
The Effect of Acetylsalicylic Acid, as a Representative Non-Steroidal Anti-Inflammatory Drug, on the Activity of Myeloperoxidase


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
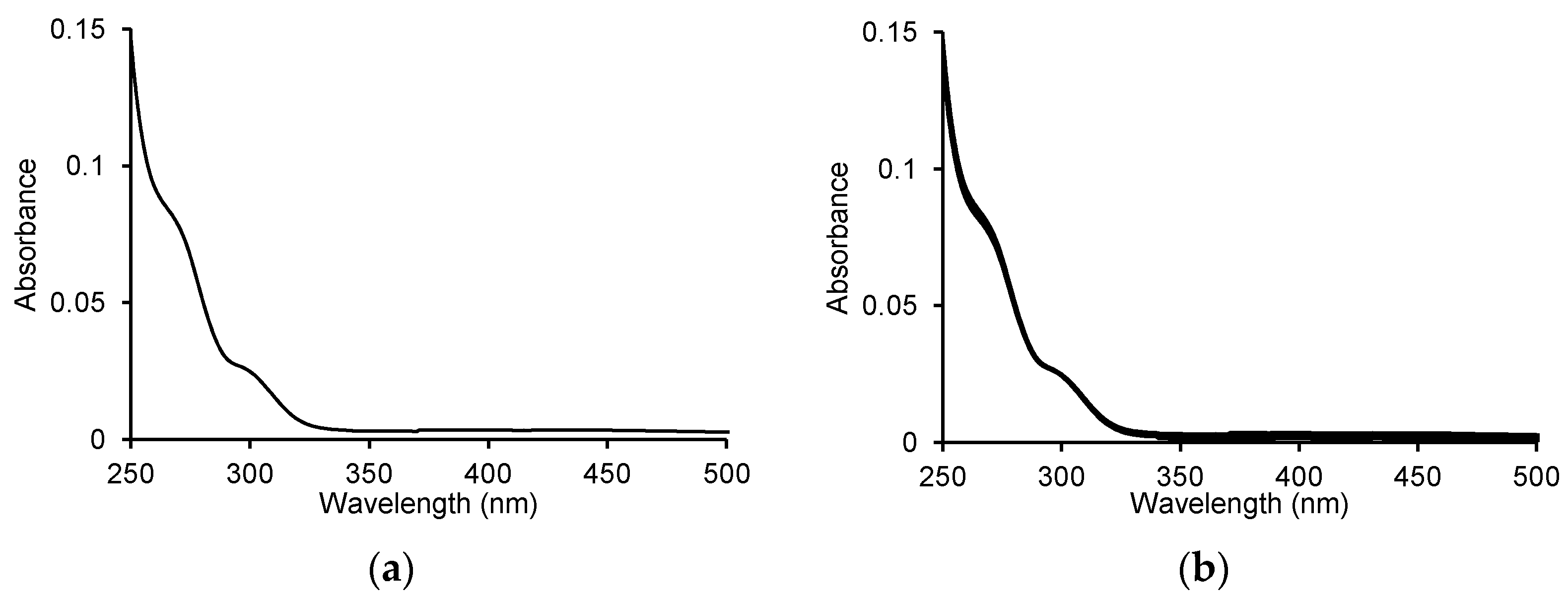
2.1. Oxidation of ASA by MPO
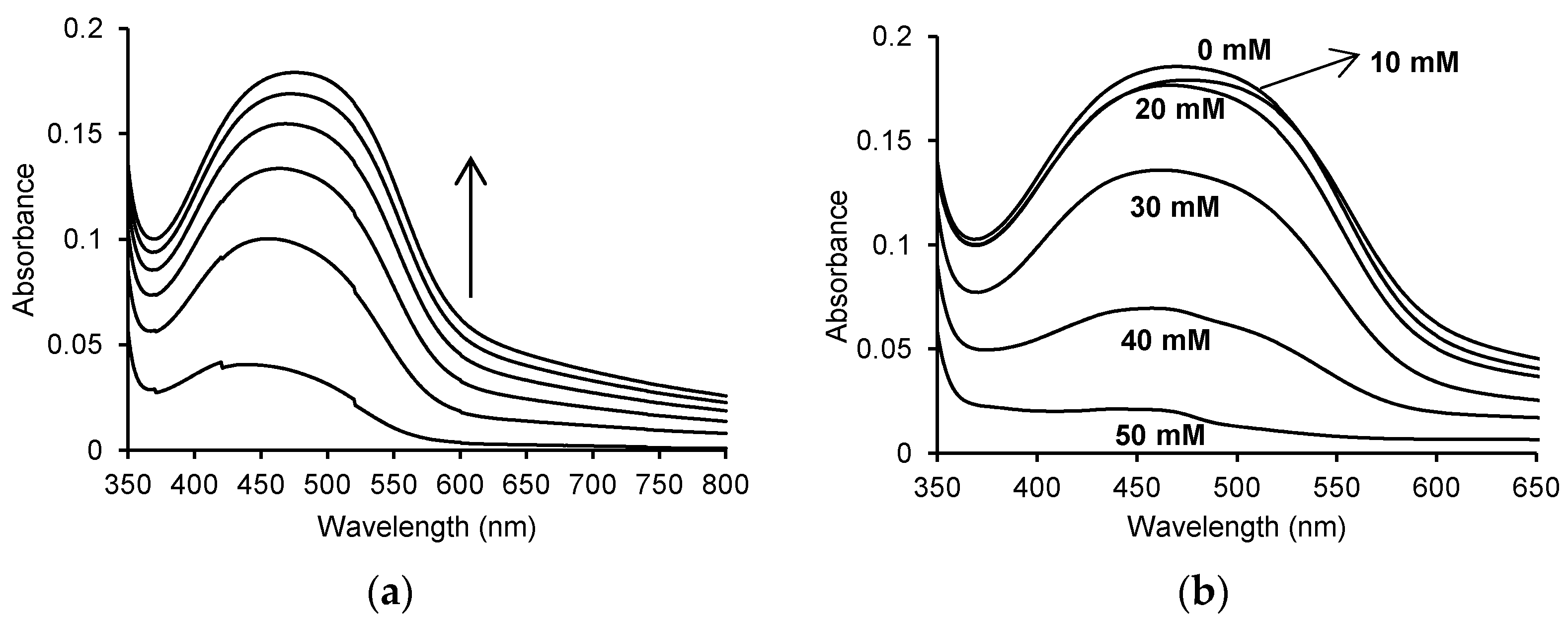
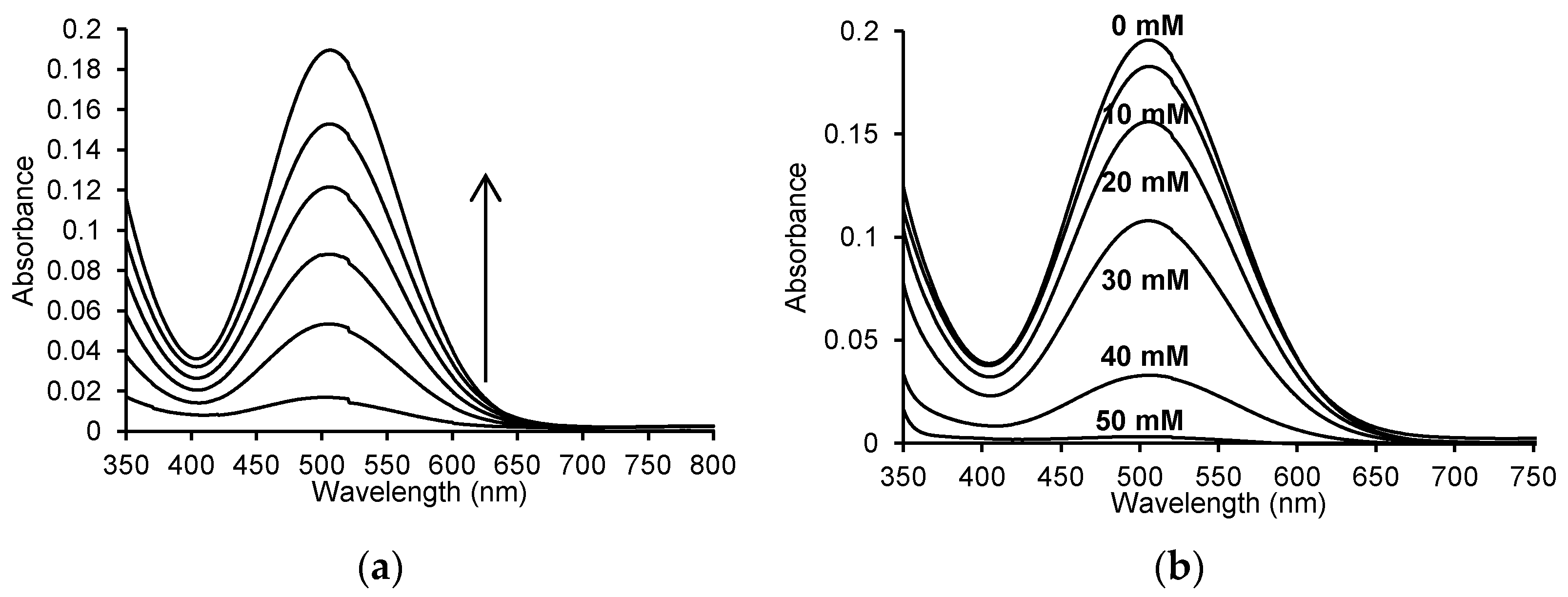
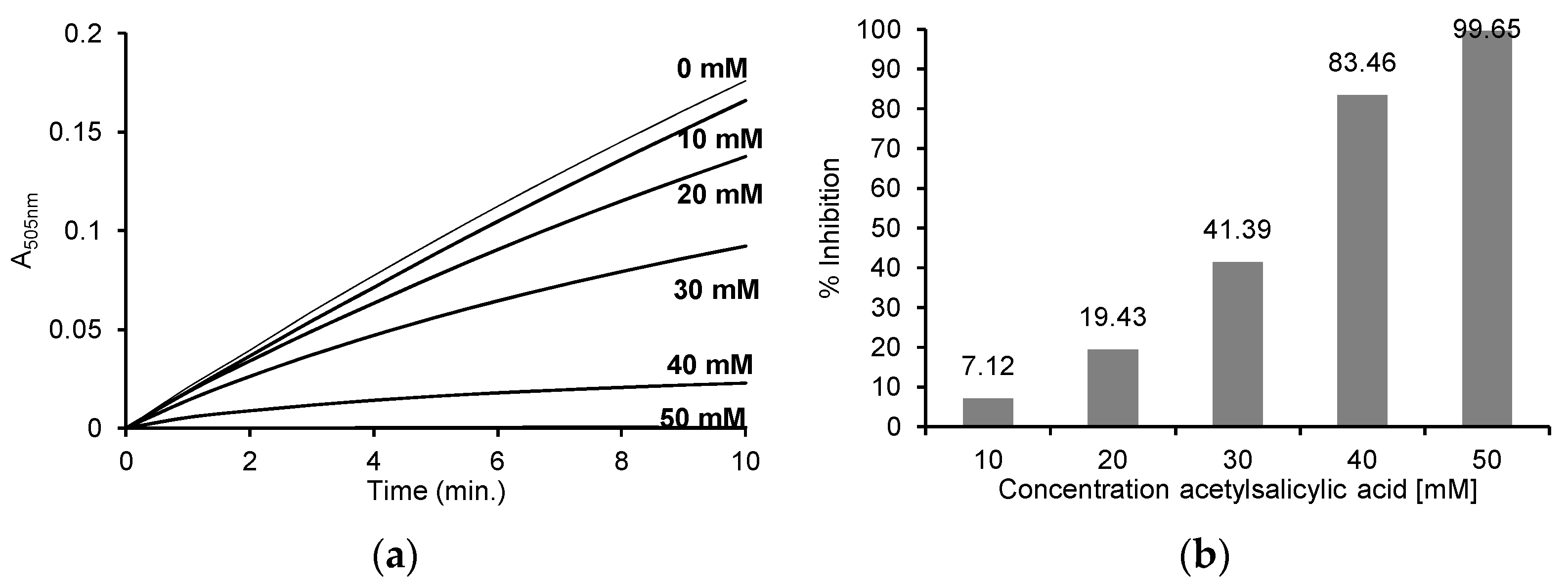
2.2. Oxidation of O-Dianisidine Dihydrochloride by MPO in the Presence of ASA
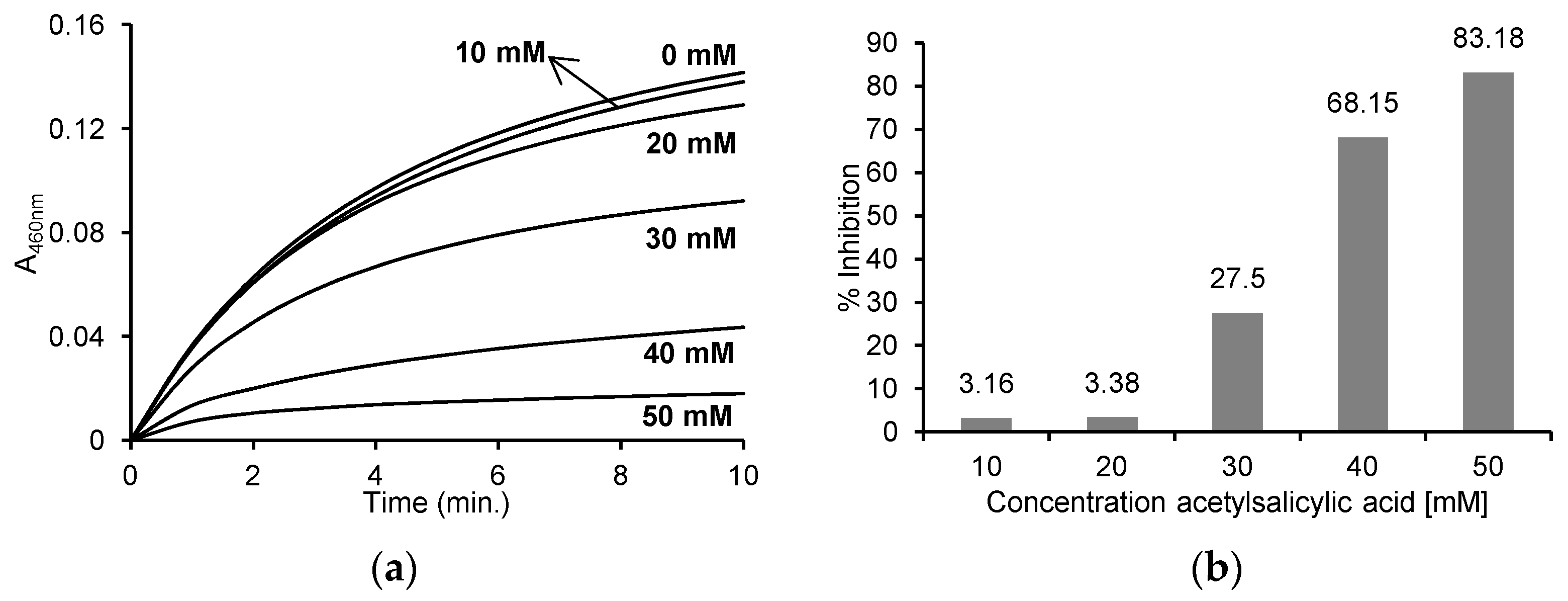
2.3. Oxidation of MCD by MPO in the Presence of ASA
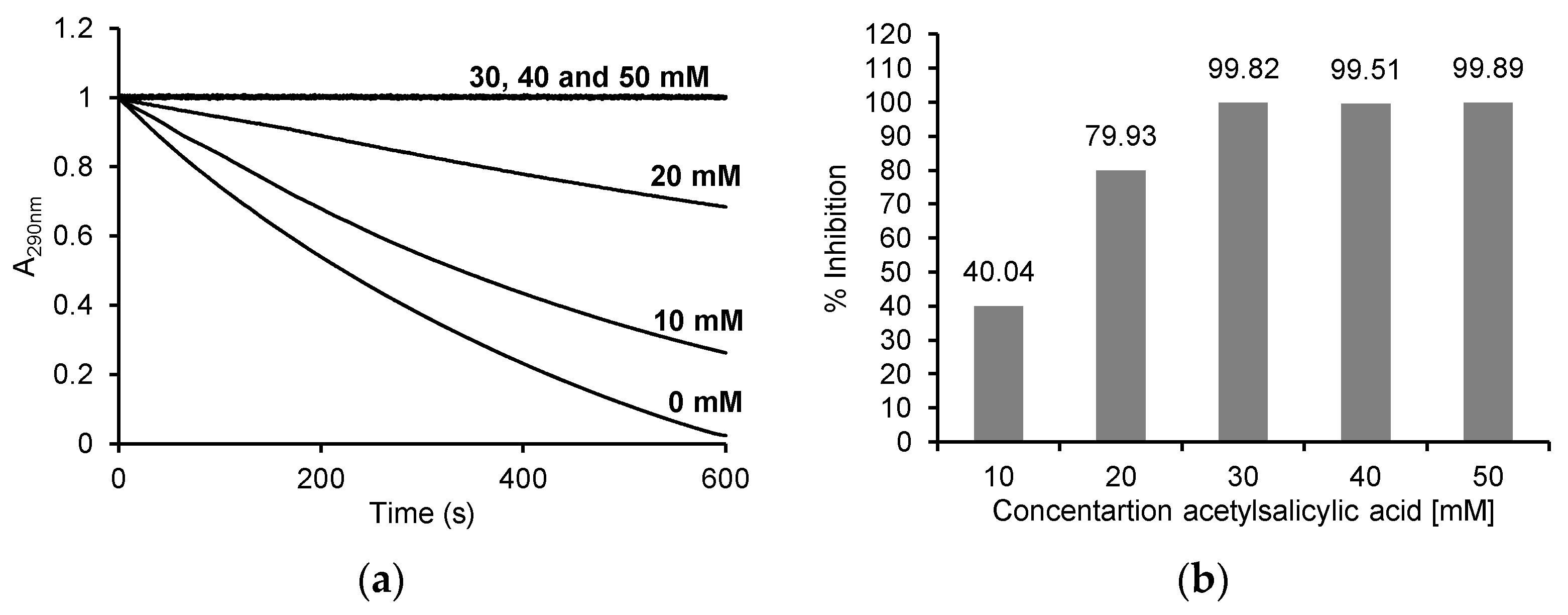
2.4. Oxidation of 4-Aminoantipyrine by MPO in the Presence of ASA
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Spectrophotometric Measurements
4.3. The Effect of ASA on the Peroxidase Activity of MPO
4.4. The Effect of ASA on the Chlorinating Activity of MPO
4.5. The Effect of ASA on MPO Activity Using 4-Aminoantipyrine as a Hydrogen Donor
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zederbauer, M.; Jantschko, W.; Neugschwandtner, K.; Jakopitsch, C.; Moguilevsky, N.; Obinger, C.; Furtmüller, P.G. Role of the covalent glutamic acid 242−heme linkage in the formation and reactivity of redox intermediates of human myeloperoxidase. Biochemistry 2005, 44, 6482–6491. [Google Scholar] [CrossRef]
- Davies, M.J.; Hawkins, C.L.; Pattison, D.I.; Rees, M.D. Mammalian heme peroxidases: From molecular mechanisms to health implications. Antioxid. Redox Signal. 2008, 10, 1199–1234. [Google Scholar] [CrossRef] [PubMed]
- Gungor, N.; Knaapen, A.M.; Munnia, A.; Peluso, M.; Haenen, G.R.; Chiu, R.K.; Godschalk, R.W.L.; van Schooten, F.J. Genetoxic effects of neutrophils and hypochlorous acid. Mutagenesis 2010, 25, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Alsahli, M.A.; Rahmani, A.H. Myeloperoxidase as an Active Disease Biomarker: Recent Biochemical and Pathological Perspectives. Med. Sci. 2018, 6, 33. [Google Scholar] [CrossRef]
- Castillo-Tong, D.C.; Pils, D.; Heinze, G.; Braicu, I.; Sehouli, J.; Reinthaller, A.; Schauster, E.; Wolf, A.; Watrowski, R.; Maki, R.A.; et al. Association of myeloperoxidase with ovarian cancer. Tumour Biol. 2014, 35, 141–148. [Google Scholar] [CrossRef]
- Saed, G.M.; Ali-Fehm, R.; Jiang, Z.L.; Flechter, N.M.; Diamond, M.P.; Abu-Soud, H.M.; Munkarah, A.R. Myeloperoxidase serves as a redox switch that regulates apoptosis in epithelial ovarian cancer. Gynecol. Oncol. 2010, 116, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Samborski, W.; Niklas, A.; Filipiak, K.J.; Kaczmarczyk, J.; Dobrowolska-Zachwieja, A.; Tykarski, A. Niesteroidowe leki przeciwzapalne a powikłania sercowo-naczyniowe i gastroenterologiczne—Algorytm wyboru. Chor. Serca Naczyń 2017, 14, 238–247. [Google Scholar]
- Ghlichloo, I.; Gerriets, V. Nonsteroidal Anti-inflammatory Drugs (NSAIDs). In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Czyż, M.; Watała, C. Aspirin—The prodigious panacea? Molecular mechanisms of the action of acetylsalicylic acid in the organism. Postepy. Hig. Med. Dosw. 2005, 59, 105–115. [Google Scholar]
- Guo, J.; Zhu, Y.; Yu, L.; Li, Y.; Guo, J.; Cai, J.; Liu, L.; Wang, Z. Aspirin inhibits tumor progression and enhances cisplatin sensitivity in epithelial ovarian cancer. PeerJ 2021, 9, e11591. [Google Scholar] [CrossRef]
- Bashir, A.U.I.J.; Kankipati, C.S.; Jones, S.; Newman, R.M.; Safrany, S.T.; Perry, C.J.; Nicholl, I.D. A novel mechanism for the anticancer activity of aspirin and salicylates International. J. Oncol. 2019, 54, 1256–1270. [Google Scholar]
- Chan, A.T.; Arber, N.; Burn, J.; Chia, W.K.; Elwood, P.; Hull, M.A.; Logan, R.F.; Rothwell, P.M.; Schroer, K.; Baron, J.A. Aspiryn in the chemoprevention of colorectal neoplasia: An overview. Cancer Prev. Res. 2012, 5, 164–178. [Google Scholar] [CrossRef] [PubMed]
- Merritt, M.A.; Rice, M.S.; Barnard, M.E. Pre-diagnosis and post-diagnosis use of common analgesics and ovarian cancer prognosis (NHS/NHSII): A prospective cohort study. Lancet Oncol. 2018, 19, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Rahmani, A.H.; Aldebasi, Y.H.; Aly, S.M. Biochemical and Pathological Studies on Peroxidases: An Updated Review. Glob. J. Health Sci. 2014, 6, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, N.M.; Jiang, Z.; Ali-Fehmi, R.; Levin, N.K.; Belotte, J.; Tainsky, M.A.; Diamond, M.P.; Abu-Soud, H.M.; Saed, G.M. Myeloperoxidase and free iron levels: Potential biomarkers for early detection and prognosis of ovarian cancer. Cancer Biomark. 2012, 10, 267–275. [Google Scholar] [CrossRef]
- Olson, S.H.; Carlson, M.D.A.; Ostrer, H.; Harlap, S.; Stone, A.; Winters, M.; Ambrosone, C.B. Genetic variants in SOD2, MPO, and NQO1, and risk of ovarian cancer. Gynecol. Oncol. 2004, 93, 615–620. [Google Scholar] [CrossRef]
- Droeser, R.A.; Mechera, R.; Däster, S.; Weixler, B.; Kraljević, M.; Delko, T.; Güth, U.; Stadlmann, S.; Terracciano, L.; Singer, G. MPO density in primary cancer biopsies of ovarian carcinoma enhances the indicative value of IL-17 for chemosensitivity. BMC Cancer 2016, 16, 639. [Google Scholar] [CrossRef]
- Dai, Y.; Cheng, S.; Wang, Z.; Zhang, R.; Yang, Z.; Wang, J.; Yung, B.C.; Wang, Z.; Jacobson, O.; Xu, C.; et al. Hypochlorous acid promoted platinum drug chemotherapy by meloperoxidase-encapsulated therapeutic metal phenolic nanoparticles. ACS Nano 2018, 12, 455–463. [Google Scholar] [CrossRef]
- Masucci, M.T.; Minopoli, M.; Del Vecchio, S.; Carriero, M.V. The Emerging Role of Neutrophil Extracellular Traps (NETs) in Tumor Progression and Metastasis. Front. Immunol. 2020, 11, 1749. [Google Scholar] [CrossRef]
- Lockhart, J.S.; Sumagin, R. Non-Canonical Functions of Myeloperoxidase in Immune Regulation, Tissue Inflammation and Cancer. Int. J. Mol. Sci. 2022, 23, 12250. [Google Scholar] [CrossRef]
- Panagopoulos, V.; Leach, D.A.; Zinonos, I.; Ponomarev, V.; Licari, G.; Liapis, V.; Ingman, W.V.; Anderson, P.; DeNichilo, M.O.; Evdokiou, A. Inflammatory peroxidases promote breast cancer progression in mice via regulation of the tumour microenvironment. Int. J. Oncol. 2017, 50, 1191–1200. [Google Scholar] [CrossRef]
- Liu, T.W.; Gammon, S.T.; Yang, P.; Fuentes, D.; Piwnica-Worms, D. Myeloid cell-derived HOCl is a paracrine effector that trans-inhibits IKK/NF-κB in melanoma cells and limits early tumor progression. Sci. Signal. 2021, 14, eaax5971. [Google Scholar] [CrossRef]
- Xiao, Y.; Bi, M.; Guo, H.; Li, M. Multi-omics approaches for biomarker discovery in early ovarian cancer diagnosis. eBiomed. Part Lancet Discov. Sci. 2022, 79, 104001. [Google Scholar] [CrossRef] [PubMed]
- Gąsowska-Bajger, B.; Gąsowska-Bodnar, A.; Bodnar, L. Properties and functions of myeloperoxidase and its role in ovarian cancer. Med. Sci. Pulse 2022, 16, 23–32. [Google Scholar] [CrossRef]
- Hyuna Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Ahmedin Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Doherty, J.A.; Peres, L.C.; Wang, C.; Way, G.P.; Greene, C.S.; Schildkraut, J.M. Challenges and opportunities in studying the epidemiology of ovarian cancer subtypes. Curr. Epidemiol. Rep. 2017, 4, 211–220. [Google Scholar] [CrossRef]
- Joharatnam-Hogan, N.; Cafferty, F.H.; Macnair, A.; Ring, A.; Langley, R.E. The role of aspirin in the prevention of ovarian, endometrial and cervical cancers. Womens Health 2020, 16, 1745506520961710. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.W.; Gammon, S.T.; Yang, P.; Ma, W.; Wang, J.; Piwnica-Worms, D. Inhibition of myeloperoxidase enhances immune checkpoint therapy for melanoma. J. Immunother. Cancer 2023, 11, e005837. [Google Scholar] [CrossRef]
- Pollard, M.; Luckert, P.H.; Schmidt, M.A. The suppressive effect of piroxicam on autochthonous intestitial tumours in the rat. Cancer Lett. 1983, 21, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Reddy, B.B.; Maruyama, H.; Kelloff, G. Dose-related inhibition of colon carcinogenesis by dietary piroxicam, a nonsteroidal antiinflammatory drug, during different stages of rat colon tumour development. Cancer Res. 1987, 47, 5340–5346. [Google Scholar]
- Rao, C.V.; Rivenson, A.; Simi, B.; Zang, E.; Kelloff, G.; Steele, V.; Reddy, B.S. Chemoprevention of colon carcinogenesis by sulindac, a nonsteroidal antiinflammatory agent. Cancer Res. 1995, 55, 1464–1472. [Google Scholar]
- Craven, P.A.; DeRubertis, F.R. Effect of aspirin on 1,2-dimethylhydrazine-induced colonic carcinogenesis. Carcinogenesis 1992, 13, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Moorghen, M.; Ince, P.; Finney, K.J.; Sunter, J.P.; Appleton, D.R.; Watson, A.J. A protective effect of sulindac against chemically-induced primary colonic tumours in mice. J. Pathol. 1988, 156, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Waddell, W.R.; Loughry, R.W. Sulindac for polyposis of the colon. J. Surg. Oncol. 1983, 24, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Kune, G.A.; Kune, S.; Watson, L.F. Colorectal cancer risk, chronic illnesses, operations and medications: Case control results from the Melbourne Colorectal Cancer study. Cancer Res. 1988, 48, 4399–4404. [Google Scholar] [CrossRef]
- Gridley, G.; McLaughlin, J.K.; Ekbom, A.; Klareskog, L.; Adami, H.O.; Hacker, D.G.; Hoover, R.; Fraumeni, J.F., Jr. Incidence of cancer among patients with rheumatoid arthritis. J. Natl. Cancer Inst. 1993, 85, 307–311. [Google Scholar] [CrossRef]
- La Vecchia, C.; Negri, E.; Franceschi, S.; Conti, E.; Montella, M.; Giacosa, A.; Falcini, A.; Decarli, A. Aspirin and colorectal cancer. Br. J. Cancer 1997, 76, 675–677. [Google Scholar] [CrossRef]
- Giovannuci, E.; Egan, K.M.; Hunter, D.J.; Stampfer, M.J.; Colditz, G.A.; Eillett, W.C.; Speizer, F.E. Aspirin and the risk of colorectal cancer in woman. N. Engl. J. Med. 1995, 333, 609–614. [Google Scholar] [CrossRef]
- Schreinemachers, D.M.; Everson, R.B. Aspirin use and lung, colon and breast cancer incidence in a prospective study. Epidemiology 1994, 5, 138–146. [Google Scholar] [CrossRef]
- Fischer, S.M.; Mills, G.D.; Slaga, T.J. Inhibition of mouse skin tumour promotion by several inhibitors of arachidonic acid and metabolism. Carcinogenesis 1982, 3, 1243–1245. [Google Scholar] [CrossRef]
- Moon, R.C.; Kelloff, G.J.; Detrisac, C.J.; Steele, V.E.; Thomas, C.F.; Sigman, C.C. Chemoprevention of OH-BBN-induced bladder cancer in mice by piroxicam. Carcinogenesis 1993, 14, 1487–1489. [Google Scholar] [CrossRef]
- McCormick, D.L.; Medigan, M.J.; Moon, R.C. Modulation of rat mammary carcinogenesis by indomethacin. Cancer Res. 1985, 45, 1803–1805. [Google Scholar] [PubMed]
- Bardia, A.; Olson, J.E.; Vachon, C.M.; Lazovich, A.; Vierkant, R.A.; Wang, A.H.; Limburg, P.J.; Anderson, K.E.; Cerhan, J.R. Effect of Aspirin and other NSAIDs on Postmenopausal Breast Cancer Incidence by Hormone Receptor Status: Results from a Prospective Cohort Study. Breast Cancer Res. Treat. 2011, 126, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.Y.; Chuah, K.L.; Eng, P.; Leong, S.S.; Lim, E.; Lim, T.K.; Ng, A.; Poh, W.T.; Tee, A.; Teh, M.; et al. Aspirin and non-aspirin non-steroidal anti-inflammatory drug use and risk of lung cancer. Lung Cancer 2012, 77, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.B.; Yan, Y.; Guo, Z.F.; Zhang, X.L.; Liu, H.; Geng, J.; Yao, X.D.; Zheng, J.H. Aspirin use and the risk of prostate cancer: A meta-analysis of 24 epidemiologic studies. Int. Urol. Nephrol. 2014, 46, 715–1728. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Nishihara, R.; Wu, K.; Wang, M.; Ogino, S.; Willett, W.C.; Spiegelman, D.; Fuchs, C.S.; Giovannucci, E.L.; Chan, A.T. Population-wide Impact of Long-term Use of Aspirin and the Risk for Cancer. JAMA Oncol. 2016, 2, 762–769. [Google Scholar] [CrossRef]
- Chen, W.Y.; Holmes, M.D. Role of Aspirin in Breast Cancer Survival. Curr. Oncol. Rep. 2017, 19, 48. [Google Scholar] [CrossRef]
- Takiuchi, T.; Blake, E.A.; Matsuo, K.; Sood, A.K.; Brasky, T.M. Aspirin use and endometrial cancer risk and survival. Gynecol. Oncol. 2018, 148, 222–232. [Google Scholar] [CrossRef]
- Gan, H.; Lin, L.; Hu, N.; Yang, Y.; Gao, Y.; Pei, Y.; Chen, K.; Sun, B. Aspirin ameliorates lung cancer by targeting the miR-98/WNT1 axis. Thorac. Cancer 2019, 10, 744–750. [Google Scholar] [CrossRef]
- Loomans-Kropp, H.A.; Pinsky, P.; Cao, Y.; Chan, A.T.; Umar, A. Association of Aspirin Use with Mortality Risk among Older Adult Participants in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. JAMA Netw. Open 2019, 2, e1916729. [Google Scholar] [CrossRef]
- Trabert, B.; Ness, R.B.; Lo-Ciganic, W.H.; Murphy, M.A.; Goode, E.L.; Poole, E.M.; Brinton, L.A.; Webb, P.M.; Nagle, C.M.; Jordan, S.J.; et al. Aspirin, Nonaspirin Nonsteroidal Anti-inflammatory Drug, and Acetaminophen Use and Risk of Invasive Epithelial Ovarian Cancer: A Pooled Analysis in the Ovarian Cancer Association Consortium. J. Natl. Cancer Inst. 2014, 106, djt431. [Google Scholar] [CrossRef]
- Trabert, B.; Poole, E.M.; White, E.; Visvanathan, K.; Adami, H.O.; Anderson, G.L.; Brasky, T.M.; Brinton, L.A.; Fortner, R.T.; Gaudet, M.; et al. Analgesic use and ovarian cancer risk: An analysis in the Ovarian Cancer Cohort Consortium. JNCI J. Natl. Cancer Inst. 2019, 111, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, L.M.; Webb, P.M.; Jordan, S.J.; Doherty, J.A.; Harris, H.R.H.; Goodman, M.T.; Modugno, F.; Moysich, K.B.; Schildkraut, J.M.; Berchuck, A.; et al. Association of Frequent Aspirin Use with Ovarian Cancer Risk According to Genetic Susceptibility. JAMA Netw. Open 2023, 6, e230666. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gąsowska-Bajger, B.; Sosnowska, K.; Gąsowska-Bodnar, A.; Bodnar, L. The Effect of Acetylsalicylic Acid, as a Representative Non-Steroidal Anti-Inflammatory Drug, on the Activity of Myeloperoxidase. Pharmaceuticals 2023, 16, 1012. https://doi.org/10.3390/ph16071012
Gąsowska-Bajger B, Sosnowska K, Gąsowska-Bodnar A, Bodnar L. The Effect of Acetylsalicylic Acid, as a Representative Non-Steroidal Anti-Inflammatory Drug, on the Activity of Myeloperoxidase. Pharmaceuticals. 2023; 16(7):1012. https://doi.org/10.3390/ph16071012
Chicago/Turabian StyleGąsowska-Bajger, Beata, Kinga Sosnowska, Agnieszka Gąsowska-Bodnar, and Lubomir Bodnar. 2023. "The Effect of Acetylsalicylic Acid, as a Representative Non-Steroidal Anti-Inflammatory Drug, on the Activity of Myeloperoxidase" Pharmaceuticals 16, no. 7: 1012. https://doi.org/10.3390/ph16071012
APA StyleGąsowska-Bajger, B., Sosnowska, K., Gąsowska-Bodnar, A., & Bodnar, L. (2023). The Effect of Acetylsalicylic Acid, as a Representative Non-Steroidal Anti-Inflammatory Drug, on the Activity of Myeloperoxidase. Pharmaceuticals, 16(7), 1012. https://doi.org/10.3390/ph16071012