
Unravelling Transplant-Ineligible Newly Diagnosed Multiple Myeloma Treatment in Real-World Practice in Spain: The CARINAE Study

 , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. Patients and Treatment
2.2. Laboratory/Molecular Findings
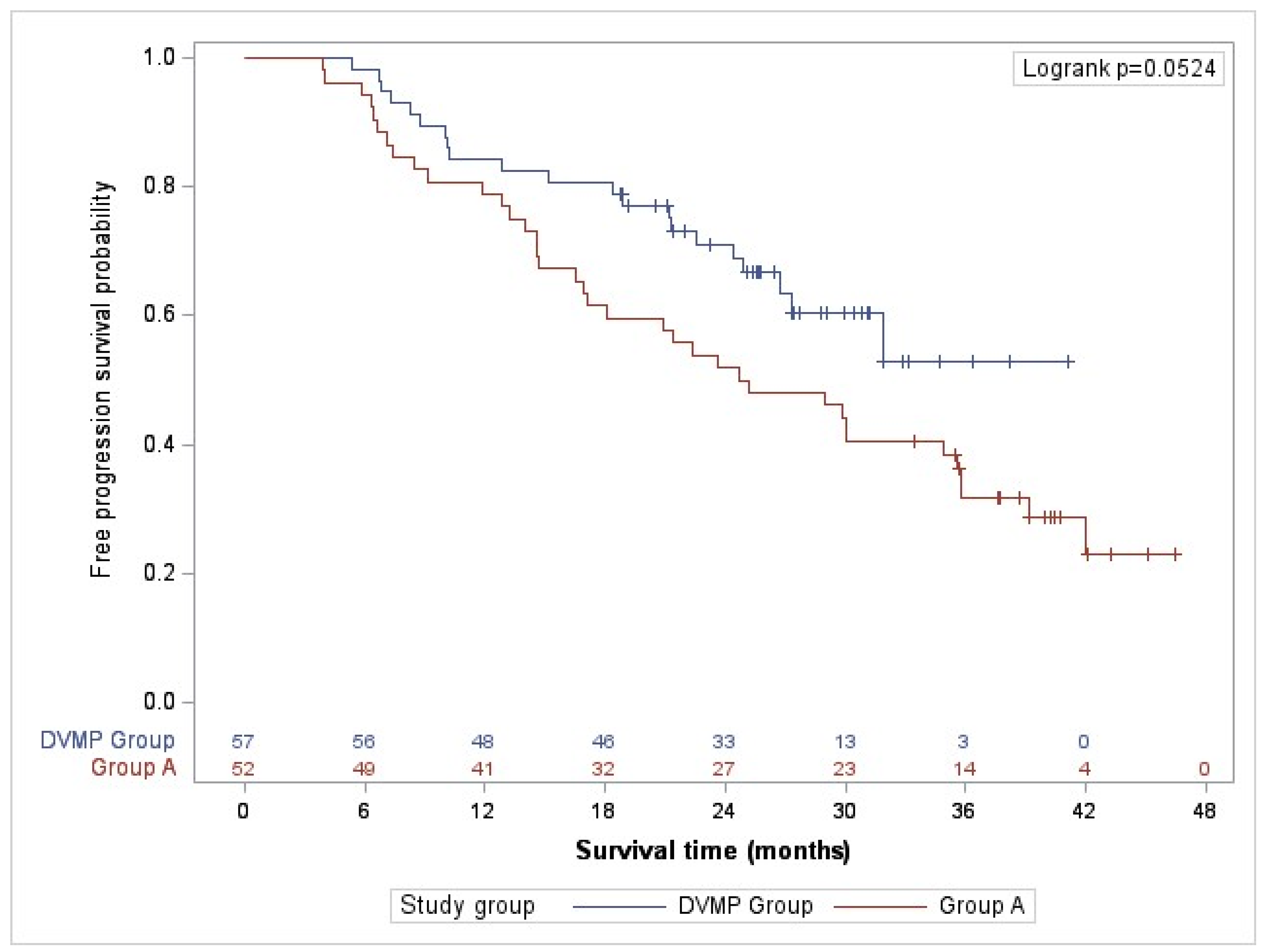
2.3. Effectiveness. Primary Objective
2.4. Clinical Response to Therapy
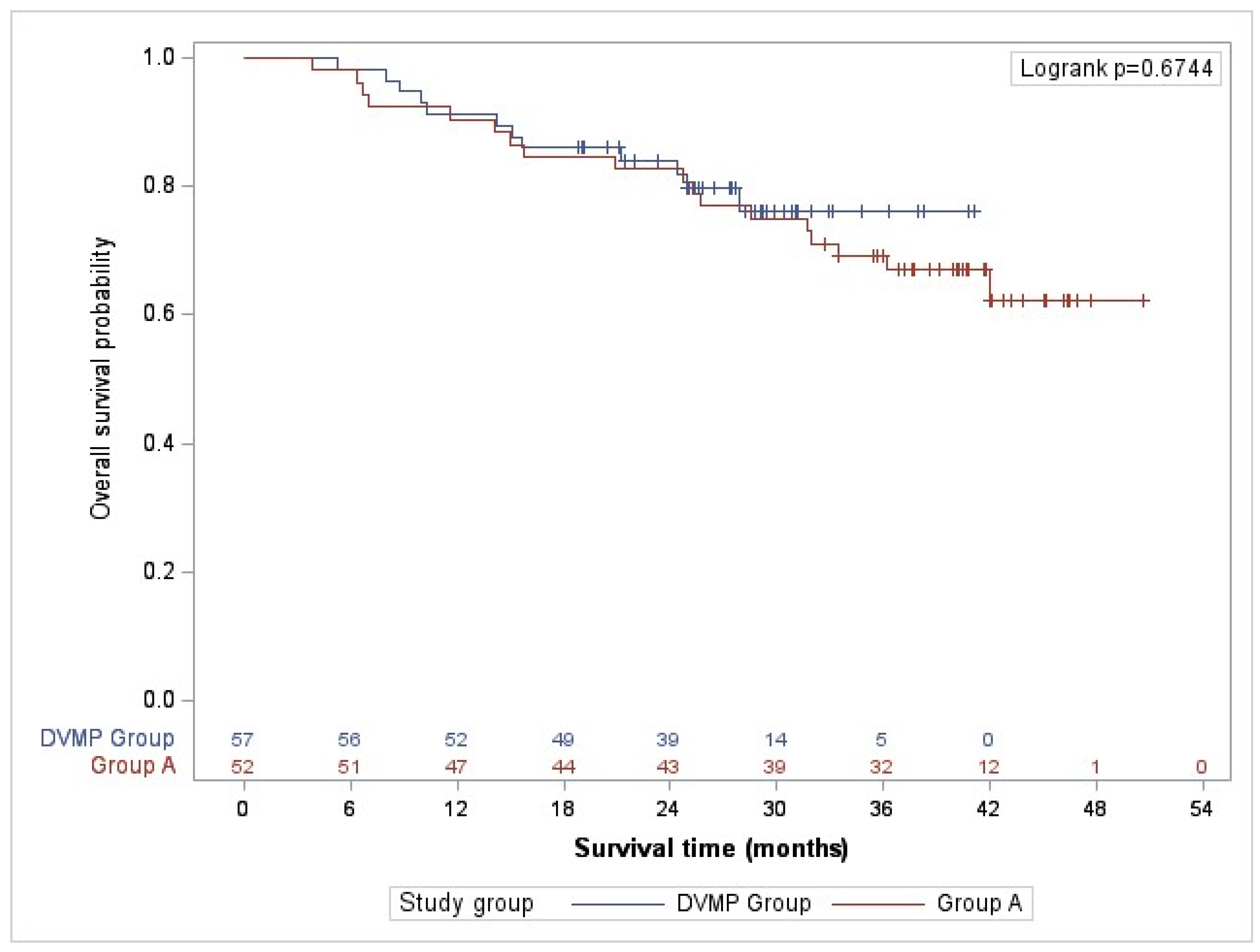
2.5. Overall Survival
2.6. Treatment Management in Clinical Practice in Spain
2.7. Safety
2.8. Patient’s Study Participation and Perspective
3. Discussion
4. Materials and Methods
4.1. Study Design and Patient Population
4.2. Primary and Secondary Endpoints
4.3. Statistical Methodology
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rajkumar, S.V. Multiple myeloma: 2016 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2016, 91, 719–734. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hernández-Rivas, J.; Mesa, M.G. Healthcare reality of the treatment of the high-risk multiple myeloma in Spain. Med. Clin. 2020, 154, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, A.; Rajkumar, S.V.; San Miguel, J.F.; Larocca, A.; Niesvizky, R.; Morgan, G.; Landgren, O.; Hajek, R.; Einsele, H.; Anderson, K.C.; et al. International Myeloma Working Group Consensus Statement for the Management, Treatment, and Supportive Care of Patients with Myeloma Not Eligible for Standard Autologous Stem-Cell Transplantation. J. Clin. Oncol. 2014, 32, 587–600. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Moreau, P.; Attal, M.; Hulin, C.; Arnulf, B.; Belhadj, K.; Benboubker, L.; Béné, M.C.; Broijl, A.; Caillon, H.; Caillot, D.; et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab before and after autologous stem-cell transplantation for newly diagnosed multiple myeloma (CASSIOPEIA): A randomised, open-label, phase 3 study. Lancet 2019, 394, 29–38, Erratum in Lancet 2019. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, S.V. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am. J. Hematol. 2022, 97, 1086–1107. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- D’Agostino, M.; Cairns, D.A.; Lahuerta, J.J.; Wester, R.; Bertsch, U.; Waage, A.; Zamagni, E.; Mateos, M.-V.; Dall’Olio, D.; van de Donk, N.W.; et al. Second Revision of the International Staging System (R2-ISS) for Overall Survival in Multiple Myeloma: A European Myeloma Network (EMN) Report Within the HARMONY Project. J. Clin. Oncol. 2022, 40, 3406–3418, Erratum in J. Clin. Oncol. 2022, 40, 4032. [Google Scholar] [CrossRef] [PubMed]
- Davies, F.E.; Pawlyn, C.; Usmani, S.Z.; San-Miguel, J.F.; Einsele, H.; Boyle, E.M.; Corre, J.; Auclair, D.; Cho, H.J.; Lonial, S.; et al. Perspectives on the Risk-Stratified Treatment of Multiple Myeloma. Blood Cancer Discov. 2022, 3, 273–284. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De Lusignan, S.; Crawford, L.; Munro, N. Creating and using real-world evidence to answer questions about clinical effectiveness. J. Innov. Health Inform. 2015, 22, 368–373. [Google Scholar] [CrossRef]
- Terpos, E.; Mikhael, J.; Hajek, R.; Chari, A.; Zweegman, S.; Lee, H.C.; Mateos, M.-V.; Larocca, A.; Ramasamy, K.; Kaiser, M.; et al. Management of patients with multiple myeloma beyond the clinical-trial setting: Understanding the balance between efficacy, safety and tolerability, and quality of life. Blood Cancer J. 2021, 11, 40. [Google Scholar] [CrossRef]
- Richardson, P.G.; Miguel, J.F.S.; Moreau, P.; Hajek, R.; Dimopoulos, M.A.; Laubach, J.P.; Palumbo, A.; Luptakova, K.; Romanus, D.; Skacel, T.; et al. Interpreting clinical trial data in multiple myeloma: Translating findings to the real-world setting. Blood Cancer J. 2018, 8, 109. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sanchez, L.; Wang, Y.; Siegel, D.S.; Wang, M.L. Daratumumab: A first-in-class CD38 monoclonal antibody for the treatment of multiple myeloma. J. Hematol. Oncol. 2016, 9, 51. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.; Ribeiro, M.; Scott, S.; Lonial, S. Daratumumab: Monoclonal antibody therapy to treat multiple myeloma. Drugs Today 2016, 52, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Krejcik, J.; Casneuf, T.; Nijhof, I.S.; Verbist, B.; Bald, J.; Plesner, T.; Syed, K.; Liu, K.; van de Donk, N.W.C.J.; Weiss, B.M.; et al. Daratumumab depletes CD38+ immune regulatory cells, promotes T-cell expansion, and skews T-cell repertoire in multiple myeloma. Blood 2016, 128, 384–394. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.C.; Stevenaert, F.; Krejcik, J.; Van Der Borght, K.; Smets, T.; Bald, J.; Abraham, Y.; Ceulemans, H.; Chiu, C.; Vanhoof, G.; et al. High-Parameter Mass Cytometry Evaluation of Relapsed/Refractory Multiple Myeloma Patients Treated with Daratumumab Demonstrates Immune Modulation as a Novel Mechanism of Action. Cytom. Part A 2019, 95, 279–289. [Google Scholar] [CrossRef]
- Mateos, M.-V.; Dimopoulos, M.A.; Cavo, M.; Suzuki, K.; Jakubowiak, A.; Knop, S.; Doyen, C.; Lúcio, P.; Nagy, Z.; Kaplan, P.; et al. Daratumumab plus Bortezomib, Melphalan, and Prednisone for Untreated Myeloma. N. Engl. J. Med. 2018, 378, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Mateos, M.-V.; Cavo, M.; Blade, J.; Dimopoulos, M.A.; Suzuki, K.; Jakubowiak, A.; Knop, S.; Doyen, C.; Lucio, P.; Nagy, Z.; et al. Overall survival with daratumumab, bortezomib, melphalan, and prednisone in newly diagnosed multiple myeloma (ALCYONE): A randomised, open-label, phase 3 trial. Lancet 2020, 395, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Facon, T.; Kumar, S.; Plesner, T.; Orlowski, R.Z.; Moreau, P.; Bahlis, N.; Basu, S.; Nahi, H.; Hulin, C.; Quach, H.; et al. Daratumumab plus Lenalidomide and Dexamethasone for Untreated Myeloma. N. Engl. J. Med. 2019, 380, 2104–2115. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rodriguez-Otero, P.; Boccadoro, M.; Hajek, R.; Fujisaki, T.; Lee, J.H.; Martinez-Lopez, J.; Lucio, P.; Nagy, Z.; Usenko, G.; Liberati, A.M.; et al. Long-Term Outcomes and Health-Related Quality of Life (HRQoL) By Response Status for Bortezomib, Melphalan, and Prednisone (VMP) ± Daratumumab (DARA) in Alcyone. Blood 2020, 136, 43–44. [Google Scholar] [CrossRef]
- Perrot, A.; Facon, T.; Plesner, T.; Usmani, S.Z.; Kumar, S.; Bahlis, N.J.; Hulin, C.; Orlowski, R.Z.; Nahi, H.; Mollee, P.; et al. Health-Related Quality of Life in Transplant-Ineligible Patients with Newly Diagnosed Multiple Myeloma: Findings from the Phase III MAIA Trial. J. Clin. Oncol. 2021, 39, 227–237. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rosiñol, L.; Oriol, A.; Teruel, A.I.; Hernández, D.; López-Jiménez, J.; de la Rubia, J.; Granell, M.; Besalduch, J.; Palomera, L.; González, Y.; et al. Superiority of bortezomib, thalidomide, and dexamethasone (VTD) as induction pretransplantation therapy in multiple myeloma: A randomized phase 3 PETHEMA/GEM study. Blood 2012, 120, 1589–1596. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; Jacobus, S.J.; Weller, E.A.; Hassoun, H.; Lonial, S.; Raje, N.S.; Medvedova, E.; McCarthy, P.L.; Libby, E.N.; Voorhees, P.M.; et al. Triplet Therapy, Transplantation, and Maintenance until Progression in Myeloma. New Engl. J. Med. 2022, 387, 132–147. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dimopoulos, M.A.; Moreau, P.; Terpos, E.; Mateos, M.V.; Zweegman, S.; Cook, G.; Delforge, M.; Hájek, R.; Schjesvold, F.; Cavo, M.; et al. Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 32, 309–322, Erratum in Ann Oncol. 2022, 33, 117. [Google Scholar] [CrossRef] [PubMed]
- Janssen [Data on File]. Number of patients treated with DARZALEX worldwide as of 31 March 2024. RF-412474.
- Miguel, J.F.S.; Schlag, R.; Khuageva, N.K.; Dimopoulos, M.A.; Shpilberg, O.; Kropff, M.; Spicka, I.; Petrucci, M.T.; Palumbo, A.; Samoilova, O.S.; et al. Continued Overall Survival Benefit After 5 Years’ Follow-up with Bortezomib-Melphalan-Prednisone (VMP) Versus Melphalan-Prednisone (MP) in Patients with Previously Untreated Multiple Myeloma, and No Increased Risk of Second Primary Malignancies: Final Results of the Phase 3 VISTA Trial. Blood 2011, 118, 476. [Google Scholar] [CrossRef]
- Mateos, M.-V.; Richardson, P.G.; Schlag, R.; Khuageva, N.K.; Dimopoulos, M.A.; Shpilberg, O.; Kropff, M.; Spicka, I.; Petrucci, M.T.; Palumbo, A.; et al. Bortezomib Plus Melphalan and Prednisone Compared with Melphalan and Prednisone in Previously Untreated Multiple Myeloma: Updated Follow-Up and Impact of Subsequent Therapy in the Phase III VISTA Trial. J. Clin. Oncol. 2010, 28, 2259–2266. [Google Scholar] [CrossRef] [PubMed]
- Benboubker, L.; Dimopoulos, M.A.; Dispenzieri, A.; Catalano, J.; Belch, A.R.; Cavo, M.; Pinto, A.; Weisel, K.; Ludwig, H.; Bahlis, N.; et al. Lenalidomide and Dexamethasone in Transplant-Ineligible Patients with Myeloma. N. Engl. J. Med. 2014, 371, 906–917. [Google Scholar] [CrossRef] [PubMed]
- Lahuerta, J.-J.; Paiva, B.; Vidriales, M.-B.; Cordón, L.; Cedena, M.-T.; Puig, N.; Martinez-Lopez, J.; Rosiñol, L.; Gutierrez, N.C.; Martín-Ramos, M.-L.; et al. Depth of Response in Multiple Myeloma: A Pooled Analysis of Three PETHEMA/GEM Clinical Trials. J. Clin. Oncol. 2017, 35, 2900–2910. [Google Scholar] [CrossRef]
- SEHH. Guía de Mieloma Múltiple Grupo Español de Mieloma. 2021. Available online: https://www.sehh.es/publicaciones/guias-recomendaciones/123889-guiasrecomendaciones-2020-2019 (accessed on 31 May 2024).
- Cedena, M.; Puig, N.; Paiva, B.; Pérez, A.; De Arriba, F.; Cuéllar, C.; Blanchard, M.J.; Martínez-Chamorro, C.; Casanova, M.; Sirvent, M.; et al. Enfermedad mínima residual en la práctica clínica de pacientes con mieloma múltiple, C0-013. In Proceedings of the LXI Congreso nacional de la sociedad Española de hematología y hemoterapia, Valencia, España, 24–26 October 2019; pp. 1–470. [Google Scholar]
- Janssen [Data on File]. Cavex program Spain_ Affidavit. As of 7 May 2024. RF-418728.
- Huynh, L.; Birsen, R.; Mora, L.; Couderc, A.L.; Mitha, N.; Farcet, A.; Chebib, A.; Chaibi, P. Multiple Myeloma in Patients over 80: A Real World Retrospective Study of First Line Conservative Approach with Bortezomib Dexamethasone Doublet Therapy and Mini-Review of Literature. Cancers 2022, 14, 4741. [Google Scholar] [CrossRef]
- He, J.; Duenas, A.; Collacott, H.; Lam, A.; Gries, K.S.; Carson, R.; Potthoff, D.; Trevor, N.; Tervonen, T. Patient Perceptions Regarding Multiple Myeloma and Its Treatment: Qualitative Evidence from Interviews with Patients in the United Kingdom, France, and Germany. Patient Patient Centered Outcomes Res. 2021, 14, 613–623. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
| Characteristics | Total (n = 109) | Group A (n = 52) | DVMP Group (n = 57) | p 1 |
|---|---|---|---|---|
| Age median (range) | 75.0 (63.0–88.0) | 76.5 (66.0–86.0) | 75.0 (63.0–88.0) | 0.2393 (u) |
| Sex n (%) | 0.7426 (c) | |||
| Male | 59 (54.1%) | 29 (55.8%) | 30 (52.6%) | |
| Female | 50 (45.9%) | 23 (44.2%) | 27 (47.4%) | |
| Comorbidities n (%) | ||||
| Cardiopathy | 31 (28.4%) | 17 (32.7%) | 14 (24.6%) | 0.3473 (c) |
| Peripheral neuropathy | 3 (2.8%) | 3 (5.8%) | 0 (0.0%) | 0.1053 (f) |
| Renal failure | 27 (24.8%) | 16 (30.8%) | 11 (19.3%) | 0.1658 (c) |
| Charlson’s comorbidities index median (range) | 3 (2–4) | 3 (2–4) | 3 (2–4) | 0.3005 (u) |
| ECOG PS n (%) | 0.1284 (c) | |||
| 0 | 23 (21.1%) | 7 (13.5%) | 16 (28.1%) | |
| 1 | 43 (39.4%) | 25 (48.1%) | 18 (31.6%) | |
| 2 | 24 (22.0%) | 9 (17.3%) | 15 (26.3%) | |
| 3 | 8 (7.3%) | 4 (7.7%) | 4 (7.0%) | |
| 4 | 1 (0.9%) | 0 (0.0%) | 1 (1.8%) | |
| NA | 10 (9.2%) | 7 (13.5%) | 3 (5.3%) | |
| Creatinine clearance n (%) | 0.1980 (c) | |||
| <30 mL/min | 13 (11.9%) | 8 (15.4%) | 5 (8.8%) | |
| 30–60 mL/min | 32 (29.4%) | 18 (34.6%) | 14 (24.6%) | |
| >60 mL/min | 52 (47.7%) | 23 (44.2%) | 29 (50.9%) | |
| NA | 12 (11.0%) | 3 (5.8%) | 9 (15.8%) | |
| Myeloma type 2 n (%) | ||||
| IgG 3 | 51 (46.8%) | 23 (44.2%) | 28 (49.1%) | 0.6092 (c) |
| IgA 3 | 35 (32.1%) | 15 (28.8%) | 20 (35.1%) | 0.4857 (c) |
| NA | 21 (19.3%) | 12 (23.1%) | 9 (15.8%) | 0.3353 (c) |
| Oligosecretory 4 | 5 (4.6%) | 3 (5.8%) | 2 (3.5%) | 0.6679 (f) |
| High-risk CG profile (FISH) 5 n (%) | ||||
| t (4;14) (p16; q32) | 8 (16.0%) | 5 (19.2%) | 3 (12.5%) | 0.7041 (f) |
| t (14;16) (q32; q23) | 2 (4.0%) | 1 (3.8%) | 1 (4.2%) | 1.0000 (f) |
| Del (17 p) | 5 (10.0%) | 2 (7.7%) | 3 (12.5%) | 0.6613 (f) |
| No CG abnormalities (FISH) 6 n (%) | 44 (40.4%) | 21 (40.4%) | 23 (40.4%) | 0.4467 (c) |
| Plasmacytoma 7,8 n (%) | 26 (24.1%) | 11 (21.6%) | 15 (26.3%) | 0.5646 (c) |
| Lytic bone lesions 7 n (%) | 66 (61.1%) | 29 (56.9%) | 37 (64.9%) | 0.3916 (c) |
| Disease staging ISS n (%) | 0.3126 (c) | |||
| I | 25 (22.9%) | 9 (17.3%) | 16 (28.1%) | |
| II | 39 (35.8%) | 19 (36.5%) | 20 (35.1%) | |
| III | 40 (36.7%) | 20 (38.5%) | 20 (35.1%) | |
| NA | 5 (4.6%) | 4 (7.7%) | 1 (1.8%) | |
| Revised disease staging R-ISS n (%) | 0.3294 (c) | |||
| I | 19 (17.4%) | 6 (11.5%) | 13 (22.8%) | |
| II | 54 (49.5%) | 28 (53.8%) | 26 (45.6%) | |
| III | 17 (15.6%) | 10 (19.2%) | 7 (12.3%) | |
| NA | 19 (17.4%) | 8 (15.4%) | 11 (19.3%) |
| Front-Line Treatment 1 n (%) | Group A (n = 52) |
|---|---|
| Bortezomib-based regimens | 30 (57.7%) |
| Bortezomib-Melphalan-Prednisone | 17 (32.7%) |
| Lenalidomide-based regimens | 14 (26.9%) |
| Lenalidomide-Dexamethasone | 14 (26.9%) |
| Bortezomib + lenalidomide-based regimens | 4 (7.7%) |
| Bortezomib-Lenalidomide-Dexamethasone | 3 (5.8%) |
| Alkylating Agents-based regimens | 4 (7.7%) |
| Melphalan-Prednisone | 2 (3.8%) |
| Event n (%) | Censored n (%) | Survival Probability | Log Rank | |
|---|---|---|---|---|
| Complete follow-up | 0.0524 | |||
| Group A | 37 (71.2%) | 15 (28.8%) | 0.2306 | |
| DVMP Group | 21 (36.8%) | 36 (63.2%) | 0.5285 | |
| 18-month follow-up | 0.0325 | |||
| Group A | 20 (38.5%) | 32 (61.5%) | 0.6154 | |
| DVMP Group | 11 (19.3%) | 46 (80.7%) | 0.8070 | |
| 24-month follow-up | 0.0390 | |||
| Group A | 25 (48.1%) | 27 (51.9%) | 0.5192 | |
| DVMP Group | 16 (28.1%) | 41 (71.9%) | 0.7107 | |
| 36-month follow-up 1 | 0.0545 | |||
| Group A | 35 (67.3%) | 17 (32.7%) | 0.3170 | |
| DVMP Group | 21 (36.8%) | 36 (63.2%) | 0.5285 |
| Best Response n (%) | Total (n = 109) | Group A (n = 52) | DVMP Group (n = 57) | p 1 |
|---|---|---|---|---|
| ≥Complete response | 36 (33.0%) | 15 (28.8%) | 21 (36.8%) | 0.3753 |
| ≥Very good partial response | 73 (67.0%) | 30 (57.7%) | 43 (75.4%) | 0.0491 |
| Strict complete response | 15 (13.8%) | 10 (19.2%) | 5 (8.8%) | 0.0803 |
| Complete response | 21 (19.3%) | 5 (9.6%) | 16 (28.1%) | |
| Very good partial response | 37 (33.9%) | 15 (28.8%) | 22 (38.6%) | |
| Partial response | 23 (21.1%) | 13 (25.0%) | 10 (17.5%) | |
| Minimum response | 3 (2.8%) | 2 (3.8%) | 1 (1.8%) | |
| Stable disease | 9 (8.3%) | 6 (11.5%) | 3 (5.3%) | |
| Disease progression | 1 (0.9%) | 1 (1.9%) | 0 (0.0%) |
| Relapse/PD | Total (n = 109) | Group A (n = 52) | DVMP Group (n = 57) | p 1 |
|---|---|---|---|---|
| First-line treatment PD n (%) | 0.0004 | |||
| Yes | 44 (40.4%) | 30 (57.7%) | 14 (24.6%) | |
| No | 65 (59.6%) | 22 (42.3%) | 43 (75.4%) | |
| Tye of relapse 2 n (%) | 0.7204 | |||
| Biological–No treatment | 11 (25.0%) | 7 (23.3%) | 4 (28.6%) | |
| Biological–Treatment | 13 (29.5%) | 10 (33.3%) | 3 (21.4%) | |
| Symptomatic relapse | 20 (45.5%) | 13 (43.3%) | 7 (50.0%) |
| RAMs | Total (n = 111) | Group A (n = 53) | DVMP Group (n = 58) | p 1 |
|---|---|---|---|---|
| Patients with RAMs n (%) | 0.4734 | |||
| Yes | 81 (73.0%) | 37 (69.8%) | 44 (75.9%) | |
| No | 30 (27.0%) | 16 (30.2%) | 14 (24.1%) | |
| No RAMs reported | 251 | 129 | 122 | -- |
| Patients with serious RAMs n (%) | 0.8030 | |||
| Yes | 24 (21.6%) | 12 (22.6%) | 12 (20.7%) | |
| No | 87 (78.4%) | 41 (77.4%) | 46 (79.3%) | |
| No serious RAMs reported | 28 | 13 | 15 | |
| RAMs characteristics 2 | ||||
| Serious n (%) | 0.5770 | |||
| Yes | 28 (11.2%) | 13 (10.1%) | 15 (12.3%) | |
| No | 223 (88.8%) | 116 (89.9%) | 107 (87.7%) | |
| Severity criterion 3 n (%) | 0.2657 | |||
| Life-threatening | 2 (7.1%) | 2 (15.4%) | 0 (0.0%) | |
| Hospitalization | 14 (50.0%) | 7 (53.8%) | 7 (46.7%) | |
| Hospitalization prolonged | 3 (10.7%) | 1 (7.7%) | 2 (13.3%) | |
| Other medical reason | 8 (28.6%) | 2 (15.4%) | 6 (40.0%) | |
| Death | 1 (3.6%) | 1 (7.7%) | 0 (0.0%) | |
| Intensity n (%) | 0.0277 | |||
| Grade 1 | 104 (41.4%) | 48 (37.2%) | 56 (45.9%) | |
| Grade 2 | 93 (37.1%) | 50 (38.8%) | 43 (35.2%) | |
| Grade 3 | 41 (16.3%) | 28 (21.7%) | 13 (10.7%) | |
| Grade 4 | 11 (4.4%) | 2 (1.6%) | 9 (7.4%) | |
| Grade 5 | 2 (0.8%) | 1 (0.8%) | 1 (0.8%) | |
| Result n (%) | 0.9276 | |||
| Recovered without sequalae | 227 (90.4%) | 116 (89.9%) | 111 (91.0%) | |
| Not recovered, improving | 7 (2.8%) | 4 (3.1%) | 3 (2.5%) | |
| Not recovered, ongoing | 9 (3.6%) | 4 (3.1%) | 5 (4.1%) | |
| Recovered with sequalae | 5 (2.0%) | 3 (2.3%) | 2 (1.6%) | |
| Unknown | 1 (0.4%) | 1 (0.8%) | 0 (0.0%) | |
| Death | 2 (0.8%) | 1 (0.8%) | 1 (0.8%) |
| AEs | Total (n = 111) | Group A (n = 53) | DVMP Group (n = 58) | p 1 |
|---|---|---|---|---|
| Patients with AEs n (%) | <0.0001 | |||
| Yes | 45 (40.5%) | 11 (20.8%) | 34 (58.6%) | |
| No | 66 (59.5%) | 42 (79.2%) | 24 (41.4%) | |
| No of AEs reported | 172 | 39 | 133 | |
| Patients with serious AEs (SAEs) n (%) | 0.0002 | |||
| Yes | 17 (15.3%) | 1 (1.9%) | 16 (27.6%) | |
| No | 94 (84.7%) | 52 (98.1%) | 42 (72.4%) | |
| No of SAEs reported | 26 | 3 | 23 | |
| AEs characteristics 2 | ||||
| Serious n (%) | 0.1411 | |||
| Yes | 26 (15.1%) | 3 (7.7%) | 23 (17.3%) | |
| No | 146 (84.9%) | 36 (92.3%) | 110 (82.7%) | |
| Severity criterion 3 n (%) | 0.6013 | |||
| Life-threatening | 2 (7.7%) | 0 (0.0%) | 2 (8.7%) | |
| Hospitalization | 20 (76.9%) | 2 (66.7%) | 18 (78.3%) | |
| Death | 4 (15.4%) | 1 (33.3%) | 3 (13.0%) | |
| Intensity n (%) | 0.3903 | |||
| Grade 1 | 86 (50.0%) | 23 (59.0%) | 63 (47.4%) | |
| Grade 2 | 58 (33.7%) | 13 (33.3%) | 45 (33.8%) | |
| Grade 3 4 | 24 (14.0%) | 2 (5.1%) | 22 (16.5%) | |
| Grade 4 | 1 (0.6%) | 0 (0.0%) | 1 (0.8%) | |
| Grade 5 | 3 (1.7%) | 1 (2.6%) | 2 (1.5%) | |
| Result n (%) | 0.3856 | |||
| Recovered without sequalae | 120 (69.8%) | 27 (69.2%) | 93 (69.9%) | |
| Not recovered, improving | 8 (4.7%) | 2 (5.1%) | 6 (4.5%) | |
| Not recovered, ongoing | 33 (19.2%) | 8 (20.5%) | 25 (18.8%) | |
| Recovered with sequalae | 6 (3.5%) | 0 (0.0%) | 6 (4.5%) | |
| Unknown | 1 (0.6%) | 1 (2.6%) | 0 (0.0%) | |
| Death | 4 (2.3%) | 1 (2.6%) | 3 (2.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Arriba de la Fuente, F.; Gironella Mesa, M.; Hernández García, M.T.; Soler Campos, J.A.; Herráez Rodríguez, S.; Moreno Belmonte, M.J.; Regueiro López, T.; González-Pardo, M.; Casanova Espinosa, M.; on behalf of the CARINAE Study Investigators. Unravelling Transplant-Ineligible Newly Diagnosed Multiple Myeloma Treatment in Real-World Practice in Spain: The CARINAE Study. Pharmaceuticals 2024, 17, 1272. https://doi.org/10.3390/ph17101272
de Arriba de la Fuente F, Gironella Mesa M, Hernández García MT, Soler Campos JA, Herráez Rodríguez S, Moreno Belmonte MJ, Regueiro López T, González-Pardo M, Casanova Espinosa M, on behalf of the CARINAE Study Investigators. Unravelling Transplant-Ineligible Newly Diagnosed Multiple Myeloma Treatment in Real-World Practice in Spain: The CARINAE Study. Pharmaceuticals. 2024; 17(10):1272. https://doi.org/10.3390/ph17101272
Chicago/Turabian Stylede Arriba de la Fuente, Felipe, Mercedes Gironella Mesa, Miguel Teodoro Hernández García, Juan Alonso Soler Campos, Susana Herráez Rodríguez, María José Moreno Belmonte, Teresa Regueiro López, Miriam González-Pardo, María Casanova Espinosa, and on behalf of the CARINAE Study Investigators. 2024. "Unravelling Transplant-Ineligible Newly Diagnosed Multiple Myeloma Treatment in Real-World Practice in Spain: The CARINAE Study" Pharmaceuticals 17, no. 10: 1272. https://doi.org/10.3390/ph17101272
APA Stylede Arriba de la Fuente, F., Gironella Mesa, M., Hernández García, M. T., Soler Campos, J. A., Herráez Rodríguez, S., Moreno Belmonte, M. J., Regueiro López, T., González-Pardo, M., Casanova Espinosa, M., & on behalf of the CARINAE Study Investigators. (2024). Unravelling Transplant-Ineligible Newly Diagnosed Multiple Myeloma Treatment in Real-World Practice in Spain: The CARINAE Study. Pharmaceuticals, 17(10), 1272. https://doi.org/10.3390/ph17101272