
Short-Term Outcomes of Three Consecutive Monthly Loading Administrations of Aflibercept 8 Mg for Treatment-Naïve Exudative Age-Related Macular Degeneration

 ,
, 
Abstract
1. Introduction
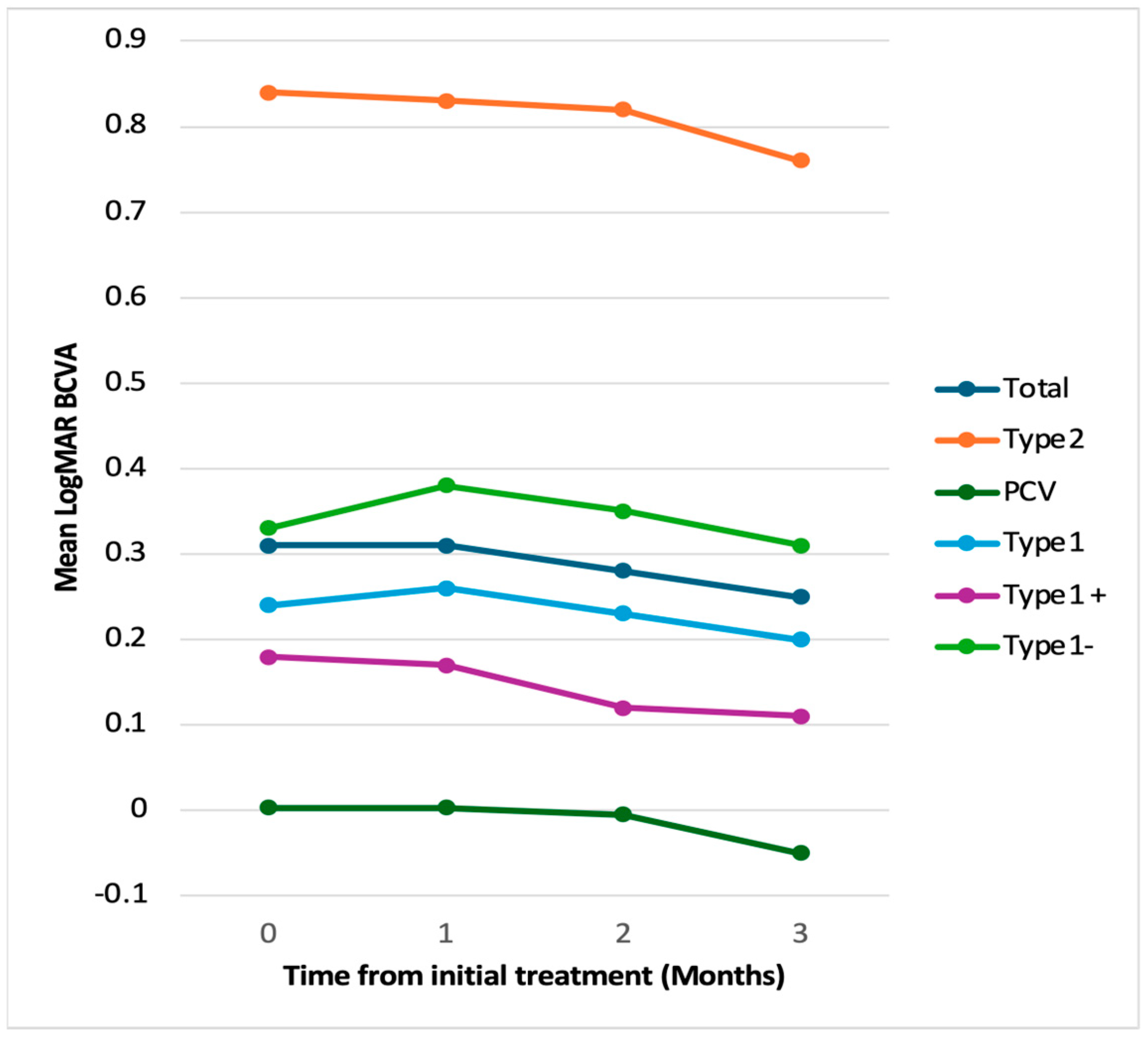
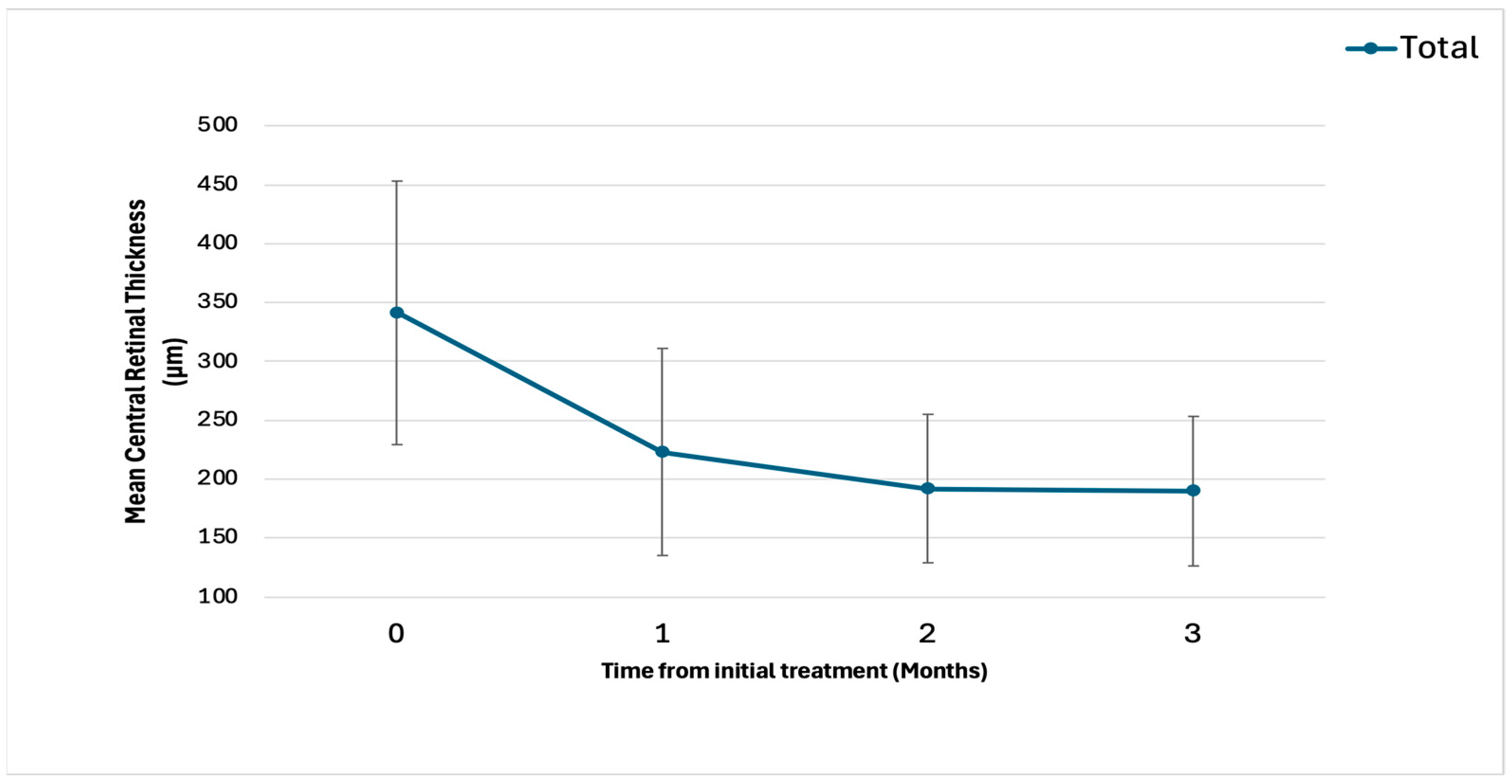
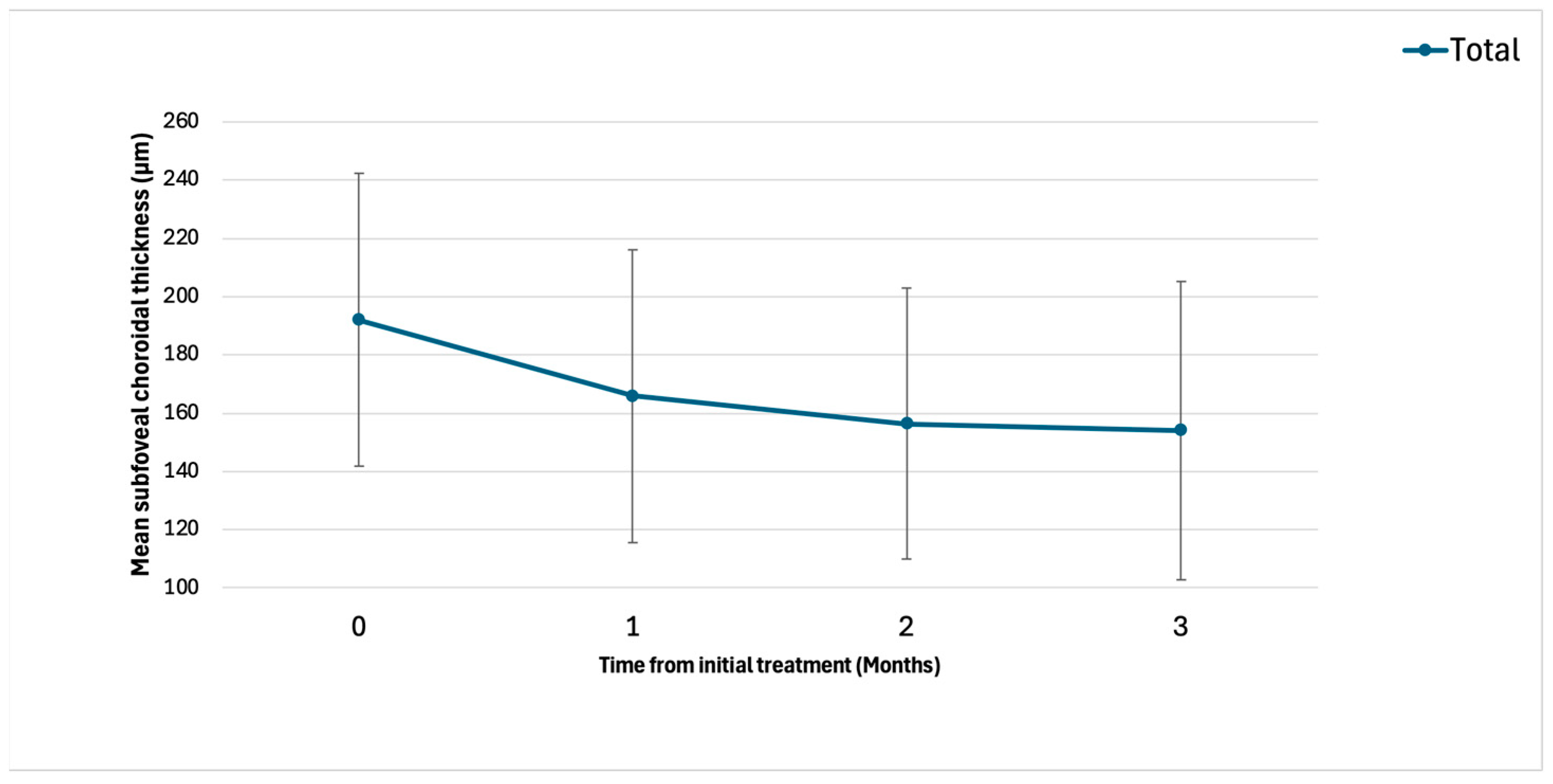
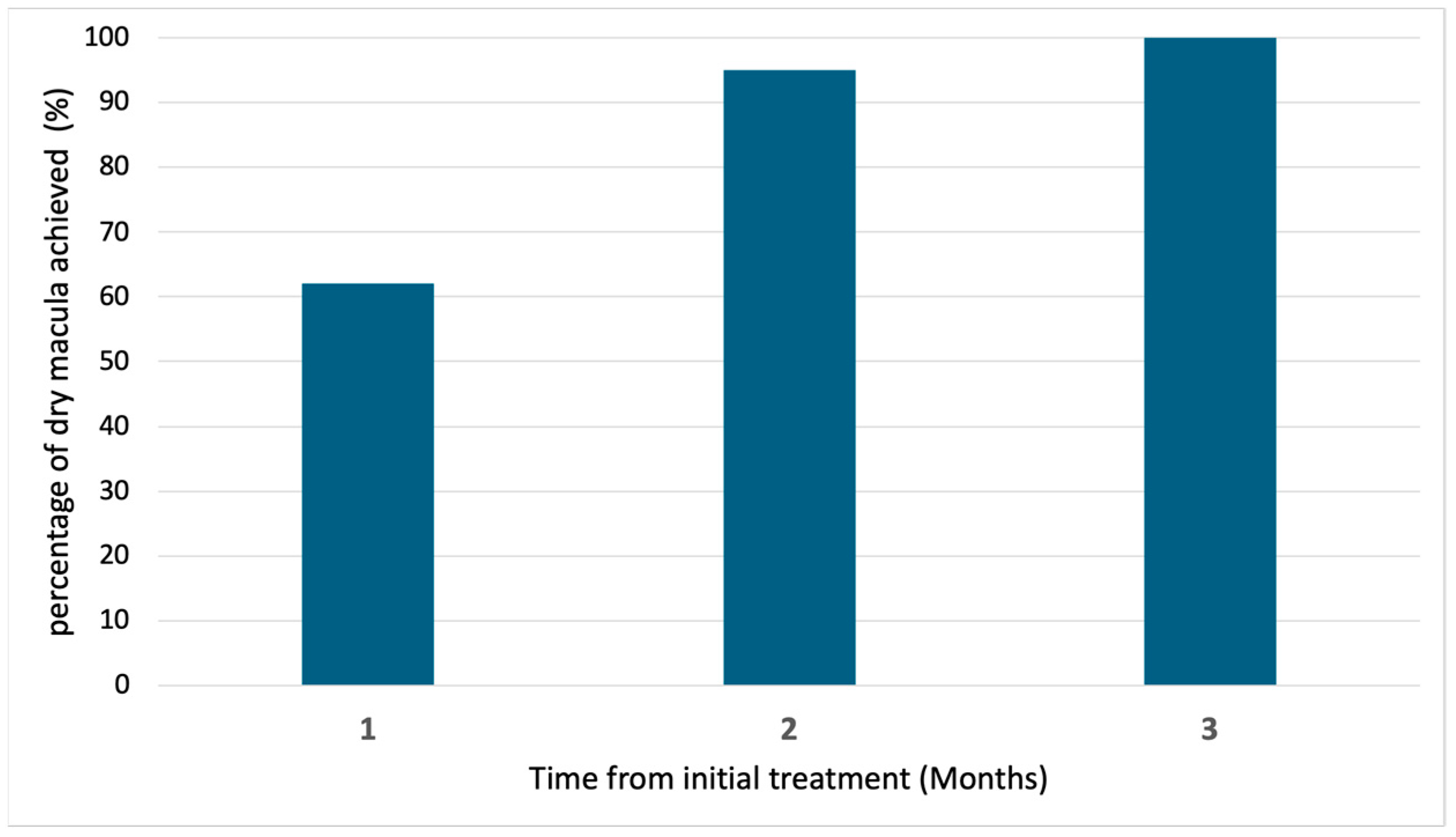
2. Results
3. Discussion
4. Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.-Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [PubMed]
- Sakurada, Y.; Tanaka, K.; Fragiotta, S. Differentiating drusen and drusenoid deposits subtypes on multimodal imaging and risk of advanced age-related macular degeneration. Jpn. J. Ophthalmol. 2023, 67, 1–13. [Google Scholar] [PubMed]
- Sasaki, M.; Kawasaki, R.; Yanagi, Y. Early Stages of Age-Related Macular Degeneration: Racial/Ethnic Differences and Proposal of a New Classification Incorporating Emerging Concept of Choroidal Pathology. J. Clin. Med. 2022, 11, 6274. [Google Scholar] [CrossRef] [PubMed]
- Sadda, S.R.; Guymer, R.; Holz, F.G.; Schmitz-Valckenberg, S.; Curcio, C.A.; Bird, A.C.; Blodi, B.A.; Bottoni, F.; Chakravarthy, U.; Chew, E.Y.; et al. Consensus Definition for Atrophy Associated with Age-Related Macular Degeneration on OCT: Classification of Atrophy Report 3. Ophthalmology 2018, 125, 537–548. [Google Scholar] [CrossRef]
- Spaide, R.F.; Jaffe, G.J.; Sarraf, D.; Freund, K.B.; Sadda, S.R.; Staurenghi, G.; Waheed, N.K.; Chakravarthy, U.; Rosenfeld, P.J.; Holz, F.G.; et al. Consensus Nomenclature for Reporting Neovascular Age-Related Macular Degeneration Data: Consensus on Neovascular Age-Related Macular Degeneration Nomenclature Study Group. Ophthalmology 2020, 127, 616–636. [Google Scholar]
- Photodynamic therapy of subfoveal choroidal neovascularization in age-related macular degeneration with verteporfin: One-year results of 2 randomized clinical trials—TAP report. Treatment of age-related macular degeneration with photodynamic therapy (TAP) Study Group. Arch. Ophthalmol. 1999, 117, 1329–1345. [Google Scholar]
- Gragoudas, E.S.; Adamis, A.P.; Cunningham, E.T., Jr.; Feinsod, M.; Guyer, D.R.; VEGF Inhibition Study in Ocular Neovascularization Clinical Trial Group. Pegaptanib for neovascular age-related macular degeneration. N. Engl. J. Med. 2004, 351, 2805–2816. [Google Scholar] [CrossRef]
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.K.; Chung, C.Y.; MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar]
- Heier, J.S.; Brown, D.M.; Chong, V.; Korobelnik, J.-F.; Kaiser, P.K.; Nguyen, Q.D.; Kirchhof, B.; Ho, A.; Ogura, Y.; Yancopoulos, G.D.; et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology 2012, 119, 2537–2548. [Google Scholar]
- Azuma, K.; Okubo, A.; Nomura, Y.; Zhou, H.; Terao, R.; Hashimoto, Y.; Asano, K.S.; Azuma, K.; Inoue, T.; Obata, R. Association between pachychoroid and long-term treatment outcomes of photodynamic therapy with intravitreal ranibizumab for polypoidal choroidal vasculopathy. Sci. Rep. 2020, 10, 8337. [Google Scholar]
- Hashimoto, Y.; Okada, A.; Matsui, H.; Yasunaga, H.; Aihara, M.; Obata, R. Recent trends in anti-vascular endothelial growth factor intravitreal injections: A large claims database study in Japan. Jpn. J. Ophthalmol. 2023, 67, 109–118. [Google Scholar]
- Kume, A.; Ohshiro, T.; Sakurada, Y.; Kikushima, W.; Yoneyama, S.; Kashiwagi, K. Treatment Patterns and Health Care Costs for Age-Related Macular Degeneration in Japan: An Analysis of National Insurance Claims Data. Ophthalmology 2016, 123, 1263–1268. [Google Scholar] [CrossRef]
- Nguyen, Q.D.; Das, A.; Do, D.V.; Dugel, P.U.; Gomes, A.; Holz, F.G.; Koh, A.; Pan, C.K.; Sepah, Y.J.; Patel, N.; et al. Brolucizumab: Evolution through Preclinical and Clinical Studies and the Implications for the Management of Neovascular Age-Related Macular Degeneration. Ophthalmology 2020, 127, 963–976. [Google Scholar]
- Dugel, P.U.; Singh, R.P.; Koh, A.; Ogura, Y.; Weissgerber, G.; Gedif, K.; Jaffe, G.J.; Tadayoni, R.; Schmidt-Erfurth, U.; Holz, F.G. HAWK and HARRIER: Ninety-Six-Week Outcomes from the Phase 3 Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2021, 128, 89–99. [Google Scholar]
- Heier, J.S.; Khanani, A.M.; Ruiz, C.Q.; Basu, K.; Ferrone, P.J.; Brittain, C.; Figueroa, M.S.; Lin, H.; Holz, F.G.; Patel, V.; et al. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): Two randomised, double-masked, phase 3, non-inferiority trials. Lancet 2022, 399, 729–740. [Google Scholar] [PubMed]
- Khanani, A.M.; Kotecha, A.; Chang, A.; Chen, S.-J.; Chen, Y.; Guymer, R.; Heier, J.S.; Holz, F.G.; Iida, T.; Ives, J.A.; et al. TENAYA and LUCERNE: Two-Year Results from the Phase 3 Neovascular Age-Related Macular Degeneration Trials of Faricimab with Treat-and-Extend Dosing in Year 2. Ophthalmology 2024, 131, 914–926. [Google Scholar] [CrossRef]
- Dugel, P.U.; Koh, A.; Ogura, Y.; Jaffe, G.J.; Schmidt-Erfurth, U.; Brown, D.M.; Gomes, A.V.; Warburton, J.; Weichselberger, A.; Holz, F.G.; et al. HAWK and HARRIER: Phase 3, Multicenter, Randomized, Double-Masked Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2020, 127, 72–84. [Google Scholar] [PubMed]
- Lanzetta, P.; Korobelnik, J.-F.; Heier, J.S.; Leal, S.; Holz, F.G.; Clark, W.L.; Eichenbaum, D.; Iida, T.; Xiaodong, S.; Berliner, A.J.; et al. Intravitreal aflibercept 8 mg in neovascular age-related macular degeneration (PULSAR): 48-week results from a randomised, double-masked, non-inferiority, phase 3 trial. Lancet 2024, 403, 1141–1152. [Google Scholar] [CrossRef]
- Ghezala, I.B.; Gabrielle, P.-H.; Sibert, M.; Steinberg, L.-A.; Dautriche, A.; Arnould, L.; Creuzot-Garcher, C. Severe Intraocular Inflammation After Intravitreal Injection of Faricimab: A Single-Site Case Series of Six Patients. Am. J. Ophthalmol. 2025, 269, 11–19. [Google Scholar] [PubMed]
- Montesel, A.; Sen, S.; Preston, E.; Patel, P.J.; Huemer, J.; Hamilton, R.D.; Nicholson, L.; Papasavvas, I.; Tucker, W.R.; Yeung, I. Intraocular Inflammation (IOI) Associated with Faricimab Therapy: One-year Real World Outcomes. Retina 2025. ahead of print. [Google Scholar] [CrossRef]
- Bruening, W.; Kim, S.; Yeh, S.; Rishi, P.; Conrady, C.D. Inflammation and Occlusive Retinal Vasculitis Post Faricimab. JAMA Ophthalmol. 2025. ahead of print. [Google Scholar] [CrossRef]
- Baumal, C.R.; Bodaghi, B.; Singer, M.; Tanzer, D.J.; Seres, A.; Joshi, M.R.; Feltgen, N.; Gale, R. Expert Opinion on Management of Intraocular Inflammation, Retinal Vasculitis, and Vascular Occlusion after Brolucizumab Treatment. Ophthalmol. Retin. 2021, 5, 519–527. [Google Scholar]
- Fukuda, Y.; Sakurada, Y.; Matsubara, M.; Kotoda, Y.; Kasai, Y.; Sugiyama, A.; Kashiwagi, K. Comparison of one-year outcomes between as-needed brolucizumab and aflibercept for polypoidal choroidal vasculopathy. Jpn. J. Ophthalmol. 2023, 67, 402–409. [Google Scholar] [PubMed]
- Matsumoto, H.; Hoshino, J.; Nakamura, K.; Nagashima, T.; Akiyama, H. Short-term outcomes of intravitreal faricimab for treatment-naive neovascular age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 2023, 261, 2945–2952. [Google Scholar] [PubMed]
- Mukai, R.; Kataoka, K.; Tanaka, K.; Miyara, Y.; Maruko, I.; Nakayama, M.; Watanabe, Y.; Yamamoto, A.; Wakatsuki, Y.; Onoe, H.; et al. Three-month outcomes of faricimab loading therapy for wet age-related macular degeneration in Japan. Sci. Rep. 2023, 13, 8747. [Google Scholar]
- Allehyani, M.H.; Alsaeedi, A.K.; Alqthmi, R.O.; Saleh, R.E.; Alsamli, R.S.; Almalki, H.A.; Alshehri, A.F.; Felimban, S.A.; Kambiji, G.J.; Almatrafi, M.I.; et al. Comparative Efficacy of Brolucizumab and Aflibercept in Polypoidal Choroidal Vasculopathy: A Systematic Review and Meta-Analysis. Cureus 2025, 17, e77073. [Google Scholar]
- Kimura, M.; Sakurada, Y.; Fukuda, Y.; Matsubara, M.; Kotoda, Y.; Kasai, Y.; Sugiyama, A.; Kikushima, W.; Tsuru, D.V.; Kashiwagi, K. Association of Polyp Regression after Loading Phase with 12-Month Outcomes of Eyes with Polypoidal Choroidal Vasculopathy. Pharmaceuticals 2024, 17, 687. [Google Scholar] [CrossRef]
- Sayanagi, K.; Fujimoto, S.; Hara, C.; Fukushima, Y.; Maruyama, K.; Kawasaki, R.; Sato, S.; Nishida, K. Effect of polyp regression and reduction on treatment efficacy in polypoidal choroidal vasculopathy treated with aflibercept. Sci. Rep. 2024, 14, 1833. [Google Scholar]
- Ferrara, N.; Mass, R.D.; Campa, C.; Kim, R. Targeting VEGF-A to treat cancer and age-related macular degeneration. Annu. Rev. Med. 2007, 58, 491–504. [Google Scholar]
- Kikushima, W.; Sakurada, Y.; Fukuda, Y.; Matsubara, M.; Yoneyama, S.; Shijo, T.; Sugiyama, A.; Kotoda, Y.; Kashiwagi, K. Incidence And Characteristics Of Neovascular Age-Related Macular With Over A 12-Month Remission After Three Monthly Aflibercept Administration: 60 Months Results of a Pro Re Nata Regimen. Retina 2024, 44, 498–505. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (N = 21) | Values |
|---|---|
| Age (years) | 75 ± 9.9 |
| Sex Male/Female (%) | 11 (52)/10 (48) |
| R/L (%) | 7 (33)/14 (67) |
| Phakia/IOL (%) | 16 (76)/5 (24) |
| BCVA (logMAR) | 0.31 ± 0.38 |
| CRT (μm) | 341 ± 112 |
| SCT (μm) | 192 ± 50 |
| Type1 MNV/Type2 MNV/PCV (%) | 11 (52)/4 (19)/6 (29) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosoda, S.; Sakurada, Y.; Fukuda, Y.; Kotoda, Y.; Kikushima, W.; Kashiwagi, K. Short-Term Outcomes of Three Consecutive Monthly Loading Administrations of Aflibercept 8 Mg for Treatment-Naïve Exudative Age-Related Macular Degeneration. Pharmaceuticals 2025, 18, 438. https://doi.org/10.3390/ph18030438
Hosoda S, Sakurada Y, Fukuda Y, Kotoda Y, Kikushima W, Kashiwagi K. Short-Term Outcomes of Three Consecutive Monthly Loading Administrations of Aflibercept 8 Mg for Treatment-Naïve Exudative Age-Related Macular Degeneration. Pharmaceuticals. 2025; 18(3):438. https://doi.org/10.3390/ph18030438
Chicago/Turabian StyleHosoda, Shuhei, Yoichi Sakurada, Yoshiko Fukuda, Yumi Kotoda, Wataru Kikushima, and Kenji Kashiwagi. 2025. "Short-Term Outcomes of Three Consecutive Monthly Loading Administrations of Aflibercept 8 Mg for Treatment-Naïve Exudative Age-Related Macular Degeneration" Pharmaceuticals 18, no. 3: 438. https://doi.org/10.3390/ph18030438
APA StyleHosoda, S., Sakurada, Y., Fukuda, Y., Kotoda, Y., Kikushima, W., & Kashiwagi, K. (2025). Short-Term Outcomes of Three Consecutive Monthly Loading Administrations of Aflibercept 8 Mg for Treatment-Naïve Exudative Age-Related Macular Degeneration. Pharmaceuticals, 18(3), 438. https://doi.org/10.3390/ph18030438