

Probiotics in the Treatment of Radiotherapy-Induced Oral Mucositis: Systematic Review with Meta-Analysis

 ,
,  ,
, 
 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
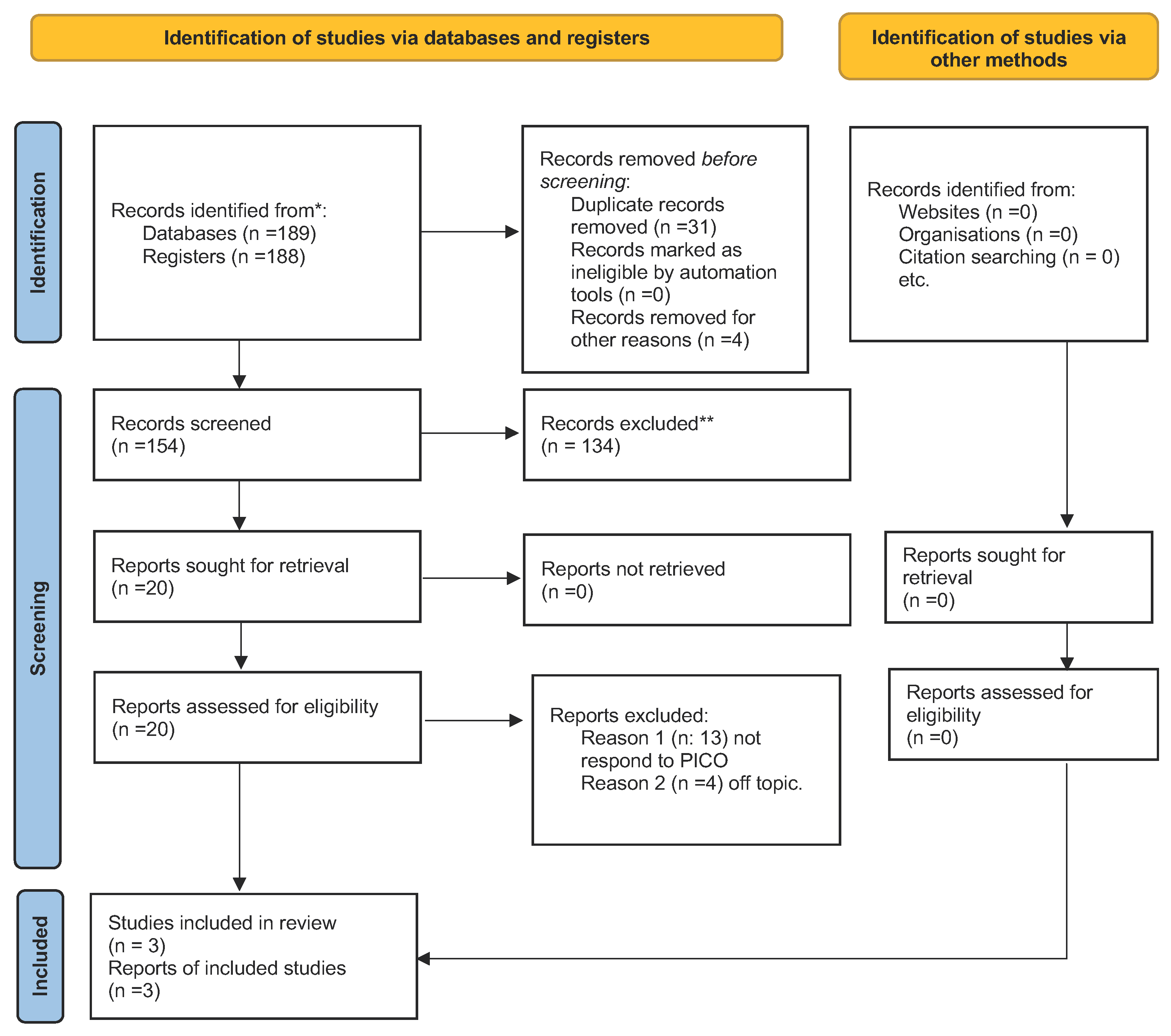
3. Results
3.1. Study Characteristics
3.2. Main Findings
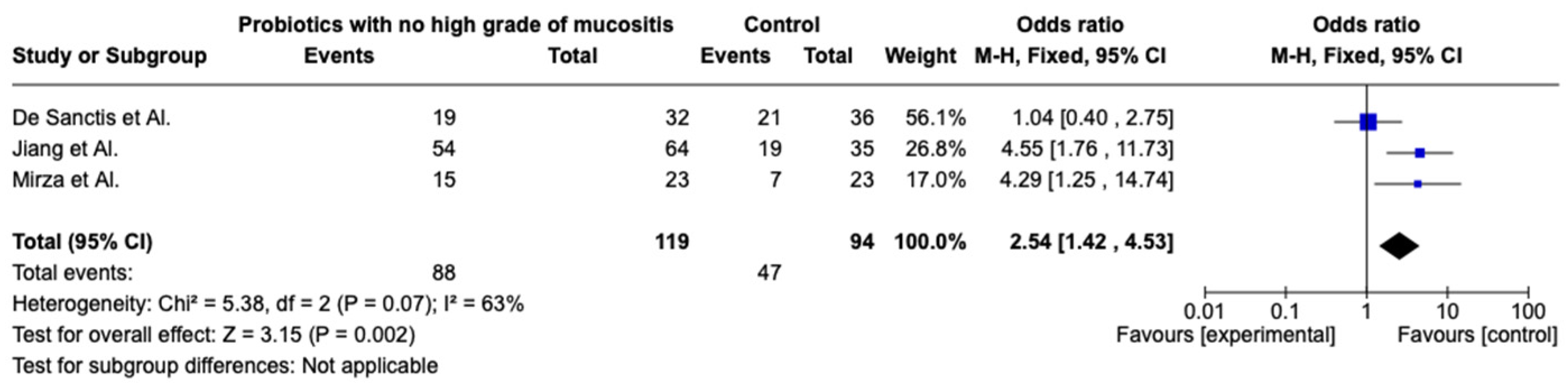
3.3. Metanalysis

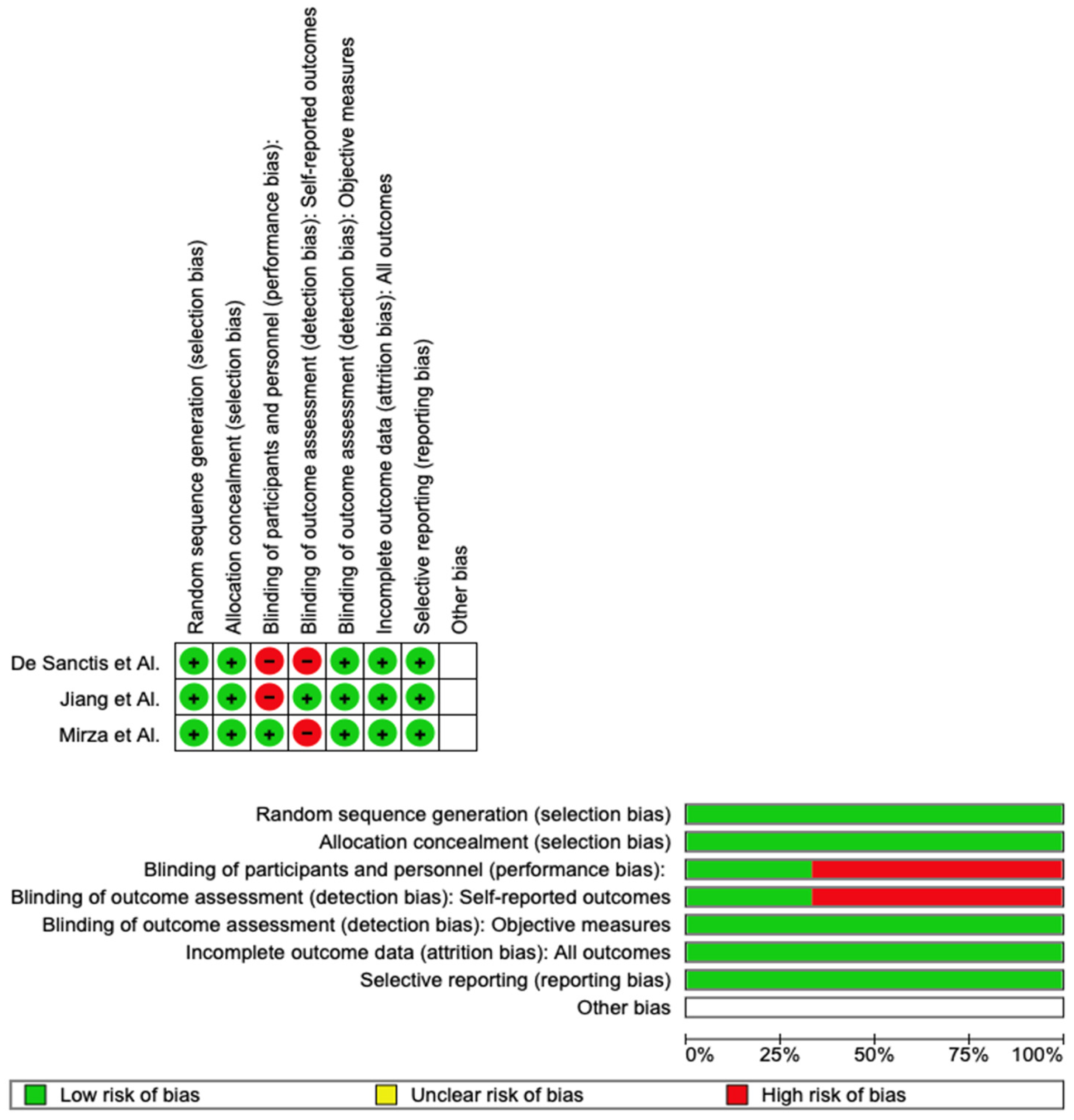
3.4. Quality Assessment and Risk of Bias
4. Discussion
Limitation of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HSCT | hematopoietic cell transplantation |
| IMRT | intensity modulated radiotherapy |
| OM | oral mucositis |
| LB | lactobacillus |
| CCRT | radiotherapy |
| CCRT-p | radiotherapy and probiotics |
| RT | radiotherapy |
| TLR | toll-like receptor |
| LTA | lipoteichoic acid |
| FDA | food and drug administration |
| IND | investigation new drug |
| AHRQ | Agency for Healthcare Research and Quality |
References
- Zhao, R.; Hu, H.; Wang, Y.; Lai, W.; Jian, F. Efficacy of Probiotics as Adjunctive Therapy to Nonsurgical Treatment of Peri-Implant Mucositis: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2021, 11, 541752. [Google Scholar] [CrossRef] [PubMed]
- Maiorana, C.; Beretta, M.; Grossi, G.B.; Santoro, F.; Herford, A.S.; Nagursky, H.; Cicciù, M. Histomorphometric Evaluation of Anorganic Bovine Bone Coverage to Reduce Autogenous Grafts Resorption: Preliminary Results. Open Dent. J. 2011, 5, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Meurman, J.H.; Stamatova, I. Probiotics: Contributions to Oral Health. Oral Dis. 2007, 13, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Gupta, G. Probiotics and Periodontal Health. J. Med. Life 2011, 4, 387–394. [Google Scholar] [PubMed]
- Gungor, O.E.; Kirzioglu, Z.; Kivanc, M. Probiotics: Can They Be Used to Improve Oral Health? Benef. Microbes 2015, 6, 647–656. [Google Scholar] [CrossRef]
- Meurman, J.H.; Stamatova, I.V. Probiotics: Evidence of Oral Health Implications. Folia Med. 2018, 60, 21–29. [Google Scholar] [CrossRef]
- Bonifait, L.; Chandad, F.; Grenier, D. Probiotics for Oral Health: Myth or Reality? J. Can. Dent. Assoc. 2009, 75, 585–590. [Google Scholar]
- Mann, S.; Park, M.S.; Johnston, T.V.; Ji, G.E.; Hwang, K.T.; Ku, S. Isolation, Characterization and Biosafety Evaluation of Lactobacillus Fermentum OK with Potential Oral Probiotic Properties. Probiot. Antimicrob. Proteins 2021, 13, 1363–1386. [Google Scholar] [CrossRef]
- Alqahtani, F.; Alshaikh, M.; Mehmood, A.; Alqhtani, N.; Alkhtani, F.; Alenazi, A. Role of Probiotics for the Treatment of Peri-Implant Mucositis in Patients with and Without Type 2 Diabetes Mellitus. J. Oral Implantol. 2022, 48, 37–42. [Google Scholar] [CrossRef]
- Mehta, V.; Sarode, G.S.; Obulareddy, V.T.; Sharma, T.; Kokane, S.; Cicciù, M.; Minervini, G. Clinicopathologic Profile, Management and Outcome of Sinonasal Ameloblastoma—A Systematic Review. J. Clin. Med. 2023, 12, 381. [Google Scholar] [CrossRef]
- Herford, A.S.; Lu, M.; Akin, L.; Cicciù, M. Evaluation of a Porcine Matrix with and without Platelet-Derived Growth Factor for Bone Graft Coverage in Pigs. Int. J. Oral Maxillofac. Implant. 2012, 27, 1351–1358. [Google Scholar]
- Homayouni Rad, A.; Pourjafar, H.; Mirzakhani, E. A Comprehensive Review of the Application of Probiotics and Postbiotics in Oral Health. Front. Cell Infect. Microbiol. 2023, 13, 1120995. [Google Scholar] [CrossRef] [PubMed]
- Sayardoust, S.; Johansson, A.; Jönsson, D. Do Probiotics Cause a Shift in the Microbiota of Dental Implants—A Systematic Review and Meta-Analysis. Front. Cell Infect. Microbiol. 2022, 12, 823985. [Google Scholar] [CrossRef] [PubMed]
- Temelci, A.; Yılmaz, H.G.; Ünsal, G.; Uyanik, L.O.; Yazman, D.; Ayali, A.; Minervini, G. Investigation of the Wetting Properties of Thalassemia Patients’ Blood Samples on Grade 5 Titanium Implant Surfaces: A Pilot Study. Biomimetics 2023, 8, 25. [Google Scholar] [CrossRef] [PubMed]
- Gugnacki, P.; Sierko, E. Is There an Interplay between Oral Microbiome, Head and Neck Carcinoma and Radiation-Induced Oral Mucositis? Cancers 2021, 13, 5902. [Google Scholar] [CrossRef]
- Nguyen, T.; Brody, H.; Radaic, A.; Kapila, Y. Probiotics for Periodontal Health-Current Molecular Findings. Periodontol. 2000 2021, 87, 254–267. [Google Scholar] [CrossRef]
- Cicciù, M.; Herford, A.S.; Stoffella, E.; Cervino, G.; Cicciù, D. Protein-Signaled Guided Bone Regeneration Using Titanium Mesh and Rh-BMP2 in Oral Surgery: A Case Report Involving Left Mandibular Reconstruction after Tumor Resection. Open Dent. J. 2012, 6, 51–55. [Google Scholar] [CrossRef]
- Shu, Z.; Li, P.; Yu, B.; Huang, S.; Chen, Y. The effectiveness of probiotics in prevention and treatment of cancer therapy-induced oral mucositis: A systematic review and meta-analysis. Oral Oncol. 2020, 102, 104559. [Google Scholar] [CrossRef]
- Das, M. Probiotics for chemoradiotherapy-induced oral mucositis. Lancet Oncol. 2019, 20, e14. [Google Scholar] [CrossRef]
- Contaldo, M.; Di Stasio, D.; Romano, A.; Fiori, F.; Vella, F.D.; Rupe, C.; Lajolo, C.; Petruzzi, M.; Serpico, R.; Lucchese, A. Oral candidiasis and novel therapeutic strategies: Antifungals, phytotherapy, probiotics, and photodynamic therapy. Curr. Drug Deliv. 2022, 20, 441–456. [Google Scholar] [CrossRef]
- Cheng, B.; Zeng, X.; Liu, S.; Zou, J.; Wang, Y. The efficacy of probiotics in management of recurrent aphthous stomatitis: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 21181. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-C.; Wu, C.-R.; Huang, T.-W. Preventive Effect of Probiotics on Oral Mucositis Induced by Cancer Treatment: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2022, 23, 13268. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Caraccia, M.; Caccialanza, R. Probiotics and mucositis. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 399–404. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Wang, H.; Xia, C.; Dong, Q.; Chen, E.; Qiu, Y.; Su, Y.; Xie, H.; Zeng, L.; Kuang, J.; et al. A randomized, double-blind, placebo-controlled trial of probiotics to reduce the severity of oral mucositis induced by chemoradiotherapy for patients with nasopharyngeal carcinoma. Cancer 2019, 125, 1081–1090. [Google Scholar] [CrossRef]
- De Sanctis, V.; Belgioia, L.; Cante, D.; La Porta, M.R.; Caspiani, O.; Guarnaccia, R.; Argenone, A.; Muto, P.; Musio, D.; De Felice, F.; et al. Lactobacillus brevis CD2 for Prevention of Oral Mucositis in Patients with Head and Neck Tumors: A Multicentric Randomized Study. Anticancer Res. 2019, 39, 1935–1942. [Google Scholar] [CrossRef]
- Mirza, M.A.; Aruna, D.; Irukulla, M. Efficacy of Bacillus clausii UBBC-07 spores in the amelioration of oral mucositis in head and neck cancer patients undergoing radiation therapy. Cancer Treat. Res. Commun. 2022, 31, 100523. [Google Scholar] [CrossRef]
- Gupta, N.; Ferreira, J.; Hong, C.H.L.; Tan, K.S. Lactobacillus reuteri DSM 17938 and ATCC PTA 5289 ameliorates chemotherapy-induced oral mucositis. Sci. Rep. 2020, 10, 16189. [Google Scholar] [CrossRef]
- Maria-Aggeliki, K.; Nikolaos, K.; George, K.; Vassilis, K.; Kyrias, G. The Potential Clinical Impact of Probiotic Treatment for the Prevention and/or Anti-Inflammatory Therapeutic Effect Against Radiation Induced Intestinal Mucositis. A Review. Recent Pat. Inflamm. Allergy Drug Discov. 2009, 3, 195–200. [Google Scholar] [CrossRef]
- Lu, Y.; Luo, X.; Yang, D.; Li, Y.; Gong, T.; Wang, J.; Li, B.; Cheng, J.; Chen, R.; Guo, X.; et al. Effects of probiotic supplementation on related side effects after chemoradiotherapy in cancer patients. Front. Oncol. 2022, 12, 5962. [Google Scholar] [CrossRef]
- Araujo, L.D.C.; Furlaneto, F.A.C.; da Silva, L.A.B.; Kapila, Y.L. Use of the Probiotic Bifidobacterium animalis subsp. lactis HN019 in Oral Diseases. Int. J. Mol. Sci. 2022, 23, 9334. [Google Scholar] [PubMed]
- Yeung, C.Y.; Chan, W.T.; Jiang, C.B.; Cheng, M.L.; Liu, C.Y.; Chang, S.W.; Chiang Chiau, J.S.; Lee, H.C. Amelioration of Chemotherapy-Induced Intestinal Mucositis by Orally Administered Probiotics in a Mouse Model. PLoS ONE 2015, 10, e0138746. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Chiau, J.S.C.; Cheng, M.L.; Chan, W.T.; Jiang, C.B.; Chang, S.W.; Yeung, C.Y.; Lee, H.C. SCID/NOD mice model for 5-FU induced intestinal mucositis: Safety and effects of probiotics as therapy. Pediatr. Neonatol. 2019, 60, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Cappello, F.; Rappa, F.; Canepa, F.; Carini, F.; Mazzola, M.; Tomasello, G.; Bonaventura, G.; Giuliana, G.; Leone, A.; Saguto, D.; et al. Probiotics Can Cure Oral Aphthous-Like Ulcers in Inflammatory Bowel Disease Patients: A Review of the Literature and a Working Hypothesis. Int. J. Mol. Sci. 2019, 20, 5026. [Google Scholar] [CrossRef]
- Prisciandaro, L.D.; Geier, M.S.; Butler, R.N.; Cummins, A.G.; Howarth, G.S. Evidence Supporting the use of Probiotics for the Prevention and Treatment of Chemotherapy-Induced Intestinal Mucositis. Crit. Rev. Food Sci. Nutr. 2011, 51, 239–247. [Google Scholar] [CrossRef]
- Jayaraj, R.; Kumaraswamy, C.; Shetty, S.; Raymond, G.; Govind, S.K.; Chandramoorthy, H.C.; Shaw, P. Clinical approaches to interpreting the findings of systematic review and meta-analysis of the effectiveness of probiotics in the prevention and treatment of Cancer Therapy-Induced Oral Mucositis (CTIOM). Oral Oncol. 2020, 104, 104622. [Google Scholar] [CrossRef]
- Li, D.; Li, Q.; Liu, C.; Lin, M.; Li, X.; Xiao, X.; Zhu, Z.; Gong, Q.; Zhou, H. Efficacy and safety of probiotics in the treatment of Candida-associated stomatitis. Mycoses 2014, 57, 141–146. [Google Scholar] [CrossRef]
- Sangild, P.T.; Shen, R.L.; Pontoppidan, P.; Rathe, M. Animal models of chemotherapy-induced mucositis: Translational relevance and challenges. Am. J. Physiol. Gastrointest. Liver Physiol. 2018, 314, G231–G246. [Google Scholar] [CrossRef]
- Ozen, M.; Dinleyici, E.C. The history of probiotics: The untold story. Benef. Microbes 2015, 6, 159–165. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| PubMed (“probiotics”) AND (“oral mucositis”) |
| Web of Science ((ALL = (probiotics)) AND ((ALL = (oral mucositis)) |
| Lilacs “probiotics” (palavras) AND “oral mucositis” (palavras) |
| Author | Year | Sample | Type of Therapy | Criteria | Results of Therapy |
|---|---|---|---|---|---|
| Jiang et al. [25] | 2018 | 99 Patients: 64 probiotic 35 placebo | Cisplatinum plus radiotherapy 70 Gy | National Cancer Institute’s Common Terminology Criteria for Adverse Events | Reduces the severity of OM through changes in the gut microbiome |
| De Sanctis et al. [26] | 2019 | 68 Patients: 32 probiotic 36 placebo | Cisplatinum plus radiotherapy 68 Gy | National Cancer Institute’s Common Terminology Criteria for Adverse Events | No difference between the two groups |
| Mirza et al. [27] | 2022 | 46 Patients: 23 probiotic 23 placebo | Radiotherapy with or no chemotherapy 60–70 Gy | National Cancer Institute’s Common Terminology Criteria for Adverse Events | Reduces the severity of OM |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minervini, G.; Franco, R.; Marrapodi, M.M.; Fiorillo, L.; Badnjević, A.; Cervino, G.; Cicciù, M. Probiotics in the Treatment of Radiotherapy-Induced Oral Mucositis: Systematic Review with Meta-Analysis. Pharmaceuticals 2023, 16, 654. https://doi.org/10.3390/ph16050654
Minervini G, Franco R, Marrapodi MM, Fiorillo L, Badnjević A, Cervino G, Cicciù M. Probiotics in the Treatment of Radiotherapy-Induced Oral Mucositis: Systematic Review with Meta-Analysis. Pharmaceuticals. 2023; 16(5):654. https://doi.org/10.3390/ph16050654
Chicago/Turabian StyleMinervini, Giuseppe, Rocco Franco, Maria Maddalena Marrapodi, Luca Fiorillo, Almir Badnjević, Gabriele Cervino, and Marco Cicciù. 2023. "Probiotics in the Treatment of Radiotherapy-Induced Oral Mucositis: Systematic Review with Meta-Analysis" Pharmaceuticals 16, no. 5: 654. https://doi.org/10.3390/ph16050654
APA StyleMinervini, G., Franco, R., Marrapodi, M. M., Fiorillo, L., Badnjević, A., Cervino, G., & Cicciù, M. (2023). Probiotics in the Treatment of Radiotherapy-Induced Oral Mucositis: Systematic Review with Meta-Analysis. Pharmaceuticals, 16(5), 654. https://doi.org/10.3390/ph16050654