
Therapeutic Vaccines for Follicular Lymphoma: A Systematic Review

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Types of Studies
2.1.2. Types of Participants
2.1.3. Types of Interventions
- Autologous therapeutic vaccines:
- ◦
- Vaccination with inactivated autologous tumor cells and adjuvant;
- ◦
- In situ vaccination;
- ◦
- Autologous dendritic cell vaccines.
- Allogeneic therapeutic vaccines:
- ◦
- Tumor-associated antigen-based vaccines;
- ◦
- Neoantigen-based vaccines;
- ◦
- Idiotype therapeutic vaccines.
2.1.4. Types of Outcome Measures
2.2. Information Sources
2.3. Search Strategy
2.4. Study Records
2.4.1. Data Management
2.4.2. Selection Process
2.4.3. Data Collection Process
2.5. Data Items
2.6. Outcomes and Prioritization
2.7. Risk of Bias in Individual Studies
2.8. Data Synthesis
2.9. Meta-Bias(es)
2.10. Confidence in Cumulative Evidence
3. Results
3.1. Summary of Findings
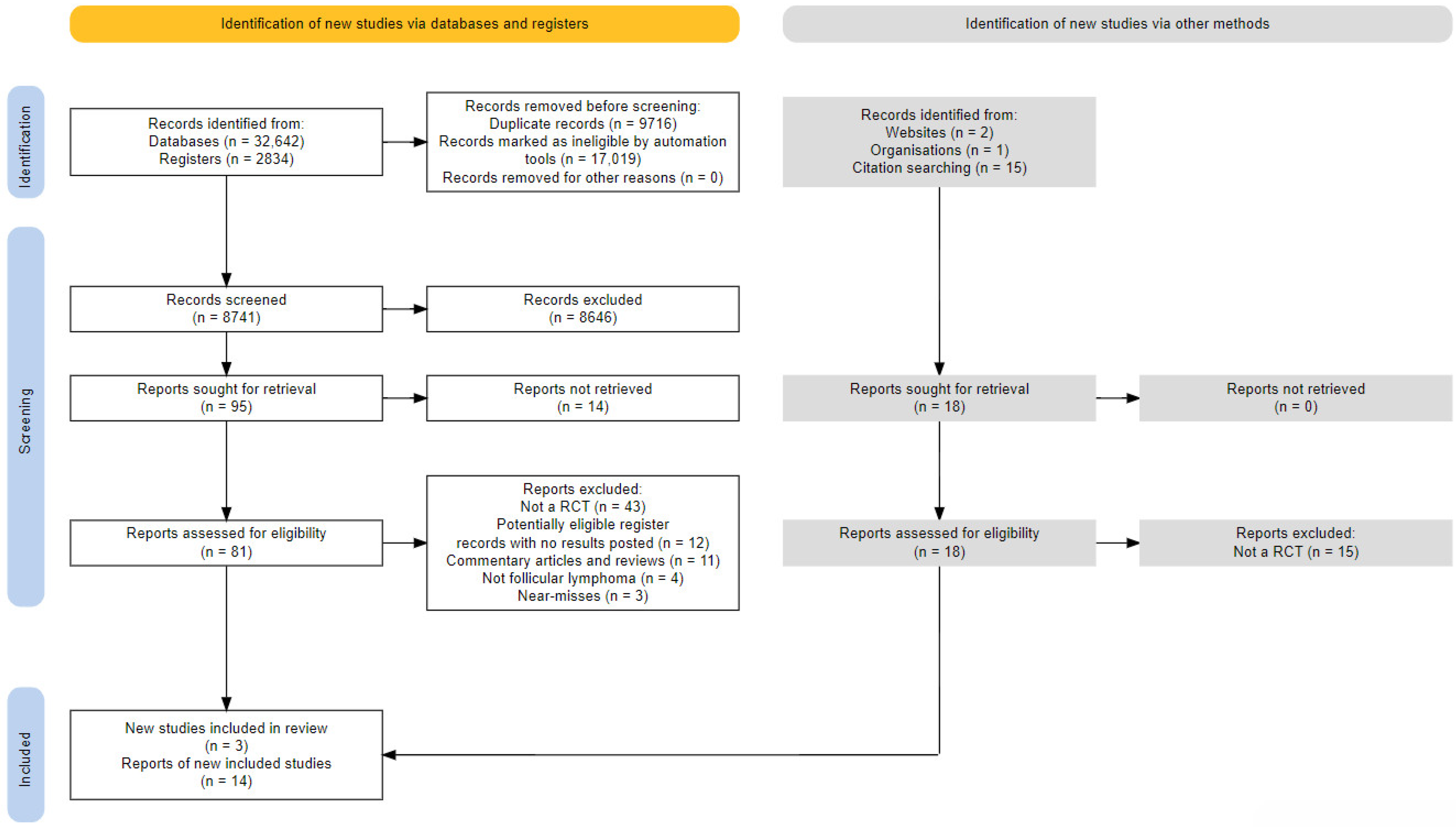
3.2. Study Selection
3.3. Patient Characteristics
3.4. Study Designs
3.5. Outcomes
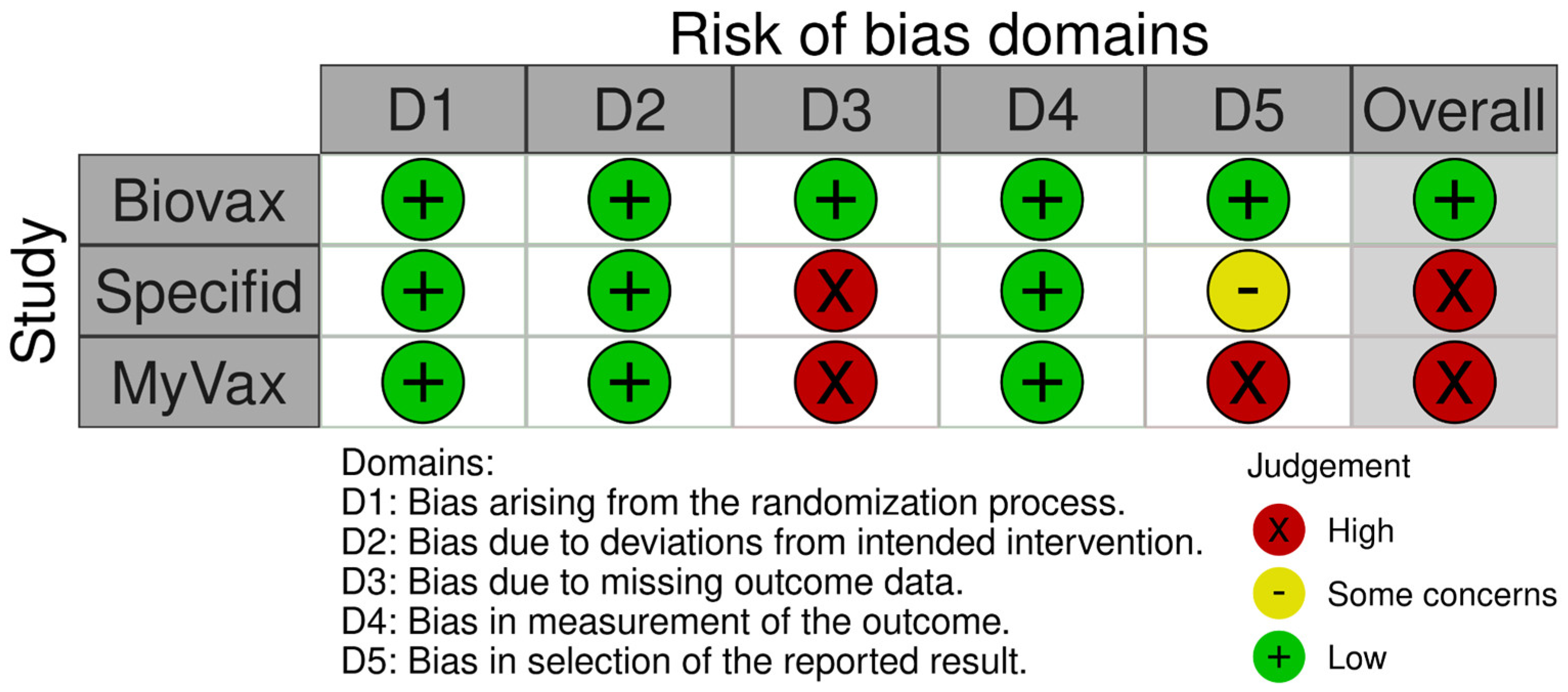
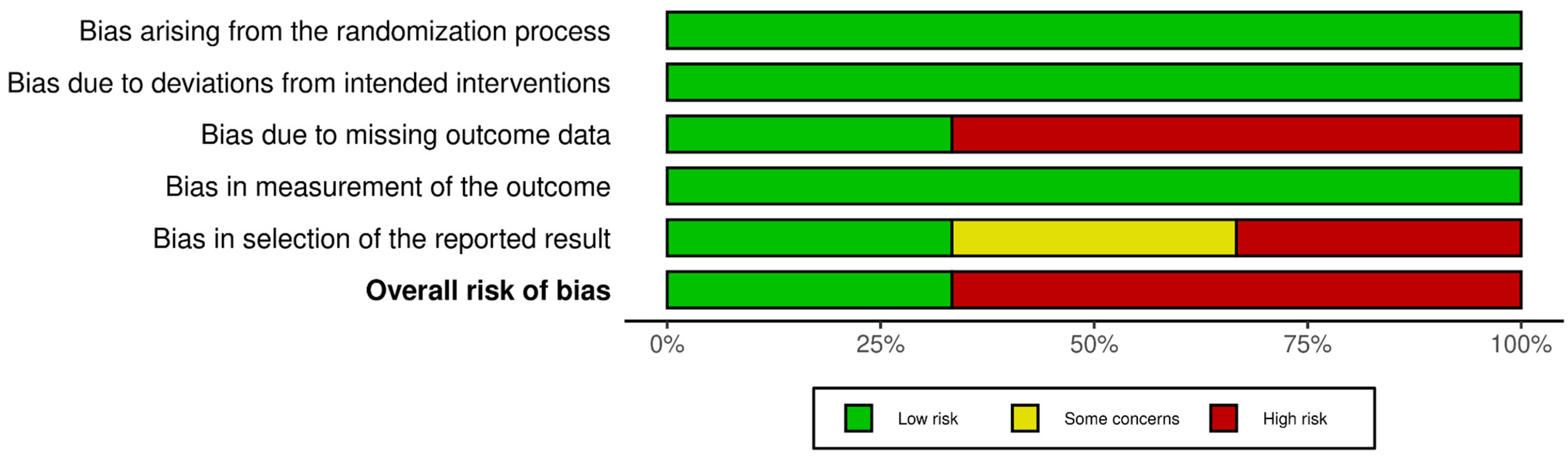
3.6. Risk of Bias in Studies
3.6.1. Bias Due to Randomization
3.6.2. Bias Due to Deviation from the Intended Interventions
3.6.3. Bias Due to Missing Outcome Data
3.6.4. Bias Due to Outcome Measurement
3.6.5. Bias Due to Selection of the Reported Results
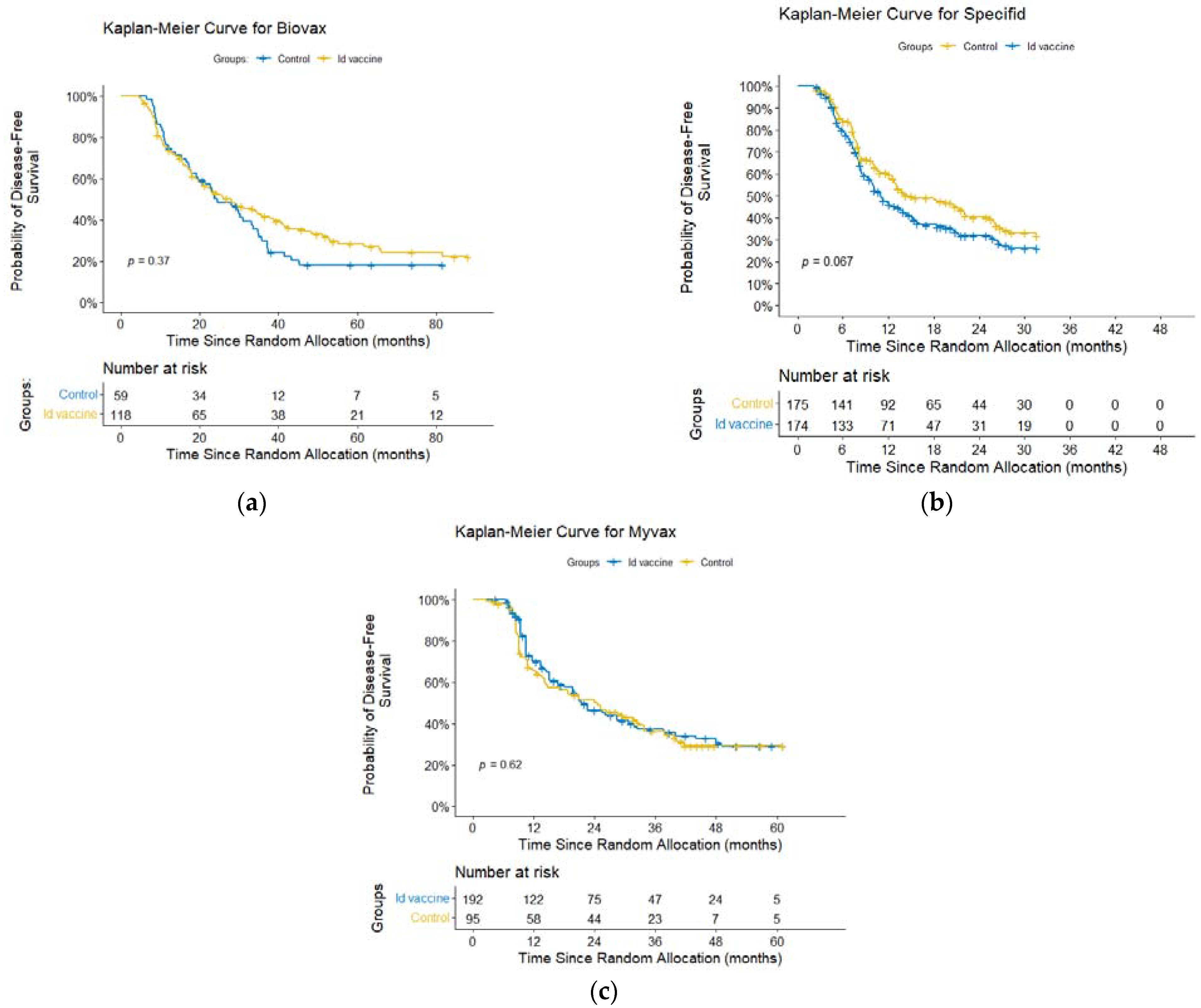
3.7. Results of Individual Studies
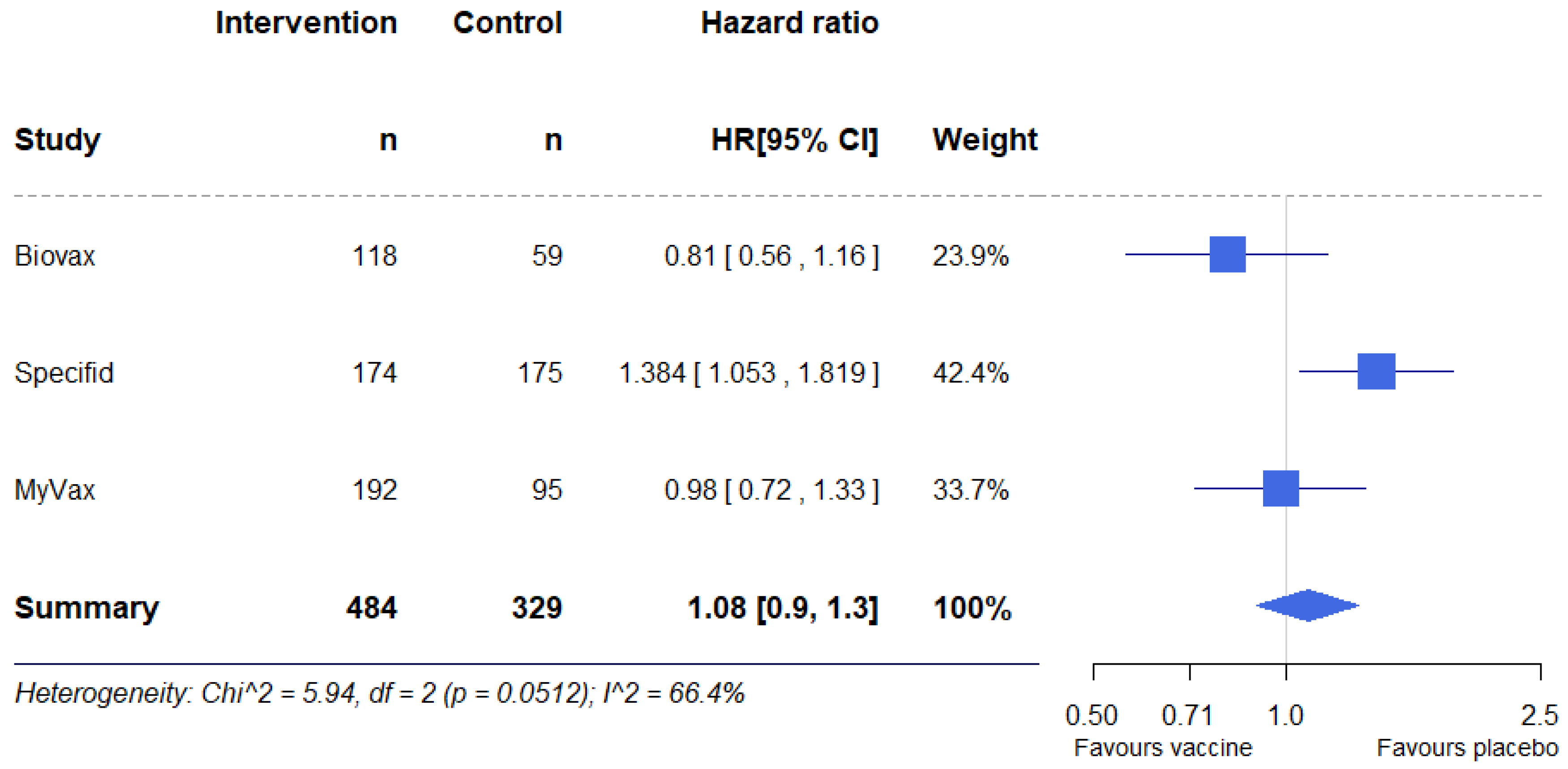
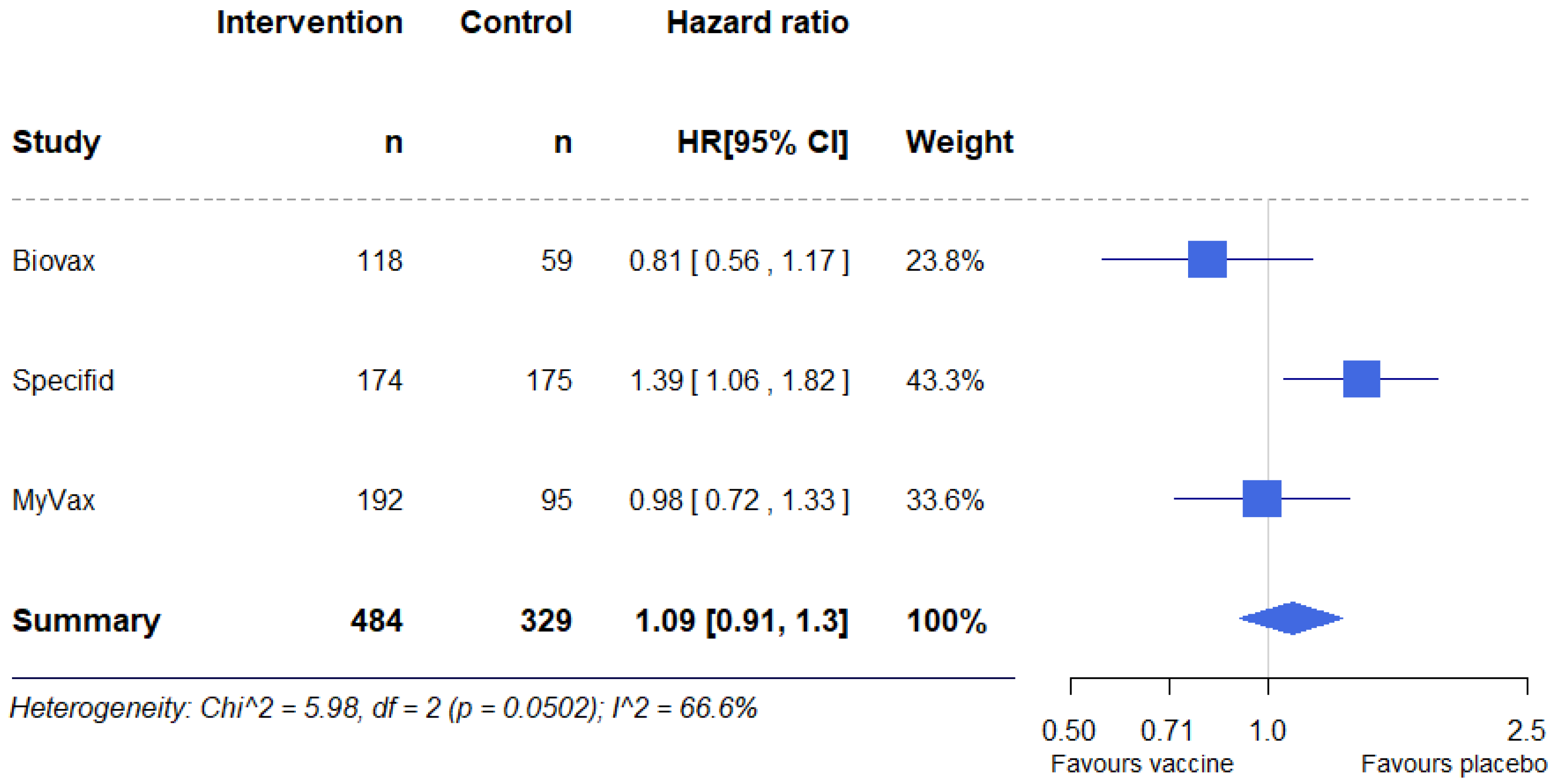
3.8. Results of Syntheses
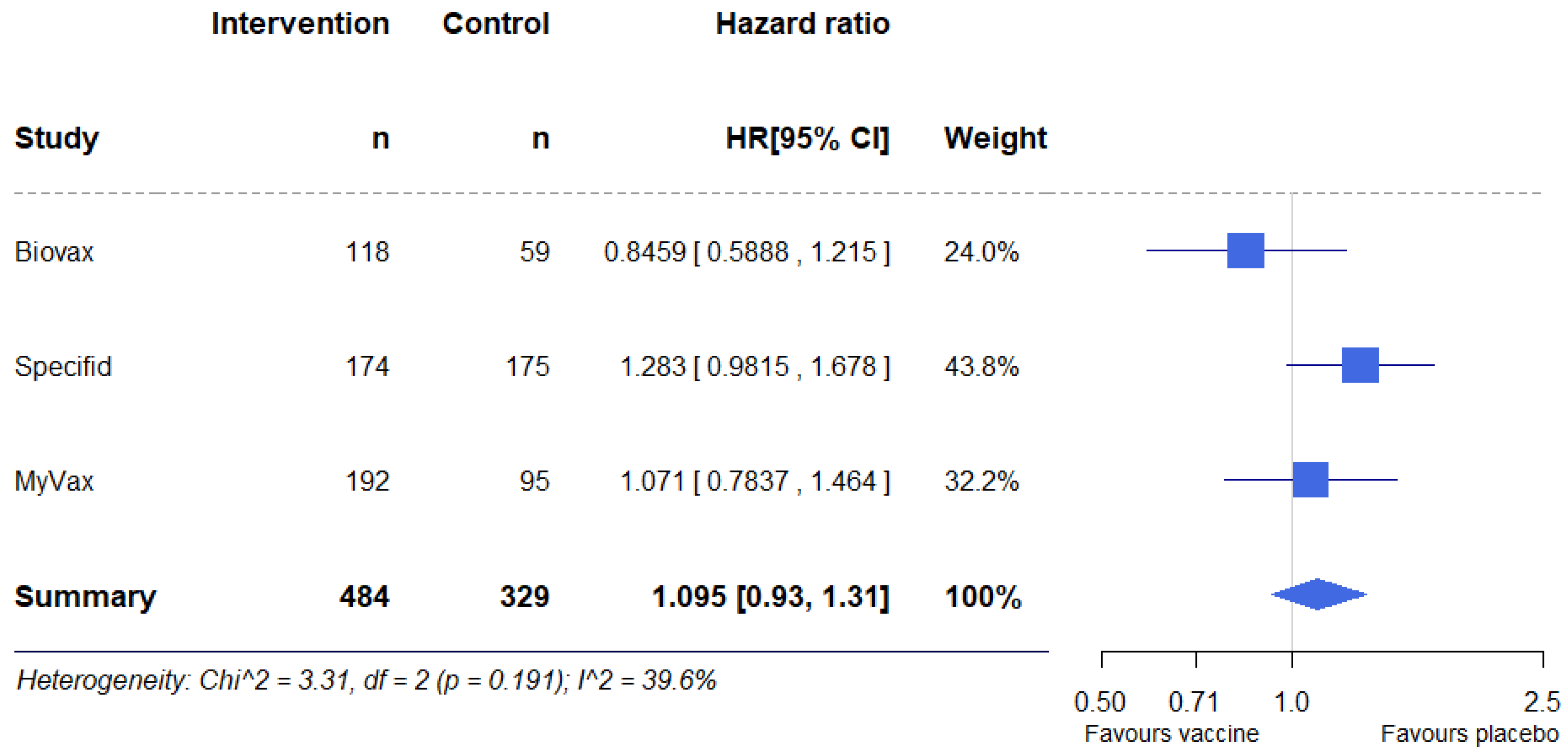
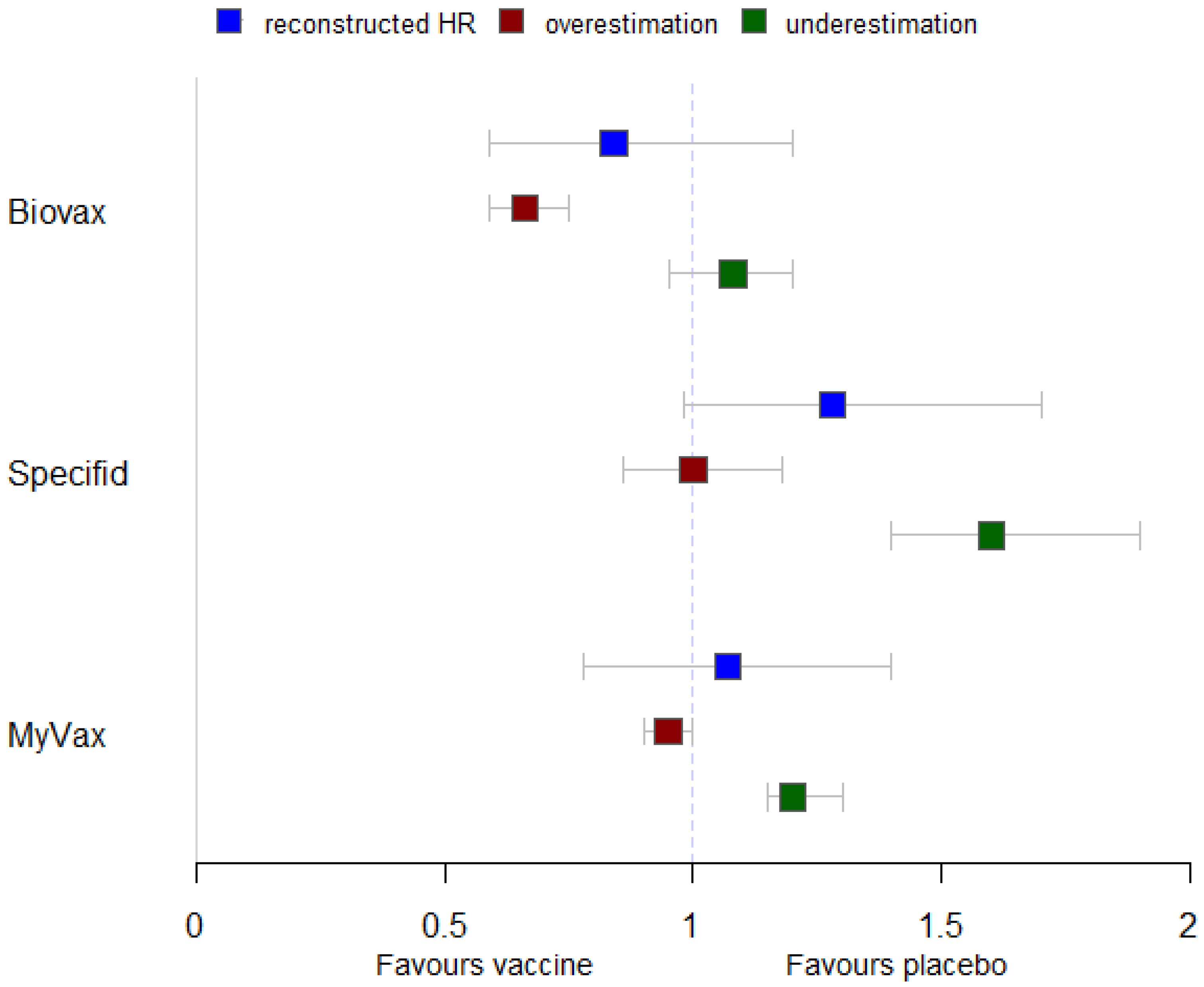
3.9. Additional Analyses
3.10. Safety
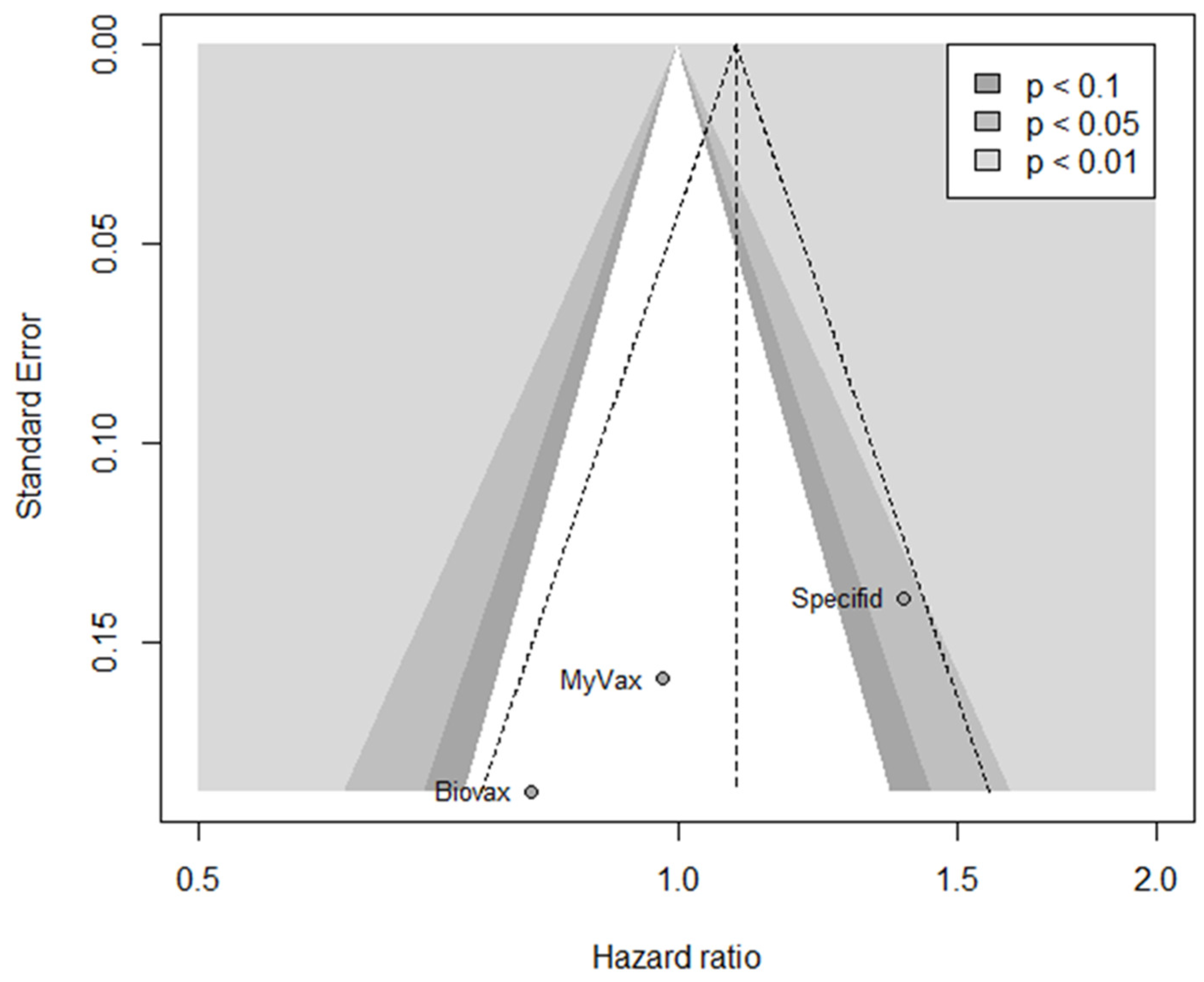
3.11. Reporting Biases
3.12. Certainty of Evidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoffman, R.; Benz, E.J.; Silberstein, L.E.; Heslop, H.E.; Weitz, J.I.; Salama, M.E.; Abutalib, S.A. (Eds.) Hematology: Basic Principles and Practice, 8th ed.; Elsevier: Philadelphia, PA, USA, 2023; ISBN 9780323733892. [Google Scholar]
- WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues; Organisation Mondiale de la Santé, Centre International de Recherche Sur le Cancer (Eds.) World Health Organization Classification of Tumours, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2008; ISBN 9789283224310. [Google Scholar]
- Morton, L.M.; Wang, S.S.; Devesa, S.S.; Hartge, P.; Weisenburger, D.D.; Linet, M.S. Lymphoma Incidence Patterns by WHO Subtype in the United States, 1992–2001. Blood 2006, 107, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Crouch, S.; Lax, S.; Li, J.; Painter, D.; Howell, D.; Patmore, R.; Jack, A.; Roman, E. Lymphoma Incidence, Survival and Prevalence 2004–2014: Sub-Type Analyses from the UK’s Haematological Malignancy Research Network. Br. J. Cancer 2015, 112, 1575–1584. [Google Scholar] [CrossRef] [PubMed]
- Junlén, H.R.; Peterson, S.; Kimby, E.; Lockmer, S.; Lindén, O.; Nilsson-Ehle, H.; Erlanson, M.; Hagberg, H.; Rådlund, A.; Hagberg, O.; et al. Follicular Lymphoma in Sweden: Nationwide Improved Survival in the Rituximab Era, Particularly in Elderly Women: A Swedish Lymphoma Registry Study. Leukemia 2015, 29, 668–676. [Google Scholar] [CrossRef]
- Sud, A.; Chattopadhyay, S.; Thomsen, H.; Sundquist, K.; Sundquist, J.; Houlston, R.S.; Hemminki, K. Analysis of 153 115 Patients with Hematological Malignancies Refines the Spectrum of Familial Risk. Blood 2019, 134, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Vitolo, U.; Ferreri, A.J.M.; Montoto, S. Follicular Lymphomas. Crit. Rev. Oncol. Hematol. 2008, 66, 248–261. [Google Scholar] [CrossRef]
- Green, M.R. Chromatin Modifying Gene Mutations in Follicular Lymphoma. Blood 2018, 131, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Luminari, S.; Bellei, M.; Biasoli, I.; Federico, M. Follicular Lymphoma: Treatment and Prognostic Factors. Rev. Bras. Hematol. E Hemoter. 2011, 34, 54–59. [Google Scholar] [CrossRef]
- Dreyling, M.; Ghielmini, M.; Rule, S.; Salles, G.; Ladetto, M.; Tonino, S.H.; Herfarth, K.; Seymour, J.F.; Jerkeman, M. Newly Diagnosed and Relapsed Follicular Lymphoma: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up. Ann. Oncol. 2021, 32, 298–308. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. J. Clin. Oncol. 2014, 32, 3059–3067. [Google Scholar] [CrossRef]
- Brice, P.; Bastion, Y.; Lepage, E.; Brousse, N.; Haïoun, C.; Moreau, P.; Straetmans, N.; Tilly, H.; Tabah, I.; Solal-Céligny, P. Comparison in Low-Tumor-Burden Follicular Lymphomas Between an Initial No-Treatment Policy, Prednimustine, or Interferon Alfa: A Randomized Study from the Groupe d’Etude Des Lymphomes Folliculaires. Groupe d’Etude Des Lymphomes de l’Adulte. J. Clin. Oncol. 1997, 15, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Ardeshna, K.; Smith, P.; Norton, A.; Hancock, B.; Hoskin, P.; MacLennan, K.; Marcus, R.; Jelliffe, A.; Hudson, G.V.; Linch, D. Long-Term Effect of a Watch and Wait Policy Versus Immediate Systemic Treatment for Asymptomatic Advanced-Stage Non-Hodgkin Lymphoma: A Randomised Controlled Trial. Lancet 2003, 362, 516–522. [Google Scholar] [CrossRef]
- Schulz, H.; Bohlius, J.; Skoetz, N.; Trelle, S.; Kober, T.; Reiser, M.; Dreyling, M.; Herold, M.; Schwarzer, G.; Hallek, M.; et al. Chemotherapy Plus Rituximab Versus Chemotherapy Alone for B-Cell Non-Hodgkin’s Lymphoma. Cochrane Database Syst. Rev. 2007, 2007, CD003805. [Google Scholar] [CrossRef]
- Morschhauser, F.; Fowler, N.H.; Feugier, P.; Bouabdallah, R.; Tilly, H.; Palomba, M.L.; Fruchart, C.; Libby, E.N.; Casasnovas, R.-O.; Flinn, I.W.; et al. Rituximab Plus Lenalidomide in Advanced Untreated Follicular Lymphoma. N. Engl. J. Med. 2018, 379, 934–947. [Google Scholar] [CrossRef]
- Budde, L.E.; Sehn, L.H.; Matasar, M.; Schuster, S.J.; Assouline, S.; Giri, P.; Kuruvilla, J.; Canales, M.; Dietrich, S.; Fay, K.; et al. Safety and Efficacy of Mosunetuzumab, a Bispecific Antibody, in Patients with Relapsed or Refractory Follicular Lymphoma: A Single-Arm, Multicentre, Phase 2 Study. Lancet Oncol. 2022, 23, 1055–1065. [Google Scholar] [CrossRef]
- Denlinger, N.; Bond, D.; Jaglowski, S. CAR T-Cell Therapy for B-Cell Lymphoma. Curr. Probl. Cancer 2022, 46, 100826. [Google Scholar] [CrossRef] [PubMed]
- Mohty, R.; Kharfan-Dabaja, M.A. CAR T-Cell Therapy for Follicular Lymphoma and Mantle Cell Lymphoma. Ther. Adv. Hematol. 2022, 13, 204062072211421. [Google Scholar] [CrossRef] [PubMed]
- Mohty, R.; Kharfan-Dabaja, M.A.; Chavez, J.C. Axicabtagene Ciloleucel in the Management of Follicular Lymphoma: Current Perspectives on Clinical Utility, Patient Selection and Reported Outcomes. Cancer Manag. Res. 2023, 15, 367–375. [Google Scholar] [CrossRef]
- Ghione, P.; Palomba, M.L.; Patel, A.R.; Bobillo, S.; Deighton, K.; Jacobson, C.A.; Nahas, M.; Hatswell, A.J.; Jung, A.S.; Kanters, S.; et al. Comparative Effectiveness of ZUMA-5 (Axi-Cel) Vs SCHOLAR-5 External Control in Relapsed/Refractory Follicular Lymphoma. Blood 2022, 140, 851–860. [Google Scholar] [CrossRef]
- Liu, J.; Fu, M.; Wang, M.; Wan, D.; Wei, Y.; Wei, X. Cancer Vaccines as Promising Immuno-Therapeutics: Platforms and Current Progress. J. Hematol. Oncol. 2022, 15, 28. [Google Scholar] [CrossRef]
- Hollingsworth, R.E.; Jansen, K. Turning the Corner on Therapeutic Cancer Vaccines. Npj Vaccines 2019, 4, 7. [Google Scholar] [CrossRef] [PubMed]
- Sobhani, N.; Scaggiante, B.; Morris, R.; Chai, D.; Catalano, M.; Tardiel-Cyril, D.R.; Neeli, P.; Roviello, G.; Mondani, G.; Li, Y. Therapeutic Cancer Vaccines: From Biological Mechanisms and Engineering to Ongoing Clinical Trials. Cancer Treat. Rev. 2022, 109, 102429. [Google Scholar] [CrossRef]
- Le, I.; Dhandayuthapani, S.; Chacon, J.; Eiring, A.M.; Gadad, S.S. Harnessing the Immune System with Cancer Vaccines: From Prevention to Therapeutics. Vaccines 2022, 10, 816. [Google Scholar] [CrossRef]
- Xu-Monette, Z.Y.; Young, K.H. Therapeutic Vaccines for Aggressive B-Cell Lymphoma. Leuk. Lymphoma 2020, 61, 3038–3051. [Google Scholar] [CrossRef] [PubMed]
- Kantoff, P.W.; Higano, C.S.; Shore, N.D.; Berger, E.R.; Small, E.J.; Penson, D.F.; Redfern, C.H.; Ferrari, A.C.; Dreicer, R.; Sims, R.B.; et al. Sipuleucel-T Immunotherapy for Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2010, 363, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Andtbacka, R.H.I.; Kaufman, H.L.; Collichio, F.; Amatruda, T.; Senzer, N.; Chesney, J.; Delman, K.A.; Spitler, L.E.; Puzanov, I.; Agarwala, S.S.; et al. Talimogene Laherparepvec Improves Durable Response Rate in Patients with Advanced Melanoma. J. Clin. Oncol. 2015, 33, 2780–2788. [Google Scholar] [CrossRef] [PubMed]
- Morse, M.A.; Gwin, W.R.; Mitchell, D.A. Vaccine Therapies for Cancer: Then and Now. Target. Oncol. 2021, 16, 121–152. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.4 (Updated August 2023). Available online: www.training.cochrane.org/handbook (accessed on 15 February 2024).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B.; PRISMA-S Group; Blunt, H.; Brigham, T.; et al. PRISMA-S: An Extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef] [PubMed]
- Hunter, K.E.; Webster, A.C.; Page, M.J.; Willson, M.; McDonald, S.; Berber, S.; Skeers, P.; Tan-Koay, A.G.; Parkhill, A.; Seidler, A.L. Searching Clinical Trials Registers: Guide for Systematic Reviewers. BMJ 2022, 377, e068791. [Google Scholar] [CrossRef] [PubMed]
- Freedman, A.; Neelapu, S.S.; Nichols, C.; Robertson, M.J.; Djulbegovic, B.; Winter, J.N.; Bender, J.F.; Gold, D.P.; Ghalie, R.G.; Stewart, M.E.; et al. Placebo-Controlled Phase III Trial of Patient-Specific Immunotherapy with Mitumprotimut-T and Granulocyte-Macrophage Colony-Stimulating Factor After Rituximab in Patients with Follicular Lymphoma. J. Clin. Oncol. 2009, 27, 3036–3043. [Google Scholar] [CrossRef]
- Schuster, S.J.; Neelapu, S.S.; Gause, B.L.; Janik, J.E.; Muggia, F.M.; Gockerman, J.P.; Winter, J.N.; Flowers, C.R.; Nikcevich, D.A.; Sotomayor, E.M.; et al. Vaccination with Patient-Specific Tumor-Derived Antigen in First Remission Improves Disease-Free Survival in Follicular Lymphoma. J. Clin. Oncol. 2011, 29, 2787–2794. [Google Scholar] [CrossRef] [PubMed]
- Levy, R.; Ganjoo, K.N.; Leonard, J.P.; Vose, J.M.; Flinn, I.W.; Ambinder, R.F.; Connors, J.M.; Berinstein, N.L.; Belch, A.R.; Bartlett, N.L.; et al. Active Idiotypic Vaccination Versus Control Immunotherapy for Follicular Lymphoma. J. Clin. Oncol. 2014, 32, 1797–1803. [Google Scholar] [CrossRef] [PubMed]
- Vidal, L.; Gafter-Gvili, A.; Leibovici, L.; Shpilberg, O. Rituximab as Maintenance Therapy for Patients with Follicular Lymphoma. Cochrane Database Syst. Rev. 2009, 2009, CD00655. [Google Scholar] [CrossRef] [PubMed]
- Itchaki, G.; Gafter-Gvili, A.; Lahav, M.; Vidal, L.; Raanani, P.; Shpilberg, O.; Paul, M. Anthracycline-Containing Regimens for Treatment of Follicular Lymphoma in Adults. Cochrane Database Syst. Rev. 2013, 2013, CD008909. [Google Scholar] [CrossRef]
- Baldo, P.; Rupolo, M.; Compagnoni, A.; Lazzarini, R.; Bearz, A.; Cannizzaro, R.; Spazzapan, S.; Truccolo, I.; Moja, L. Interferon-Alpha for Maintenance of Follicular Lymphoma. Cochrane Database Syst. Rev. 2010, 2010, CD004629. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Jofré, M.; Uranga, R.; Torres Pombert, A.; Arango Prado, M.D.C.; Caballero Aguirrechu, I.; Pacheco, C.; Ortiz Reyes, R.M.; Chuecas, F.; Mas Bermejo, P.I. Therapeutic Vaccines for Advanced Non-Small Cell Lung Cancer. Cochrane Database Syst. Rev. 2019, 2019, CD013377. [Google Scholar] [CrossRef]
- Suponin, A.; Zhelnov, P.; Potanin, A.; Chekalov, A.; Lomazov, A.; Vladimirova, K.; Lepik, K.; Muslimov, A. Therapeutic Vaccines for Follicular Lymphoma: A Systematic Review. 2022. Available online: https://osf.io/kbzfw/ (accessed on 15 February 2024).
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Clark, J.; Glasziou, P.; Del Mar, C.; Bannach-Brown, A.; Stehlik, P.; Scott, A.M. A Full Systematic Review Was Completed in 2 Weeks Using Automation Tools: A Case Study. J. Clin. Epidemiol. 2020, 121, 81–90. [Google Scholar] [CrossRef]
- Rathbone, J.; Carter, M.; Hoffmann, T.; Glasziou, P. Better Duplicate Detection for Systematic Reviewers: Evaluation of Systematic Review Assistant-Deduplication Module. Syst. Rev. 2015, 4, 6. [Google Scholar] [CrossRef] [PubMed]
- Systematic Review Accelerator: Deduplicator. Available online: https://sr-accelerator.com/#/deduplicator (accessed on 10 October 2023).
- Github Taren Sanders’ RobotSearch. Available online: https://github.com/tarensanders/robotsearch (accessed on 10 September 2023).
- Marshall, I.J.; Noel-Storr, A.; Kuiper, J.; Thomas, J.; Wallace, B.C. Machine Learning for Identifying Randomized Controlled Trials: An Evaluation and Practitioner’s Guide. Res. Synth. Methods 2018, 9, 602–614. [Google Scholar] [CrossRef] [PubMed]
- RANDOM.ORG—Integer Set Generator. Available online: https://www.random.org/integer-sets/?mode=advanced (accessed on 19 May 2023).
- Rotondi, M.A. kappaSize: Sample Size Estimation Functions for Studies of Interobserver Agreement 2018. Available online: https://CRAN.R-project.org/package=kappaSize (accessed on 2 May 2023).
- Randolph’s Kappa Calculator. Available online: http://justus.randolph.name/kappa (accessed on 20 May 2023).
- Github Rayyan_tools. Available online: https://github.com/Andreyhok/rayyan_tools (accessed on 25 September 2023).
- DeepL Translate. Available online: https://www.deepl.com/translator/files (accessed on 7 August 2023).
- Follicular-Lymphoma-Vaccines Sysrev. Available online: https://sysrev.com/u/11470/p/123185 (accessed on 15 October 2023).
- Masson, D.; Malacria, S.; Vogel, D.; Lank, E.; Casiez, G. ChartDetective: Easy and Accurate Interactive Data Extraction from Complex Vector Charts. In Proceedings of the 2023 CHI Conference on Human Factors in Computing Systems, Hamburg, Germany, 23–28 April 2023; ACM: Hamburg, Germany, 2023; pp. 1–17. [Google Scholar]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. Revised Response Criteria for Malignant Lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, L.A. Robvis: An R Package and Web Application for Visualising Risk-of-Bias Assessments 2019. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Therneau, T. A Package for Survival Analysis in R. 2023. Available online: https://CRAN.R-project.org/package=survival (accessed on 15 February 2024).
- Terry, M.T.; Patricia, M. Grambsch Modeling Survival Data: Extending the Cox Model; Springer: New York, NY, USA, 2000; ISBN 0-387-98784-3. [Google Scholar]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- Kassambara, A.; Kosinski, M.; Biecek, P.; Fabian, S. survminer: Survival Analysis and Visualization, version 0.4.9; 2021. Available online: https://rpkgs.datanovia.com/survminer/index.html (accessed on 15 February 2024).
- Gordon, M.; Lumley, T. forestplot: Advanced Forest Plot Using ’Grid’ Graphics, Version 3.1.3; 2023. Available online: https://gforge.se/packages/ (accessed on 15 February 2024).
- Page, M.J.; Sterne, J.A.C.; Boutron, I.; Hróbjartsson, A.; Kirkham, J.J.; Li, T.; Lundh, A.; Mayo-Wilson, E.; McKenzie, J.E.; Stewart, L.A.; et al. ROB-ME: A Tool for Assessing Risk of Bias Due to Missing Evidence in Systematic Reviews with Meta-Analysis. BMJ 2023, 383, e076754. [Google Scholar] [CrossRef]
- Guideline Development Tool. Available online: https://gdt.gradepro.org/ (accessed on 15 February 2024).
- Stein, B.; Struss, Y.; Fritzsche, K. a) 3.2.2 Psycho-Onkologie b) 3.2.3 Tumorspezifische Immuntherapie. Oncol. Res. Treat. 2000, 23, 41–43. [Google Scholar] [CrossRef]
- Cabrera, J.R.; Barrios, Y.; Yáñez, R.; Fernández, M.N.; De Espada, F.D. Vacunación Idiotípica En Linfomas B de Bajo Grado: Una Nueva Terapia Antitumoral. Rev. Oncol. 2001, 3, 201–206. [Google Scholar] [CrossRef]
- Neelapu, S.S.; Gause, B.L.; Nikcevich, D.A.; Schuster, S.J.; Winter, J.; Gockerman, J.P.; Loughran, T.; Takeshita, K.; Inghirami, G.; McGaughey, D.; et al. Phase III Randomized Trial of Patient-Specific Vaccination for Previously Untreated Patients with Follicular Lymphoma in First Complete Remission: Protocol Summary and Interim Report. Clin. Lymphoma 2005, 6, 61–64. [Google Scholar] [CrossRef]
- Stergiou, A.M.; Neelapu, S.S.; Casciano, R.; Jaffee, M.A.; Kwak, L.W. BiovaxId Vaccine Therapy of Follicular Lymphoma in First Remission: Phase III Blinded Safety Update. Blood 2007, 110, 4500. [Google Scholar] [CrossRef]
- Schuster, S.J.; Neelapu, S.S.; Gause, B.L.; Muggia, F.M.; Gockerman, J.P.; Sotomayor, E.M.; Winter, J.N.; Flowers, C.R.; Stergiou, A.M.; Kwak, L.W. Idiotype Vaccine Therapy (BiovaxID) in Follicular Lymphoma in First Complete Remission: Phase III Clinical Trial Results. J. Clin. Oncol. 2009, 27, 2. [Google Scholar] [CrossRef]
- Schuster, S.J.; Santos, C.F.; Neelapu, S.S.; Berry, D.A.; Popa, M.A.; McCord, A.M.; Chong, E.A.; Kwak, L. Vaccination with IgM but Not IgG Idiotype Prolongs Remission Duration in Follicular Lymphoma Patients. Blood 2010, 116, 429. [Google Scholar] [CrossRef]
- Biovest International. Randomized Trial of Patient-Specific Vaccination with Conjugated Follicular Lymphoma-Derived Idiotype (FNHLId1) with Local GM-CSF in First Complete Remission. 2012. Available online: https://clinicaltrials.gov/study/NCT00091676 (accessed on 15 February 2024).
- Bendandi, M.; Gocke, C.D.; Kobrin, C.B.; Benko, F.A.; Sternas, L.A.; Pennington, R.; Watson, T.M.; Reynolds, C.W.; Gause, B.L.; Duffey, P.L.; et al. Complete Molecular Remissions Induced by Patient-Specific Vaccination Plus Granulocyte-Monocyte Colony-Stimulating Factor Against Lymphoma. Nat. Med. 1999, 5, 1171–1177. [Google Scholar] [CrossRef] [PubMed]
- Freedman, A.S.; Hamlin, P.A.; Neelapu, S.; Nichols, C.; Robertson, M.; Bergier, G.; Winter, J.N.; Polikoff, J.; Lin, T.; Pohlman, B.; et al. Phase III Trial of Active Immunotherapy (FavId®, Id/KLH) Following Rituximab Induction Therapy: Clinical Responses in Patients (Pts) with Follicular Non-Hodgkin’s Lymphoma (FNHL). Blood 2006, 108, 2756. [Google Scholar] [CrossRef]
- Freedman, A.S.; Neelapu, S.; Nichols, C.R.; Robertson, M.; Djulbegovic, B.; Winter, J.N.; Gold, D.; Bender, J.; Stewart, M.; Ghalie, R.G.; et al. A Placebo-Controlled Phase III Trial of Patient-Specific Immunotherapy with Mitumprotimut-T (Id-KLH) and GM-CSF Following Rituximab in Patients with Cd20+ Follicular Lymphoma. Blood 2008, 112, 236. [Google Scholar] [CrossRef]
- Santos, C.; Stern, L.; Katz, L.; Watson, T.; Barry, G. BiovaxID™ Vaccine Therapy of Follicular Lymphoma in First Remission: Long-Term Follow-Up of a Phase II Trial and Status of a Controlled, Randomized Phase III Trial. Blood 2005, 106, 2441. [Google Scholar] [CrossRef]
- Timmerman, J.M.; Vose, J.M.; Czerwinski, D.K.; Weng, W.-K.; Ingolia, D.; Mayo, M.; Denney, D.W.; Levy, R. Tumor-Specific Recombinant Idiotype Immunisation After Chemotherapy as Initial Treatment for Follicular Non-Hodgkin Lymphoma. Leuk. Lymphoma 2009, 50, 37–46. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Koc, O.N.; Redfern, C.; Wiernik, P.H.; Rosenfelt, F.; Winter, J.N.; Guthrie, T.H.; Kaplan, L.; Holman, P.; Densmore, J.; Hainsworth, J.; et al. Id/KLH Vaccine (FavId™) Following Treatment with Rituximab: An Analysis of Response Rate Improvement (RRI) and Time-to-Progression (TTP) in Follicular Lymphoma (FL). Blood 2004, 104, 587. [Google Scholar] [CrossRef]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical Methods for Incorporating Summary Time-to-Event Data into Meta-Analysis. Trials 2007, 8, 16. [Google Scholar] [CrossRef]
- Guyot, P.; Ades, A.; Ouwens, M.J.; Welton, N.J. Enhanced Secondary Analysis of Survival Data: Reconstructing the Data from Published Kaplan-Meier Survival Curves. BMC Med. Res. Methodol. 2012, 12, 9. [Google Scholar] [CrossRef]
- Tusé, D.; Ku, N.; Bendandi, M.; Becerra, C.; Collins, R.; Langford, N.; Sancho, S.I.; López-Díaz De Cerio, A.; Pastor, F.; Kandzia, R.; et al. Clinical Safety and Immunogenicity of Tumor-Targeted, Plant-Made Id-KLH Conjugate Vaccines for Follicular Lymphoma. BioMed Res. Int. 2015, 2015, 648143. [Google Scholar] [CrossRef]
- Meleshko, A.N.; Petrovskaya, N.A.; Savelyeva, N.; Vashkevich, K.P.; Doronina, S.N.; Sachivko, N.V. Phase I Clinical Trial of Idiotypic DNA Vaccine Administered as a Complex with Polyethylenimine to Patients with B-Cell Lymphoma. Hum. Vaccines Immunother. 2017, 13, 1398–1403. [Google Scholar] [CrossRef] [PubMed]
- Meleshko, A.; Piatrouskaya, N.; Vashkevich, K.; Lutskovich, D.; Wang, C.; Dormeshkin, D.; Savelyeva, N.; Katsin, M. Safety and Immunogenicity of Combined DNA-Polyethylenimine and Oral Bacterial Idiotypic Vaccine for Patients with B-Cell Non-Hodgkin Lymphoma: A Pilot Study. Cancers 2022, 14, 3298. [Google Scholar] [CrossRef] [PubMed]
- Klausen, U.; Grønne Dahlager Jørgensen, N.; Grauslund, J.H.; Munir Ahmad, S.; Gang, A.O.; Martinenaite, E.; Weis-Banke, S.E.; Breinholt, M.F.; Novotny, G.W.; Kjeldsen, J.W.; et al. An Immunogenic First-in-Human Immune Modulatory Vaccine with PD-L1 and PD-L2 Peptides Is Feasible and Shows Early Signs of Efficacy in Follicular Lymphoma. OncoImmunology 2021, 10, 1975889. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Leet, D.E.; Allesøe, R.L.; Oliveira, G.; Li, S.; Luoma, A.M.; Liu, J.; Forman, J.; Huang, T.; Iorgulescu, J.B.; et al. Personal Neoantigen Vaccines Induce Persistent Memory T Cell Responses and Epitope Spreading in Patients with Melanoma. Nat. Med. 2021, 27, 515–525. [Google Scholar] [CrossRef]
- Khan, M.; Li, X.; Yan, M.; Li, Z.; Yang, H.; Liao, G. Efficacy and Safety of Actively Personalized Neoantigen Vaccination in the Management of Newly Diagnosed Glioblastoma: A Systematic Review. Int. J. Gen. Med. 2021, 14, 5209–5220. [Google Scholar] [CrossRef] [PubMed]
- Haddaway, N.R.; Page, M.J.; Pritchard, C.C.; McGuinness, L.A. Prisma2020: An R Package and Shiny App for Producing PRISMA 2020-compliant Flow Diagrams, with Interactivity for Optimised Digital Transparency and Open Synthesis. Campbell Syst. Rev. 2022, 18, e1230. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome N° of Participants (Studies) | Relative Effect (95% CI) | Anticipated Absolute Effects (95% CI) | Certainty | What Happens | ||
|---|---|---|---|---|---|---|
| With Placebo | With Vaccine | Difference | ||||
| Progression-free survival (PFS) assessed with: Hazard Ratio follow-up: median 42.8 months N° of participants: 813 (3 RCTs) | HR 1.09 (0.91 to 1.3) [Progression-free survival] | With baseline risk from the BiovaxID trial | ⨁⨁⨁◯ Moderate | Therapeutic antitumor vaccines likely result in little to no difference in progression-free survival, with a non-significant increase in hazards of disease progression with vaccines. | ||
| 78.0% | 80.8% (74.8 to 86) | 2.8% more (3.2 fewer to 8 more) | ||||
| With baseline risk from the Specifid trial | ||||||
| 57.0% | 60.1% (53.6 to 66.6) | 3.1% more (3.4 fewer to 9.6 more) | ||||
| With baseline risk from the MyVax trial | ||||||
| 63.0% | 66.2% (59.5 to 72.5) | 3.2% more (3.5 fewer to 9.5 more) | ||||
| All Patients | BiovaxID | Specifid | MyVax |
|---|---|---|---|
| Newly diagnosed, relapsed, or refractory disease? | All treatment-naïve | Treatment-naïve and relapsed refractory | All treatment-naïve |
| Number of patients randomized | 177 | 349 | 287 |
| Age | Mean, 49.5 SD, 10.4 | Median, 54 Range, 21–86 | Median, 50 Range, 23–80 |
| Female, % | 45.7 | 43.3 | 54.7 |
| Previous treatment | Previously untreated (except: prednisone for < 2 months, radiation alone) | No more than two systemic lymphoma therapies | Previously untreated |
| FLIPI (risk group, %) | Low or intermediate, 87.6 High intermediate or high, 12.0 Unknown, 0.4 | Low, 37.0 Intermediate, 39.3 High, 22.3 Unknown, 1.4 | Low, 10.0 Intermediate, 53.3 High, 36.0 Unknown, 0.7 |
| Grade, % | Grade 1, 45.7 Grade 2, 53.4 Unknown, 0.9 | Grade 1, 52.0 Grade 2, 41.0 Grade 3 (or unknown), 7.0 | Grade 1, 51.0 Grade 2, 39.0 Grade 3, 7.0 Unknown, 3.0 |
| Stage, % | Stage 2, 2.9 Stage 3, 26.5 Stage 4, 69.7 | Stage 1, 2.0 Stage 2, 11.0 Stage 3, 40.1 Stage 4, 46.0 Unknown, 0.9 | Stage 3, 40.4 Stage 4, 59.6 |
| Histologic confirmation | All | All | All |
| ECOG performance status, % | ECOG 0, 75.6 ECOG 1, 23.1 ECOG 2, 0.9 Unknown, 0.4 | ECOG 0, 85.4 ECOG 1, 14.3 ECOG 2 (or unknown), 0.3 | ECOG 0, 70.0 ECOG 1, 28.6 Unknown, 1.4 |
| All patients | BiovaxID | Specifid | MyVax |
| Study Characteristic | BiovaxID | Specifid | MyVax |
|---|---|---|---|
| Pre-vaccination therapy | PACE (min 6 cycles) or R-CHOP | Rituximab mg/m2 weekly for 4 weeks | CVP 8 cycles |
| Response status after pre-vaccination therapy | CR or unconfirmed CR | SD, PR, or CR | PR, CR, or unconfirmed CR |
| Randomization parameters | Randomization 2:1 in favor of the vaccine group Patients were stratified by IPI group (0–2 vs. 3–4) and number of chemotherapy cycles given (≤8 vs. >8) | Randomization 1:1 Patients were stratified by prior treatment (treatment-naïve vs. relapsed/refractory disease) and response to rituximab therapy (CR/PR vs. SD) | Randomization 2:1 in favor of the vaccine group Patients were stratified by study site and disease response status (CRu/PR vs. CR) |
| Vaccine manufacturing details | Isotype-matched (IgM/IgG) Id protein manufactured using a heterohybridoma technology | Isotype-matched Id protein manufactured using a proprietary recombinant technology | Isotype-matched Id protein manufactured using a recombinant technology |
| Therapy by study arm | Vaccine: 0.5 mg ID-KLH (1 day) + GM-CSF 100 mcg/m2/d (1 to 4 days) Control: 0.5 mg KLH + GM-CSF 100 mcg/m2/d (1 to 4 days) | Vaccine: 0.5 mg ID + 0.5 mg KLH (1 day) + 250 mcg/d GM-CSF (1 to 4 days) Control: 0.5 mg KLH + 250 mcg/d GM-CSF (1 to 4 days) | Vaccine: 0.5 mg ID + 0.5 mg KLH (1 day) 250 mcg/d GM-CSF (1 to 4 days) Control: 0.5 mg KLH + 250 mcg/d GM-CSF (1 to 4 days); |
| Therapy regimen | Five ID vaccine or control injections at 1, 2, 3, 4, and 6 months | Monthly for first 6 doses, every 2 months for next 6 doses, and then every 3 months until evidence of progressive disease or unacceptable toxicity was observed | Seven ID vaccine or control injections at 4-week intervals over a period of 24 weeks |
| Primary outcomes | DFS | TTP | PFS |
| Secondary outcomes | OS, safety, immunologic, and molecular responses | ORR, RRI, duration of response, safety | SALT-FS, IRS, safety |
| Study characteristic | BiovaxID | Specifid | MyVax |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suponin, A.; Zhelnov, P.; Potanin, A.; Chekalov, A.; Lomazov, A.; Vladimirova, K.; Lepik, K.; Muslimov, A. Therapeutic Vaccines for Follicular Lymphoma: A Systematic Review. Pharmaceuticals 2024, 17, 272. https://doi.org/10.3390/ph17030272
Suponin A, Zhelnov P, Potanin A, Chekalov A, Lomazov A, Vladimirova K, Lepik K, Muslimov A. Therapeutic Vaccines for Follicular Lymphoma: A Systematic Review. Pharmaceuticals. 2024; 17(3):272. https://doi.org/10.3390/ph17030272
Chicago/Turabian StyleSuponin, Andrei, Pavel Zhelnov, Artem Potanin, Andrey Chekalov, Aleksandr Lomazov, Kseniia Vladimirova, Kirill Lepik, and Albert Muslimov. 2024. "Therapeutic Vaccines for Follicular Lymphoma: A Systematic Review" Pharmaceuticals 17, no. 3: 272. https://doi.org/10.3390/ph17030272
APA StyleSuponin, A., Zhelnov, P., Potanin, A., Chekalov, A., Lomazov, A., Vladimirova, K., Lepik, K., & Muslimov, A. (2024). Therapeutic Vaccines for Follicular Lymphoma: A Systematic Review. Pharmaceuticals, 17(3), 272. https://doi.org/10.3390/ph17030272