

Quantification of Etoricoxib in Low Plasma Volume by UPLC-PDA and Application to Preclinical Pharmacokinetic Study



Abstract
1. Introduction
2. Results
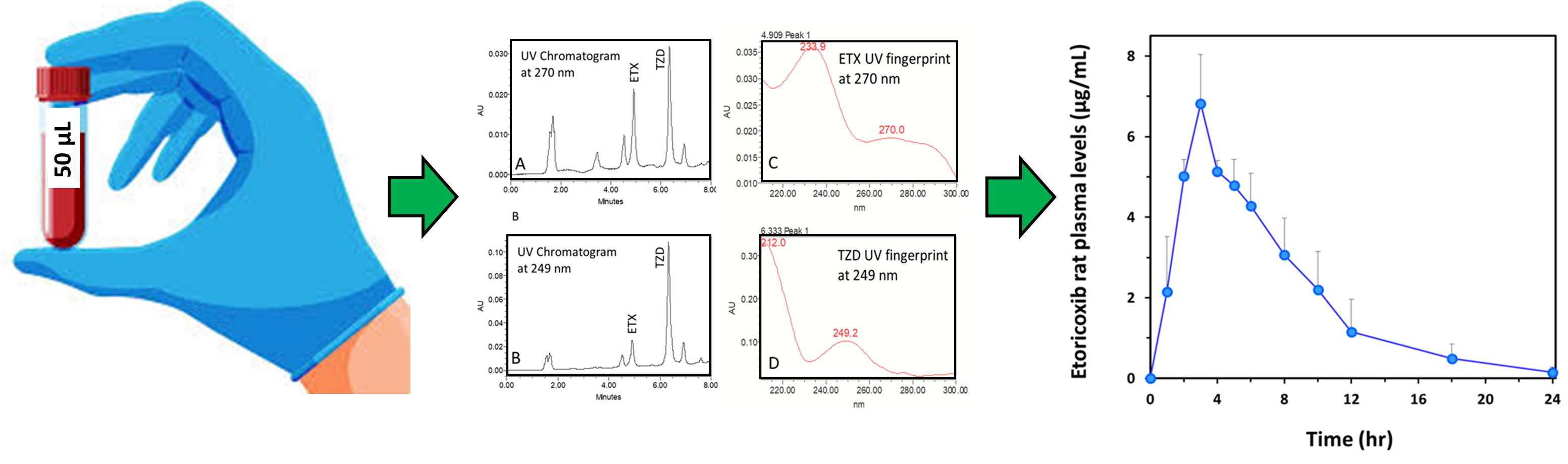
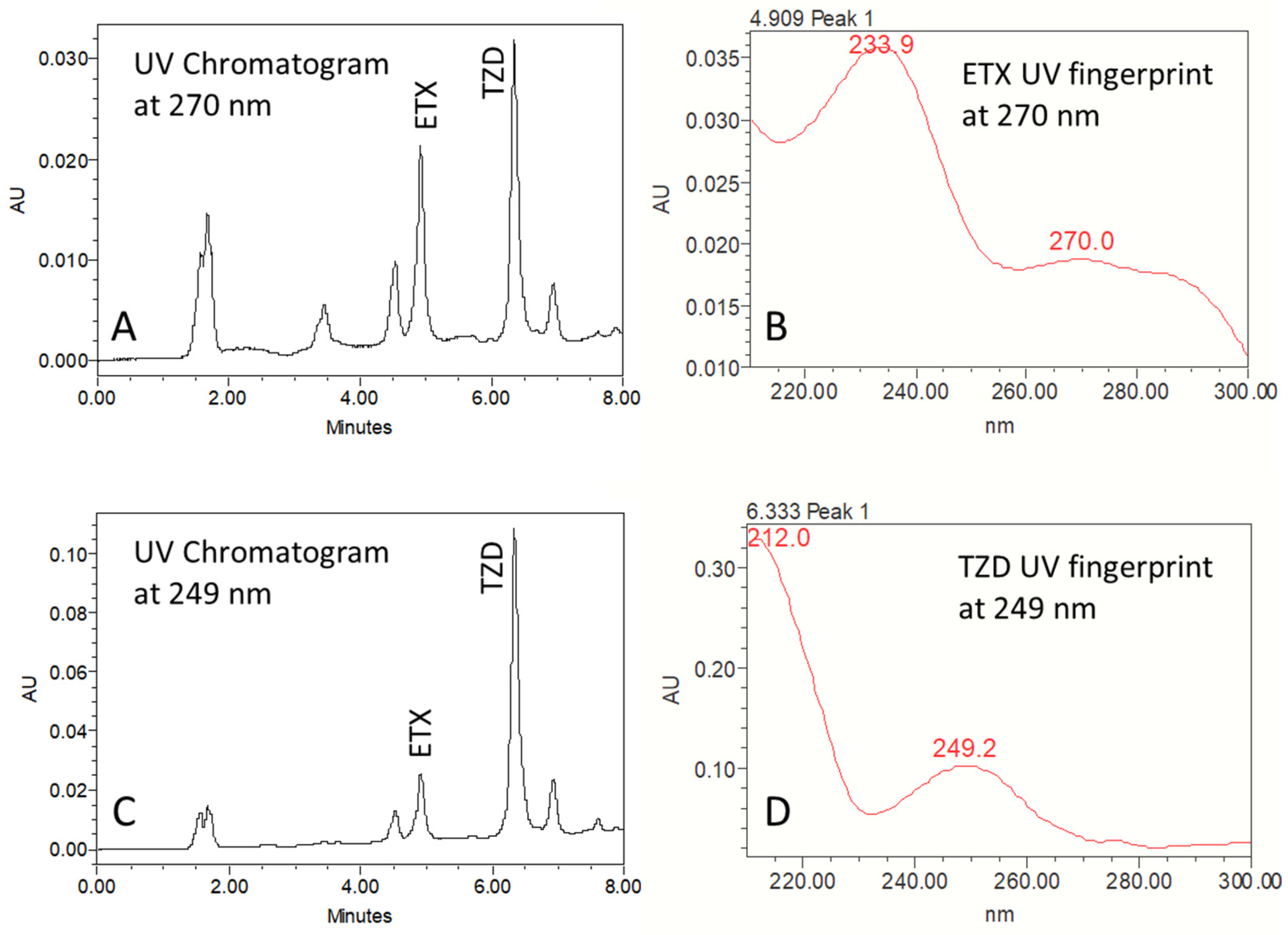
2.1. Chromatography
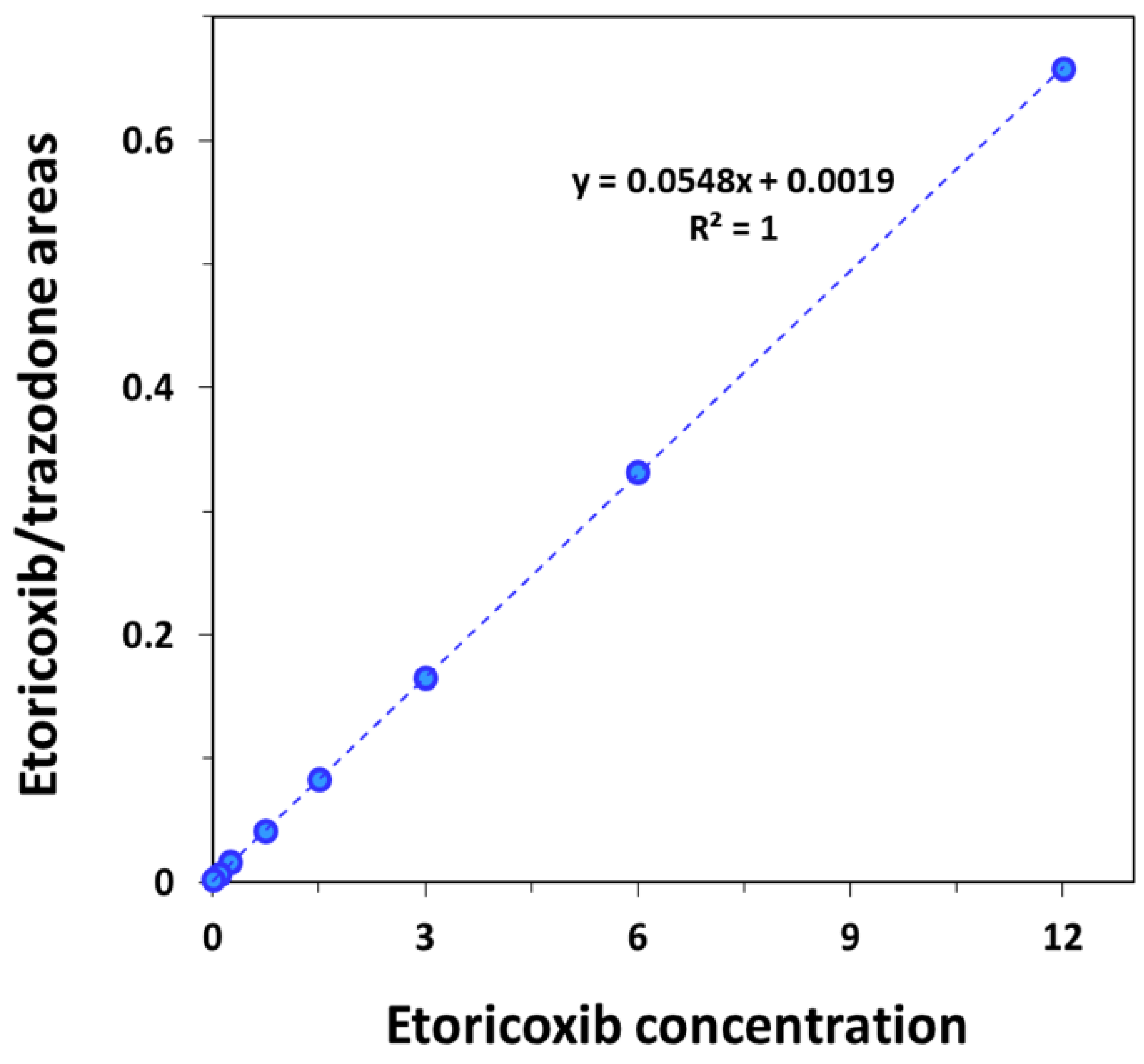
2.2. Method Validation
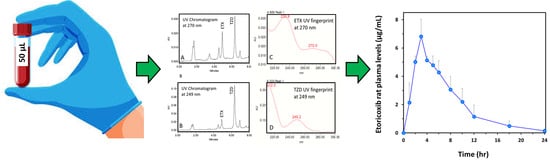
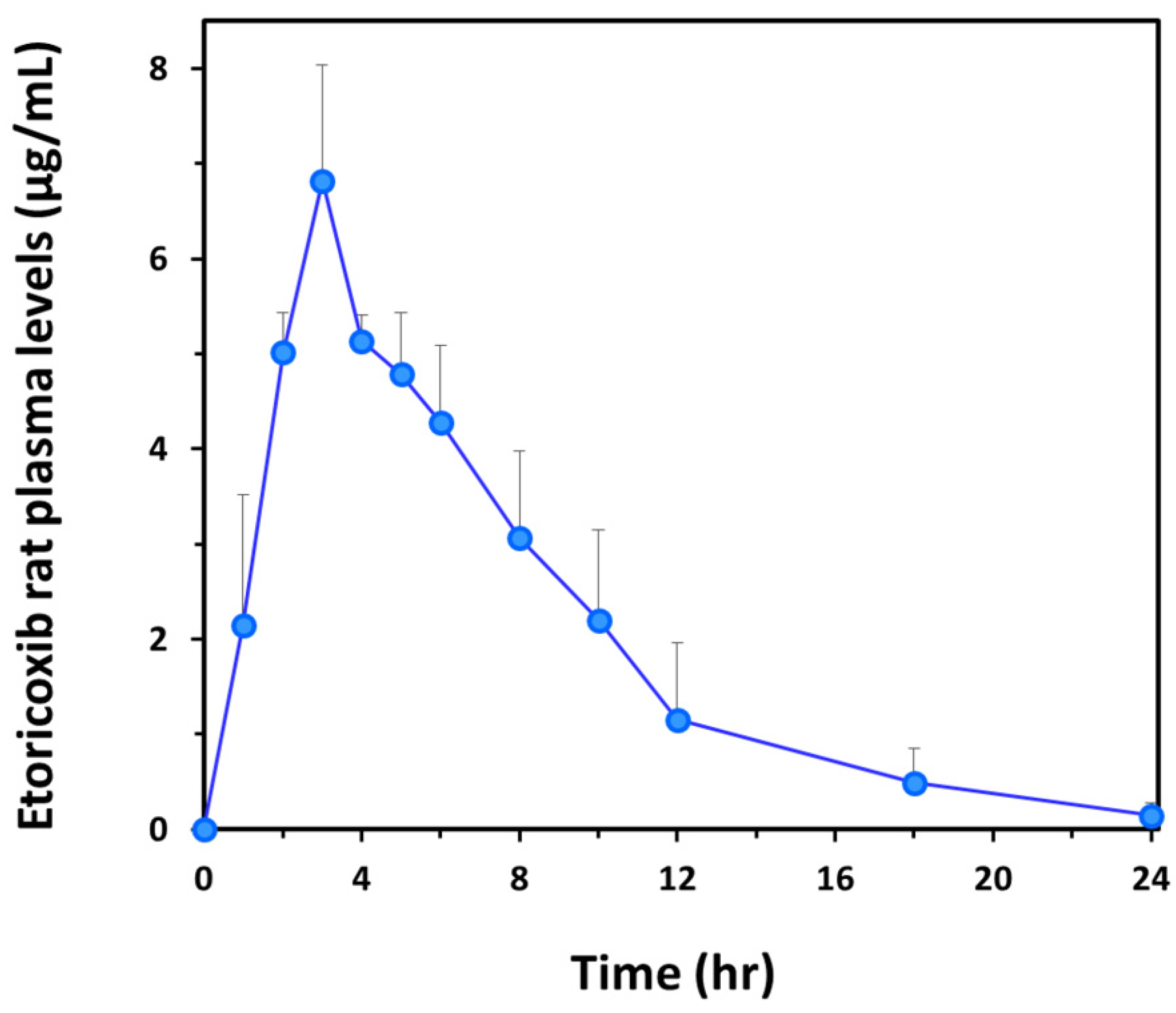
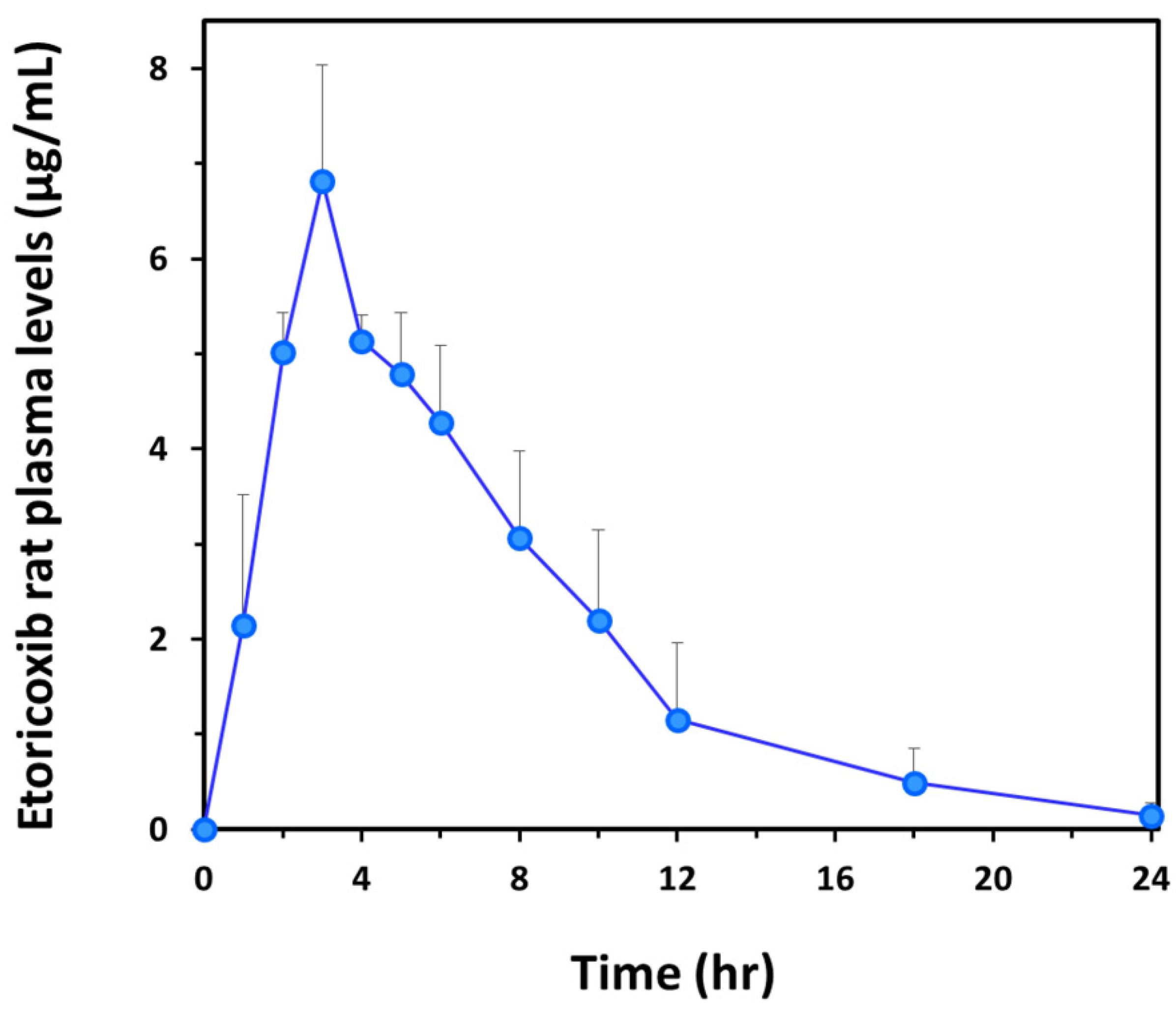
2.3. Pharmacokinetic Study
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Stocks and Working Solutions
4.3. Equipment
4.4. Calibration Curve
4.5. Method Validation
4.6. Pharmacokinetic Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clarke, R.; Derry, S.; Moore, R.A. Single dose oral etoricoxib for acute postoperative pain in adults. Cochrane Database Syst. Rev. 2014, 2014, CD004309. [Google Scholar] [CrossRef]
- Cochrane, D.J.; Jarvis, B.; Keating, G.M. Etoricoxib. Drugs 2002, 62, 2637–2651, discussion 2633–2652. [Google Scholar] [CrossRef]
- Takemoto, J.K.; Reynolds, J.K.; Remsberg, C.M.; Vega-Villa, K.R.; Davies, N.M. Clinical pharmacokinetic and pharmacodynamic profile of etoricoxib. Clin. Pharmacokinet. 2008, 47, 703–720. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Alvarez, I.; Bermejo, M.; Tsume, Y.; Ruiz-Picazo, A.; Gonzalez-Alvarez, M.; Hens, B.; Garcia-Arieta, A.; Amidon, G.E.; Amidon, G.L. An In Vivo Predictive Dissolution Methodology (iPD Methodology) with a BCS Class IIb Drug Can Predict the In Vivo Bioequivalence Results: Etoricoxib Products. Pharmaceutics 2021, 13, 507. [Google Scholar] [CrossRef]
- Matthews, C.Z.; Woolf, E.J.; Lin, L.; Fang, W.; Hsieh, J.; Ha, S.; Simpson, R.; Matuszewski, B.K. High-throughput, semi-automated determination of a cyclooxygenase II inhibitor in human plasma and urine using solid-phase extraction in the 96-well format and high-performance liquid chromatography with post-column photochemical derivatization-fluorescence detection. J. Chromatogr. B Biomed. Sci. Appl. 2001, 751, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, N.V.; Vishwottam, K.N.; Wishu, S.; Koteshwara, M. Validated liquid chromatographic ultraviolet method for the quantitation of Etoricoxib in human plasma using liquid-liquid extraction. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2005, 816, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Pavan Kumar, V.V.; Vinu, M.C.; Ramani, A.V.; Mullangi, R.; Srinivas, N.R. Simultaneous quantitation of etoricoxib, salicylic acid, valdecoxib, ketoprofen, nimesulide and celecoxib in plasma by high-performance liquid chromatography with UV detection. Biomed. Chromatogr. 2006, 20, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Rose, M.J.; Agrawal, N.; Woolf, E.J.; Matuszewski, B.K. Simultaneous determination of unlabeled and carbon-13-labeled etoricoxib, a new cyclooxygenase-2 inhibitor, in human plasma using HPLC-MS/MS. J. Pharm. Sci. 2002, 91, 405–416. [Google Scholar] [CrossRef]
- Brautigam, L.; Nefflen, J.U.; Geisslinger, G. Determination of etoricoxib in human plasma by liquid chromatography-tandem mass spectrometry with electrospray ionisation. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2003, 788, 309–315. [Google Scholar] [CrossRef]
- Zhang, X.; Guo, N.; Ji, W.; Wen, Q. Rapid quantitative analysis of etoricoxib in human plasma by UPLC-MS/MS and application to a pharmacokinetic study in Chinese healthy volunteers. Biomed. Chromatogr. 2019, 33, e4414. [Google Scholar] [CrossRef]
- Brigham, N.C.; Nofsinger, R.; Luo, X.; Dreger, N.Z.; Abel, A.K.; Gustafson, T.P.; Forster, S.P.; Hermans, A.; Ji, R.R.; Becker, M.L. Controlled release of etoricoxib from poly(ester urea) films for post-operative pain management. J. Control. Release 2021, 329, 316–327. [Google Scholar] [CrossRef] [PubMed]
- Kirschneck, C.; Kuchler, E.C.; Wahlmann, U.; Proff, P.; Schroder, A. Effects of the highly COX-2-selective analgesic NSAID etoricoxib on the rate of orthodontic tooth movement and cranial growth. Ann. Anat. 2018, 220, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Balap, A.; Atre, B.; Lohidasan, S.; Sinnathambi, A.; Mahadik, K. Pharmacokinetic and pharmacodynamic herb-drug interaction of Andrographis paniculata (Nees) extract and andrographolide with etoricoxib after oral administration in rats. J. Ethnopharmacol. 2016, 183, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Loh, G.O.K.; Wong, E.Y.L.; Tan, Y.T.F.; Heng, S.C.; Saaid, M.; Cheah, K.Y.; Mohd Sali, N.D.; Damenthi, N.; Ng, S.S.M.; Ming, L.C.; et al. Fast and Sensitive HPLC-ESI-MS/MS Method for Etoricoxib Quantification in Human Plasma and Application to Bioequivalence Study. Molecules 2022, 27, 5706. [Google Scholar] [CrossRef] [PubMed]
- Xie, F.; Liu, L.; Wang, Y.; Peng, Y.; Li, S. An UPLC-PDA assay for simultaneous determination of seven antibiotics in human plasma. J. Pharm. Biomed. Anal. 2022, 210, 114558. [Google Scholar] [CrossRef] [PubMed]
- Beig, A.; Dahan, A. Quantification of carbamazepine and its 10,11-epoxide metabolite in rat plasma by UPLC-UV and application to pharmacokinetic study. Biomed. Chromatogr. 2014, 28, 934–938. [Google Scholar] [CrossRef] [PubMed]
- Meulman, J.; Davanco, M.G.; Vianna, D.R.B.; da Silva, T.M.; Costa, F.; Pacheco, F.B.C.; de Oliveira, M.E.; Vespasiano, C.F.P. Etoricoxib Coated Tablets: Bioequivalence Assessment between Two Formulations Administered under Fasting Conditions. Pharmaceutics 2023, 15, 2569. [Google Scholar] [CrossRef] [PubMed]
- Sapkal, S.B.; Adhao, V.S.; Thenge, R.R.; Darakhe, R.A.; Shinde, S.A.; Shrikhande, V.N. Formulation and Characterization of Solid Dispersions of Etoricoxib Using Natural Polymers. Turk. J. Pharm. Sci. 2020, 17, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Salama, A.H.; Abdelkhalek, A.A.; Elkasabgy, N.A. Etoricoxib-loaded bio-adhesive hybridized polylactic acid-based nanoparticles as an intra-articular injection for the treatment of osteoarthritis. Int. J. Pharm. 2020, 578, 119081. [Google Scholar] [CrossRef]
- Arunkumar, P.; Indulekha, S.; Vijayalakshmi, S.; Srivastava, R. Poly (caprolactone) microparticles and chitosan thermogels based injectable formulation of etoricoxib for the potential treatment of osteoarthritis. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 61, 534–544. [Google Scholar] [CrossRef]
- Kulkarni, V.S.; Alagarsamy, V.; Solomon, V.R.; Jose, P.A.; Murugesan, S. Drug Repurposing: An Effective Tool in Modern Drug Discovery. Russ. J. Bioorg. Chem. 2023, 49, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Bak, U.; Krupa, A. Challenges and Opportunities for Celecoxib Repurposing. Pharm. Res. 2023, 40, 2329–2345. [Google Scholar] [CrossRef] [PubMed]
- Md, S.; Alhakamy, N.A.; Alharbi, W.S.; Ahmad, J.; Shaik, R.A.; Ibrahim, I.M.; Ali, J. Development and Evaluation of Repurposed Etoricoxib Loaded Nanoemulsion for Improving Anticancer Activities against Lung Cancer Cells. Int. J. Mol. Sci. 2021, 22, 13284. [Google Scholar] [CrossRef] [PubMed]
- Kuzminska, J.; Sobczak, A.; Majchrzak-Celinska, A.; Zolnowska, I.; Gostynska, A.; Jadach, B.; Krajka-Kuzniak, V.; Jelinska, A.; Stawny, M. Etoricoxib-Cannabidiol Combo: Potential Role in Glioblastoma Treatment and Development of PLGA-Based Nanoparticles. Pharmaceutics 2023, 15, 2104. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.; Ou, S.; Dong, X.; Liu, J.; Xiao, C. Association of Etoricoxib treatment and incident hypoxia in patients with aortic dissection undergoing endovascular aortic repair. Biomed. Pharmacother. 2021, 139, 111625. [Google Scholar] [CrossRef] [PubMed]
- Kabir, F.; Nahar, K.; Rahman, M.M.; Mamun, F.; Lasker, S.; Khan, F.; Yasmin, T.; Akter, K.A.; Subhan, N.; Alam, M.A. Etoricoxib treatment prevented body weight gain and ameliorated oxidative stress in the liver of high-fat diet-fed rats. Naunyn Schmiedeberg’s Arch. Pharmacol. 2021, 394, 33–47. [Google Scholar] [CrossRef] [PubMed]
- Tjandrawinata, R.R.; Setiawati, A.; Nofiarny, D.; Susanto, L.W.; Setiawati, E. Pharmacokinetic equivalence study of nonsteroidal anti-inflammatory drug etoricoxib. Clin. Pharmacol. 2018, 10, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, N.G.; Porras, A.G.; Matthews, C.Z.; Rose, M.J.; Woolf, E.J.; Musser, B.J.; Dynder, A.L.; Mazina, K.E.; Lasseter, K.C.; Hunt, T.L.; et al. Single- and multiple-dose pharmacokinetics of etoricoxib, a selective inhibitor of cyclooxygenase-2, in man. J. Clin. Pharmacol. 2003, 43, 268–276. [Google Scholar] [CrossRef]
- Zaghloul, I.; Abdelbaky, N. Stability indicating high performance liquid chromatographic assay for the pharmacokinetics of cyclooxygenase (COX-2) inhibitor etoricoxib in rats. Afr. J. Pharm. Pharmacol. 2009, 3, 339–346. [Google Scholar]
- Lipka, E.; Amidon, G.L. Setting bioequivalence requirements for drug development based on preclinical data: Optimizing oral drug delivery systems. J. Control. Release 1999, 62, 41–49. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Spiked Concentration (µg/mL) | Measured Area Overall Mean ± SD (μg∙h/mL) | Intra-Day Precision (%) | Inter-Day Precision (%) | Accuracy (%) |
|---|---|---|---|---|
| 0.1 | 18,188 ± 859 | 2.65 | 4.72 | 3.97 |
| 3 | 536,753 ± 12,531 | 1.69 | 2.33 | 1.26 |
| 12 | 2,152,069 ± 35,528 | 0.39 | 1.57 | 1.54 |
| Parameter | Description | Mean (SD) | Rat 1 | Rat 2 | Rat 3 |
|---|---|---|---|---|---|
| t1/2 | Half-life, h | 3.7 (1.0) | 4.5 | 2.5 | 3.6 |
| tmax | Time to reach Cmax, h | 3 | 3 | 3 | 3 |
| Cmax | Maximum plasma concentration, µg/mL | 6.8 (1.2) | 5.5 | 7.9 | 7.0 |
| AUC0–t | Area under the curve (0–t), μg∙h/mL | 48.9 (13.0) | 51.8 | 37.7 | 63.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ifrah, S.; Porat, D.; Deutsch, M.; Dahan, A. Quantification of Etoricoxib in Low Plasma Volume by UPLC-PDA and Application to Preclinical Pharmacokinetic Study. Pharmaceuticals 2024, 17, 507. https://doi.org/10.3390/ph17040507
Ifrah S, Porat D, Deutsch M, Dahan A. Quantification of Etoricoxib in Low Plasma Volume by UPLC-PDA and Application to Preclinical Pharmacokinetic Study. Pharmaceuticals. 2024; 17(4):507. https://doi.org/10.3390/ph17040507
Chicago/Turabian StyleIfrah, Sapir, Daniel Porat, Mordechai Deutsch, and Arik Dahan. 2024. "Quantification of Etoricoxib in Low Plasma Volume by UPLC-PDA and Application to Preclinical Pharmacokinetic Study" Pharmaceuticals 17, no. 4: 507. https://doi.org/10.3390/ph17040507
APA StyleIfrah, S., Porat, D., Deutsch, M., & Dahan, A. (2024). Quantification of Etoricoxib in Low Plasma Volume by UPLC-PDA and Application to Preclinical Pharmacokinetic Study. Pharmaceuticals, 17(4), 507. https://doi.org/10.3390/ph17040507