
Neurological Adverse Events Related to Immune Checkpoint Inhibitors: A Practical Review

Abstract
1. Introduction
2. General Management
2.1. Classification
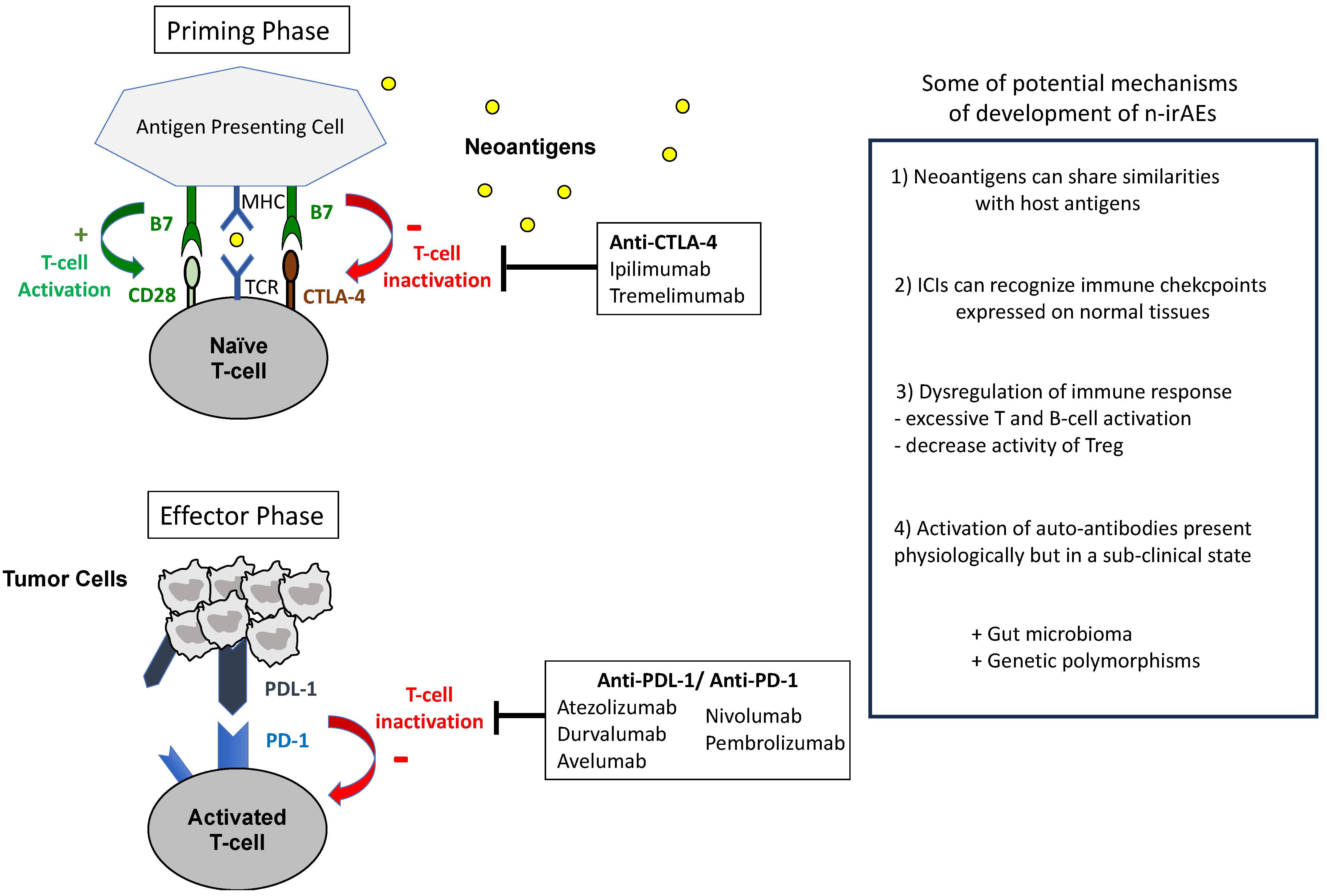
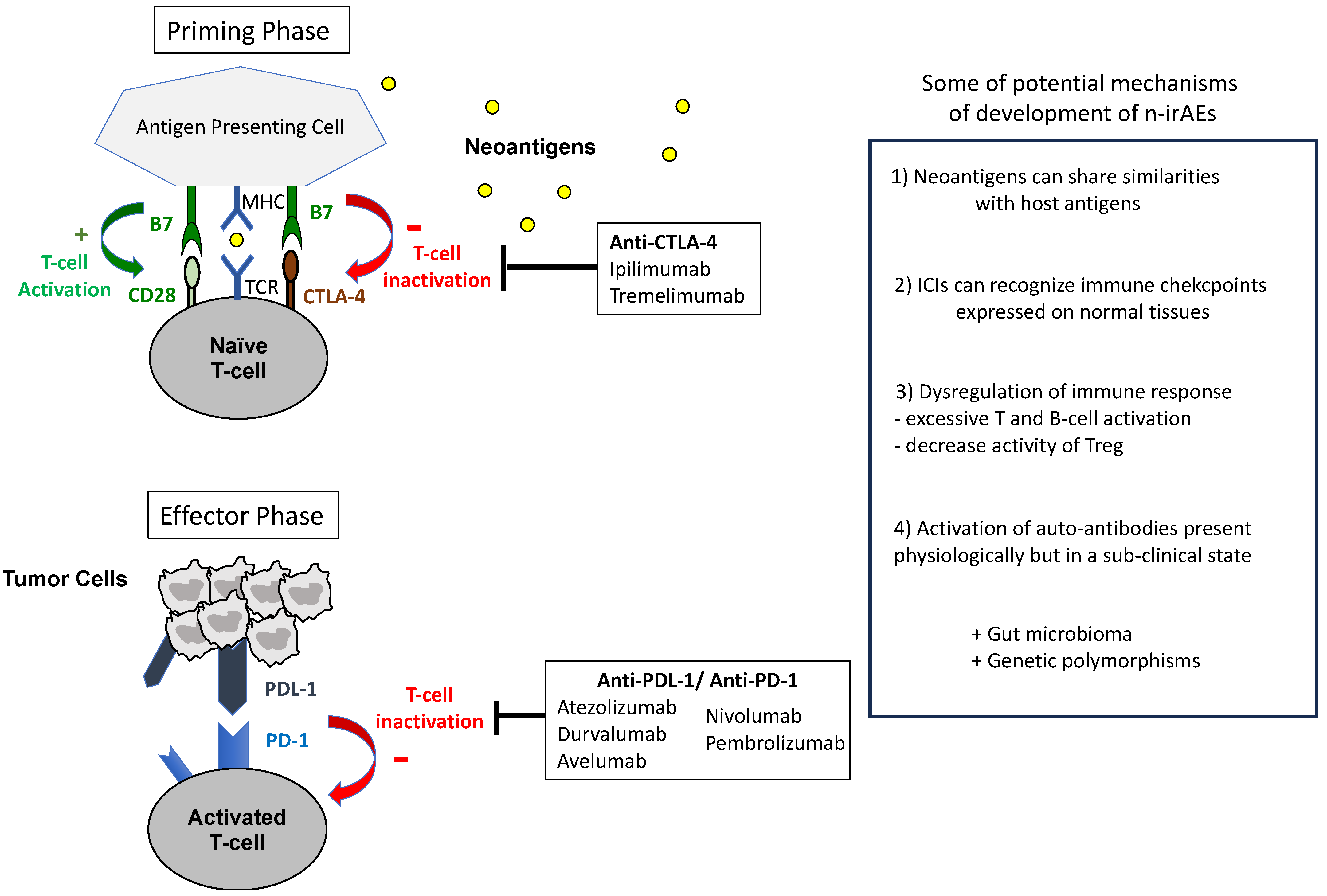
2.2. Pathogenesis
2.3. Approaching the Diagnosis
- (a)
- Timing is crucial for identifying n-irAEs, as they usually emerge within 3–6 months after initiating ICI treatment, with a median onset of 4 weeks (ranging from 1 to 85 weeks) [9,22,23,24,25]. Neurological symptoms emerging beyond 6 months after the last ICI dose are less likely to be secondary to an irAE, although it cannot be entirely ruled out solely on this basis [8];
- (b)
- Clinical and/or radiological evidence of cancer control coinciding with the onset of neurological symptoms supports n-irAE diagnosis rather than attributing the symptoms to cancer progression [22];
- (c)
- (d)
- A positive response to ICI interruption and/or immunosuppression also suggests a n-irAE, although it is not a definitive indicator [8].
2.4. Diagnosis Tools
3. Importance of Rapid Diagnosis and Severity Score
4. Recognizing the Key Neurological Immune-Related Adverse Events
4.1. irMyopathy/Myositis (irM/M)
4.1.1. General Overview
4.1.2. Clinical Presentation
- -
- Proximal limb muscles are more affected than distal ones, leading to limitations in ambulating, raising, and lifting arms;
- -
- Axial weakness, particularly in the cervical region, results in difficulties in neck extension and flexion;
- -
- Oculo-bulbar involvement, characterized by ptosis, diplopia, dysphagia, and dysarthria, is a distinct and prominent feature of irM/M, being the primary or sole manifestation in 42% of patients, contrasting with those unexposed to ICI [37].
4.1.3. Diagnostic Tools
- -
- -
- -
- EKG and troponin levels;
- -
- Assessment of MG-specific antibodies (AChR, MuSK, LRP4) can also help to evaluate the presence of co-occurring myasthenia, especially when ocular or bulbar symptoms are present [35,37]. While myositis-specific antibodies (e.g., ANA, Jo-1, PL-7, PL-12, EJ) may be considered for pretherapeutic muscular manifestations or suspected underlying dermatomyositis, they often yield negative results in ir-M/M [31,37,38];
- -
- Limb MRI with contrast typically reveals STIR hyperintensity or contrast enhancement in affected muscles. While these findings are non-specific and can be observed in denervated muscles, they provide diagnostic support and assist in directing biopsy [8].
- -
- -
- Pulmonary function tests and video-fluoroscopic swallow studies to assess restrictive syndromes and dysphagia, respectively.
4.2. irNeuromuscular Junction Disorders (irNMJD), Including Mysthenia Gravis (MG)
4.2.1. General Overview
4.2.2. Clinical Presentation
- -
- Proximal and axial cervical muscles (neck and shoulder weakness) [16];
- -
- Ocular muscles (diplopia, asymmetrical ptosis, and/or fatigability);
- -
- Bulbar muscles (dysphagia, dysphonia, and dysarthria);
- -
4.2.3. Diagnostic Tools
- -
- Electrodiagnostic studies to detect a decremental pattern (reduction in the amplitude of action potentials with repeated nerve stimulation), a hallmark of MG [45];
- -
- -
- Consideration of MuSK and LRP4 antibodies, especially in those with pre-existing NMJ disorders, due to their rare documentation [41];
- -
- Myocarditis and myositis evaluation via EKG, troponin, CK, or aldolase, given their frequent association with irNMJD;
- -
- MRI of the brain, spinal cord, or orbit to exclude cancer involvement of CNS.
- -
- Pulmonary function tests and fluoroscopic swallow evaluation for patients with respiratory symptoms or dysphagia;
- -
- TSH levels, given the potential impact of thyroid disorders on neuromuscular function.
4.3. irNeuropathy, Including Guillain–Barré Syndrome
4.3.1. General Overview
4.3.2. Clinical Presentation
4.3.3. Diagnostic Tools
- -
- -
- -
- -
- A large infectious screening, as many infections can cause idiopathic GBS: CMV, mycoplasma, HIV, campylobacter, syphilis, Lyme…;
- -
4.4. irMeningitis
4.4.1. General Overview
4.4.2. Clinical Presentation
4.4.3. Diagnostic Tools
4.5. irEncephalitis
4.5.1. General Overview
4.5.2. Clinical Presentation
- -
- Diffuse, meningoencephalitis-like picture, with general symptoms (fever, headache, altered consciousness, and/or seizures) and without focal signs;
- -
- Focal presentations, including limbic encephalitis (neuropsychiatric disturbances, memory issues, behavioral changes, delusions, hallucinations, temporal epilepsy), cerebellitis (ataxia, dysmetria), brainstem encephalitis (altered vigilance, cranial nerve paresis, vertigo, bulbar syndromes), basal ganglia encephalitis (extrapyramidal syndrome with abnormal movements), dysphasia, pyramidal syndrome, sensory disturbances, and dysautonomia.
4.5.3. Diagnostic Tools
- -
- Brain MRI with contrast. The most frequent findings are hyperintensities in the mesial temporal regions on T2/FLAIR sequences for limbic encephalitis and meningeal enhancement/thickening for meningoencephalitis [51]. MRI can be repeated, as radiological abnormalities are sometimes delayed [10,42,52,53,54,55];
- -
- -
- Neuronal antibody testing in blood and CSF. The seropositivity rate ranges from 6% to 54% [52,54]. Specifically, onco-neuronal antibodies targeting intracellular antigens are more common [52]. There have also been reports of other antibodies, including anti-GFAP in the context of meningoencephalitis, as well as anti-Ri, anti-GAD, anti-NMDAR, anti-CASPR2, anti-CRMP5, and anti-SOX1 [42,43]. The presence of these antibodies is often linked to an unfavorable prognosis;
- -
- EEG, which can indicate focal or diffuse slowing, subclinical seizures, or status epilepticus;
- -
- Additional assessments may involve spinal MRI, further infectious workup, and—in rare cases—brain biopsy to rule out oncological progression.
4.6. irDemyelinating Diseases (irDDs)
4.6.1. General Overview
4.6.2. Clinical Presentation
- -
- Involvement of cerebral hemispheres can lead to muscle weakness with pyramidal signs, sensory disturbances, and mental status changes;
- -
- Posterior fossa localization is associated with diplopia, ophthalmoplegia, nystagmus, ataxia, dysmetria, dysarthria, and dysphagia;
- -
- Optic neuropathy results in reduced visual acuity, visual field loss, dyschromatopsia, afferent pupillary defect, and optic disc edema;
- -
- Transverse myelitis manifests as sensory disturbances with a sensory level, pyramidal weakness, and ataxia.
4.6.3. Diagnostic Tools
- -
- Brain, orbit, and/or spinal MRI with contrast, which typically shows enhancements and/or hyperintense T2/FLAIR lesions, although no definitive imaging feature has been identified [43];
- -
- Lumbar puncture, usually revealing lymphocytic pleocytosis and elevated protein levels [56];
- -
- Autoantibody testing, including demyelinating antibodies (i.e., AQP4 and MOG) in serum and spinal fluid, although the impact on sensitivity is limited compared to serum analysis alone. While most patients test negative for these antibodies, AQP4, CRMP5, Hu, or other neural antibodies can be present in some patients [10,43,56,57];
- -
- Other diagnostic tools include EEG, neuro-ophthalmologic evaluation and evoked potentials;
- -
- Brain biopsy—exceptionally—to allow definitive proof of CNS demyelination.
5. Treatment
5.1. General Management
- (a)
- Prioritize excluding bacterial infections and—if feasible—viral infections before initiating immunosuppression;
- (b)
- Administer antimicrobials concurrently while awaiting negative PCR and culture results, particularly in severe cases.
5.2. Steroids, IVIG, and Plasmapheresis
5.3. ICI Re-Challenge
- -
- ICI re-challenge or continuation should always be discussed with the patient, and the risk/benefit balance should always be weighted. A close collaboration with neurologists specialized in n-irAEs is highly recommended;
- -
- Since irAEs may correlate with an oncologic response, assessing disease control before deciding to re-challenge or continue ICI therapy is crucial in evaluating the real benefit for the patient. Retrospective analysis of a cohort of 937 patients with melanoma treated with ICIs showed an association between the development of n-irAEs (n = 76, 8%) and longer survival (HR = 0.4, 95% CI 0.32–0.77) [63];
- -
- Reinitiating ICI can be considered if irAE severity did not exceed Grade 1 or 2, the patient’s symptoms have resolved or at least stabilized, and corticosteroids have been reduced to a dose of less than 10 mg/day of prednisone [16]. However, particularly in Grade 2, the oncological situation should be re-evaluated in order to confirm the need to reinitiate ICI.
- -
- However, for severe symptoms (Grades 3 and 4) or conditions such as MG, GBS, or transverse myelitis, permanent ICI discontinuation is advised [16].
5.4. Pre-Existing Autoimmune and Paraneoplastic Neurological Syndromes (PNSs)
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Iranzo, P.; Callejo, A.; Assaf, J.D.; Molina, G.; Lopez, D.E.; Garcia-Illescas, D.; Pardo, N.; Navarro, A.; Martinez-Marti, A.; Cedres, S.; et al. Overview of Checkpoint Inhibitors Mechanism of Action: Role of Immune-Related Adverse Events and Their Treatment on Progression of Underlying Cancer. Front. Med. 2022, 9, 875974. [Google Scholar] [CrossRef]
- Riha, P.; Rudd, C.E. CD28 Co-Signaling in the Adaptive Immune Response. Self Nonself 2010, 1, 231. [Google Scholar] [CrossRef]
- Patsoukis, N.; Brown, J.; Petkova, V.; Liu, F.; Li, L.; Boussiotis, V.A. Selective Effects of PD-1 on Akt and Ras Pathways Regulate Molecular Components of the Cell Cycle and Inhibit T Cell Proliferation. Sci. Signal. 2012, 5, ra46. [Google Scholar] [CrossRef]
- Shiravand, Y.; Khodadadi, F.; Kashani, S.M.A.; Hosseini-Fard, S.R.; Hosseini, S.; Sadeghirad, H.; Ladwa, R.; O’byrne, K.; Kulasinghe, A. Immune Checkpoint Inhibitors in Cancer Therapy. Curr. Oncol. 2022, 29, 3044. [Google Scholar] [CrossRef]
- Haslam, A.; Gill, J.; Prasad, V. Estimation of the Percentage of US Patients with Cancer Who Are Eligible for Immune Checkpoint Inhibitor Drugs. JAMA Netw. Open 2020, 3, e200423. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Zhang, D.; Cui, X.; Zhang, L. Meta-Analysis of Immune-Related Adverse Events of Immune Checkpoint Inhibitor Therapy in Cancer Patients. Thorac. Cancer 2020, 11, 2406–2430. [Google Scholar] [CrossRef] [PubMed]
- Cuzzubbo, S.; Javeri, F.; Tissier, M.; Roumi, A.; Barlog, C.; Doridam, J.; Lebbe, C.; Belin, C.; Ursu, R.; Carpentier, A.F. Neurological Adverse Events Associated with Immune Checkpoint Inhibitors: Review of the Literature. Eur. J. Cancer 2017, 73, 1–8. [Google Scholar] [CrossRef]
- Guidon, A.C.; Burton, L.B.; Chwalisz, B.K.; Hillis, J.; Schaller, T.H.; Amato, A.A.; Betof Warner, A.; Brastianos, P.K.; Cho, T.A.; Clardy, S.L.; et al. Consensus Disease Definitions for Neurologic Immune-Related Adverse Events of Immune Checkpoint Inhibitors. J. Immunother. Cancer 2021, 9, e002890. [Google Scholar] [CrossRef] [PubMed]
- Babu, A.P.; Sharda, E.; Kolli, A.; Mora-Rodriguez, K.; Boldig, C.; Gatewood, T.; Shah, A.; Swank, J.; Pina, Y.; Peguero, E.; et al. Neurological Complications of Immune Checkpoint Inhibitors (P12-13.004). Neurology 2023, 100, 2188. [Google Scholar] [CrossRef]
- Marini, A.; Bernardini, A.; Gigli, G.L.; Valente, M.; Muñiz-Castrillo, S.; Honnorat, J.; Vogrig, A. Neurologic Adverse Events of Immune Checkpoint Inhibitors: A Systematic Review. Neurology 2021, 96, 754–766. [Google Scholar] [CrossRef]
- Dubey, D.; David, W.S.; Reynolds, K.L.; Chute, D.F.; Clement, N.F.; Cohen, J.V.; Lawrence, D.P.; Mooradian, M.J.; Sullivan, R.J.; Guidon, A.C. Severe Neurological Toxicity of Immune Checkpoint Inhibitors: Growing Spectrum. Ann. Neurol. 2020, 87, 659–669. [Google Scholar] [CrossRef]
- Wang, D.Y.; Salem, J.E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L.; et al. Fatal Toxic Effects Associated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Khan, E.; Shrestha, A.K.; Elkhooly, M.; Wilson, H.; Ebbert, M.; Srivastava, S.; Wen, S.; Rollins, S.; Sriwastava, S. CNS and PNS Manifestation in Immune Checkpoint Inhibitors: A Systematic Review. J. Neurol. Sci. 2022, 432, 120089. [Google Scholar] [CrossRef]
- Haanen, J.; Obeid, M.; Spain, L.; Carbonnel, F.; Wang, Y.; Robert, C.; Lyon, A.R.; Wick, W.; Kostine, M.; Peters, S.; et al. Management of Toxicities from Immunotherapy: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-up. Ann. Oncol. 2022, 33, 1217–1238. [Google Scholar] [CrossRef] [PubMed]
- Schneider, B.J.; Naidoo, J.; Santomasso, B.D.; Lacchetti, C.; Adkins, S.; Anadkat, M.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; et al. Management of Immune-Related Adverse Events in Patients Treated with Immune Checkpoint Inhibitor Therapy: ASCO Guideline Update. J. Clin. Oncol. 2021, 39, 4073–4126. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Abu-Sbeih, H.; Ascierto, P.A.; Brufsky, J.; Cappelli, L.C.; Cortazar, F.B.; Gerber, D.E.; Hamad, L.; Hansen, E.; Johnson, D.B.; et al. Society for Immunotherapy of Cancer (SITC) Clinical Practice Guideline on Immune Checkpoint Inhibitor-Related Adverse Events. J. Immunother. Cancer 2021, 9, e002435. [Google Scholar] [CrossRef]
- Vilariño, N.; Bruna, J.; Kalofonou, F.; Anastopoulou, G.G.; Argyriou, A.A. Immune-Driven Pathogenesis of Neurotoxicity after Exposure of Cancer Patients to Immune Checkpoint Inhibitors. Int. J. Mol. Sci. 2020, 21, 5774. [Google Scholar] [CrossRef]
- Menotti, S.; Giampietro, A.; Raia, S.; Veleno, M.; Angelini, F.; Tartaglione, T.; Gaudino, S.; Doglietto, F.; De Marinis, L.; Pontecorvi, A.; et al. Unveiling the Etiopathogenic Spectrum of Hypophysitis: A Narrative Review. J. Pers. Med. 2023, 13, 1210. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Casals, M.; Brahmer, J.R.; Callahan, M.K.; Flores-Chávez, A.; Keegan, N.; Khamashta, M.A.; Lambotte, O.; Mariette, X.; Prat, A.; Suárez-Almazor, M.E. Immune-Related Adverse Events of Checkpoint Inhibitors. Nat. Rev. Dis. Primers 2020, 6, 38. [Google Scholar] [CrossRef]
- Zhang, Y.; Cheng, S.; Zou, H.; Han, Z.; Xie, T.; Zhang, B.; Dai, D.; Yin, X.; Liang, Y.; Kou, Y.; et al. Correlation of the Gut Microbiome and Immune-Related Adverse Events in Gastrointestinal Cancer Patients Treated with Immune Checkpoint Inhibitors. Front. Cell. Infect. Microbiol. 2023, 13, 1099063. [Google Scholar] [CrossRef]
- Chaput, N.; Lepage, P.; Coutzac, C.; Soularue, E.; Le Roux, K.; Monot, C.; Boselli, L.; Routier, E.; Cassard, L.; Collins, M.; et al. Baseline Gut Microbiota Predicts Clinical Response and Colitis in Metastatic Melanoma Patients Treated with Ipilimumab. Ann. Oncol. 2017, 28, 1368–1379. [Google Scholar] [CrossRef] [PubMed]
- Vogrig, A.; Muñiz-Castrillo, S.; Farina, A.; Honnorat, J.; Joubert, B. How to Diagnose and Manage Neurological Toxicities of Immune Checkpoint Inhibitors: An Update. J. Neurol. 2022, 269, 1701–1714. [Google Scholar] [CrossRef] [PubMed]
- Dubey, D.; David, W.; Reynolds, K.; Chute, D.; Clement, N.F.; Cohen, J.V.; Lawrence, D.P.; Mooradian, M.J.; Sullivan, R.J.; Guidon, A. Immune Checkpoint Inhibitor Related Neurologic Adverse Events: Clinical Spectrum, Management and Outcomes (S21.003). Neurology 2019, 92, 15. [Google Scholar] [CrossRef]
- Johnson, D.B.; Manouchehri, A.; Haugh, A.M.; Quach, H.T.; Balko, J.M.; Lebrun-Vignes, B.; Mammen, A.; Moslehi, J.J.; Salem, J.E. Neurologic Toxicity Associated with Immune Checkpoint Inhibitors: A Pharmacovigilance Study. J. Immunother. Cancer 2019, 7, 134. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.Q.; Tang, L.L.; Mao, Y.P.; Li, W.F.; Chen, L.; Zhang, Y.; Guo, Y.; Liu, Q.; Sun, Y.; Xu, C.; et al. The Pattern of Time to Onset and Resolution of Immune-Related Adverse Events Caused by Immune Checkpoint Inhibitors in Cancer: A Pooled Analysis of 23 Clinical Trials and 8,436 Patients. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2021, 53, 339. [Google Scholar] [CrossRef]
- Seki, M.; Kitano, S.; Suzuki, S. Neurological Disorders Associated with Immune Checkpoint Inhibitors: An Association with Autoantibodies. Cancer Immunol. Immunother. 2022, 71, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Déchelotte, B.; Muñiz-Castrillo, S.; Joubert, B.; Vogrig, A.; Picard, G.; Rogemond, V.; Pinto, A.L.; Lombard, C.; Desestret, V.; Fabien, N.; et al. Diagnostic Yield of Commercial Immunodots to Diagnose Paraneoplastic Neurologic Syndromes. Neurol. Neuroimmunol. Neuroinflammation 2020, 7, e701. [Google Scholar] [CrossRef]
- Belgian Multidisciplinary Immunotoxicity Board (BITOX)—BSMO. Available online: https://www.bsmo.be/immunomanager/start/ (accessed on 27 November 2023).
- Zubiri, L.; Molina, G.E.; Mooradian, M.J.; Cohen, J.; Durbin, S.M.; Petrillo, L.; Boland, G.M.; Juric, D.; Dougan, M.; Thomas, M.F.; et al. Effect of a Multidisciplinary Severe Immunotherapy Complications Service on Outcomes for Patients Receiving Immune Checkpoint Inhibitor Therapy for Cancer. J. Immunother. Cancer 2021, 9, e002886. [Google Scholar] [CrossRef]
- Moreira, A.; Loquai, C.; Pföhler, C.; Kähler, K.C.; Knauss, S.; Heppt, M.V.; Gutzmer, R.; Dimitriou, F.; Meier, F.; Mitzel-Rink, H.; et al. Myositis and Neuromuscular Side-Effects Induced by Immune Checkpoint Inhibitors. Eur. J. Cancer 2019, 106, 12–23. [Google Scholar] [CrossRef]
- Touat, M.; Maisonobe, T.; Knauss, S.; Ben Hadj Salem, O.; Hervier, B.; Auré, K.; Szwebel, T.A.; Kramkimel, N.; Lethrosne, C.; Bruch, J.F.; et al. Immune Checkpoint Inhibitor-Related Myositis and Myocarditis in Patients with Cancer. Neurology 2018, 91, e985–e994. [Google Scholar] [CrossRef]
- Rossi, S.; Gelsomino, F.; Rinaldi, R.; Muccioli, L.; Comito, F.; Di Federico, A.; De Giglio, A.; Lamberti, G.; Andrini, E.; Mollica, V.; et al. Peripheral Nervous System Adverse Events Associated with Immune Checkpoint Inhibitors. J. Neurol. 2023, 270, 2975–2986. [Google Scholar] [CrossRef] [PubMed]
- Cappelli, L.C.; Gutierrez, A.K.; Bingham, C.O.; Shah, A.A. Rheumatic and Musculoskeletal Immune-Related Adverse Events Due to Immune Checkpoint Inhibitors: A Systematic Review of the Literature. Arthritis Care Res. 2017, 69, 1751–1763. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Tayar, J.H.; Abdel-Wahab, N.; Suarez-Almazor, M.E. Myositis as an Adverse Event of Immune Checkpoint Blockade for Cancer Therapy. Semin. Arthritis Rheum. 2019, 48, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Aldrich, J.; Pundole, X.; Tummala, S.; Palaskas, N.; Andersen, C.R.; Shoukier, M.; Abdel-Wahab, N.; Deswal, A.; Suarez-Almazor, M.E. Inflammatory Myositis in Cancer Patients Receiving Immune Checkpoint Inhibitors. Arthritis Rheumatol. 2021, 73, 866–874. [Google Scholar] [CrossRef] [PubMed]
- Pathak, R.; Katel, A.; Massarelli, E.; Villaflor, V.M.; Sun, V.; Salgia, R. Immune Checkpoint Inhibitor–Induced Myocarditis with Myositis/Myasthenia Gravis Overlap Syndrome: A Systematic Review of Cases. Oncologist 2021, 26, 1052–1061. [Google Scholar] [CrossRef] [PubMed]
- Shelly, S.; Triplett, J.D.; Pinto, M.V.; Milone, M.; Diehn, F.E.; Zekeridou, A.; Liewluck, T. Immune Checkpoint Inhibitor-Associated Myopathy: A Clinicoseropathologically Distinct Myopathy. Brain Commun. 2020, 2, fcaa181. [Google Scholar] [CrossRef] [PubMed]
- Sechi, E.; Markovic, S.N.; McKeon, A.; Dubey, D.; Liewluck, T.; Lennon, V.A.; Lopez-Chiriboga, A.S.; Klein, C.J.; Mauermann, M.; Pittock, S.J.; et al. Neurologic Autoimmunity and Immune Checkpoint Inhibitors. Neurology 2020, 95, e2442–e2452. [Google Scholar] [CrossRef] [PubMed]
- Safa, H.; Johnson, D.H.; Trinh, V.A.; Rodgers, T.E.; Lin, H.; Suarez-Almazor, M.E.; Fa’Ak, F.; Saberian, C.; Yee, C.; Davies, M.A.; et al. Immune Checkpoint Inhibitor Related Myasthenia Gravis: Single Center Experience and Systematic Review of the Literature. J. Immunother. Cancer 2019, 7, 319. [Google Scholar] [CrossRef] [PubMed]
- Guidon, A.C. Lambert-Eaton Myasthenic Syndrome, Botulism, and Immune Checkpoint Inhibitor-Related Myasthenia Gravis. Continuum 2019, 25, 1785–1806. [Google Scholar] [CrossRef]
- Huang, Y.T.; Chen, Y.P.; Lin, W.C.; Su, W.C.; Sun, Y.T. Immune Checkpoint Inhibitor-Induced Myasthenia Gravis. Front. Neurol. 2020, 11, 528324. [Google Scholar] [CrossRef]
- Farina, A.; Villagrán-García, M.; Honnorat, J. Neurological Adverse Events of Immune Checkpoint Inhibitors: An Update of Clinical Presentations, Diagnosis, and Management. Rev. Neurol. 2023, 179, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Alsalem, A.N.; Scarffe, L.A.; Briemberg, H.R.; Aaroe, A.E.; Harrison, R.A. Neurologic Complications of Cancer Immunotherapy. Curr. Oncol. 2023, 30, 5876–5897. [Google Scholar] [CrossRef] [PubMed]
- Giannoccaro, M.P.; Paolucci, M.; Zenesini, C.; Di Stasi, V.; Donadio, V.; Avoni, P.; Liguori, R. Comparison of Ice Pack Test and Single-Fiber EMG Diagnostic Accuracy in Patients Referred for Myasthenic Ptosis. Neurology 2020, 95, E1800–E1806. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Haggiagi, A.; Tzatha, E.; DeAngelis, L.M.; Santomasso, B. Electrophysiological Findings in Immune Checkpoint Inhibitor-Related Peripheral Neuropathy. Clin. Neurophysiol. 2019, 130, 1440–1445. [Google Scholar] [CrossRef] [PubMed]
- Dubey, D.; David, W.S.; Amato, A.A.; Reynolds, K.L.; Clement, N.F.; Chute, D.F.; Cohen, J.V.; Lawrence, D.P.; Mooradian, M.J.; Sullivan, R.J.; et al. Varied Phenotypes and Management of Immune Checkpoint Inhibitor-Associated Neuropathies. Neurology 2019, 93, e1093–e1103. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, X.; Zhao, C. Guillain-Barré Syndrome-like Polyneuropathy Associated with Immune Checkpoint Inhibitors: A Systematic Review of 33 Cases. Biomed. Res. Int. 2021, 2021, 9800488. [Google Scholar] [CrossRef] [PubMed]
- Diamanti, L.; Picca, A.; Bini, P.; Gastaldi, M.; Alfonsi, E.; Pichiecchio, A.; Rota, E.; Rudà, R.; Bruno, F.; Villani, V.; et al. Characterization and Management of Neurological Adverse Events during Immune-Checkpoint Inhibitors Treatment: An Italian Multicentric Experience. Neurol. Sci. 2022, 43, 2031–2041. [Google Scholar] [CrossRef] [PubMed]
- Mikami, T.; Liaw, B.; Asada, M.; Niimura, T.; Zamami, Y.; Green-LaRoche, D.; Pai, L.; Levy, M.; Jeyapalan, S. Neuroimmunological Adverse Events Associated with Immune Checkpoint Inhibitor: A Retrospective, Pharmacovigilance Study Using FAERS Database. J. Neurooncol. 2021, 152, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Nannini, S.; Koshenkova, L.; Baloglu, S.; Chaussemy, D.; Noël, G.; Schott, R. Immune-Related Aseptic Meningitis and Strategies to Manage Immune Checkpoint Inhibitor Therapy: A Systematic Review. J. Neurooncol 2022, 157, 533–550. [Google Scholar] [CrossRef]
- Sato, K.; Mano, T.; Iwata, A.; Toda, T. Neurological and Related Adverse Events in Immune Checkpoint Inhibitors: A Pharmacovigilance Study from the Japanese Adverse Drug Event Report Database. J. Neurooncol 2019, 145, 1–9. [Google Scholar] [CrossRef]
- Velasco, R.; Villagrán, M.; Jové, M.; Simó, M.; Vilariño, N.; Alemany, M.; Palmero, R.; Martínez-Villacampa, M.M.; Nadal, E.; Bruna, J. Encephalitis Induced by Immune Checkpoint Inhibitors: A Systematic Review. JAMA Neurol. 2021, 78, 864–873. [Google Scholar] [CrossRef] [PubMed]
- Nersesjan, V.; McWilliam, O.; Krarup, L.H.; Kondziella, D. Autoimmune Encephalitis Related to Cancer Treatment with Immune Checkpoint Inhibitors. Neurology 2021, 97, e191–e202. [Google Scholar] [CrossRef] [PubMed]
- Müller-Jensen, L.; Zierold, S.; Versluis, J.M.; Boehmerle, W.; Huehnchen, P.; Endres, M.; Mohr, R.; Compter, A.; Blank, C.U.; Hagenacker, T.; et al. Characteristics of Immune Checkpoint Inhibitor-Induced Encephalitis and Comparison with HSV-1 and Anti-LGI1 Encephalitis: A Retrospective Multicentre Cohort Study. Eur. J. Cancer 2022, 175, 224–235. [Google Scholar] [CrossRef] [PubMed]
- Vogrig, A.; Muñiz-Castrillo, S.; Joubert, B.; Picard, G.; Rogemond, V.; Marchal, C.; Chiappa, A.M.; Chanson, E.; Skowron, F.; Leblanc, A.; et al. Central Nervous System Complications Associated with Immune Checkpoint Inhibitors. J. Neurol. Neurosurg. Psychiatry 2020, 91, 772–778. [Google Scholar] [CrossRef]
- Oliveira, M.C.B.; de Brito, M.H.; Simabukuro, M.M. Central Nervous System Demyelination Associated with Immune Checkpoint Inhibitors: Review of the Literature. Front. Neurol. 2020, 11, 538695. [Google Scholar] [CrossRef] [PubMed]
- Picca, A.; Berzero, G.; Bihan, K.; Jachiet, V.; Januel, E.; Coustans, M.; Cauquil, C.; Perrin, J.; Berlanga, P.; Kramkimel, N.; et al. Longitudinally Extensive Myelitis Associated with Immune Checkpoint Inhibitors. Neurol. Neuroimmunol. Neuroinflammation 2021, 8, e967. [Google Scholar] [CrossRef] [PubMed]
- Katsumoto, T.R.; Wilson, K.L.; Giri, V.K.; Zhu, H.; Anand, S.; Ramchandran, K.J.; Martin, B.A.; Yunce, M.; Muppidi, S. Plasma Exchange for Severe Immune-Related Adverse Events from Checkpoint Inhibitors: An Early Window of Opportunity? Immunother. Adv. 2022, 2, ltac012. [Google Scholar] [CrossRef] [PubMed]
- Hottinger, A.F.; De Micheli, R.; Guido, V.; Karampera, A.; Hagmann, P.; Du Pasquier, R. Natalizumab May Control Immune Checkpoint Inhibitor–Induced Limbic Encephalitis. Neurol. Neuroimmunol. Neuroinflammation 2018, 5, 439. [Google Scholar] [CrossRef] [PubMed]
- Eskian, M.; Singh, B.; Zubiri, L.; Burton, L.B.; Philpotts, L.; Reynolds, K.; Guidon, A. Immune Checkpoint Inhibitor Rechallenge Following Neurologic Immune-Related Adverse Events in Cancer Patients: A Systematic Review (P8-1.002). Neurology 2022, 98, 18. [Google Scholar] [CrossRef]
- Farina, A.; Birzu, C.; Elsensohn, M.H.; Picca, A.; Muniz-Castrillo, S.; Vogrig, A.; Villagran-Garcia, M.; Ciano-Petersen, N.L.; Massacesi, L.; Hervier, B.; et al. Neurological Outcomes in Immune Checkpoint Inhibitor-Related Neurotoxicity. Brain Commun. 2023, 5, 20. [Google Scholar] [CrossRef]
- Pepys, J.; Stoff, R.; Ramon-Gonen, R.; Ben-Betzalel, G.; Grynberg, S.; Frommer, R.S.; Schachter, J.; Asher, N.; Taliansky, A.; Nikitin, V.; et al. Incidence and Outcome of Neurologic Immune-Related Adverse Events Associated with Immune Checkpoint Inhibitors in Patients with Melanoma. Neurology 2023, 101, E2472–E2482. [Google Scholar] [CrossRef] [PubMed]
- Dolladille, C.; Ederhy, S.; Sassier, M.; Cautela, J.; Thuny, F.; Cohen, A.A.; Fedrizzi, S.; Chrétien, B.; Da-Silva, A.; Plane, A.F.; et al. Immune Checkpoint Inhibitor Rechallenge After Immune-Related Adverse Events in Patients with Cancer. JAMA Oncol. 2020, 6, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Ishikawa, N.; Konoeda, F.; Seki, N.; Fukushima, S.; Takahashi, K.; Uhara, H.; Hasegawa, Y.; Inomata, S.; Otani, Y.; et al. Nivolumab-Related Myasthenia Gravis with Myositis and Myocarditis in Japan. Neurology 2017, 89, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Garcia, C.R.; Jayswal, R.; Adams, V.; Anthony, L.B.; Villano, J.L. Multiple Sclerosis Outcomes after Cancer Immunotherapy. Clin. Transl. Oncol. 2019, 21, 1336–1342. [Google Scholar] [CrossRef] [PubMed]
- Aoun, R.; Gratch, D.; Kaminetzky, D.; Kister, I. Immune Checkpoint Inhibitors in Patients with Pre-Existing Neurologic Autoimmune Disorders. Curr. Neurol. Neurosci. Rep. 2023, 23, 735–750. [Google Scholar] [CrossRef] [PubMed]
- Vogrig, A.; Fouret, M.; Joubert, B.; Picard, G.; Rogemond, V.; Pinto, A.L.; Muñiz-Castrillo, S.; Roger, M.; Raimbourg, J.; Dayen, C.; et al. Increased Frequency of Anti-Ma2 Encephalitis Associated with Immune Checkpoint Inhibitors. Neurol. Neuroimmunol. Neuroinflammation 2019, 6, e604. [Google Scholar] [CrossRef] [PubMed]
- Farina, A.; Villagrán-García, M.; Ciano-Petersen, N.L.; Vogrig, A.; Muñiz-Castrillo, S.; Taillandier, L.; Michaud, M.; Lefilliatre, M.; Wang, A.; Lepine, Z.; et al. Anti-Hu Antibodies in Patients with Neurologic Side Effects of Immune Checkpoint Inhibitors. Neurol. Neuroimmunol. Neuroinflammation 2023, 10, e200058. [Google Scholar] [CrossRef]
- Graus, F.; Dalmau, J. Paraneoplastic Neurological Syndromes in the Era of Immune-Checkpoint Inhibitors. Nat. Rev. Clin. Oncol. 2019, 16, 535–548. [Google Scholar] [CrossRef]

{kind=link}
| Severity Grade Based on CTCAE v5.0 (Guidon et al.’s Severity Equivalent) | Impact on Activities of Daily Life (ADL) |
|---|---|
| Grade 1 (Mild) | Symptoms do not interfere with ADLs or are subclinical |
| Grade 2 (Moderate) | Symptoms interfere with ADL and may require outpatient treatment |
| Grade 3 (Severe) | Symptoms interfere with ADLs and may require hospitalization for treatment |
| Grade 4 (Fulminant) | Life-threatening symptoms requiring emergent intervention (intubation, feeding tube) |
| Grade 5 (Death) | Death attributable to symptoms |
| Condition | Severity | Management |
|---|---|---|
| irMyositis/Myopathy | Grade 1: Pauci-symptomatic increase in CK levels and/or asymptomatic weakness on neurological exam or mild myalgia without weakness. | Continue ICI therapy with close follow-up with regular swallowing and respiratory assessment. |
| Grade 2: Mild-to-moderate weakness, including ocular weakness. | Discontinue temporary ICI and start oral prednisone (0.5–1 mg/kg/day) for at least 4 weeks, followed by a gradual tapering over 4–6 weeks. Permanently discontinue ICI in case of deterioration of symptoms despite steroids. | |
| Grade 3: Moderate-to-severe weakness in limbs or neck, altered walking or new need for an assistive device, bulbar symptoms (dysphagia, dysarthria, dysphonia), and/or dyspnea requiring monitoring. | Permanently discontinue ICI. Hospitalization is recommended, with IV methylprednisolone (1–2 mg/kg/day), followed by a gradual tapering regimen over 4–8 weeks, depending on symptom severity. Pulse methylprednisolone therapy (1 g/day for 5 days) may also be considered. In case of rapid progression with bulbar involvement or in case of persistent symptoms (after 7 days of steroids), start IVIG or plasmapheresis. After stabilization, continue with steroids (methylprednisolone at 1–2 mg/kg/day, followed by gradual tapering). In case of symptom persistence or recurrence despite steroids, consider methotrexate, azathioprine, mycophenolate mofetil, rituximab, anti-IL-6, or anti-TNF-α therapy. Formal contra-indication for ICI re-challenge. | |
| Grade 4: Respiratory weakness requiring intubation or non-invasive ventilation and/or dysphagia requiring feeding tube. | ||
| irMyasthenia Gravis (MG) | Grade 1: Not applicable, given the potential for rapid deterioration and the importance of early management. | Discontinue temporary ICI and
|
| Grade 2: Mild-to-moderate weakness, including ocular weakness. | ||
| Grade 3: Moderate-to-severe weakness in limbs or neck, altered walking or new need for an assistive device, bulbar symptoms (dysphagia, dysarthria, dysphonia), and/or dyspnea requiring monitoring. | Definitively discontinue ICI. Start IV methylprednisone plus pyridostigmine (as below), and start IVIG or plasmapheresis. Pulse methylprednisone therapy (1 g/day for 5 days) may also be considered. For patients who do not respond, second-line therapies, such as rituximab, tacrolimus, or infliximab, should be considered. Formal contra-indication for ICI re-challenge. | |
| Grade 4: Respiratory weakness requiring intubation or non-invasive ventilation and/or dysphagia requiring feeding tube. | ||
| irGuillain–Barré Syndrome (GBS) | Grade 1: Not applicable, given the potential for rapid deterioration and the importance of early management. | Discontinue ICI. Start IVIG or plasma exchange, and start IV methylprednisolone (2–4 mg/kg/day), with a gradual tapering regimen over 4–8 weeks. Globally, ICI re-challenge in irGBS should be avoided; however, a re-challenge may be considered in case of complete irAEs recovery after steroid arrest, progressive disease and limited therapeutic alternative. |
| Grade 2: Any neuropathy-related weakness. | ||
| Grade 3: Walking impairment requiring assistive devices, bulbar symptoms (dysphagia, dysarthria, dysphonia), and respiratory dysfunction needing monitoring. | Definitively discontinue ICI. Start IVIG or plasma exchange, and start IV pulse methylprednisolone therapy (1 g/day for 5 days), with a gradual tapering regimen over 4–8 weeks. Formal contra-indication for ICI re-challenge. | |
| Grade 4: Respiratory weakness requiring intubation or non-invasive ventilation and/or dysphagia requiring feeding tube. | ||
| irMeningitis | Grade 1: Headaches manageable with over-the-counter analgesics. | Discontinue ICI and resume ICI in case of Grade 1 confirmation and symptom recovery. |
| Grade 2: Headaches requiring prescription analgesics. | Start oral prednisone (0.5–1 mg/kg/day) for a minimum of 2–4 weeks, followed by a gradual tapering regimen over 4–8 weeks. ICI re-challenge may be considered only in case of complete irAEs recovery after steroid arrest. | |
| Grade 3: Headaches necessitating intravenous analgesics or any corticosteroids; severe papilledema with associated visual deficit. | Definitively discontinue ICI. Start IV methylprednisolone at 1–2 mg/kg/day for a minimum of 2–4 weeks, with a gradual tapering regimen over 4–8 weeks. Methylprednisolone pulse therapy, IVIG, plasmapheresis, rituximab, and tacrolimus are potential treatments in refractory cases. Formal contra-indication for ICI re-challenge. | |
| Grade 4: Extra-ventricular drain for increased intracranial pressure. | ||
| irEncephalitis | Grade 1: Not applicable, given the potential for rapid deterioration and the importance of early management. | Definitively discontinue ICI. Start IV methylprednisolone (1–2 mg/kg/day) with a gradual tapering regimen over 4–8 weeks. IVIG or plasmapheresis can be considered. Globally, ICI re-challenge in irEncephalitis should be avoided; however, a re-challenge may be considered in case of complete irAEs recovery after steroid arrest, progressive disease and limited therapeutic alternative. |
| Grade 2: Subjective or mild cognitive deficits not significantly restricting daily activities. | ||
| Grade 3: Cognitive deficits limiting ADLs and/or seizures. | Definitively discontinue ICI. Consider ICU admission and start IV pulse methylprednisolone therapy (1 g/day for 5 days), followed by a gradual tapering regimen over 4–8 weeks and the addition of IVIG or plasmapheresis. In refractory situations, rituximab may also be used. Formal contra-indication for ICI re-challenge. | |
| Grade 4: Status epilepticus. | ||
| irDDs (immune-related demyelinating diseases) | Grade 1: Asymptomatic or experiencing mild symptoms. | Discontinue temporary ICI in asymptomatic cases in order to exclude rapid deterioration. |
| Grade 2: Mild unilateral visual changes, diplopia, and limitations in instrumental ADL due to deficits. | Discontinue ICI. Start oral or IV prednisolone (1–2 mg/kg/day), followed by a gradual tapering regimen over 4–8 weeks. Globally, ICI re-challenge in irDDs should be avoided; however, a re-challenge may be considered in case of complete irAEs recovery after steroid arrest, progressive disease and limited therapeutic alternative. | |
| Grade 3: Severe unilateral or bilateral vision loss, acute urinary retention, limitations in basic ADL. | Definitively discontinue ICI and start IV methylprednisolone pulse therapy (1 g/day for 5 days), followed by a gradual tapering regimen over 4–8 weeks. Consider addition of IVIG and plasmapheresis, or rituximab in case of symptom persistence or worsening. | |
| Grade 4: Intubation required due to respiratory failure caused by cervical or brainstem lesions. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zammit, F.; Seront, E. Neurological Adverse Events Related to Immune Checkpoint Inhibitors: A Practical Review. Pharmaceuticals 2024, 17, 501. https://doi.org/10.3390/ph17040501
Zammit F, Seront E. Neurological Adverse Events Related to Immune Checkpoint Inhibitors: A Practical Review. Pharmaceuticals. 2024; 17(4):501. https://doi.org/10.3390/ph17040501
Chicago/Turabian StyleZammit, François, and Emmanuel Seront. 2024. "Neurological Adverse Events Related to Immune Checkpoint Inhibitors: A Practical Review" Pharmaceuticals 17, no. 4: 501. https://doi.org/10.3390/ph17040501
APA StyleZammit, F., & Seront, E. (2024). Neurological Adverse Events Related to Immune Checkpoint Inhibitors: A Practical Review. Pharmaceuticals, 17(4), 501. https://doi.org/10.3390/ph17040501