
Association of Polyp Regression after Loading Phase with 12-Month Outcomes of Eyes with Polypoidal Choroidal Vasculopathy
 ,
, 
Abstract
1. Introduction
2. Results
2.1. Demographics and Clinical Characteristics
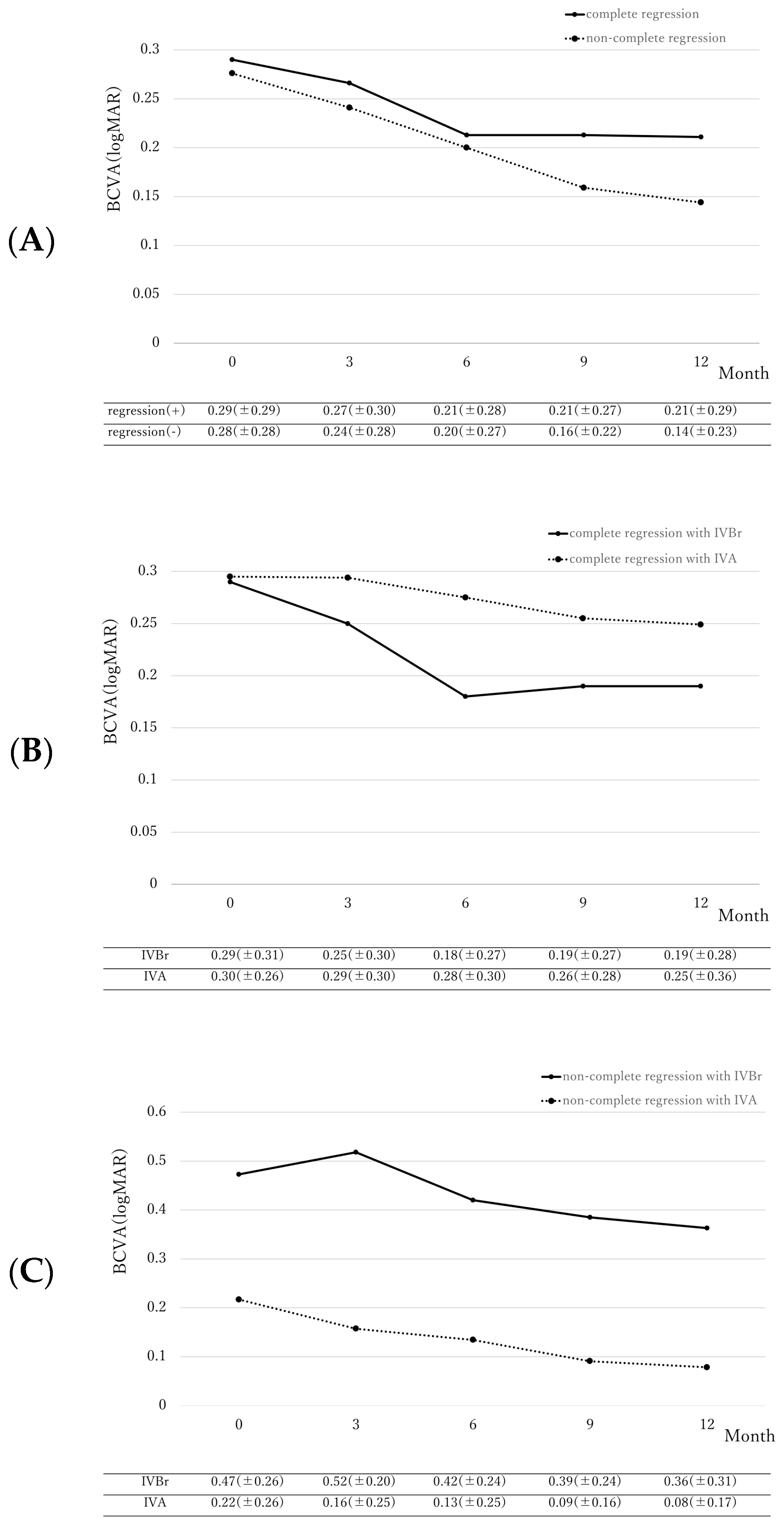
2.2. Differences in Best-Corrected Visual Acuity
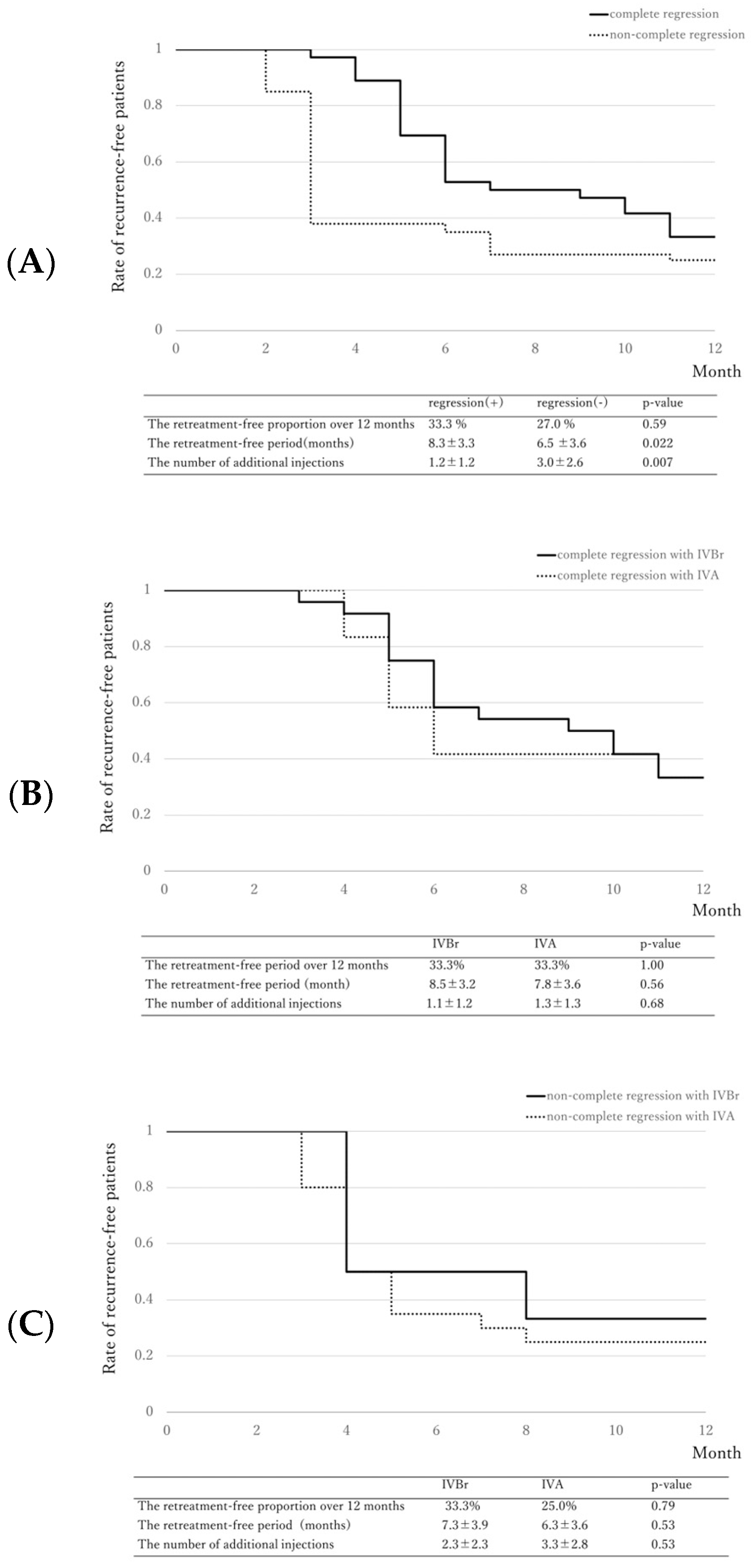
2.3. Retreatment-Free Period
3. Discussion
4. Materials and Methods
4.1. Patient Selection
4.2. Follow-Up and Examination
4.3. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sakurada, Y.; Yoneyama, S.; Sugiyama, A.; Tanabe, N.; Kikushima, W.; Mabuchi, F.; Kume, A.; Kubota, T.; Iijima, H. Prevalence and Genetic Characteristics of Geographic Atrophy among Elderly Japanese with Age-Related Macular Degeneration. PLoS ONE 2016, 11, e0149978. [Google Scholar] [CrossRef] [PubMed]
- Maruko, I.; Iida, T.; Saito, M.; Nagayama, D.; Saito, K. Clinical characteristics of exudative age-related macular degeneration in Japanese patients. Am. J. Ophthalmol. 2007, 144, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Yamashiro, K.; Yanagi, Y.; Koizumi, H.; Matsumoto, H.; Cheung, C.M.G.; Gomi, F.; Iida, T.; Tsujikawa, A. Relationship between Pachychoroid and Polypoidal Choroidal Vasculopathy. J. Clin. Med. 2022, 11, 4614. [Google Scholar] [CrossRef] [PubMed]
- Sakurada, Y.; Tanaka, K.; Fragiotta, S. Differentiating drusen and drusenoid deposits subtypes on multimodal imaging and risk of advanced age-related macular degeneration. Jpn. J. Ophthalmol. 2023, 67, 1–13. [Google Scholar] [CrossRef]
- Koh, A.; Lee, W.K.; Chen, L.J.; Chen, S.J.; Hashad, Y.; Kim, H.; Lai, T.Y.; Pilz, S.; Ruamviboonsuk, P.; Tokaji, E.; et al. EVEREST study: Efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina 2012, 32, 1453–1464. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.K.; Iida, T.; Ogura, Y.; Chen, S.J.; Wong, T.Y.; Mitchell, P.; Cheung, G.C.M.; Zhang, Z.; Leal, S.; Ishibashi, T.; et al. Efficacy and Safety of Intravitreal Aflibercept for Polypoidal Choroidal Vasculopathy in the PLANET Study: A Randomized Clinical Trial. JAMA Ophthalmol. 2018, 136, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Hoshino, J.; Mukai, R.; Nakamura, K.; Akiyama, H. Short-term outcomes of intravitreal brolucizumab for treatment-naive neovascular age-related macular degeneration with type 1 choroidal neovascularization including polypoidal choroidal vasculopathy. Sci. Rep. 2021, 11, 6759. [Google Scholar] [CrossRef] [PubMed]
- Matsumiya, W.; Honda, S.; Otsuka, K.; Miki, A.; Nagai, T.; Imai, H.; Kusuhara, S.; Nakamura, M. One-year outcome of combination therapy with intravitreal aflibercept and verteporfin photodynamic therapy for polypoidal choroidal vasculopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 541–548. [Google Scholar] [CrossRef]
- Morimoto, M.; Matsumoto, H.; Mimura, K.; Akiyama, H. Two-year results of a treat-and-extend regimen with aflibercept for polypoidal choroidal vasculopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 1891–1897. [Google Scholar] [CrossRef]
- Kikushima, W.; Sakurada, Y.; Sugiyama, A.; Tanabe, N.; Kume, A.; Iijima, H. Comparison of initial treatment between 3-monthly intravitreal aflibercept monotherapy and combined photodynamic therapy with single intravitreal aflibercept for polypoidal choroidal vasculopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 311–316. [Google Scholar] [CrossRef]
- Fukuda, Y.; Sakurada, Y.; Matsubara, M.; Hasebe, Y.; Sugiyama, A.; Kikushima, W.; Kashiwagi, K. Comparison of Outcomes between 3 Monthly Brolucizumab and Aflibercept Injections for Polypoidal Choroidal Vasculopathy. Biomedicines 2021, 9, 1164. [Google Scholar] [CrossRef] [PubMed]
- Ito, A.; Maruyama-Inoue, M.; Kitajima, Y.; Ikeda, S.; Inoue, T.; Kadonosono, K. One-year outcomes of intravitreal brolucizumab injections in patients with polypoidal choroidal vasculopathy. Sci. Rep. 2022, 12, 7987. [Google Scholar] [CrossRef] [PubMed]
- Ijiri, S.; Sugiyama, K. Short-term efficacy of intravitreal aflibercept for patients with treatment-naive polypoidal choroidal vasculopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 351–357. [Google Scholar] [CrossRef]
- Tanaka, K.; Koizumi, H.; Tamashiro, T.; Itagaki, K.; Nakayama, M.; Maruko, I.; Wakugawa, S.; Terao, N.; Onoe, H.; Wakatsuki, Y.; et al. Short-term results for brolucizumab in treatment-naive neovascular age-related macular degeneration: A Japanese multicenter study. Jpn. J. Ophthalmol. 2022, 66, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, Y.; Sakurada, Y.; Matsubara, M.; Kotoda, Y.; Kasai, Y.; Sugiyama, A.; Kashiwagi, K. Comparison of one-year outcomes between as-needed brolucizumab and aflibercept for polypoidal choroidal vasculopathy. Jpn. J. Ophthalmol. 2023, 67, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Azzolini, C.; Pagani, I.S.; Pirrone, C.; Borroni, D.; Donati, S.; Al Oum, M.; Pigni, D.; Chiaravalli, A.M.; Vinciguerra, R.; Simonelli, F.; et al. Expression of VEGF-A, Otx homeobox and p53 family genes in proliferative vitreoretinopathy. Mediat. Inflamm. 2013, 2013, 857380. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, A.; Okada, A.A.; Kano, M.; Koizumi, H.; Saito, M.; Maruko, I.; Sekiryu, T.; Iida, T. One-Year Results of Intravitreal Aflibercept for Polypoidal Choroidal Vasculopathy. Ophthalmology 2015, 122, 1866–1872. [Google Scholar] [CrossRef] [PubMed]
- Sayanagi, K.; Fujimoto, S.; Hara, C.; Fukushima, Y.; Maruyama, K.; Kawasaki, R.; Sato, S.; Nishida, K. Effect of polyp regression and reduction on treatment efficacy in polypoidal choroidal vasculopathy treated with aflibercept. Sci. Rep. 2024, 14, 1833. [Google Scholar] [CrossRef] [PubMed]
- Borroni, D.; Erts, R.; Vallabh, N.A.; Bonzano, C.; Sepetiene, S.; Krumina, Z.; Romano, V.; Parekh, M.; Iannetta, D. Solar retinopathy: A new setting of red, green, and blue channels. Eur. J. Ophthalmol. 2021, 31, 1261–1266. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, M.; Sakurada, Y.; Sugiyama, A.; Fukuda, Y.; Parikh, R.; Kashiwagi, K. Response to photodynamic therapy combined with intravitreal aflibercept for polypoidal choroidal vasculopathy depending on fellow-eye condition:2-year results. PLoS ONE 2020, 15, e0237330. [Google Scholar] [CrossRef]
- Fukuda, Y.; Sakurada, Y.; Sugiyama, A.; Yoneyama, S.; Matsubara, M.; Kikushima, W.; Tanabe, N.; Parikh, R.; Kashiwagi, K. Pachydrusen in Fellow Eyes Predict Response to Aflibercept Monotherapy in Patients with Polypoidal Choroidal Vasculopathy. J. Clin. Med. 2020, 9, 2459. [Google Scholar] [CrossRef] [PubMed]
- Yanagi, Y.; Ting, D.S.W.; Ng, W.Y.; Lee, S.Y.; Mathur, R.; Chan, C.M.; Yeo, I.; Wong, T.Y.; Cheung, G.C.M. Choroidal Vascular Hyperpermeability as a Predictor of Treatment Response for Polypoidal Choroidal Vasculopathy. Retina 2018, 38, 1509–1517. [Google Scholar] [CrossRef] [PubMed]
- Sakurada, Y.; Sugiyama, A.; Tanabe, N.; Kikushima, W.; Kume, A.; Iijima, H. Choroidal Thickness as a Prognostic Factor of Photodynamic Therapy with Aflibercept or Ranibizumab for Polypoidal Choroidal Vasculopathy. Retina 2017, 37, 1866–1872. [Google Scholar] [CrossRef] [PubMed]
- Dansingani, K.K.; Gal-Or, O.; Sadda, S.R.; Yannuzzi, L.A.; Freund, K.B. Understanding aneurysmal type 1 neovascularization (polypoidal choroidal vasculopathy): A lesson in the taxonomy of ‘expanded spectra’-A review. Clin. Exp. Ophthalmol. 2018, 46, 189–200. [Google Scholar] [CrossRef]
- Tan, C.S.; Cheung, C.M.; Lai, T.Y.; Pataluskaite, R.; Margaron, P.; Lim, T.H. Predictors and importance of complete polypoidal lesion regression in the Everest II study: predictors of polyp regression in polypoidal choroidal vasculopathy. Retina 2022, 42, 2091–2098. [Google Scholar] [CrossRef]
- Choi, K.E.; Lee, Y.J.; Bae, S.H. Imaging and clinical features of pulsatile polypoidal choroidal vasculopathy. Retina 2024, 44, 1083–1091. [Google Scholar] [CrossRef]
- Koizumi, H.; Yamagishi, T.; Yamazaki, T.; Kinoshita, S. Predictive factors of resolved retinal fluid after intravitreal ranibizumab for polypoidal choroidal vasculopathy. Br. J. Ophthalmol. 2011, 95, 1555–1559. [Google Scholar] [CrossRef]
- Nguyen, Q.D.; Das, A.; Do, D.V.; Dugel, P.U.; Gomes, A.; Holz, F.G.; Koh, A.; Pan, C.K.; Sepah, Y.J.; Patel, N.; et al. Brolucizumab: Evolution through Preclinical and Clinical Studies and the Implications for the Management of Neovascular Age-Related Macular Degeneration. Ophthalmology 2020, 127, 963–976. [Google Scholar] [CrossRef] [PubMed]
- Dugel, P.U.; Koh, A.; Ogura, Y.; Jaffe, G.J.; Schmidt-Erfurth, U.; Brown, D.M.; Gomes, A.V.; Warburton, J.; Weichselberger, A.; Holz, F.G.; et al. HAWK and HARRIER: Phase 3, Multicenter, Randomized, Double-Masked Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2020, 127, 72–84. [Google Scholar] [CrossRef]
- Mones, J.; Srivastava, S.K.; Jaffe, G.J.; Tadayoni, R.; Albini, T.A.; Kaiser, P.K.; Holz, F.G.; Korobelnik, J.F.; Kim, I.K.; Pruente, C.; et al. Risk of Inflammation, Retinal Vasculitis, and Retinal Occlusion-Related Events with Brolucizumab: Post Hoc Review of HAWK and HARRIER. Ophthalmology 2021, 128, 1050–1059. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics n = 62 | Values |
|---|---|
| Age (years) | 72.7 ± 7.9 |
| Male (%)/Female (%) | 47 (76)/15 (24) |
| BCVA (logMAR) | 0.28 ± 0.28 |
| CRT (μm) | 320 ± 130.0 |
| SCT (μm) | 210 ± 90 |
| Number of polyps | 2.7 ± 2.6 |
| Maximum diameter of polyps (μm) | 362 ± 214 |
| Characteristics | Complete Regression Group (n = 36) | Non- Regression Group (n = 26) | p-Value | Adjusted p-Value |
|---|---|---|---|---|
| Age (years) | 73.8 ± 7.7 | 71.1 ± 8.0 | 0.11 | |
| Male (%)/Female (%) | 29 (81)/7 (19) | 18 (69)/8 (31) | 0.31 | |
| BCVA (logMAR) | 0.29 ± 0.29 | 0.28 ± 0.28 | 0.86 | |
| CRT (μm) | 211 ± 96.0 | 208 ± 84 | 0.86 | |
| SCT (μm) | 304 ± 121 | 342 ± 142 | 0.21 | |
| Number of polyps | 2.5 ±2.5 | 3.0 ± 2.8 | 0.17 | |
| Maximum diameter of polyps(μm) | 293 ± 140 | 457 ± 262 | 0.024 * | 0.005 * |
| IVBr (%)/IVA (%) | 24 (67)/12 (33) | 6 (23)/20 (77) | 0.001 * | 0.012 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kimura, M.; Sakurada, Y.; Fukuda, Y.; Matsubara, M.; Kotoda, Y.; Kasai, Y.; Sugiyama, A.; Kikushima, W.; Tsuru, D.V.; Kashiwagi, K. Association of Polyp Regression after Loading Phase with 12-Month Outcomes of Eyes with Polypoidal Choroidal Vasculopathy. Pharmaceuticals 2024, 17, 687. https://doi.org/10.3390/ph17060687
Kimura M, Sakurada Y, Fukuda Y, Matsubara M, Kotoda Y, Kasai Y, Sugiyama A, Kikushima W, Tsuru DV, Kashiwagi K. Association of Polyp Regression after Loading Phase with 12-Month Outcomes of Eyes with Polypoidal Choroidal Vasculopathy. Pharmaceuticals. 2024; 17(6):687. https://doi.org/10.3390/ph17060687
Chicago/Turabian StyleKimura, Misa, Yoichi Sakurada, Yoshiko Fukuda, Mio Matsubara, Yumi Kotoda, Yuka Kasai, Atsushi Sugiyama, Wataru Kikushima, Daphne Viel Tsuru, and Kenji Kashiwagi. 2024. "Association of Polyp Regression after Loading Phase with 12-Month Outcomes of Eyes with Polypoidal Choroidal Vasculopathy" Pharmaceuticals 17, no. 6: 687. https://doi.org/10.3390/ph17060687
APA StyleKimura, M., Sakurada, Y., Fukuda, Y., Matsubara, M., Kotoda, Y., Kasai, Y., Sugiyama, A., Kikushima, W., Tsuru, D. V., & Kashiwagi, K. (2024). Association of Polyp Regression after Loading Phase with 12-Month Outcomes of Eyes with Polypoidal Choroidal Vasculopathy. Pharmaceuticals, 17(6), 687. https://doi.org/10.3390/ph17060687