
The Influence of Dapagliflozin on Foot Microcirculation in Patients with Type 2 Diabetes with and without Peripheral Arterial Disease—A Pilot Study


 ,
,
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
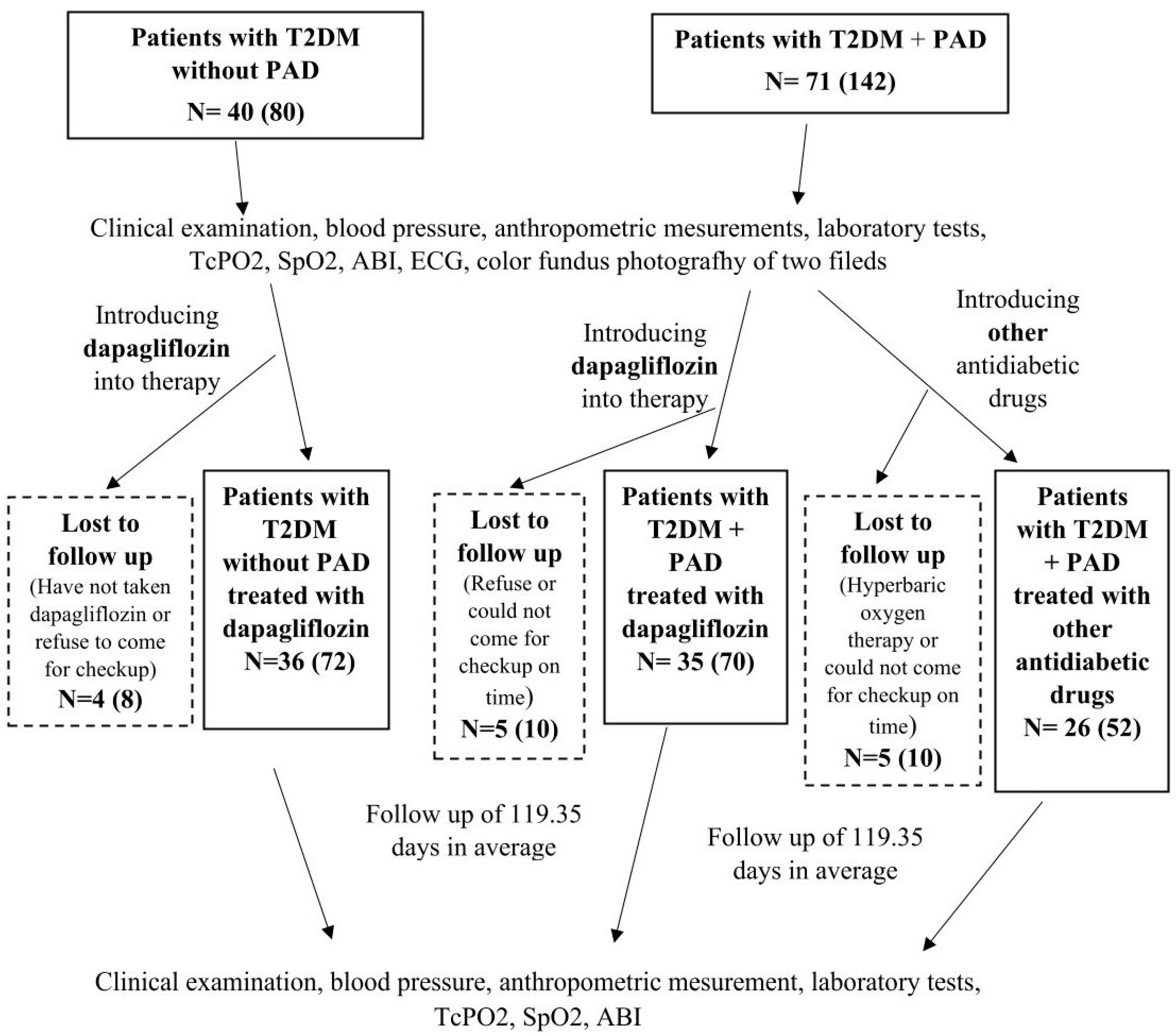
4.1. Study Design and Subjects
4.2. Data Collection
4.3. Diagnosis of Peripheral Arterial Disease
4.4. Microcirculation Assessment—Transcutaneous Oxygen Pressure Measurement
4.5. Ankle Brachial Index
4.6. Fundus Photography
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gregg, E.W.; Sorlie, P.; Paulose-Ram, R.; Gu, Q.; Eberhardt, M.S.; Wolz, M.; Burt, V.; Curtin, L.; Engelgau, M.; Geiss, L. 1999–2000 national health and nutrition examination survey. Prevalence of lower-extremity disease in the US adult population ≥ 40 years of age with and without diabetes: 1999–2000 national health and nutrition examination survey. Diabetes Care 2004, 27, 1591–1597. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.L.; Zhu, L.Y.; Han, R.; Sun, L.L.; Li, J.X.; Dou, J.T. Pathophysiology of peripheral arterial disease in diabetes mellitus. J. Diabetes 2016, 9, 133–140. [Google Scholar] [CrossRef]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119, Erratum in Diabetes Res. Clin. Pract. 2023, 204, 110945. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- E Reiber, G.; Vileikyte, L.; Boyko, E.J.; del Aguila, M.; Smith, D.G.; A Lavery, L.; Boulton, A.J. Causal pathways for incident lower-extremity ulcers in patients with diabetes from two settings. Diabetes Care 1999, 22, 157–162. [Google Scholar] [CrossRef]
- Hinchliffe, R.J.; Andros, G.; Apelqvist, J.; Bakker, K.; Fiedrichs, S.; Lammer, J.; Lepantalo, M.; Mills, J.L.; Reekers, J.; Shearman, C.P.; et al. A systematic review of the effectiveness of revascularization of the ulcerated foot in patients with diabetes and peripheral arterial disease. Diabetes/Metab. Res. Rev. [CrossRef]
- Boulton, A.J.M. The diabetic foot. Preface. Med. Clin. N. Am. 2013, 97, 775–992. [Google Scholar] [CrossRef]
- Stoberock, K.; Kaschwich, M.; Nicolay, S.S.; Mahmoud, N.; Heidemann, F.; Rieß, H.C.; Debus, E.S.; Behrendt, C.-A. The interrelationship between diabetes mellitus and peripheral arterial disease. Vasa 2021, 50, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Mauricio, D.; Gratacòs, M.; Franch-Nadal, J. Diabetic microvascular disease in non-classical beds: The hidden impact beyond the retina, the kidney, and the peripheral nerves. Cardiovasc. Diabetol. 2023, 22, 314. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Deng, H.; Li, B.; Shen, Q.; Zhang, C.; Kuang, L.; Chen, R.; Wang, S.; Ma, Z.; Li, G. Mechanisms of diabetic foot ulceration: A review. J. Diabetes 2023, 15, 299–312. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fife, C.E.; Smart, D.R.; Sheffield, P.J.; Hopf, H.W.; Hawkins, G.; Clarke, D. Transcutaneous oximetry in clinical practice: Con-sensus statements from an expert panel based on evidence. Undersea Hyperb. Med. 2009, 36, 43–53. [Google Scholar]
- Larsen, J.F.; Christensen, K.S.; Egeblad, K. Transcutaneous oxygen tension exercise profile. A method for objectively assessing the results after reconstructive peripheral arterial surgery. Eur. J. Vasc. Surg. 1988, 2, 377–381. [Google Scholar] [CrossRef]
- Rooke, T.W. The use of transcutaneous oximetry in the noninvasive vascular laboratory. Int. Angiol. 1992, 11, 36–40. [Google Scholar] [PubMed]
- de Graaff, J.C.; Ubbink, D.T.; Legemate, D.A.; de Haan, R.J.; Jacobs, M.J. Interobserver and intraobserver reproducibility of peripheral blood and oxygen pressure measurements in the assessment of lower extremity arterial disease. J. Vasc. Surg. 2001, 33, 1033–1040. [Google Scholar] [CrossRef]
- Sprenger, L.; Mader, A.; Larcher, B.; Mächler, M.; Vonbank, A.; Zanolin-Purin, D.; Leiherer, A.; Muendlein, A.; Drexel, H.; Saely, C.H. Type 2 diabetes and the risk of cardiovascular events in peripheral artery disease versus coronary artery disease. BMJ Open Diabetes Res. Care 2021, 9, e002407. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee; ElSayed, N.A.; Aleppo, G.; Bannuru, R.R.; Bruemmer, D.; Collins, B.S.; Ekhlaspour, L.; Gaglia, J.L.; Hilliard, M.E.; Johnson, E.L.; et al. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes—2024. Diabetes Care 2023, 47 (Suppl. S1), S158–S178. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Bonaca, M.P.; Wiviott, S.D.; Zelniker, T.A.; Mosenzon, O.; Bhatt, D.L.; Leiter, L.A.; McGuire, D.K.; Goodrich, E.L.; Furtado, R.H.D.M.; Wilding, J.P.; et al. Dapagliflozin and Cardiac, Kidney, and Limb Outcomes in Patients with and Without Peripheral Artery Disease in DECLARE-TIMI 58. Circulation 2020, 142, 734–747. [Google Scholar] [CrossRef]
- Chertow, G.M.; Correa-Rotter, R.; Vart, P.; Jongs, N.; McMurray, J.J.V.; Rossing, P.; Langkilde, A.M.; Sjöström, C.D.; Toto, R.D.; Wheeler, D.C.; et al. Effects of Dapagliflozin in Chronic Kidney Disease, With and Without Other Cardiovascular Medications: DAPA-CKD Trial. J. Am. Hear. Assoc. 2023, 12, e028739. [Google Scholar] [CrossRef]
- The EMPA-KIDNEY Collaborative Group; Herrington, W.G.; Staplin, N.; Wanner, C.; Green, J.B.; Hauske, S.J.; Emberson, J.R.; Preiss, D.; Judge, P.; Mayne, K.J.; et al. Empagliflozin in Patients with Chronic Kidney Disease. N. Engl. J. Med. 2023, 388, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; DeMets, D.L.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Langkilde, A.M.; Martinez, F.A.; Bengtsson, O.; Ponikowski, P.; Sabatine, M.S.; et al. A trial to evaluate the effect of the sodium–glucose co-transporter 2 inhibitor dapagliflozin on morbidity and mortality in patients with heart failure and reduced left ventricular ejection fraction (DAPA-HF). Eur. J. Heart Fail. 2019, 21, 665–675. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Burke, D.T.; Armour, D.J.; McCargo, T.; Al-Adawi, S. Change over time of the ankle brachial index. Wound Med. 2019, 28, 100174. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee; ElSayed, N.A.; Aleppo, G.; Bannuru, R.R.; Bruemmer, D.; Collins, B.S.; Das, S.R.; Ekhlaspour, L.; Hilliard, M.E.; Johnson, E.L.; et al. 10. Cardiovascular Disease and Risk Management: Standards of Care in Diabetes—2024. Diabetes Care 2023, 47 (Suppl. S1), S179–S218. [Google Scholar] [CrossRef]
- Forxiga 10 mg Film-Coated Tablets (07 March 2024). Available online: https://www.medicines.org.uk/emc/product/7607/smpc (accessed on 30 May 2024).
- Jardiance 10 mg Film-Coated Tablets, (14 September 2023). Available online: https://www.medicines.org.uk/emc/product/5441/smpc#gref (accessed on 30 May 2024).
- Kalani, M.; Brismar, K.; Fagrell, B.; Ostergren, J.; Jörneskog, G. Transcutaneous oxygen tension and toe blood pressure as predictors for outcome of diabetic foot ulcers. Diabetes Care 1999, 22, 147–151. [Google Scholar] [CrossRef]
- Bulum, T.; Brkljačić, N.; Ivančić, A.T.; Čavlović, M.; Prkačin, I.; Tomić, M. In Association with Other Risk Factors, Smoking Is the Main Predictor for Lower Transcutaneous Oxygen Pressure in Type 2 Diabetes. Biomedicines 2024, 12, 381. [Google Scholar] [CrossRef]
- Bacharach, J.M.; Rooke, T.W.; Osmundson, P.J.; Gloviczki, P. Predictive value of transcutaneous oxygen pressure and amputation success by use of supine and elevation measurements. J. Vasc. Surg. 1992, 15, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Ott, C.; Jumar, A.; Striepe, K.; Friedrich, S.; Karg, M.V.; Bramlage, P.; Schmieder, R.E. A randomised study of the impact of the SGLT2 inhibitor dapagliflozin on microvascular and macrovascular circulation. Cardiovasc. Diabetol. 2017, 16, 26. [Google Scholar] [CrossRef]
- Sposito, A.C.; Breder, I.; Soares, A.A.S.; Kimura-Medorima, S.T.; Munhoz, D.B.; Cintra, R.M.R.; Bonilha, I.; Oliveira, D.C.; Breder, J.C.; Cavalcante, P.; et al. Dapagliflozin effect on endothelial dysfunction in diabetic patients with atherosclerotic disease: A randomized active-controlled trial. Cardiovasc. Diabetol. 2021, 20, 74. [Google Scholar] [CrossRef] [PubMed]
- Shigiyama, F.; Kumashiro, N.; Miyagi, M.; Ikehara, K.; Kanda, E.; Uchino, H.; Hirose, T. Effectiveness of dapagliflozin on vascular endothelial function and glycemic control in patients with early-stage type 2 diabetes mellitus: DEFENCE study. Cardiovasc. Diabetol. 2017, 16, 84. [Google Scholar] [CrossRef]
- Solini, A.; Giannini, L.; Seghieri, M.; Vitolo, E.; Taddei, S.; Ghiadoni, L.; Bruno, R.M. Dapagliflozin acutely improves endothelial dysfunction, reduces aortic stiffness and renal resistive index in type 2 diabetic patients: A pilot study. Cardiovasc. Diabetol. 2017, 16, 138. [Google Scholar] [CrossRef] [PubMed]
- Zainordin, N.A.; Hatta, S.F.W.M.; Shah, F.Z.M.; Rahman, T.A.; Ismail, N.; Ismail, Z.; Ghani, R.A. Effects of Dapagliflozin on Endothelial Dysfunction in Type 2 Diabetes with Established Ischemic Heart Disease (EDIFIED). J. Endocr. Soc. 2019, 4, bvz017. [Google Scholar] [CrossRef] [PubMed]
- Sorop, O.; Olver, T.D.; van de Wouw, J.; Heinonen, I.; van Duin, R.W.; Duncker, D.J.; Merkus, D. The microcirculation: A key player in obesity-associated cardiovascular disease. Cardiovasc. Res. 2017, 113, 1035–1045. [Google Scholar] [CrossRef] [PubMed]
- Andreieva, I.O.; Riznyk, O.I.; Myrnyi, S.P.; Surmylo, N.N. State of Cutaneous Microcirculation in Patients with Obesity. Wiad. Lek. 2021, 74, 2039–2043. [Google Scholar] [CrossRef] [PubMed]
- Sano, M.; Goto, S. Possible Mechanism of Hematocrit Elevation by Sodium Glucose Cotransporter 2 Inhibitors and Associated Beneficial Renal and Cardiovascular Effects. Circulation 2019, 139, 1985–1987. [Google Scholar] [CrossRef]
- Avogaro, A.; Kreutzenberg, S.; Fadini, G. Dipeptidyl-peptidase 4 inhibition: Linking metabolic control to cardiovascular protection. Curr. Pharm. Des. 2014, 20, 2387–2394. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jahn, L.A.; Hartline, L.; Liu, Z.; Barrett, E.J. Metformin improves skeletal muscle microvascular insulin resistance in metabolic syndrome. Am. J. Physiol. Endocrinol. Metab. 2021, 322, E173–E180. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Qiao, X.; Li, Y.; Zhou, T.; Edwards, P.A.; Gao, H. Metformin improves retinal capillary perfusion in diabetic mice. Investig. Ophthalmol. Vis. Sci. 2018, 59, 3591. [Google Scholar]
- Schönborn, M.; Gregorczyk-Maga, I.; Batko, K.; Bogucka, K.; Maga, M.; Płotek, A.; Pasieka, P.; Słowińska-Solnica, K.; Maga, P. Circulating Angiogenic Factors and Ischemic Diabetic Foot Syndrome Advancement—A Pilot Study. Biomedicines 2023, 11, 1559. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics of All Patients (n = 97) | |||||
|---|---|---|---|---|---|
| Without Peripheral Artery | Disease With Peripheral Artery Disease | ||||
| n = 36 | n = 61 | ||||
| Dapagliflozin | Dapagliflozin n = 35 | Other Antidiabetics n = 26 | p Value Group 2 vs. 3 | p Value All Groups | |
| Age, median | 67.5 | 70 | 71.5 | p = 0.780 | p = 0.817 |
| Female sex (n) | 10 | 8 | 7 | p = 0.770 | p = 0.877 |
| Body mass index, mean (SD) | 30.387 (5.717) | 28.999 (7.453) | 26.571 (3.742) | p = 0.0075 | p = 0.012 |
| History hypertension, (n) (%) | 31 (31.96) | 34 (35.05) | 23 (23.71) | p = 0.303 | p = 0.290 |
| History hyperlipidemia, n (%) | 30 (30.93) | 33 (34.02) | 17 (17.53) | p = 0.006 | p = 0.015 |
| History diabetic polyneuropathy, n (%) | 16 (16.46) | 29 (29.90) | 22 (22.68) | p = 1 | p = 0.001 |
| History diabetic retinopathy, n (%) | 7 (7.22) | 14 (14.43) | 8 (8.29) | p = 0.459 | p = 0.166 |
| Smoker, n (%) | 16 (16.49) | 26 (26.80) | 20 (20.62) | p = 0.813 | p = 0.009 |
| Hemoglobin A1c mean (SD), | 7.350 (1.289) | 7.314 (1.506) | 7.062 (1.452) | p = 0.320 | p = 0.200 |
| Duration of diabetes mellitus, (y) mean (SD) | 8.694 (7.920) | 16.829 (9.724) | 12.462 (7.393) | p = 0.248 | p = 0.216 |
| Estimated GFR (CKD-EPI) mL/min/1.73 m2, n (%) | 79.028 (19.191) | 73.400 (18.753) | 73.692 (22.922) | p = 0.455 | p = 0.476 |
| History of ischemic heart disease, n (%) | 3 (3.09) | 14 (14.43) | 6 (6.19) | p = 0.164 | p = 0.006 |
| History of myocardial infarction, n (%) | 1 (1.03) | 11 (11.34) | 4 (4.12) | p = 0.230 | p = 0.004 |
| History of cerebrovascular disease, n (%) | 4 (4.12) | 17 (17.53) | 13 (13.4) | p = 0.912 | p = 0.001 |
| History of cerebral infarction, n (%) | 3 (3.09) | 7 (7.22) | 5 (5.15) | p = 0.940 | p = 0.314 |
| Antiaggregation and/or anticoagulation therapy, n (%) | 9 (9.28) | 32 (32.99) | 21 (21.65) | p = 0.268 | p = 0.001 |
| Lipid-lowering therapy, n (%) | 27 (27.84) | 27 (27.84) | 13 (13.40) | p = 0.027 | p = 0.048 |
| ACE inhibitor or ARB therapy, n (%) | 27 (27.84) | 31 (31.96) | 19 (19.59) | p = 0.179 | p = 0.242 |
| Peripheral artery disease history | |||||
| Previous peripheral revascularization (endovascular or surgical), n (%) | 24 (24.74) | 17 (17.52) | p = 0.796 | ||
| Previous amputation, n (%) | 9 (9.28) | 1 (1.03) | p = 0.034 | ||
| Fontaine Classification at randomization | |||||
| Stage I: Asymptomatic, n (%) | 7 (11.48) | 1 (1.64) | p = 0.081 | ||
| Stage II: Claudication, n (%) | 21 (34.43) | 22 (36.07) | |||
| Stage III: Ischemia rest pain, n (%) | 0 | 0 | |||
| Stage IV: Ulceration or gangrene, n (%) | 7 (11.48) | 3 (4.92) | p > 0.05 | ||
| SINBAD score | 2.42 | 3 | |||
| Ankle Brachial index category/leg | |||||
| <0.9, n (%) | 0 | 14 (11.20) | 9 (7.20) | p = 0.958 | p = 0.001 |
| ≥0.9, n (%) | 63 | 24 (19.20) | 15 (12.0) | ||
| Transcutaneous oxygen pressure category/leg, mean, mm Hg | 51.292 (11.150) | 46.200 (10.774) | 43.404 (9.828) | p = 0.082 | p = 0.002 |
| No PAD + DAPAGLIFLOZIN (1) | PAD + DAPAGLIFLOZIN (2) | PAD + Other Antidiabetic Drugs (3) | p Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1–2 | 1–3 | 2–3 | ||||||||
| mean | sd | mean | sd | mean | sd | |||||
| BMI (kg/m2) | baseline | 30.387 | 5.717 | 28.999 | 7.453 | 26.571 | 3.742 | 0.354 | 0.002 | 0.0075 |
| follow up | 29.936 | 5.508 | 28.604 | 7.671 | 26.573 | 3.603 | 0.326 | 0.010 | 0.029 | |
| HbA1c (%) | baseline | 7.350 | 1.289 | 7.314 | 1.506 | 7.062 | 1.452 | 0.362 | 0.165 | 0.320 |
| follow up | 6.747 | 0.586 | 6.786 | 0.938 | 6.815 | 1.215 | 0.286 | 0.246 | 0.430 | |
| Glucose fasting (mmol/L) | baseline | 8.194 | 1.779 | 9.231 | 2.603 | 8.064 | 2.073 | 0.005 | 0.380 | 0.040 |
| follow up | 8.036 | 1.620 | 7.777 | 1.478 | 8.588 | 2.811 | 0.276 | 0.473 | 0.318 | |
| Hematocrit (L/L) | baseline | 0.431 | 0.003 | 0.419 | 0.035 | 0.424 | 0.037 | 0.077 | 0.414 | 0.401 |
| follow up | 0.447 | 0.032 | 0.429 | 0.033 | 0.412 | 0.043 | 0.016 | 0.001 | 0.059 | |
| Hemoglobin (g/L) | baseline | 145.944 | 13.852 | 135.614 | 27.125 | 140.038 | 12.032 | 0.009 | 0.018 | 0.471 |
| follow up | 149.917 | 13.693 | 142.371 | 11.971 | 136.808 | 14.006 | 0.001 | 0.001 | 0.081 | |
| LDL cholesterol (mmol/L) | baseline | 2.489 | 1.146 | 2.489 | 1.162 | 2.531 | 0.995 | 0.452 | 0.462 | 0.395 |
| follow up | 2.178 | 0.933 | 1.817 | 0.936 | 1.900 | 0.940 | 0.024 | 0.061 | 0.392 | |
| Total cholesterol (mmol/L) | baseline | 4.447 | 1.325 | 4.543 | 1.367 | 4.492 | 1.322 | 0.425 | 0.437 | 0.494 |
| follow up | 4.175 | 1.250 | 3.760 | 1.041 | 4.504 | 3.749 | 0.054 | 0.108 | 0.403 | |
| Non-HDL cholesterol (mmol/L) | baseline | 3.208 | 1.248 | 3.251 | 1.337 | 3.196 | 1.185 | 0.481 | 0.475 | 0.493 |
| follow up | 2.883 | 1.064 | 2.474 | 0.983 | 2.504 | 0.967 | 0.020 | 0.05 | 0.406 | |
| HDL cholesterol (mmol/L) | baseline | 1.239 | 0.289 | 1.291 | 0.342 | 1.298 | 0.409 | 0.237 | 0.396 | 0.346 |
| follow up | 1.292 | 0.285 | 1.337 | 0.469 | 1.242 | 0.412 | 0.466 | 0.120 | 0.138 | |
| Triglycerides (mmol/L) | baseline | 1.602 | 0.692 | 1.943 | 2.364 | 1.455 | 0.740 | 0.419 | 0.106 | 0.077 |
| follow up | 1.567 | 0.770 | 1.440 | 0.591 | 1.315 | 0.683 | 0.31 | 0.031 | 0.081 | |
| C-reactive protein (mg/L) | baseline | 2.923 | 3.113 | 5.397 | 9.204 | 3.212 | 4.160 | 0.198 | 0.36 | 0.335 |
| follow up | 3.044 | 3.943 | 3.674 | 4.648 | 3.050 | 3.717 | 0.488 | 0.495 | 0.494 | |
| Creatinine (umol/L) | baseline | 85.028 | 20.740 | 89.711 | 36.187 | 89.231 | 38.998 | 0.292 | 0.438 | 0.372 |
| follow up | 85.417 | 21.089 | 100.829 | 43.377 | 91.500 | 38.801 | 0.055 | 0.431 | 0.097 | |
| GROUP | Mean/mm Hg | SD | n |
|---|---|---|---|
| 1 No PAD + dapagliflozin | 51.292 | 11.150 | 72 |
| 2 PAD + dapagliflozin | 46.200 | 10.774 | 70 |
| 3 PAD + other antidiabetic drugs | 43.404 | 9.828 | 52 |
| Total | 46.96 | 10.58 | 194 |
| GROUP | Mean/mm Hg | SD | n |
|---|---|---|---|
| 1 No PAD + dapagliflozin | 49.528 | 12.238 | 72 |
| 2 PAD + dapagliflozin | 42.314 | 13.304 | 70 |
| 3 PAD + other antidiabetic drugs | 41.923 | 11.424 | 52 |
| Total | 44.58 | 12.322 | 194 |
| GROUP | Mean/mm Hg | SD | n |
|---|---|---|---|
| 1 No PAD + dapagliflozin | 1.76 | 12.93 | 72 |
| 2 PAD + dapagliflozin | 3.88 | 15.13 | 70 |
| 3 PAD + other antidiabetic drugs | 1.48 | 11.55 | 52 |
| Total | 2.4536082 | 13.41372 | 194 |
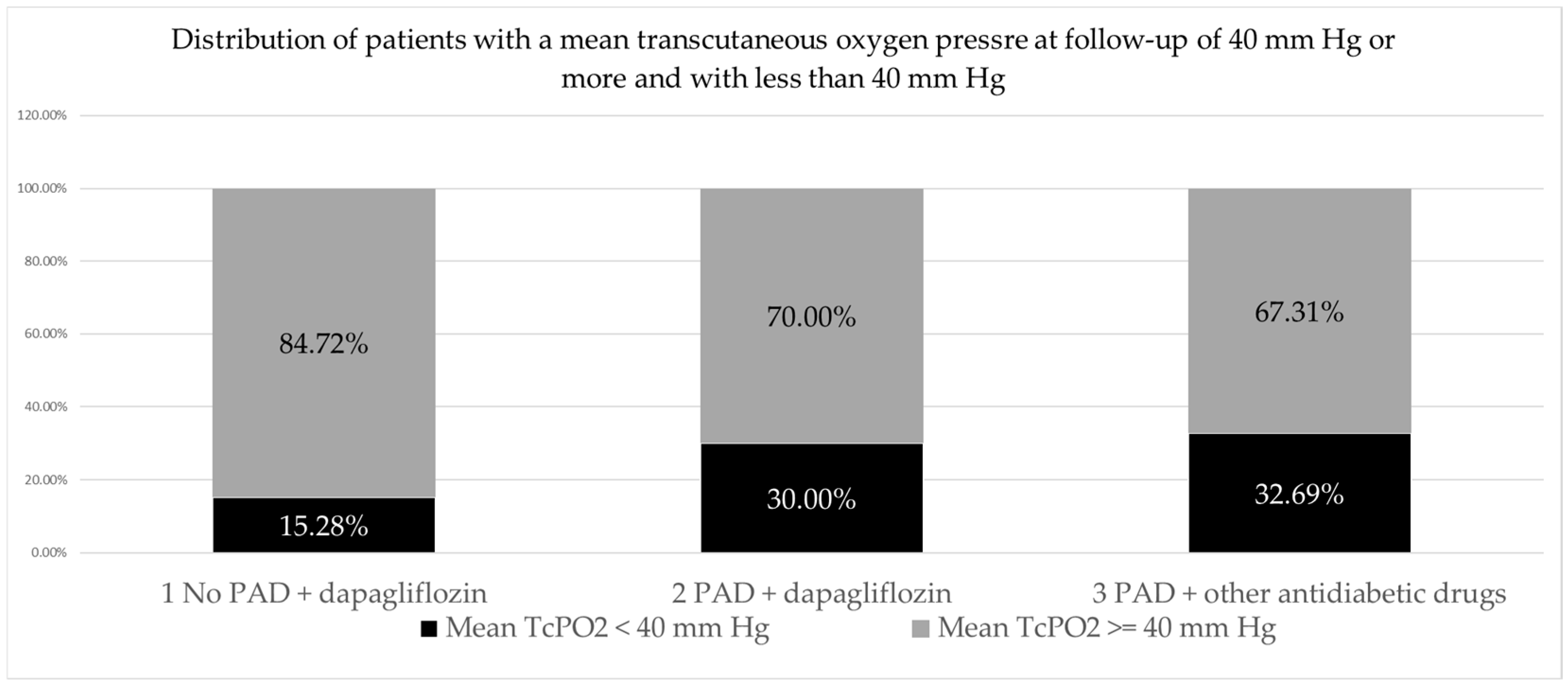
| GROUP | Mean TcPO2 < 40 mm Hg n (%) | Mean TcPO2 ≥ 40 Mm Hg n (%) | Total |
|---|---|---|---|
| 1 No PAD + dapagliflozin | 11 (15.28) | 61 (84.75) | 72 |
| 2 PAD + dapagliflozin | 21 (30) | 49 (70) | 70 |
| 3 PAD + other antidiabetic drugs | 17 (32.69) | 35 (67.31) | 52 |
| Total | 49 | 145 | 194 |
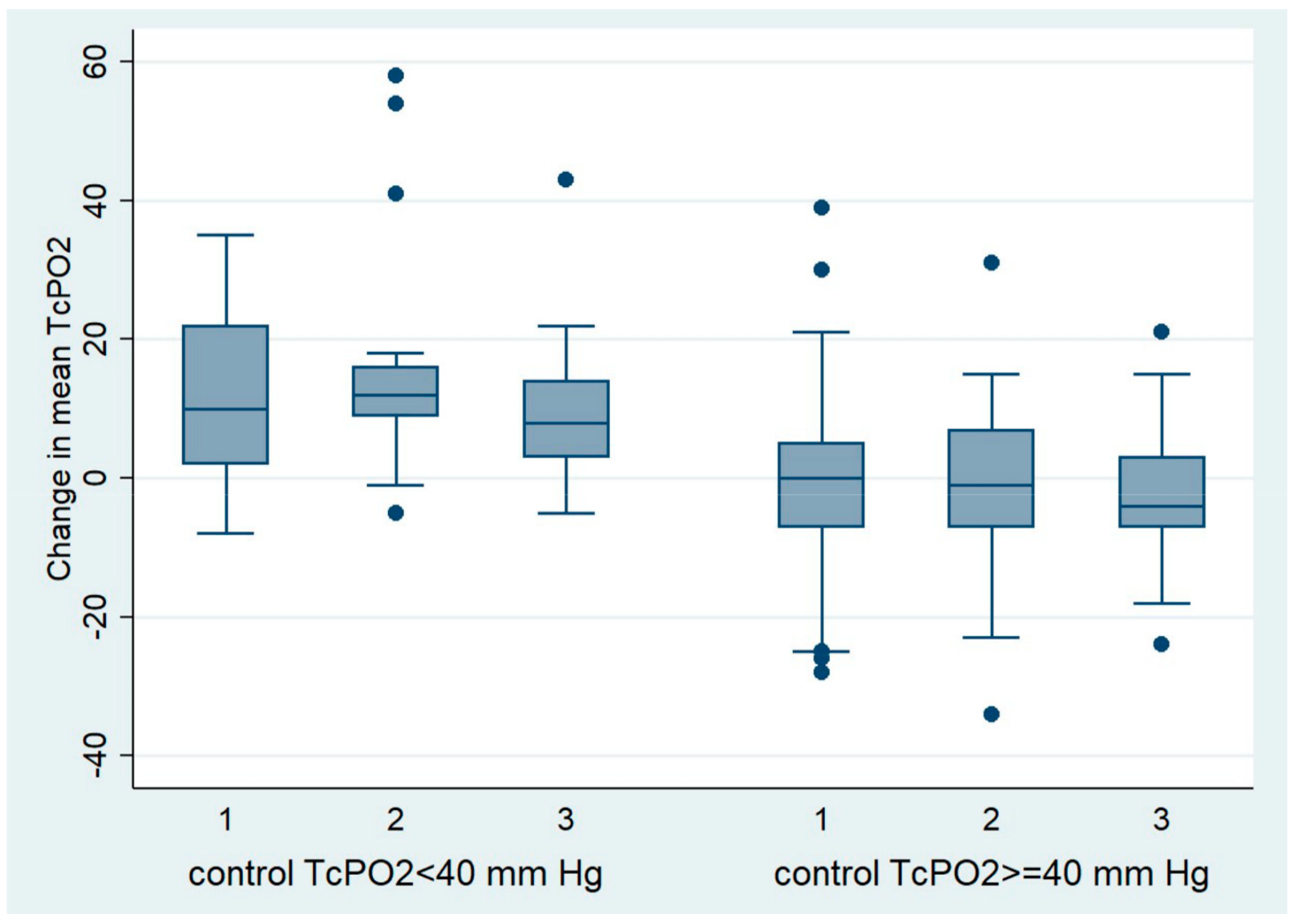
| GROUP | Mean | SD | n |
|---|---|---|---|
| 1 No PAD + dapagliflozin | 31.36 | 7.47 | 11 |
| 2 PAD + dapagliflozin | 27.71 | 11.87 | 21 |
| 3 PAD + other antidiabetic drugs | 28.70 | 9.10 | 17 |
| Total | 28.87 | 10.00 | 49 |
| GROUP | Mean | SD | n |
|---|---|---|---|
| 1 No PAD + dapagliflozin | 12.909091 | 14.046028 | 11 |
| 2 PAD + dapagliflozin | 15.809524 | 16.064305 | 21 |
| 3 PAD + other antidiabetic drugs | 9.3529412 | 11.999694 | 17 |
| Total | 12.918367 | 14.310306 | 49 |
| GROUP | Mean/mm Hg | SD | n |
|---|---|---|---|
| 1 No PAD + dapagliflozin | −0.24590164 | 11.75677 | 61 |
| 2 PAD + dapagliflozin | −1.2244898 | 11.53304 | 49 |
| 3 PAD + other antidiabetic drugs | −2.3428571 | 9.298775 | 35 |
| Total | −1.0827586 | 11.09210 | 145 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bradarić, B.; Bulum, T.; Brkljačić, N.; Mihaljević, Ž.; Benić, M.; Bradarić Lisić, B. The Influence of Dapagliflozin on Foot Microcirculation in Patients with Type 2 Diabetes with and without Peripheral Arterial Disease—A Pilot Study. Pharmaceuticals 2024, 17, 1127. https://doi.org/10.3390/ph17091127
Bradarić B, Bulum T, Brkljačić N, Mihaljević Ž, Benić M, Bradarić Lisić B. The Influence of Dapagliflozin on Foot Microcirculation in Patients with Type 2 Diabetes with and without Peripheral Arterial Disease—A Pilot Study. Pharmaceuticals. 2024; 17(9):1127. https://doi.org/10.3390/ph17091127
Chicago/Turabian StyleBradarić, Božena, Tomislav Bulum, Neva Brkljačić, Željko Mihaljević, Miroslav Benić, and Božo Bradarić Lisić. 2024. "The Influence of Dapagliflozin on Foot Microcirculation in Patients with Type 2 Diabetes with and without Peripheral Arterial Disease—A Pilot Study" Pharmaceuticals 17, no. 9: 1127. https://doi.org/10.3390/ph17091127
APA StyleBradarić, B., Bulum, T., Brkljačić, N., Mihaljević, Ž., Benić, M., & Bradarić Lisić, B. (2024). The Influence of Dapagliflozin on Foot Microcirculation in Patients with Type 2 Diabetes with and without Peripheral Arterial Disease—A Pilot Study. Pharmaceuticals, 17(9), 1127. https://doi.org/10.3390/ph17091127