
Cholinergic Stimulation Exerts Cardioprotective Effects and Alleviates Renal Inflammatory Responses after Acute Myocardial Infarction in Spontaneous Hypertensive Rats (SHRs)


Abstract
1. Introduction
2. Results
2.1. Alterations in Hemodynamic Indices and Cardiovascular Variability during AMI and Effects of Pyridostigmine
2.2. Alterations in Structural and Functional Echocardiographic Parameters during AMI and Effects of Pyridostigmine
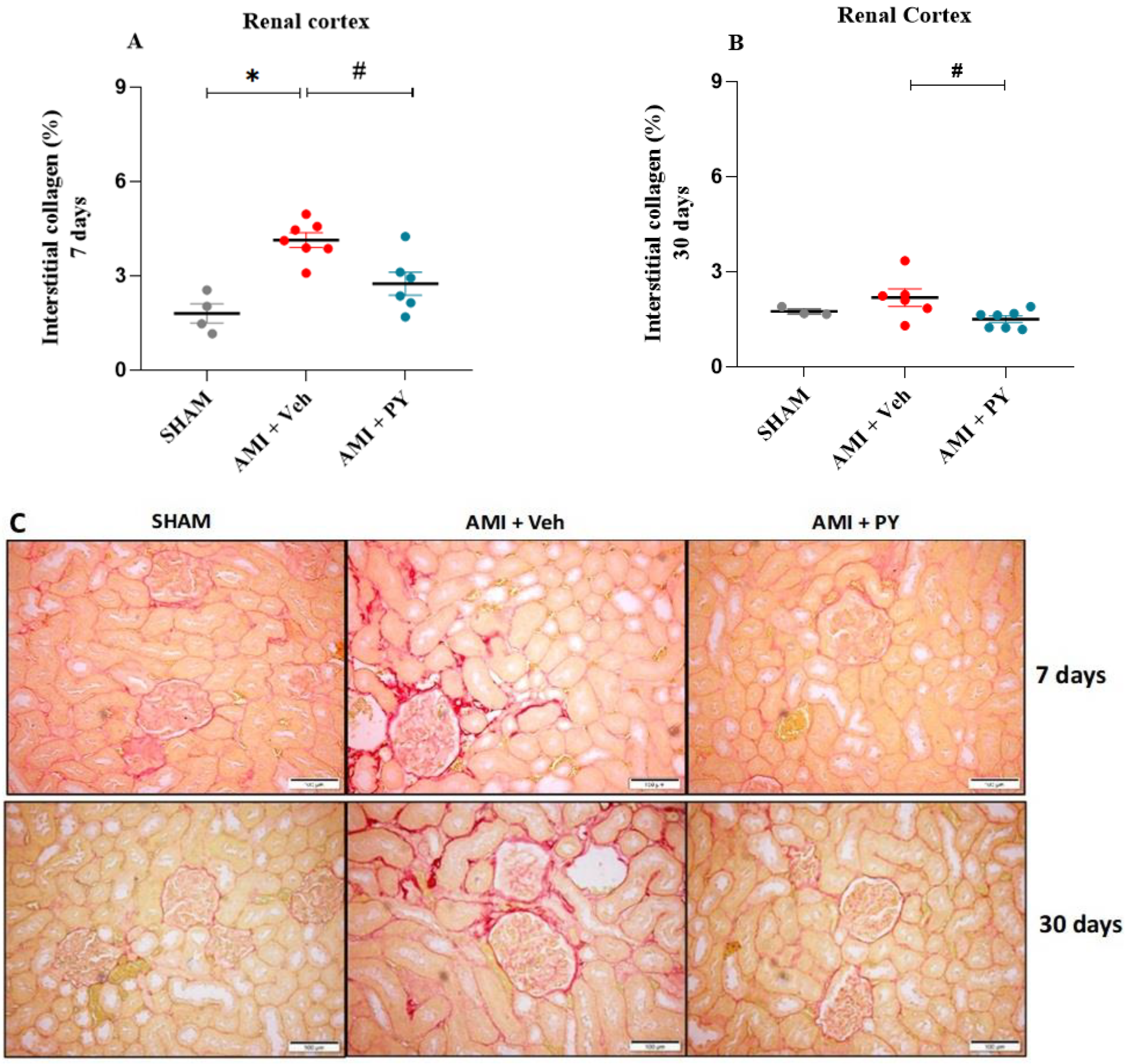
2.3. Alterations in Renal Function Markers during AMI and Effects of Pyridostigmine
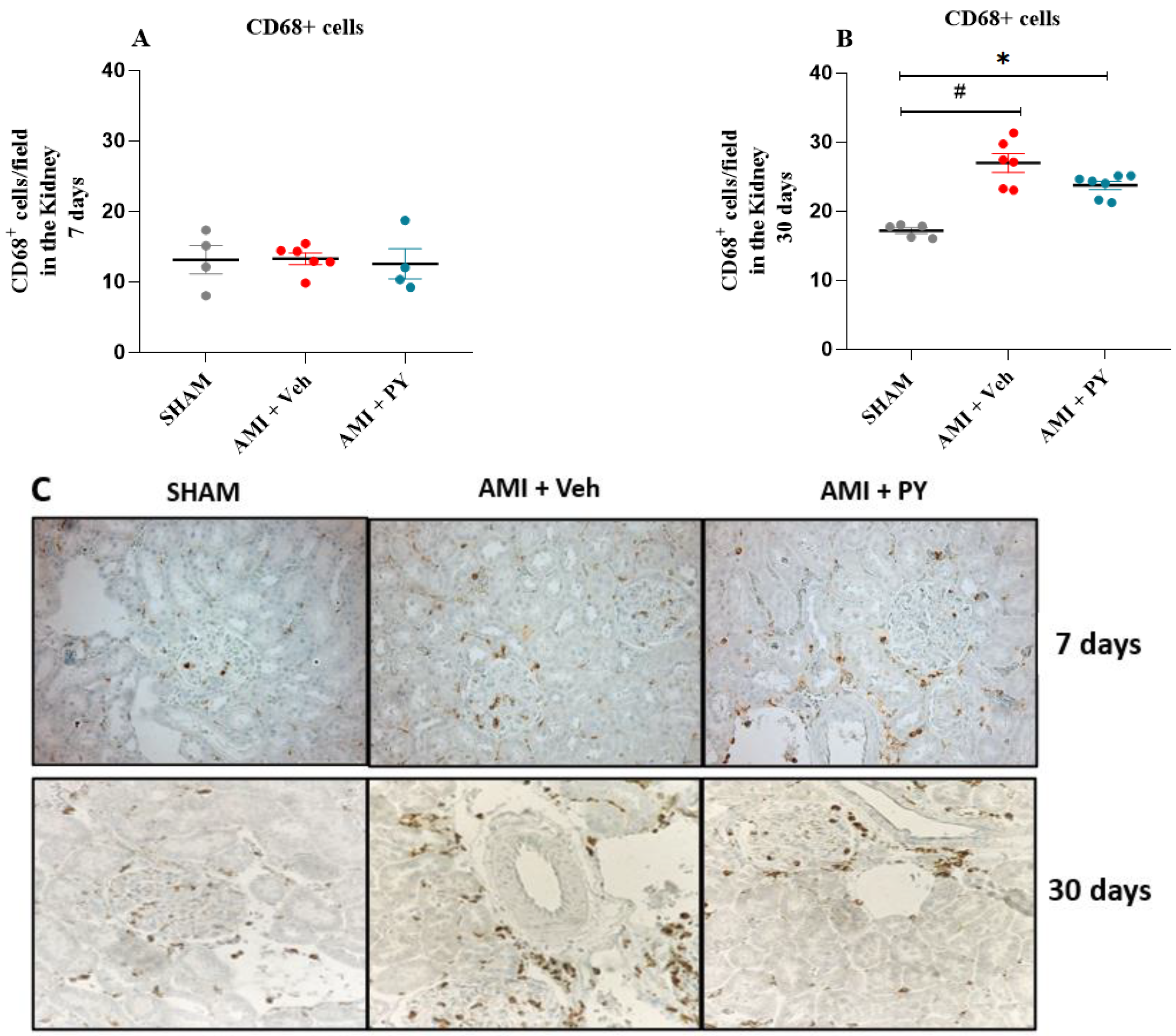
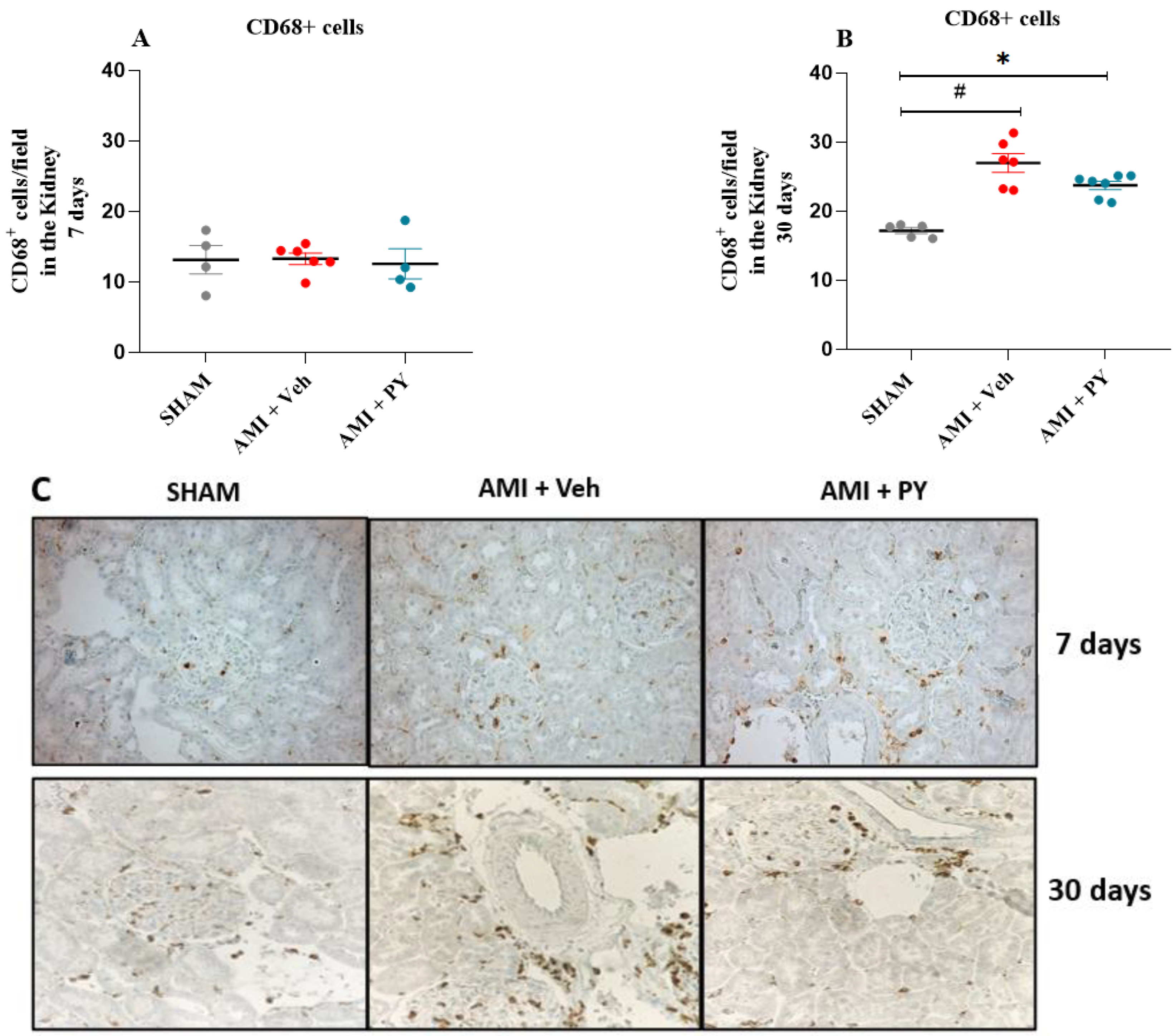
2.4. Changes in CD68+ Macrophages in Renal Tissue following AMI and Effects of Pyridostigmine
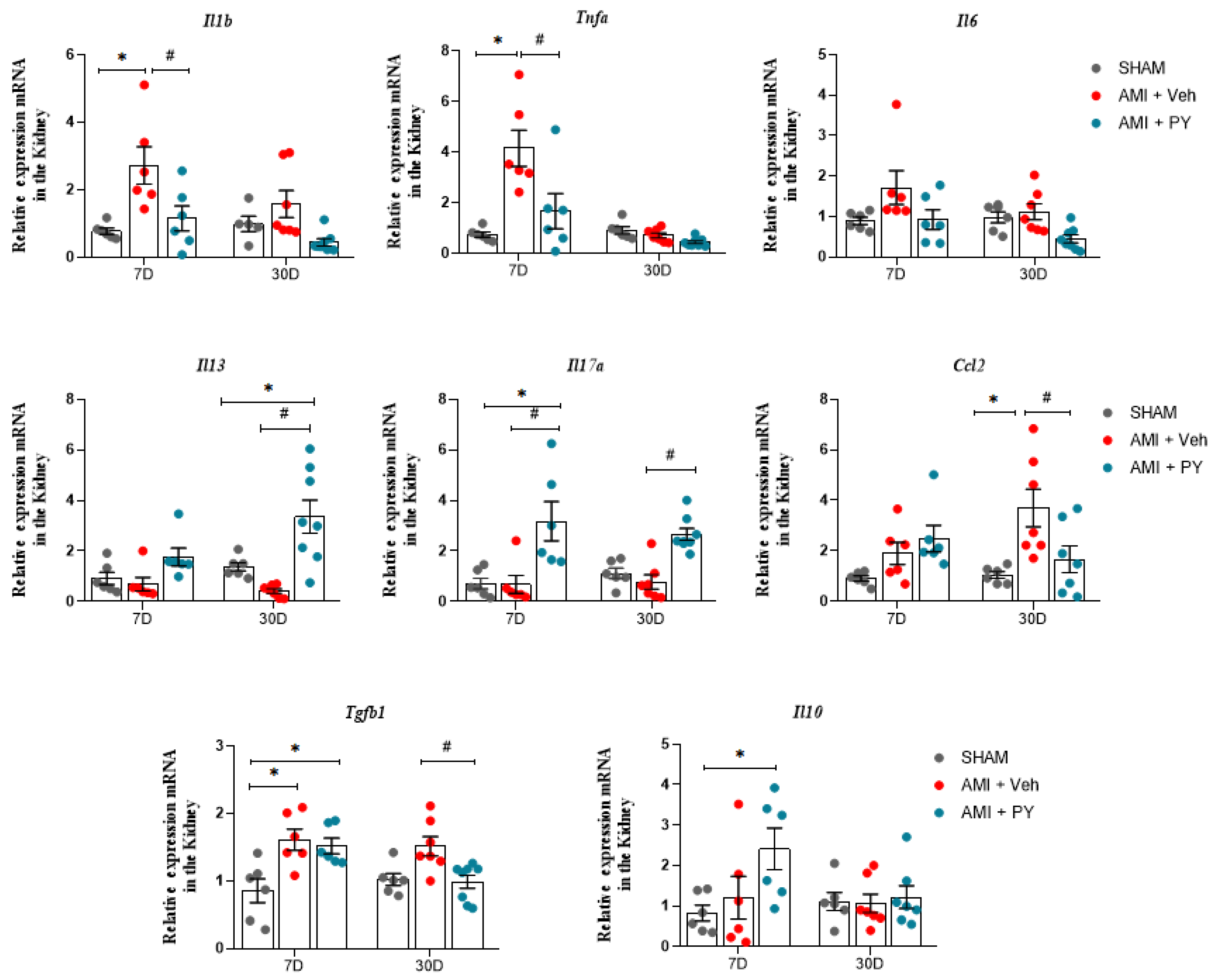
2.5. Changes in the Gene Expression of Pro-Inflammatory and Anti-Inflammatory Markers in Renal Tissue Post-Acute Myocardial Infarction and Effects of Pyridostigmine
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Animals
4.3. Experimental Design
4.4. Myocardial Infarction
4.5. Arterial Catheterization and Cardiovascular Assessments
4.6. Echocardiographic Evaluation
4.7. Renal Function Marker Analysis
4.8. Histological Examination and Quantitative Collagen Analysis
4.9. Immunohistochemistry for Immune Cells and NGAL
4.10. Real-Time Quantitative PCR
4.11. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salari, N.; Morddarvanjoghi, F.; Abdolmaleki, A.; Rasoulpoor, S.; Khaleghi, A.A.; Hezarkhani, L.A.; Shohaimi, S.; Mohammadi, M. The global prevalence of myocardial infarction: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 2023, 23, 206. [Google Scholar] [CrossRef] [PubMed]
- Frangogiannis, N.G. The immune system and cardiac repair. Pharmacol. Res. 2008, 58, 88–111. [Google Scholar] [CrossRef]
- Parikh, C.R.; Coca, S.G.; Wang, Y.; Masoudi, F.A.; Krumholz, H.M. Long-term prognosis of acute kidney injury after acute myocardial infarction. Arch. Intern. Med. 2008, 168, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, A.; Kogan, E.; Hammerman, H.; Markiewicz, W.; Aronson, D. The impact of transient and persistent acute kidney injury on long-term outcomes after acute myocardial infarction. Kidney Int. 2009, 76, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Haapio, M.; House, A.A.; Anavekar, N.; Bellomo, R. Cardiorenal syndrome. J. Am. Coll. Cardiol. 2008, 52, 1527–1539. [Google Scholar] [CrossRef] [PubMed]
- Virzì, G.; Day, S.; de Cal, M.; Vescovo, G.; Ronco, C. Heart-kidney crosstalk and role of humoral signaling in critical illness. Crit. Care 2014, 18, 201. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Cicoira, M.; McCullough, P.A. Cardiorenal syndrome type 1: Pathophysiological crosstalk leading to combined heart and kidney dysfunction in the setting of acutely decompensated heart failure. J. Am. Coll. Cardiol. 2012, 60, 1031–1042. [Google Scholar] [CrossRef] [PubMed]
- Lekawanvijit, S.; Kompa, A.R.; Zhang, Y.; Wang, B.H.; Kelly, D.J.; Krum, H. Myocardial infarction impairs renal function, induces renal interstitial fibrosis, and increases renal KIM-1 expression: Implications for cardiorenal syndrome. Am. J. Physiol. Heart Circ. Physiol. 2012, 302, H1884–H1893. [Google Scholar] [CrossRef]
- Cho, E.; Kim, M.; Ko, Y.S.; Lee, H.Y.; Song, M.; Kim, M.G.; Kim, H.K.; Cho, W.Y.; Jo, S.K. Role of inflammation in the pathogenesis of cardiorenal syndrome in a rat myocardial infarction model. Nephrol. Dial. Transplant. 2013, 28, 2766–2778. [Google Scholar] [CrossRef]
- Tracey, K.J. The inflammatory reflex. Nature 2002, 420, 853–859. [Google Scholar] [CrossRef]
- Wang, H.; Yu, M.; Ochani, M.; Amella, C.A.; Tanovic, M.; Susarla, S.; Li, J.H.; Wang, H.; Yang, H.; Ulloa, L.; et al. Nicotinic acetylcholine receptor alpha7 subunit is an essential regulator of inflammation. Nature 2003, 421, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Pohanka, M. Pharmacological Influencing of The Cholinergic Anti-inflammatory Pathway in Infectious Diseases and Inflammatory Pathologies. Mini Rev. Med. Chem. 2021, 21, 660–669. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.J.; Breathnach, C.; Tracey, K.J.; Donnelly, S.C. Manipulation of the inflammatory reflex as a therapeutic strategy. Cell Rep. Med. 2022, 3, 100696. [Google Scholar] [CrossRef] [PubMed]
- Falvey, A.; Metz, C.N.; Tracey, K.J.; Pavlov, V.A. Peripheral nerve stimulation and immunity: The expanding opportunities for providing mechanistic insight and therapeutic intervention. Int. Immunol. 2022, 34, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Metz, C.N.; Pavlov, V.A. Treating disorders across the lifespan by modulating cholinergic signaling with galantamine. J. Neurochem. 2021, 158, 1359–1380. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, P.K.; Yeboah, M.M.; Dowling, O.; Xue, X.; Powell, S.R.; Al-Abed, Y.; Metz, C.N. Nicotinic acetylcholine receptor agonists attenuate septic acute kidney injury in mice by suppressing inflammation and proteasome activity. PLoS ONE 2012, 7, e35361. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, P.K.; Yeboah, M.M.; Solanki, M.H.; Kumar, G.; Xue, X.; Pavlov, V.A.; Al-Abed, Y.; Metz, C.N. Activation of the cholinergic anti-inflammatory pathway by GTS-21 attenuates cisplatin-induced acute kidney injury in mice. PLoS ONE 2017, 12, e0188797. [Google Scholar] [CrossRef] [PubMed]
- Okusa, M.D.; Rosin, D.L.; Tracey, K.J. Targeting neural reflex circuits in immunity to treat kidney disease. Nat. Rev. Nephrol. 2017, 13, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Yeboah, M.M.; Xue, X.; Duan, B.; Ochani, M.; Tracey, K.J.; Susin, M.; Metz, C.N. Cholinergic agonists attenuate renal ischemia-reperfusion injury in rats. Kidney Int. 2008, 74, 62–69. [Google Scholar] [CrossRef]
- Rocha, J.A.; Ribeiro, S.P.; França, C.M.; Coelho, O.; Alves, G.; Lacchini, S.; Kallás, E.G.; Irigoyen, M.C.; Consolim-Colombo, F.M. Increase in cholinergic modulation with pyridostigmine induces anti-inflammatory cell recruitment soon after acute myocardial infarction in rats. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2016, 310, R697–R706. [Google Scholar] [CrossRef]
- Bezerra, O.C.; França, C.M.; Rocha, J.A.; Neves, G.A.; Souza, P.R.M.; Teixeira Gomes, M.; Malfitano, C.; Loleiro, T.C.A.; Dourado, P.M.; Llesuy, S.; et al. Cholinergic Stimulation Improves Oxidative Stress and Inflammation in Experimental Myocardial Infarction. Sci. Rep. 2017, 7, 13687. [Google Scholar] [CrossRef] [PubMed]
- Bandoni, R.L.; Bricher Choque, P.N.; Dellê, H.; de Moraes, T.L.; Porter, M.H.M.; da Silva, B.D.; Neves, G.A.; Irigoyen, M.C.; De Angelis, K.; Pavlov, V.A.; et al. Cholinergic stimulation with pyridostigmine modulates a heart-spleen axis after acute myocardial infarction in spontaneous hypertensive rats. Sci. Rep. 2021, 11, 9563. [Google Scholar] [CrossRef] [PubMed]
- Devarajan, P. Neutrophil gelatinase-associated lipocalin (NGAL): A new marker of kidney disease. Scand. J. Clin. Lab. Investig. Suppl. 2008, 241, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Cooper, T.M.; McKinley, P.S.; Seeman, T.E.; Choo, T.H.; Lee, S.; Sloan, R.P. Heart rate variability predicts levels of inflammatory markers: Evidence for the vagal anti-inflammatory pathway. Brain Behav. Immun. 2015, 49, 94–100. [Google Scholar] [CrossRef]
- Sangaleti, C.T.; Katayama, K.Y.; De Angelis, K.; Lemos de Morales, T.; Aparecida Araujo, A.; Lopes, H.F.; Camacho, C.; Aparecido Bortolotto, L.; Compagno Michelini, L.; Irigoyen, M.C.; et al. Consolim Colombo FM. The Cholinergic Drug Galantamine Alleviates Oxidative Stress Alongside Anti-inflammatory and Cardio-Metabolic Effects in Subjects with the Metabolic Syndrome in a Randomized Trial. Front. Immunol. 2021, 12, 613979. [Google Scholar] [CrossRef] [PubMed]
- de Moraes, T.L.; Costa, F.O.; Cabral, D.G.; Marques Fernandes, D.; Teles Sangaleti, C.; Aparecida Dalboni, M.; Motta E Motta, J.; Appratto de Souza, L.; Montano, N.; Irigoyen, M.C.; et al. Brief periods of transcutaneous auricular vagus nerve stimulation improve autonomic balance and alter circulating monocytes and endothelial cells in patients with metabolic syndrome: A pilot study. Bioelectron. Med. 2023, 9, 7. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, K.; Aoki, K. Development of a strain of spontaneously hypertensive rats. Jpn. Circ. J. 1963, 27, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Harwani, S.C.; Chapleau, M.W.; Legge, K.L.; Ballas, Z.K.; Abboud, F.M. Neurohormonal modulation of the innate immune system is proinflammatory in the prehypertensive spontaneously hypertensive rat, a genetic model of essential hypertension. Circ. Res. 2012, 111, 1190–1197. [Google Scholar] [CrossRef]
- Blanco, J.H.; Gastaldi, A.C.; Gardim, C.B.; Araujo, J.E.; Simões, M.V.; Oliveira, L.F.; Carvalho, E.E.; Souza, H.C. Chronic cholinergic stimulation promotes changes in cardiovascular autonomic control in spontaneously hypertensive rats. Auton. Neurosci. 2015, 193, 97–103. [Google Scholar] [CrossRef]
- Gardim, C.B.; Veiga, A.C.; Aguilar, B.A.; Philbois, S.V.; Souza, H.C.D. Effects of chronic cholinergic stimulation associated with aerobic physical training on cardiac morphofunctional and autonomic parameters in spontaneously hypertensive rats. Sci. Rep. 2021, 11, 17141. [Google Scholar] [CrossRef]
- Li, D.J.; Evans, R.G.; Yang, Z.W.; Song, S.W.; Wang, P.; Ma, X.J.; Liu, C.; Xi, T.; Su, D.F.; Shen, F.M. Dysfunction of the cholinergic anti-inflammatory pathway mediates organ damage in hypertension. Hypertension 2011, 57, 298–307. [Google Scholar] [CrossRef] [PubMed]
- La Rovere, M.T.; Pinna, G.D.; Raczak, G. Baroreflex sensitivity: Measurement and clinical implications. Ann. Noninvasive Electrocardiol. 2008, 13, 191–207. [Google Scholar] [CrossRef] [PubMed]
- La Rovere, M.T.; Pinna, G.D.; Maestri, R.; Robbi, E.; Caporotondi, A.; Guazzotti, G.; Sleight, P.; Febo, O. Prognostic implications of baroreflex sensitivity in heart failure patients in the beta-blocking era. J. Am. Coll. Cardiol. 2009, 53, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Abe, C.; Sung, S.S.; Moscalu, S.; Jankowski, J.; Huang, L.; Ye, H.; Rosin, D.L.; Guyenet, P.G.; Okusa, M.D. Vagus nerve stimulation mediates protection from kidney ischemia-reperfusion injury through α7nAChR+ splenocytes. J. Clin. Investig. 2016, 126, 1939–1952. [Google Scholar] [CrossRef] [PubMed]
- Johns, E.J.; Kopp, U.C.; DiBona, G.F. Neural control of renal function. Compr. Physiol. 2011, 1, 731–767. [Google Scholar] [CrossRef] [PubMed]
- Han, H.I.; Skvarca, L.B.; Espiritu, E.B.; Davidson, A.J.; Hukriede, N.A. The role of macrophages during acute kidney injury: Destruction and repair. Pediatr. Nephrol. 2019, 34, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.E.; Ding, Y.; Kim, S.I. TGF-β signaling via TAK1 pathway: Role in kidney fibrosis. Semin. Nephrol. 2012, 32, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.J.; Shi, Z.W.; Wang, X.; Ren, F.F.; Xie, Z.Y.; Lei, L.; Chen, P. Activation of the Cholinergic Anti-inflammatory Pathway Attenuated Angiotension II-Dependent Hypertension and Renal Injury. Front. Pharmacol. 2021, 12, 593682. [Google Scholar] [CrossRef]
- Rudemiller, N.P.; Crowley, S.D. The role of chemokines in hypertension and consequent target organ damage. Pharmacol. Res. 2017, 119, 404–411. [Google Scholar] [CrossRef]
- Liu, Y.; Xu, K.; Xiang, Y.; Ma, B.; Li, H.; Li, Y.; Shi, Y.; Li, S.; Bai, Y. Role of MCP-1 as an inflammatory biomarker in nephropathy. Front. Immunol. 2024, 14, 1303076. [Google Scholar] [CrossRef]
- Uni, R.; Inoue, T.; Nakamura, Y.; Fukaya, D.; Hasegawa, S.; Wu, C.H.; Fujii, R.; Surattichaiyakul, B.; Peerapanyasut, W.; Ozeki, A.; et al. Vagus nerve stimulation even after injury ameliorates cisplatin-induced nephropathy via reducing macrophage infiltration. Sci. Rep. 2020, 10, 9472. [Google Scholar] [CrossRef] [PubMed]
- Cantero-Navarro, E.; Rayego-Mateos, S.; Orejudo, M.; Tejedor-Santamaria, L.; Tejera-Muñoz, A.; Sanz, A.B.; Marquez-Exposito, L.; Marchant, V.; Santos-Sanchez, L.; Egido, J.; et al. Role of Macrophages and Related Cytokines in Kidney Disease. Front. Med. 2021, 8, 688060. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.Z.; Wang, X.; Wang, Y.; Niu, A.; Wang, S.; Zou, C.; Harris, R.C. IL-4/IL-13-mediated polarization of renal macrophages/dendritic cells to an M2a phenotype is essential for recovery from acute kidney injury. Kidney Int. 2017, 91, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Zahler, D.; Merdler, I.; Banai, A.; Shusterman, E.; Feder, O.; Itach, T.; Robb, L.; Banai, S.; Shacham, Y. Predictive Value of Elevated Neutrophil Gelatinase-Associated Lipocalin (NGAL) Levels for Assessment of Cardio-Renal Interactions among ST-Segment Elevation Myocardial Infarction Patients. J. Clin. Med. 2022, 11, 2162. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
|
SHAM 7 Days (n = 10) |
AMI + Veh 7 Days (n = 10) |
AMI + PY 7 Days (n = 10) |
SHAM 30 Days (n = 10) |
AMI + Veh 30 Days (n = 10) |
AMI + PY 30 Days (n = 10) | |
|---|---|---|---|---|---|---|
|
SBP mmHg Mean (SD) | 203.4 (6.9) | 74.8 *a (17.5) | 163.3 *b (9.2) | 212.5 (8.2) | 207.2 (12.5) | 189.3 *c#d (13.4) |
|
DBP mmHg Mean (SD) | 143.7 (7.2) | 129.0 *e (8.3) | 119.6 *f#g (7.9) | 148.5 (6.0) | 144.4 (6.3) | 134.2 (8.2) |
|
MBP mmHg Mean SD) | 171.1 (5.6) | 148.8 *h (13.9) | 142.4 *i (8.7) | 176.3 (7.0) | 174.8 (9.5) | 161.8 *j#k (10.0) |
|
HR bpm Mean (SD) | 373.5 (26.1) | 393.0 (22.1) | 375.7 (26.7) | 374.4 (26.3) | 384.3 (22.1) | 369.0 (11.9) |
|
SHAM 7 d (n = 10) |
AMI + Veh 7 d (n = 8) |
AMI + PY 7 d (n = 10) |
SHAM 30 d (n = 10) |
AMI + Veh 30 d (n = 10) |
AMI + PY 30 d (n = 10) | |
|---|---|---|---|---|---|---|
| HRV | ||||||
|
RMSSD (ms) SD | 6.2 (2.0) | 5.8 (2.2) | 9.1 *# (2.1) | 8.1 (2.9) | 9.8 (2.7) | 10.1 (2.0) |
|
VARPI (ms2) SD | 28.5 (13.0) | 15.7 (6.0) | 60.1 *# (27.9) | 51.5 (18.7) | 69.6 (30.6) | 91.8 * (49.0) |
|
LF ab (ms2) SD | 2.5 (1.9) | 2.5 (1.0) | 7.2 *# (4.6) | 2.2 (1.4) | 2.6 (1.4) | 3.9 (2.0) |
|
HF ab (ms2) SD | 9.6 (3.5) | 5.9 (2.9) | 22.7 *# (9.0) | 25.6 (17.5) | 26.3 (12.8) | 30.1 (11.0) |
|
LF (nu) SD | 19.3 (7.3) | 31.7 * (9.8) | 22.9 (6.9) | 10.1 (3.1) | 11.1 (4.0) | 12.0 (2.9) |
|
HF (nu) SD | 80.6 (7.3) | 68.3 * (9.8) | 77.1 (6.9) | 89.5 (2.7) | 88.5 (4.0) | 87.5 (3.8) |
|
LF/HF SD | 0.2 (0.1) | 0.5 * (0.2) | 0.3 (0.1) | 0.11 (0.03) | 0.12 (0.04) | 0.14 (0.05) |
| SAPV | ||||||
|
VAR-SBP (mmHg2) SD | 57.8 (18.5) | 28.6 * (12.1) | 30.4 * (14.2) | 41.2 (8.1) | 43.0 (18.4) | 47.6 (19.3) |
|
LF-SBP (mmHg2) SD | 14.7 (8.2) | 11.1 (8.0) | 8.7 (4.5) | 11.1 (3.0) | 12.1 (4.5) | 7.8 # (2.8) |
|
ALFA INDEX ms2/mmHg2 SD | 0.49 (0.34) | 0.55 (0.19) | 0.98 *# (0.48) | 0.44 (0.15) | 0.57 (0.17) | 0.70 * (0.26) |
|
SHAM 7 Days (n = 10) |
AMI + Veh 7 Days (n = 10) |
AMI + PY 7 Days (n = 10) |
SHAM 30 Days (n = 10) |
AMI + Veh 30 Days (n = 10) |
AMI + PY 30 Days (n = 10) | |
|---|---|---|---|---|---|---|
| PARAMETER | ||||||
|
LAD (mm) SD |
4.25 (0.95) |
4.58 (1.19) |
4.08 (0.70) |
5.11 (0.67) |
5.52 (0.66) |
5.18 (0.50) |
|
LVEF (%) SD |
51.48 (8.54) |
33.62 * (13.17) |
37.19 * (10.59) |
53.69 (6.76) |
39.54 * (6.49) |
29.21 * (6.50) |
|
LVFAC (%) SD |
43.9 (5.9) |
28.02 * (7.11) |
32.04 * (9.17) |
47.91 (6.72) |
28.11 * (6.27) |
25.26 * (3.27) |
|
LVSD (mm) SD |
5.64 (0.76) |
7.12 * (0.60) |
6.06
#
(1.21) |
6.30 (0.80) |
7.54 * (0.64) |
8.18 * (0.57) |
|
LVDD (mm) SD |
7.77 (0.61) |
8.53 * (0.92) |
7.44
#
(1.02) |
8.76 (0.38) |
9.70 * (0.63) |
9.44 * (0.26) |
|
LV M (mg) SD |
460.2 (59.52) |
522.7 (123.1) |
447.6 (142.7) |
591.2 (112.7) |
550.1 (82.42) |
531.9 (68.57) |
|
IVRT (ms) SD |
18.25 (3.11) |
17.59 (3.71) |
20.53 (4.06) |
17.24 (3.95) |
19.58 (2.12) |
24.62 * (6.64) |
|
E/A Ratio SD |
1.42 (0.12) |
2.12 * (0.62) |
1.47
#
(0.18) |
1.91 (0.67) |
2.15 (0.76) |
1.72 (0.30) |
|
E′/A′ Ratio SD |
0.69 (0.16) |
0.98 (0.37) |
1.28 * (0.53) |
1.04 (0.39) |
0.87 (0.26) |
1.05 (0.28) |
|
E/E′ Ratio SD |
24.89 (5.84) |
30.09 (9.59) |
18.15
#
(3.44) |
23.87 (8.72) |
31.84 (8.69) |
31.86 (8.19) |
| Cytokine | Sense | Antisense |
|---|---|---|
| TGF-β1 | CTGCTGACCCCCACTGATAC | AGCCCTGTATTCCGTCTCCT |
| MCP-1 | GCTGCTACTCATTCACTGGCAA | GCTGCTGGTGATTCTCTTGTA |
| IL-1β | AAATGCCTCGTGCTGTCTGA | GCTGTTTTAGGGACACCGGA |
| TNF-α | CTCAAGCCCTGGTATGAGCC | CTCCAAAGTAGACCTGCCCG |
| IL-6 | AGCGATGATGCACTGTCAGA | GGAACTCCAGAAGACCAGAGC |
| IL-13 | CCTGGAATCCCTGACCAACA | ATCCGAGGCCTTTTGGTTACA |
| IL-10 | TTGAACCACCCGGCATCTAC | CCAAGGAGTTGCTCCCGTTA |
| ß-actin | AGGAGTACGATGAGTCCGGCCC | GCAGCTCAGTAACAGTCCGCCT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bricher Choque, P.N.; Porter, M.H.; Teixeira, M.S.; Dellê, H.; Elias, R.M.; Durante, B.; Dutra, M.R.H.; Metz, C.N.; Pavlov, V.A.; Consolim Colombo, F.M. Cholinergic Stimulation Exerts Cardioprotective Effects and Alleviates Renal Inflammatory Responses after Acute Myocardial Infarction in Spontaneous Hypertensive Rats (SHRs). Pharmaceuticals 2024, 17, 547. https://doi.org/10.3390/ph17050547
Bricher Choque PN, Porter MH, Teixeira MS, Dellê H, Elias RM, Durante B, Dutra MRH, Metz CN, Pavlov VA, Consolim Colombo FM. Cholinergic Stimulation Exerts Cardioprotective Effects and Alleviates Renal Inflammatory Responses after Acute Myocardial Infarction in Spontaneous Hypertensive Rats (SHRs). Pharmaceuticals. 2024; 17(5):547. https://doi.org/10.3390/ph17050547
Chicago/Turabian StyleBricher Choque, Pamela Nithzi, Maria Helena Porter, Manuella S. Teixeira, Humberto Dellê, Rosilene Motta Elias, Bruno Durante, Marina Rascio Henriques Dutra, Christine N. Metz, Valentin A. Pavlov, and Fernanda M. Consolim Colombo. 2024. "Cholinergic Stimulation Exerts Cardioprotective Effects and Alleviates Renal Inflammatory Responses after Acute Myocardial Infarction in Spontaneous Hypertensive Rats (SHRs)" Pharmaceuticals 17, no. 5: 547. https://doi.org/10.3390/ph17050547
APA StyleBricher Choque, P. N., Porter, M. H., Teixeira, M. S., Dellê, H., Elias, R. M., Durante, B., Dutra, M. R. H., Metz, C. N., Pavlov, V. A., & Consolim Colombo, F. M. (2024). Cholinergic Stimulation Exerts Cardioprotective Effects and Alleviates Renal Inflammatory Responses after Acute Myocardial Infarction in Spontaneous Hypertensive Rats (SHRs). Pharmaceuticals, 17(5), 547. https://doi.org/10.3390/ph17050547