | [5,21,22,54,68] |
| Degradation Rate | Degradation onset (3–14 days) controlled by PLGA MW, lactide/glycolide ratio, and terminal group composition. Low MW and 50:50 ratios accelerated degradation, while higher lactide ratios slowed polymer erosion. | [4,5,14,98,99] |
| Morphology | Dense, porous, and sponge-like morphologies affected drug release and stability. Porous structures allowed faster release and better protein encapsulation, while dense morphologies delayed erosion and prolonged release. | [57,88,91,100,101] |
| Particle Size | Smaller particle sizes (~100 nm) favored rapid release and clearance, while larger particles (~10 μm) enabled prolonged drug delivery. Morphological transitions during release contributed to changing surface areas and release rates. | [3,48,73,96] |
| Controlled Porosity | Optimized pore sizes (300–500 μm) improved tissue integration and drug delivery, especially in bone regeneration. Excess porosity led to burst effects, while controlled pore architecture enabled sustained release. | [25,32,95] |
| Glass Transition Temperature (Tg) | Lower Tg (<20 °C) allowed flexible implant fabrication, critical for applications like injectable systems and neural implants. Tg affected mechanical properties and degradation rates. | [19,82,84] |
| Surface Modification | Surface coatings (e.g., plasma treatment, nanosilver, or bioactive glass) enhanced implant biocompatibility, corrosion resistance, and drug release. Modified surfaces also reduced bacterial adhesion and inflammatory responses. | [66,71,102,103] |
| Encapsulation Efficiency (Proteins/Peptides) | Protein formulations achieved encapsulation efficiencies >90%. Incorporating excipients like PEG improved protein stability and reduced denaturation, enabling effective long-term delivery. | [24,53,86,104] |
| Release Models | Korsmeyer–Peppas, Weibull, and Higuchi models effectively described release kinetics. Multi-phase models were common, reflecting the combined effects of diffusion, swelling, and polymer erosion. | [6,12,19,105,106] |
| Polymer Molecular Weight (MW) | MW directly influenced drug release and degradation. Medium MW (~34 kDa) associated with balanced release profiles; high MW (>50 kDa) delayed onset of degradation. | [5,7,22,101] |
| Lactide/Glycolide Ratio | Ratios of 75:25 provided slower, more sustained release profiles, ideal for depot formulations. Ratios of 50:50 favored faster degradation and burst effects, suitable for short-term therapies. | [2,20,64] |
| Surface Area to Volume Ratio | Higher surface-to-volume ratios accelerated release, with shape-controlled implants (e.g., honeycomb designs) demonstrating predictable release kinetics. | [17,84,107] |
| Residual Monomers | Residual monomer content increased degradation rates but reduced initial lag phases. Suitable for applications requiring rapid release initiation. | [19,30] |
| Hydrophilicity/Hydrophobicity | Hydrophobic additives (e.g., Eudragit S100) delayed drug release and reduced burst effects. Hydrophilic components (e.g., PEG) enhanced swelling and initial release. | [23,24,88] |
| Zeta Potential | Stable nanoparticle systems demonstrated zeta potentials around −30 mV, enabling efficient drug encapsulation and sustained release. | [108] |
| Drug Loading | High drug loading (>30%) accelerated burst release, requiring balancing with polymer additives to maintain controlled kinetics. | [12,88,96,109] |
| Diffusion-Controlled Release | Diffusion mechanisms dominated during early release phases, particularly in systems with large surface areas or controlled porosity. | [4,8,11,12] |
| Erosion Profiles | Implants exhibited bulk erosion in early phases and transitioned to surface erosion as structural integrity diminished. First-order kinetics commonly describes this behavior. | [54,68,98,104] |
| Elastic Modulus and Mechanical Properties | Mechanical properties decreased significantly as polymer degraded, with elastic modulus changes aligning with drug release and structural erosion. | [66,99,110,111] |
| Water Uptake | Higher water uptake correlated with rapid polymer swelling and enhanced drug diffusion. Formulations with hydrophobic additives exhibited delayed water absorption and prolonged release. | [22,85,93] |
| Biocompatibility | Additives like PEG, HPMC, and surface coatings reduced inflammatory responses. Implants demonstrated minimal toxicity in vivo, preserving tissue structure and function. | [50,102,104,112] |
| Processing Method | Key Insights and Observed Patterns | Technical Data | Refs. |
|---|---|---|---|
| Hot Melt Extrusion (HME) | Stable implants; controls polymer-drug interactions and implant stability. | Temp: 90–120 °C; Pressure: 20–50 MPa; Drug–polymer blends milled before extrusion; compatible with heat-stable drugs. | [4,11,19,22,30,59,85,100] |
| Solvent Casting and Evaporation | Produces thin films and multilayer structures; controls burst release. | Solvents: Dichloromethane (DCM), acetone; Evaporation under reduced pressure; Thickness: 50–500 μm. | [12,101,121,122,123] |
| Phase Separation/Coacervation | Encapsulates hydrophilic and hydrophobic drugs; achieves controlled release. | Solvent: DCM, NMP; Non-solvent: Mineral oil, ethanol; Stirring rate: 200–1000 rpm; Particle sizes: 1–100 μm. | [15,82,124] |
| 3D Printing | Enables tunable porosity and implant geometry. | Techniques: Fused Deposition Modeling (FDM), Direct Ink Writing (DIW); Print temp: 150–200 °C; Layer height: 0.1–0.5 mm. | [17,28,32,59,106] |
| Spray Drying | Produces uniform microspheres; enables controlled morphology. | Inlet temp: 40–80 °C; Solvent: Ethanol/DCM; Feed rate: 2–10 mL/min; Particle size: 1–10 μm; Encapsulation efficiency: 60–95%. | [3,73,107] |
| Micromolding and Compression c | Creates precise implant geometries; reduces burst release. | Compression force: 0.5–5 kN; Molding temp: 50–70 °C; Mold sizes: 1–10 mm; Drug loading: 10–50%. | [30,55,76,100] |
| Emulsion Techniques (o/w, w/o/w) | Produces microspheres and nanospheres with sustained release. | Solvents: DCM, acetone; Stabilizers: PVA, surfactants; Mixing speed: 500–1500 rpm; Encapsulation efficiency: 70–90%; Size: 200 nm–10 μm. | [27,36,48,125,126] |
| Solvent Exchange/Precipitation | Forms in situ implants with adjustable release profiles. | Solvents: NMP, DMSO; Non-solvent: PBS or aqueous buffers; Solvent exchange controlled by injection speed (1–5 mL/min); Morphology: Porous or dense structures. | [2,12,23,54,56,127] |
| Electrospinning | Produces nanofibrous scaffolds with high surface area. | Voltage: 10–20 kV; Feed rate: 0.5–2 mL/h; Solvents: DCM/DMF blends; Fiber diameters: 50–500 nm. | [60,128,129] |
| Microparticle and Nanoparticle Preparation | Enables stability for sensitive drugs; achieves extended release. | Techniques: Solvent evaporation, emulsification; Particle sizes: 100 nm–10 μm; Encapsulation efficiency: 70–95%. | [3,24,48,130] |
| Freeze-Drying (Lyophilization) | Preserves drug stability and bioactivity. | Freezing temp: −20 to −80 °C; Vacuum: 0.1–0.3 mbar; Drying temp: 0–25 °C; Process time: 24–72 h. | [107,125] |
| Microlithography | Creates precise microstructures; supports linear release. | UV-LIGA method; Resolution: 1–50 μm; Materials: PLGA 502, photoresist masks; Aspect ratio: Up to 20:1. | [120,131] |
| In Situ Phase Inversion | Injectable depots; solvent and polymer selection critical for performance. | Solvent: NMP, DMSO; Precipitation medium: PBS; Polymer concentration: 10–30%; Pore sizes: 1–100 μm. | [9,56,58,88,127] |
| Oil/Water Emulsion Solvent Evaporation | Produces uniform microspheres; scalable manufacturing. | Solvent: DCM, acetone; Emulsifiers: PVA, PEG; Stirring: 500–1500 rpm; Microsphere sizes: 500 nm–10 μm. | [40,42,48,116,123] |
| Ultrasonic Spray Coating | Applies uniform coatings for medical devices. | Ultrasonic frequency: 20–60 kHz; Solvents: Acetone, ethanol; Coating thickness: 10–100 μm. | [94,97,102] |
| High-Energy Ball Milling | Prepares uniform platforms with bioactive components. | Rotation speed: 200–400 rpm; Milling time: 2–8 h; Ball-to-powder ratio: 10:1–20:1; Size: 10–50 μm. | [99,132] |
| Hybrid Techniques (e.g., UMAOH) | Creates multifunctional implant coatings. | Process temp: 200–400 °C; Coating thickness: 10–50 μm; Hybrid layers: PLGA/CaP or PLGA/metal nanoparticles. | [66,133] |
| Multivariate Optimization Approaches | Adjusts parameters to minimize burst release and optimize drug loading. | Box–Behnken designs; Variables: Drug–polymer ratio, solvent composition, stirring speed; Results: Optimized burst control and morphology. | [55,57,127,134] |
| USP Apparatus 4 Testing | Accelerates implant release testing; correlates real-time data. | Testing medium: PBS; Flow rate: 1–10 mL/min; Temp: 37 °C; Testing duration: 1–60 days. | [135] |
| Mathematical and Computational Modeling | Predicts release kinetics; enables optimization of implant performance. | Finite element analysis; Models: Korsmeyer–Peppas, Higuchi; Inputs: Polymer properties, drug diffusion constants. | [18,80,136] |
| Test Type and Purpose | Key Observations | Practical Insights | Refs. |
|---|---|---|---|
| In Vitro Release: Assesses release kinetics, burst effects, and sustained release using HPLC, UV-Vis, etc. | Controlled release influenced by polymer type, molecular weight, and excipients. | Facilitates development of sustained delivery formulations for long-term therapies, reducing frequent dosing. | [1,9,61] |
| Morphological Analysis: SEM, TEM, and XRD to study surface properties, porosity, and internal structure. | Porosity and morphology directly affect drug diffusion and polymer degradation. | Guides design of implants with controlled release rates and predictable degradation behavior. | [4,63,82] |
| Degradation and Erosion Studies: Monitors mass loss, pH changes, and polymer erosion timelines. | Polymer degradation timelines vary with composition, pH environment, and drug loading. | Enables customization of polymer blends for targeted degradation profiles aligned with therapeutic needs. | [22,25,85] |
| Biocompatibility and Safety: Histological evaluations, inflammatory markers, and cytotoxicity assays. | Low inflammatory responses observed for optimized formulations; reduced toxicity in vivo. | Confirms safety and acceptance for clinical applications while minimizing adverse reactions. | [50,104,154] |
| Pharmacokinetics (PK): Monitors drug absorption, bioavailability, and systemic exposure in animal models. | Sustained therapeutic drug levels achieved with minimal burst effects. | Verifies prolonged action and reduces systemic toxicity, enabling better compliance in chronic treatment regimens. | [26,155,156] |
| Mechanical and Stability Testing: Evaluates tensile strength, viscoelasticity, and structural integrity. | High mechanical stability correlates with effective implantation in load-bearing environments. | Provides data for designing robust implants suitable for both load-bearing and soft tissue applications. | [49,99,111] |
| Toxicology and Immunogenicity: Quantifies immune reactions and long-term toxicity using animal models. | Minimal immune response with biodegradable polymers; compatibility varies with additives. | Supports formulation strategies that prioritize both safety and efficacy, particularly for sensitive or repeated use environments. | [50,66,89] |
| Advanced Imaging and Modeling: MRI, fluorescence imaging, and finite element analysis for in situ behavior. | Imaging revealed real-time degradation, swelling behavior, and release patterns. | Enhances prediction of in vivo performance, enabling better control over therapeutic outcomes. | [74,93,132] |
| Formulation Optimization: Designs tested using factorial designs like Box–Behnken for systematic evaluation. | Statistical modeling linked drug release with injectability and solidification parameters. | Simplifies the optimization process for formulations with complex interactions between polymer and drug characteristics. | [20,55,138] |
| Drug Stability Testing: Evaluates drug integrity post-processing and during release using FTIR, DSC, and XRD. | Structural and functional stability retained for proteins and sensitive drugs like monoclonal antibodies. | Enables reliable therapeutic delivery without loss of bioactivity, critical for sensitive treatments like cancer and autoimmune therapies. | [42,125] |
| Antimicrobial Efficacy: In vitro and in vivo tests against pathogens to verify antimicrobial properties. | Sustained activity observed against S. aureus, E. coli, and MRSA; minimal bacterial adherence on implant surfaces. | Useful for designing implants with dual therapeutic and infection prevention roles, especially for orthopedic and dental applications. | [45,128] |
| Controlled Release Evaluation: Studies using diffusion kinetics, Korsmeyer–Peppas models, and Weibull fitting. | Biphasic and triphasic release profiles validated for hydrophilic and hydrophobic drugs. | Provides mechanistic insights to tailor implants for various therapeutic needs, including cancer, diabetes, and chronic pain management. | [14,121,122] |
| Histological and Micro-CT Analysis: Quantifies tissue integration and implant–host interactions. | Enhanced bone growth and soft tissue integration in optimized formulations; reduced inflammation. | Informs development of implants with improved biocompatibility and functional outcomes for musculoskeletal and dental applications. | [28,94] |
| Gene Expression and Cellular Studies: Evaluates regenerative capabilities through qPCR, histology, and immunohistochemistry. | Increased osteogenic and chondrogenic markers; enhanced tissue repair observed in scaffolds with bioactive factors. | Supports development of bioengineered implants for tissue regeneration applications in orthopedics and neurology. | [46,157] |
| Category | Expanded Proven Benefits of PLGA-Based Implants | Refs. |
|---|---|---|
| Controlled Drug Release |
| [4,6,16,68,101] |
| Enhanced Patient Compliance |
| [64,109,127,164,169] |
| Targeted Therapeutic Effects |
| [2,74,113,125,165] |
| Biocompatibility and Safety |
| [22,29,50,141,170] |
| Versatility in Drug Delivery |
| [31,42,134,137,171] |
| Surgical and Non-Surgical Use |
| [32,83,84,117,167] |
| Reduced Environmental Impact |
| [19,49,66,98,172] |
| Stability and Protein Retention |
| [34,42,53,85,173] |
| Improved Pharmacokinetics |
| [55,56,96,155,156] |
| Customization Potential |
| [94,105,106,111,116] |
| Anti-Infective Capabilities |
| [44,45,90,124,126] |
| Facilitation of Tissue Regeneration |
| [79,89,129,148,149] |
| Theranostic Applications |
| [37,72,74,93,132] |
| Cost-Effectiveness |
| [14,30,43,135,143] |
| Application Area | Specific Purposes | Drug Examples | Refs. |
|---|---|---|---|
| Drug Delivery | Sustained release of small molecules, peptides, and proteins for chronic disease management; reduces dosing frequency and enhances compliance. | Entecavir, Naltrexone, Leuprolide, Insulin, Dexamethasone, Buprenorphine | [1,15,40,53,61,127] |
| Pain Management | Prolonged release of NSAIDs, local anesthetics, or opioids for chronic and postoperative pain; supports synergy between drugs for improved efficacy. | Ibuprofen, Bupivacaine, Hydromorphone, Biphalin, Ketoprofen | [4,10,139,143,174] |
| Antibiotic Delivery | Localized infection control; prevents biofilm formation and promotes antimicrobial activity for dental and orthopedic implants. | Ciprofloxacin, Gentamicin, Chlorhexidine, Amoxicillin | [44,45,70,87,124] |
| Anti-Inflammatory Treatments | Long-term suppression of implant-related inflammation; used in neural implants, ocular devices, and implantable medical systems. | Dexamethasone, Methotrexate, Bupivacaine, Vancomycin, Spiramyin, Mitomycin C | [22,37,40,68,146,175] |
| Cancer Therapy | Localized chemotherapy with reduced systemic toxicity; combines hyperthermia and drug release for tumor ablation. | Paclitaxel, Doxorubicin, 5-Fluorouracil, Cisplatin, Carboplatin | [6,27,43,72,73,74] |
| Neuroregeneration | Promotes nerve repair, reduces glial scarring, and enhances biocompatibility for neural implants; supports spinal cord injury recovery. | Minocycline, VEGF, Anti-Nogo receptor antibody | [89,118,151,176] |
| Ophthalmology | Sustained intraocular drug delivery for conditions like glaucoma, macular degeneration, and ocular infections; supports posterior eye applications. | Dexamethasone, Clindamycin, Tacrolimus, Spiramycin | [16,39] |
| Bone Regeneration and Repair | Osseointegration in orthopedic and dental implants; supports vascularization and defect repair with biodegradable scaffolds. | Hydroxyapatite, β-TCP, VEGF | [45,65,66,67] |
| Vascular and Stroke Therapies | Stimulates vascularization for tissue repair; supports neovascularization in stroke recovery and regenerative applications. | VEGF | [28,34,36,79] |
| Cartilage and Osteochondral Repair | Regenerates articular cartilage; combines scaffolds and therapeutic agents to enhance structural integration. | Lithium ions, IGF-1 | [14,51,149,150] |
| Hormone Therapy | Provides long-acting hormone release for prostate cancer, hormonal deficiencies, and contraception; minimizes dosing intervals. | Leuprolide acetate, Risperidone, Levonorgestrel, Rilpivirine | [2,64,75,96,101,109] |
| Periodontal Applications | Localized delivery of antibiotics and anti-inflammatory agents to treat periodontitis; improves adherence and mechanical retention. | Minocycline, Chlorhexidine, Secnidazole, Doxycycline | [81,87,163,177] |
| Diabetes Management | Controlled release of hypoglycemic agents for consistent blood glucose control; minimizes peaks and troughs in drug levels. | Linagliptin, Exendin-4, Glimepiride | [48,138,156] |
| Tissue Engineering | Sustained release scaffolds for soft and hard tissue engineering; supports adipose, cartilage, and nerve tissue formation. | IGF-1, VEGF, BSA | [51,85,95,141,148] |
| Post-Surgical Infection Control | Prevents infections at surgical sites using localized antibiotic release; avoids systemic side effects and improves healing. | Amoxicillin, Gentamicin, Rifampicin | [45,58,90,97,154] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Omidian, H.; Wilson, R.L. PLGA Implants for Controlled Drug Delivery and Regenerative Medicine: Advances, Challenges, and Clinical Potential. Pharmaceuticals 2025, 18, 631. https://doi.org/10.3390/ph18050631
Omidian H, Wilson RL. PLGA Implants for Controlled Drug Delivery and Regenerative Medicine: Advances, Challenges, and Clinical Potential. Pharmaceuticals. 2025; 18(5):631. https://doi.org/10.3390/ph18050631
Chicago/Turabian StyleOmidian, Hossein, and Renae L. Wilson. 2025. "PLGA Implants for Controlled Drug Delivery and Regenerative Medicine: Advances, Challenges, and Clinical Potential" Pharmaceuticals 18, no. 5: 631. https://doi.org/10.3390/ph18050631
APA StyleOmidian, H., & Wilson, R. L. (2025). PLGA Implants for Controlled Drug Delivery and Regenerative Medicine: Advances, Challenges, and Clinical Potential. Pharmaceuticals, 18(5), 631. https://doi.org/10.3390/ph18050631