


Efficacy of Topical Essential Oils in Musculoskeletal Disorders: Systematic Review and Meta-Analysis of Randomized Controlled Trials
 ,
,  , , ,
, , , 
 and
and
Abstract
1. Introduction
2. Results
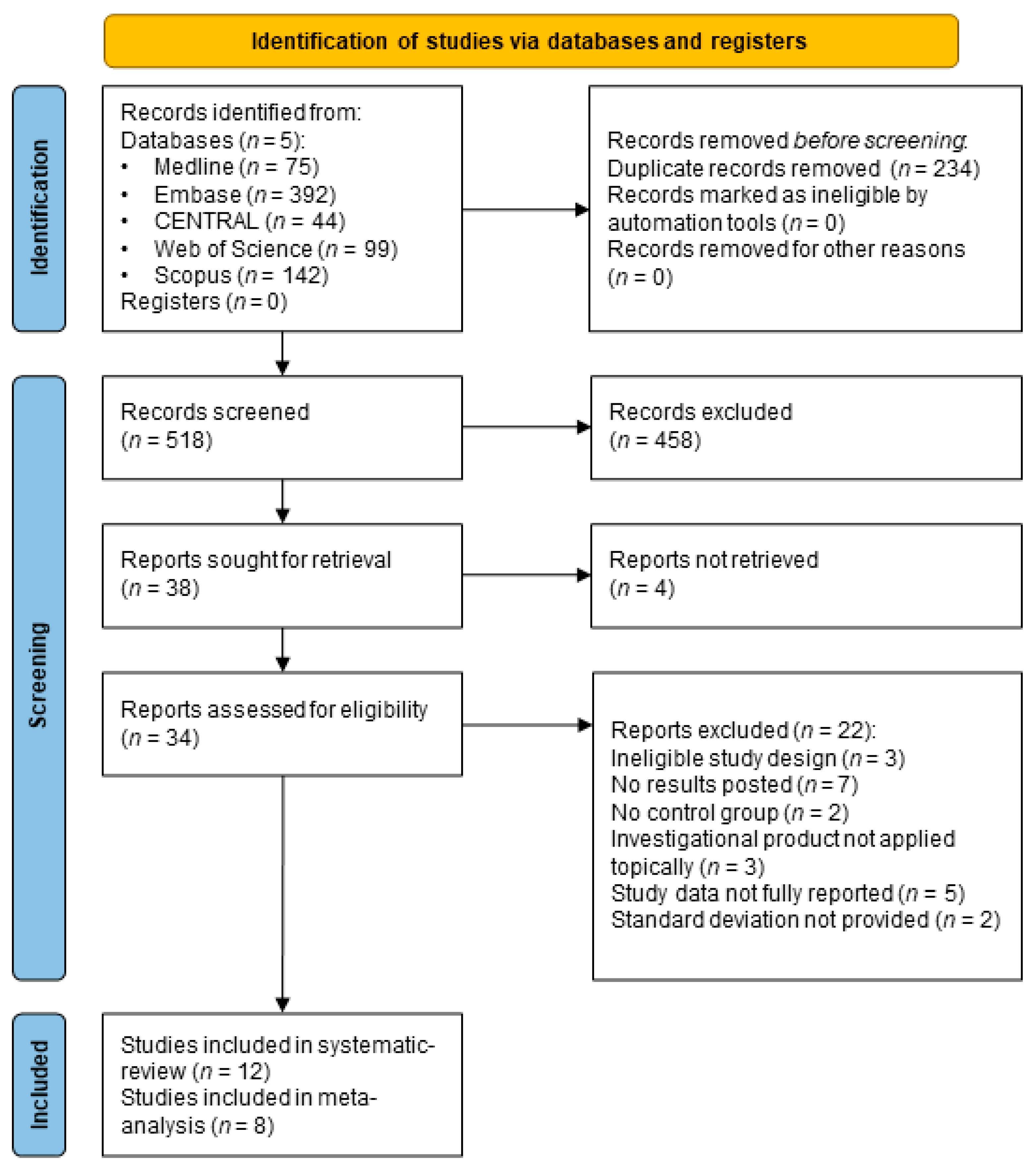
2.1. Search and Selection
2.2. Basic Characteristics of Included Studies
2.3. Qualitative Synthesis of Results
2.4. Quantitative Synthesis of Results
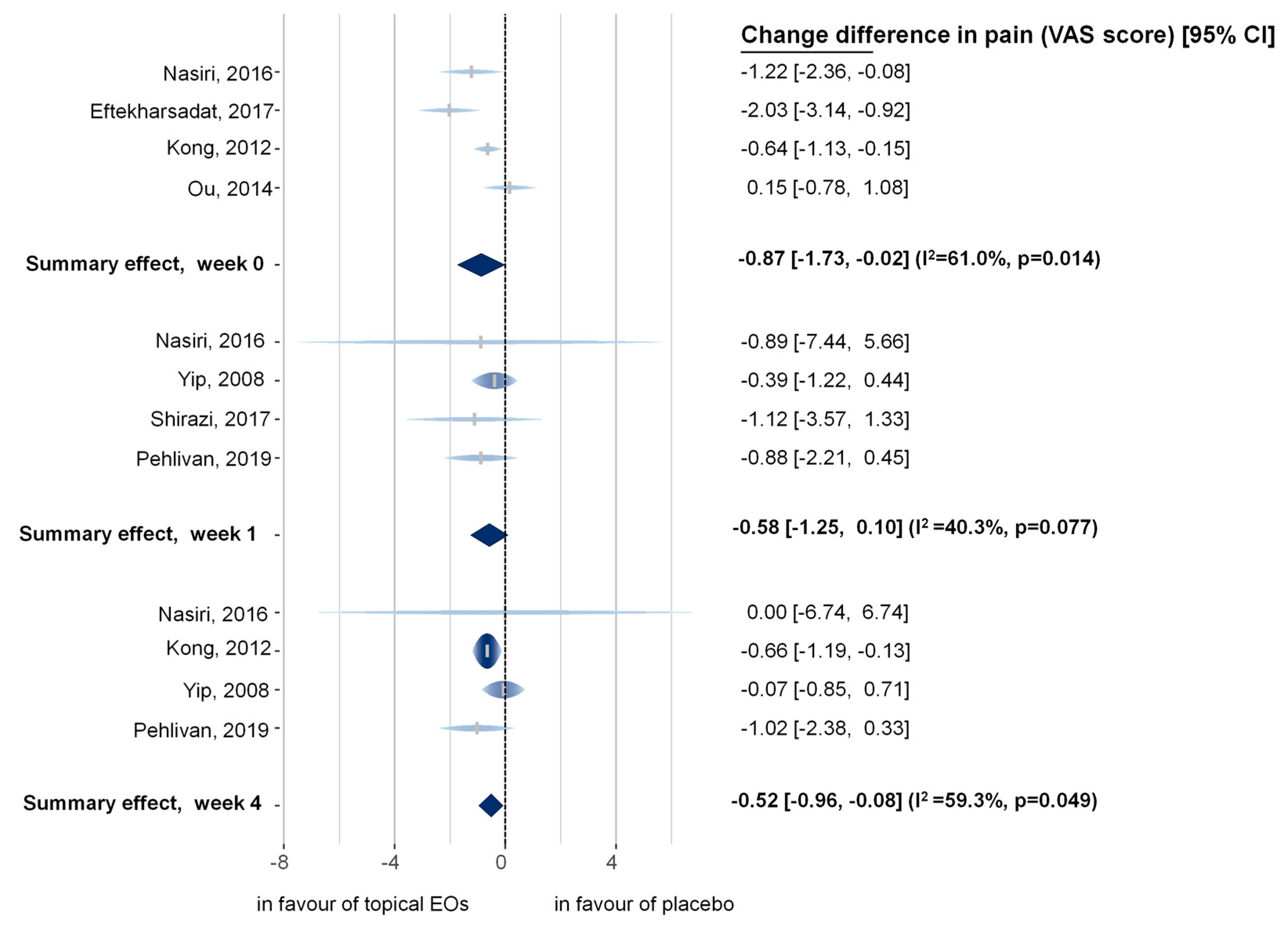
2.4.1. Primary Outcome
Pain Intensity Measured Immediately after the Intervention (Subgroup Analysis)
Pain Intensity Measured One Week after the Intervention (Subgroup Analysis)
Pain Intensity Measured Four Weeks after the Intervention (Subgroup Analysis)
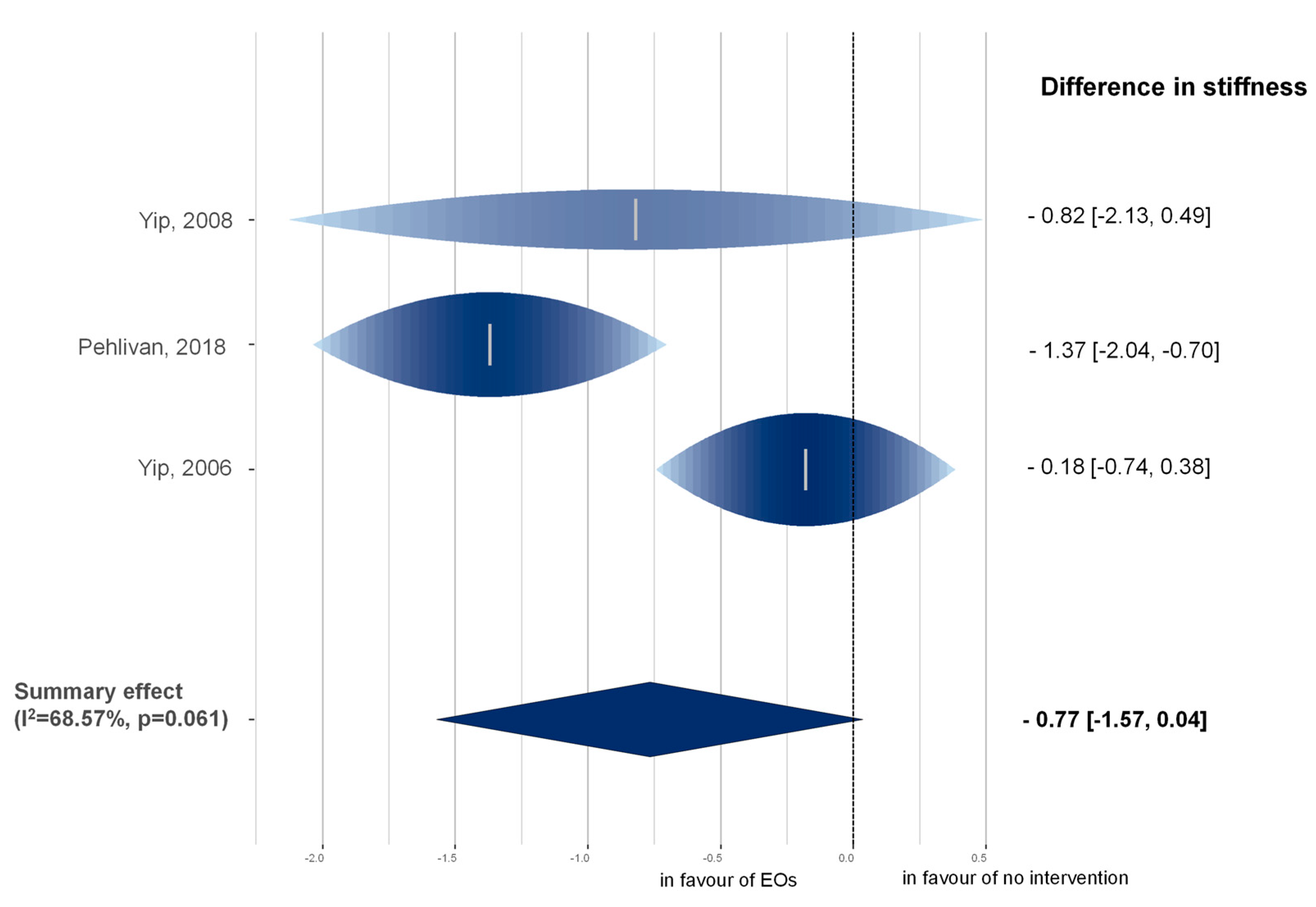
2.4.2. Secondary Outcomes
Stiffness
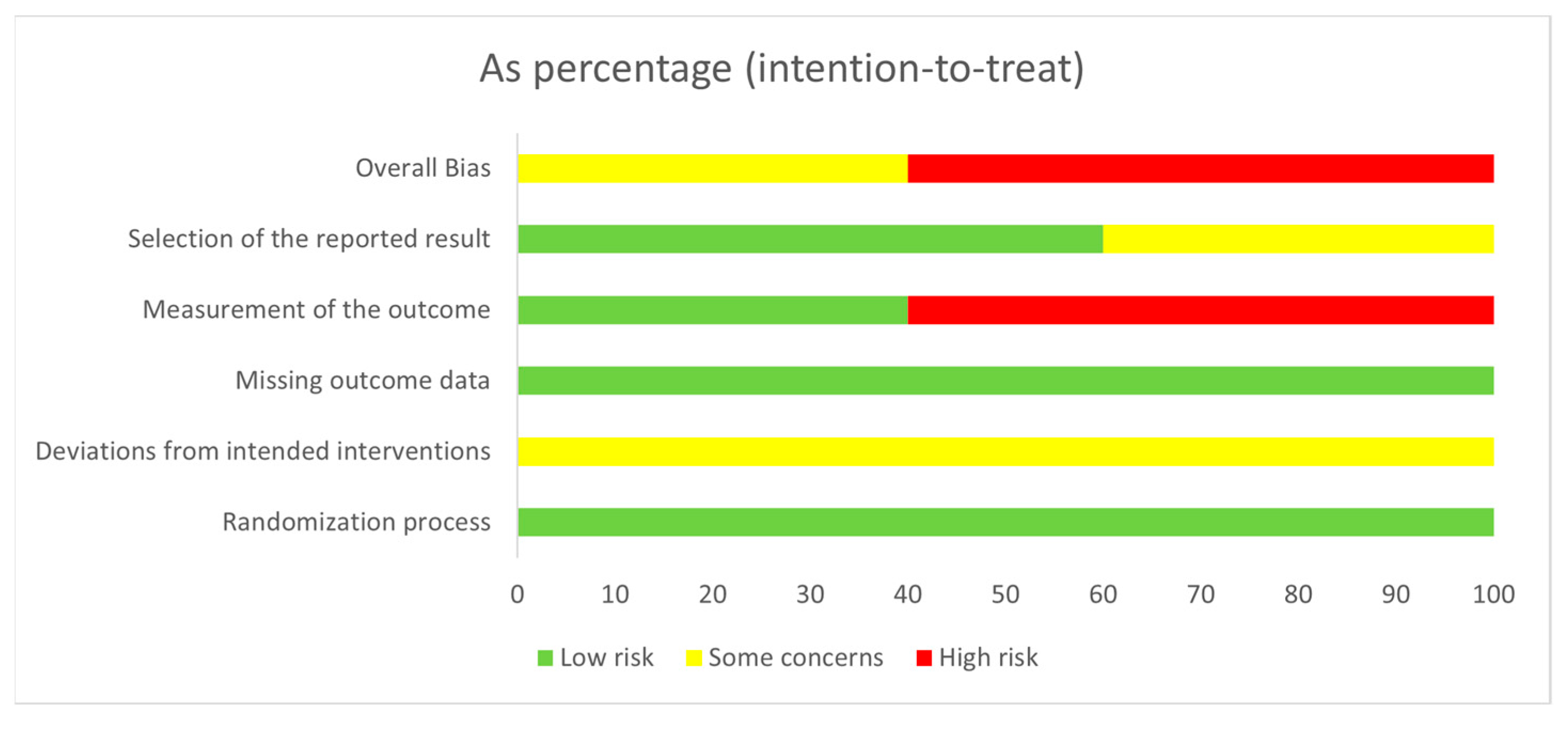
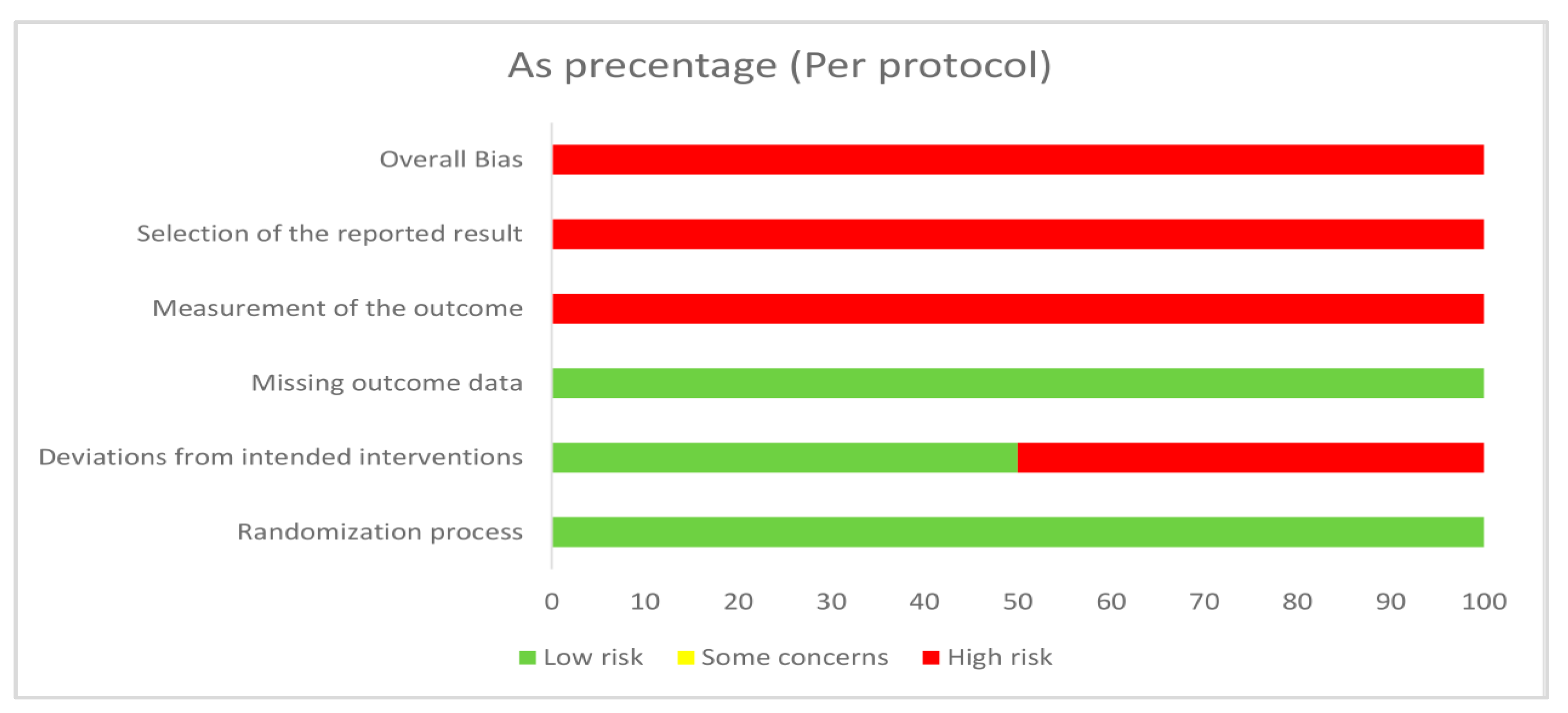
2.5. Risk of Bias Assessment and GRADE Assessment
2.6. Publication Bias
3. Discussion
3.1. Strengths and Limitation
3.2. Implication for Practice and Research
3.3. Recommendation for Future Trials Investigating the Effect of Topical EO on MSDs
4. Methods
4.1. Objectives and Protocol
4.2. Information Sources and Search Strategy
4.3. Participants, Interventions, Comparisons and Outcomes (PICO)
4.4. Eligibility Criteria
4.5. Exclusion Criteria
4.6. Selection Process
4.7. Data Collection Process
4.8. Deviation from Protocol
4.9. Study Risk of Bias Assessment
4.10. Quality of Evidence
4.11. Synthesis Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| English Name of/Local Chinese Name, If Applicable | Plant Name (Family) | Discussion of Potential Analgesic Effect of EO |
|---|---|---|
| Lavender | Lavandula angustifolia Mill. and Lavandula stoechas L. (Lamiaceae) | Antinociceptive effect of lavender EO have been described in the literature [57,58]. |
| Peppermint | Mentha × piperita L. (Lamiaceae) | Topical application of peppermint oil produces a prolonged cold sensation [59] by the stimulation of the TRPM8 cold-sensitive receptors, giving an analgesic effect [60]. |
| Cinnamomum | Cinnamomum verum J.Presl (Lauraceae) | Eugenol and cinnamaldehyde, main components of cinnamon bark EO, have analgesic-like activity [16,61]. |
| Chuanxiong Rhizoma/Chuan-xiong | Ligusticum chuanxiong S.H.Qiu, Y.Q.Zeng, K.Y.Pan, Y.C.Tang & J.M.Xu (Apiaceae) | Potential analgesic effect is based on traditional use (Traditional Chinese medicine). |
| Chinese angelica/Dang Gui | Angelica sinensis var. wilsonii (H.Wolff) Z.H.Pan & M.F.Watson (Apiaceae) | Potential analgesic effect is based on traditional use (Traditional Chinese medicine). |
| Chinese wild ginger/Xi Xin | Asarum heterotropoides F. Schmidt (Aristolochiaceae) | Potential analgesic effect is based on traditional use (Traditional Chinese medicine). |
| Rose | Rosa × damascena Herrm. (Rosaceae) | The main components of rose EO are citronellol, geraniol, and nerol [61]. Citronellol and nerol have analgesic-like activity based on animal models or human trials [16]. |
| Rosemary | Rosmarinus officinalis L. (Lamiaceae) | According to Ph. Eur., rosemary oil (Spanish type) contains 1,8-cineole, camphor, α-pinene and camphene as main components. 1,8-cineole has analgesic-like activity on the basis of animal models [62]. |
| Marjoram | Origanum majorana L. (Lamiaceae) | α-Terpineol of marjoram and β-caryophyllene, β-pinene, D-limonene of black pepper EO have analgesic-like activity based on animal models or human trials [16,62,63,64,65]. |
| Black pepper | Piper nigrum L. (Piperaceae) | α-Terpineol of marjoram and β-caryophyllene, β-pinene, D-limonene of black pepper EO have analgesic-like activity based on animal models or human trials [16,62,63,64,65] |
| Ginger | Zingiber officinale Roscoe (Zingiberaceae) | Ginger has pain lowering effect caused via different pathways [66]. |
| Orange | Citrus × aurantium L. (Rutaceae) | Orange EO was added to ginger to give a more pleasant odor of the investigational product in the trial of [29]. |
| Juniper | Juniperus communis L. (Cupressaceae) | According to the EMA monograph, topical juniper EO has pain-relieving effect in minor muscular and articular pain. |
| Ylang-ylang | Cananga odorata (Lam.) Hook.f. & Thomson (Annonaceae) | Ylang-ylang essential oil reduces pain and inflammation in animal study [67]. |
References
- Musculoskeletal Health by World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (accessed on 21 October 2022).
- Loveless, M.S.; Fry, A.L. Pharmacologic Therapies in Musculoskeletal Conditions. Med. Clin. N. Am. 2016, 100, 869–890. [Google Scholar] [CrossRef]
- Bindu, S.; Mazumder, S.; Bandyopadhyay, U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochem. Pharmacol. 2020, 180, 114147. [Google Scholar] [CrossRef] [PubMed]
- Morrone, L.A.; Scuteri, D.; Rombola, L.; Mizoguchi, H.; Bagetta, G. Opioids Resistance in Chronic Pain Management. Curr. Neuropharmacol. 2017, 15, 444–456. [Google Scholar] [CrossRef] [PubMed]
- Orchard, A.; van Vuuren, S.F. Carrier oils in dermatology. Arch. Dermatol. Res. 2019, 311, 653–672. [Google Scholar] [CrossRef]
- Moghaddam, M.; Mehdizadeh, L. Chapter 13—Chemistry of Essential Oils and Factors Influencing Their Constituents. In Soft Chemistry and Food Fermentation; Grumezescu, A.M., Holban, A.M., Eds.; Academic Press: Cambridge, MA, USA, 2017; pp. 379–419. [Google Scholar]
- Ni, Z.J.; Wang, X.; Shen, Y.; Thakur, K.; Han, J.Z.; Zhang, J.G.; Hu, F.; Wei, Z.J. Recent updates on the chemistry, bioactivities, mode of action, and industrial applications of plant essential oils. Trends Food Sci. Technol. 2021, 110, 78–89. [Google Scholar] [CrossRef]
- Buckle, J. Aromatherapy for health professionals. Beginnings (American Holistic Nurses’ Association) 2003, 23, 6–7. [Google Scholar]
- Nguyen, T.H.D.; Itoh, S.G.; Okumura, H.; Tominaga, M. Structural basis for promiscuous action of monoterpenes on TRP channels. Commun. Biol. 2021, 4, 293. [Google Scholar] [CrossRef]
- Cavanagh, H.M.; Wilkinson, J.M. Biological activities of lavender essential oil. Phytother. Res. PTR 2002, 16, 301–308. [Google Scholar] [CrossRef]
- Mahendran, G.; Rahman, L.U. Ethnomedicinal, phytochemical and pharmacological updates on Peppermint (Mentha × piperita L.)-A review. Phytother. Res. PTR 2020, 34, 2088–2139. [Google Scholar] [CrossRef]
- Ribeiro-Santos, R.; Carvalho-Costa, D.; Cavaleiro, C.; Costa, H.S.; Albuquerque, T.G.; Castilho, M.C.; Ramos, F.; Melo, N.R.; Sanches-Silva, A. A novel insight on an ancient aromatic plant: The rosemary (Rosmarinus officinalis L.). Trends Food Sci. Technol. 2015, 45, 355–368. [Google Scholar] [CrossRef]
- Silva, J.; Abebe, W.; Sousa, S.M.; Duarte, V.G.; Machado, M.I.; Matos, F.J. Analgesic and anti-inflammatory effects of essential oils of Eucalyptus. J. Ethnopharmacol. 2003, 89, 277–283. [Google Scholar] [CrossRef]
- Srivastava, J.K.; Shankar, E.; Gupta, S. Chamomile: A herbal medicine of the past with bright future. Mol. Med. Rep. 2010, 3, 895–901. [Google Scholar] [CrossRef]
- Assis, D.B.; Aragao Neto, H.C.; da Fonseca, D.V.; de Andrade, H.H.N.; Braga, R.M.; Badr, N.; Maia, M.D.S.; Castro, R.D.; Scotti, L.; Scotti, M.T.; et al. Antinociceptive Activity of Chemical Components of Essential Oils That Involves Docking Studies: A Review. Front. Pharmacol. 2020, 11, 777. [Google Scholar] [CrossRef]
- de Cassia da Silveira, E.S.R.; Lima, T.C.; da Nobrega, F.R.; de Brito, A.E.M.; de Sousa, D.P. Analgesic-Like Activity of Essential Oil Constituents: An Update. Int. J. Mol. Sci. 2017, 18, 2392. [Google Scholar] [CrossRef]
- Ilari, S.; Proietti, S.; Russo, P.; Malafoglia, V.; Gliozzi, M.; Maiuolo, J.; Oppedisano, F.; Palma, E.; Tomino, C.; Fini, M.; et al. A Systematic Review and Meta-Analysis on the Role of Nutraceuticals in the Management of Neuropathic Pain in In Vivo Studies. Antioxidants 2022, 11, 2361. [Google Scholar] [CrossRef]
- Lenardao, E.; Savegnago, L.; Jacob, R.; Victoria, F.; Martins, D. Antinociceptive Effect of Essential Oils and Their Constituents: An Update Review. J. Braz. Chem. Soc. 2015, 27, 435–474. [Google Scholar] [CrossRef]
- Scuteri, D.; Hamamura, K.; Sakurada, T.; Watanabe, C.; Sakurada, S.; Morrone, L.A.; Rombola, L.; Tonin, P.; Bagetta, G.; Corasaniti, M.T. Efficacy of Essential Oils in Pain: A Systematic Review and Meta-Analysis of Preclinical Evidence. Front. Pharmacol. 2021, 12, 640128. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br. Med. J. 2021, 372, n71. [Google Scholar] [CrossRef]
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook (accessed on 21 October 2022).
- National Institute for Health Research. International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=282201 (accessed on 21 October 2022).
- Shirazi, M.; Mohebitabar, S.; Bioos, S.; Yekaninejad, M.S.; Rahimi, R.; Shahpiri, Z.; Malekshahi, F.; Nejatbakhsh, F. The Effect of Topical Rosa damascena (Rose) Oil on Pregnancy-Related Low Back Pain: A Randomized Controlled Clinical Trial. J. Evid. Based Complement. Altern. Med. 2017, 22, 120–126. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. Br. Med. J. 2019, 366, l4898. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schunemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- GRADEpro GDT Software. Available online: http://www.gradepro.org/ (accessed on 21 October 2022).
- Konstantopoulos, S. Fixed effects and variance components estimation in three-level meta-analysis. Res. Synth. Methods 2011, 2, 61–76. [Google Scholar] [CrossRef]
- Trikalinos, T.A.; Olkin, I. Meta-analysis of effect sizes reported at multiple time points: A multivariate approach. Clin. Trials 2012, 9, 610–620. [Google Scholar] [CrossRef] [PubMed]
- Hovelstad, H.; Leirset, I.; Oyaas, K.; Fiksdahl, A. Screening analyses of pinosylvin stilbenes, resin acids and lignans in Norwegian conifers. Molecules 2006, 11, 103–114. [Google Scholar] [CrossRef]
- Ayache, S.; Strangi, A.; Chakali, G.; Dahmani, L.; Chellali, M.; Pennacchio, F.; Roversi, P.F.; Binazzi, F. A new species, Cinara tellenica Binazzi F. et Strangi (Aphididae Lachninae) associated with Cedrus atlantica in the Tell Atlas of Algeria. Bull. Insectology 2020, 73, 275–283. [Google Scholar]
- Jackson, D.; White, I.R.; Riley, R.D. Quantifying the impact of between-study heterogeneity in multivariate meta-analyses. Stat. Med. 2012, 31, 3805–3820. [Google Scholar] [CrossRef]
- Zhang, Z.; Kossmeier, M.; Tran, U.S.; Voracek, M.; Zhang, H. Rainforest plots for the presentation of patient-subgroup analysis in clinical trials. Ann. Transl. Med. 2017, 5, 485. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2012. [Google Scholar]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.A.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rucker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-on Guide; Chapman and Hall/CRC: Boca Raton, FL, USA, 2021. [Google Scholar]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Kossmeier, M.; Tran, U.S.; Voracek, M.J.R.P.V. Visualizing meta-analytic data with R package metaviz. R Package Version 2020, 3, 1. [Google Scholar]
- Bahr, T.; Allred, K.; Martinez, D.; Rodriguez, D.; Winterton, P. Effects of a massage-like essential oil application procedure using Copaiba and Deep Blue oils in individuals with hand arthritis. Complement. Ther. Clin. Pract. 2018, 33, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Eftekharsadat, B.; Roomizadeh, P.; Torabi, S.; Heshmati-Afshar, F.; Jahanjoo, F.; Babaei-Ghazani, A. Effectiveness of Lavendula stoechas essential oil in treatment of mild to moderate carpal tunnel syndrome: A randomized controlled trial. J. Hand Ther. Off. J. Am. Soc. Hand Ther. 2018, 31, 437–442. [Google Scholar] [CrossRef]
- El Sayed, E.M.; Al Sebaee, H.A.; Mohammed, H.A.; Nawito, Z.O. Effect of lavender oil massage on pain among patients with knee osteoarthritis. Indian J. Public Health Res. Dev. 2020, 11, 304–309. [Google Scholar] [CrossRef]
- Gok Metin, Z.; Ozdemir, L. The Effects of Aromatherapy Massage and Reflexology on Pain and Fatigue in Patients with Rheumatoid Arthritis: A Randomized Controlled Trial. Pain Manag. Nurs. Off. J. Am. Soc. Pain Manag. Nurses 2016, 17, 140–149. [Google Scholar] [CrossRef]
- Kong, L.J.; Fang, M.; Zhan, H.S.; Yuan, W.A.; Tao, J.M.; Qi, G.W.; Cheng, Y.W. Chinese massage combined with herbal ointment for athletes with nonspecific low back pain: A randomized controlled trial. J. Evid. Based Complement. Altern. Med. 2012, 2012, 695726. [Google Scholar] [CrossRef]
- Nasiri, A.; Mahmodi, M.A.; Nobakht, Z. Effect of aromatherapy massage with lavender essential oil on pain in patients with osteoarthritis of the knee: A randomized controlled clinical trial. Complement. Ther. Clin. Pract. 2016, 25, 75–80. [Google Scholar] [CrossRef]
- Ou, M.C.; Lee, Y.F.; Li, C.C.; Wu, S.K. The Effectiveness of Essential Oils for Patients with Neck Pain: A Randomized Controlled Study. J. Altern. Complement. Med. 2014, 20, 771–779. [Google Scholar] [CrossRef]
- Pehlivan, S.; Karadakovan, A. Effects of aromatherapy massage on pain, functional state, and quality of life in an elderly individual with knee osteoarthritis. Jpn. J. Nurs. Sci. JJNS 2019, 16, 450–458. [Google Scholar] [CrossRef]
- Yip, Y.B.; Tam, A.C. An experimental study on the effectiveness of massage with aromatic ginger and orange essential oil for moderate-to-severe knee pain among the elderly in Hong Kong. Complement. Ther. Med. 2008, 16, 131–138. [Google Scholar] [CrossRef]
- Yip, Y.B.; Tse, S.H. The effectiveness of relaxation acupoint stimulation and acupressure with aromatic lavender essential oil for non-specific low back pain in Hong Kong: A randomised controlled trial. Complement. Ther. Med. 2004, 12, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Yip, Y.B.; Tse, S.H.M. An experimental study on the effectiveness of acupressure with aromatic lavender essential oil for sub-acute, non-specific neck pain in Hong Kong. Complement. Ther. Clin. Pract. 2006, 12, 18–26. [Google Scholar] [CrossRef]
- Lakhan, S.E.; Sheafer, H.; Tepper, D. The Effectiveness of Aromatherapy in Reducing Pain: A Systematic Review and Meta-Analysis. Pain Res. Treat. 2016, 2016, 8158693. [Google Scholar] [CrossRef]
- Bervoets, D.C.; Luijsterburg, P.A.; Alessie, J.J.; Buijs, M.J.; Verhagen, A.P. Massage therapy has short-term benefits for people with common musculoskeletal disorders compared to no treatment: A systematic review. J. Physiother. 2015, 61, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Bhoi, D.; Jain, D.; Garg, R.; Iyengar, K.P.; Hoda, W.; Vaishya, R.; Jain, V.K. Complementary and Alternative Modalities (CAM) for pain management in musculoskeletal diseases (MSDs). J. Clin. Orthop. Trauma 2021, 18, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Fuller, H.R.; Humphrey, E.L.; Morris, G.E. Naturally occurring plant polyphenols as potential therapies for inherited neuromuscular diseases. Future Med. Chem. 2013, 5, 2091–2101. [Google Scholar] [CrossRef] [PubMed]
- Mishra, G.; Singh, P.; Molla, M.; Shumet Yimer, Y.; Ewunetie, A.; Yimer Tadesse, T.; Mengie Ayele, T.; Kefale, B. Nutraceuticals: A source of benefaction for neuropathic pain and fibromyalgia. J. Funct. Foods 2022, 97, 105260. [Google Scholar] [CrossRef]
- Ragozzino, E.; Brancaccio, M.; Di Costanzo, A.; Scalabri, F.; Andolfi, G.; Wanderlingh, L.G.; Patriarca, E.J.; Minchiotti, G.; Altamura, S.; Summa, V.; et al. 6-Bromoindirubin-3′-oxime intercepts GSK3 signaling to promote and enhance skeletal muscle differentiation affecting miR-206 expression in mice. Sci. Rep. 2019, 9, 18091. [Google Scholar] [CrossRef]
- Shirakawa, T.; Miyawaki, A.; Kawamoto, T.; Kokabu, S. Natural Compounds Attenuate Denervation-Induced Skeletal Muscle Atrophy. Int. J. Mol. Sci. 2021, 22, 8310. [Google Scholar] [CrossRef]
- Barocelli, E.; Calcina, F.; Chiavarini, M.; Impicciatore, M.; Bruni, R.; Bianchi, A.; Ballabeni, V. Antinociceptive and gastroprotective effects of inhaled and orally administered Lavandula hybrida Reverchon “Grosso” essential oil. Life Sci. 2004, 76, 213–223. [Google Scholar] [CrossRef]
- Hajhashemi, V.; Ghannadi, A.; Sharif, B. Anti-inflammatory and analgesic properties of the leaf extracts and essential oil of Lavandula angustifolia Mill. J. Ethnopharmacol. 2003, 89, 67–71. [Google Scholar] [CrossRef] [PubMed]
- EMA Monographs. Available online: https://www.ema.europa.eu/en/medicines/herbal/menthae-piperitae-aetheroleum (accessed on 21 November 2022).
- Peier, A.M.; Moqrich, A.; Hergarden, A.C.; Reeve, A.J.; Andersson, D.A.; Story, G.M.; Earley, T.J.; Dragoni, I.; McIntyre, P.; Bevan, S.; et al. A TRP channel that senses cold stimuli and menthol. Cell 2002, 108, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Tisserand, R.; Young, R. 13—Essential oil profiles. In Essential Oil Safety, 2nd ed.; Tisserand, R., Young, R., Eds.; Churchill Livingstone: St. Louis, MI, USA, 2014; pp. 187–482. [Google Scholar]
- de Sousa, D.P. Analgesic-like activity of essential oils constituents. Molecules 2011, 16, 2233–2252. [Google Scholar] [CrossRef] [PubMed]
- Ghelardini, C.; Galeotti, N.; Di Cesare Mannelli, L.; Mazzanti, G.; Bartolini, A. Local anaesthetic activity of beta-caryophyllene. Farmaco 2001, 56, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Khalilzadeh, E.; Hazrati, R.; Saiah, G.V. Effects of topical and systemic administration of Eugenia caryophyllata buds essential oil on corneal anesthesia and analgesia. Res. Pharm. Sci. 2016, 11, 293–302. [Google Scholar] [CrossRef]
- Malan, P.T., Jr.; Ibrahim, M.M.; Deng, H.; Liu, Q.; Mata, H.P.; Vanderah, T.; Porreca, F.; Makriyannis, A. CB2 cannabinoid receptor-mediated peripheral antinociception. Pain 2001, 93, 239–245. [Google Scholar] [CrossRef]
- Rondanelli, M.; Fossari, F.; Vecchio, V.; Gasparri, C.; Peroni, G.; Spadaccini, D.; Riva, A.; Petrangolini, G.; Iannello, G.; Nichetti, M.; et al. Clinical trials on pain lowering effect of ginger: A narrative review. Phytother. Res. PTR 2020, 34, 2843–2856. [Google Scholar] [CrossRef]
- Borgonetti, V.; Lopez, V.; Galeotti, N. Ylang-ylang (Cananga odorata (Lam.) Hook. f. & Thomson) essential oil reduced neuropathic-pain and associated anxiety symptoms in mice. J. Ethnopharmacol. 2022, 294, 115362. [Google Scholar] [CrossRef]





| Study | Patients | Study Design | Country | Number of Patients | Applied Essential Oils | Intervention | Placebo | No Intervention | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Nasiri et al., 2016 [25] | patients with knee OA | RCT | Iran | 90 | 3% lavender oil | aromatherapy massage with lavender EO | placebo massage with sweet almond oil | no massage | pain intensity (qualitative and quantitative analysis) |
| Kong et al., 2012 [24] | athletes with non-specific low back pain | RCT | China | 110 | herbal ointment containing 20% of EOs (extracted from Dang Gui, Chuan Xiong, Xi Xin, and Rou Gui) | Chinese massage combined with herbal ointment | massage therapy with placebo ointment | n/a | pain intensity (qualitative and quantitative analysis) |
| Eftekharsadat et al., 2018 [21] | patients with mild to moderate CTS | RCT | Iran | 48 | 1.5% lavender EO | night wrist orthotic and topical lavender oil ointment | night wrist orthotic and a placebo ointment | n/a | pain intensity (qualitative and quantitative analysis) |
| Pehlivan and Karadakovan, 2019 [27] | elderly individuals with knee osteoarthritis | RCT | Turkey | 90 | two EOs (2.5% ginger and 2.5% rosemary) were added to the black seed oil | aromatherapy massage | massage group (sunflower oil) | control group (no aromatherapy or massage) | pain intensity, stiffness (qualitative and quantitative analysis) |
| Shirazi et al., 2017 [28] | women with pregnancy-related low back pain | RCT | Iran | 120 | rose oil (in the carrier of almond oil) | EO applied topically | almond oil | no intervention (no EO, no massage) | pain intensity (qualitative and quantitative analysis) |
| Yip and Tam, 2008 [29] | moderate-to-severe knee pain among the elderly | RCT | China | 59 | 1% ginger and 0.5% orange EO | massage with ginger and orange oil | massage intervention with olive oil only | no massage | pain intensity, stiffness (qualitative and quantitative analysis) |
| Ou et al., 2014 [24] | patients with neck pain | RCT | Taiwan | 60 | 3% cream containing marjoram, black pepper, lavender and peppermint EOs | the cream was applied on the neck and upper trapezius muscles | placebo ointment | n/a | pain intensity (qualitative and quantitative analysis) |
| Yip and Tse, 2006 [31] | sub-acute, non-specific neck pain | RCT | China | 32 | 3% lavender oil with olive oil | manual acupressure massage with natural aromatic lavender oil | n/a | conventional treatment | stiffness (qualitative and quantitative analysis) |
| Yip and Tse, 2004 [30] | non-specific low back pain | RCT | China | 61 | 3% lavender oil with grape seed oil | acupressure massage with natural aromatic lavender oil | n/a | conventional treatment | pain intensity (qualitative analysis) |
| Bahr et al., 2018 [20] | hand arthritis | RCT | USA | 36 | mixture of EOs (main components: 16% methyl salicylate, 6% menthol, 27% beta-caryophyllene) | hand massage | coconut oil | n/a | pain intensity (qualitative analysis) |
| El Sayed et al., 2020 [22] | knee osteoarthritis | RCT | Egypt | 60 | 3% lavender EO | aromatherapy massage | n/a | conventional treatment | pain intensity (qualitative analysis) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakó, E.; Fehérvári, P.; Garami, A.; Dembrovszky, F.; Gunther, E.E.; Hegyi, P.; Csupor, D.; Böszörményi, A. Efficacy of Topical Essential Oils in Musculoskeletal Disorders: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pharmaceuticals 2023, 16, 144. https://doi.org/10.3390/ph16020144
Bakó E, Fehérvári P, Garami A, Dembrovszky F, Gunther EE, Hegyi P, Csupor D, Böszörményi A. Efficacy of Topical Essential Oils in Musculoskeletal Disorders: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pharmaceuticals. 2023; 16(2):144. https://doi.org/10.3390/ph16020144
Chicago/Turabian StyleBakó, Eszter, Péter Fehérvári, András Garami, Fanni Dembrovszky, Emese Eszter Gunther, Péter Hegyi, Dezső Csupor, and Andrea Böszörményi. 2023. "Efficacy of Topical Essential Oils in Musculoskeletal Disorders: Systematic Review and Meta-Analysis of Randomized Controlled Trials" Pharmaceuticals 16, no. 2: 144. https://doi.org/10.3390/ph16020144
APA StyleBakó, E., Fehérvári, P., Garami, A., Dembrovszky, F., Gunther, E. E., Hegyi, P., Csupor, D., & Böszörményi, A. (2023). Efficacy of Topical Essential Oils in Musculoskeletal Disorders: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pharmaceuticals, 16(2), 144. https://doi.org/10.3390/ph16020144