
Disease-Modifying Therapies (DMTs) in Pregnant and Lactating Women with Multiple Sclerosis: Analysis of Real-World Data from EudraVigilance Database

Abstract
:1. Introduction
2. Results
2.1. Characteristics of Adverse Drug Reactions (ADRs)
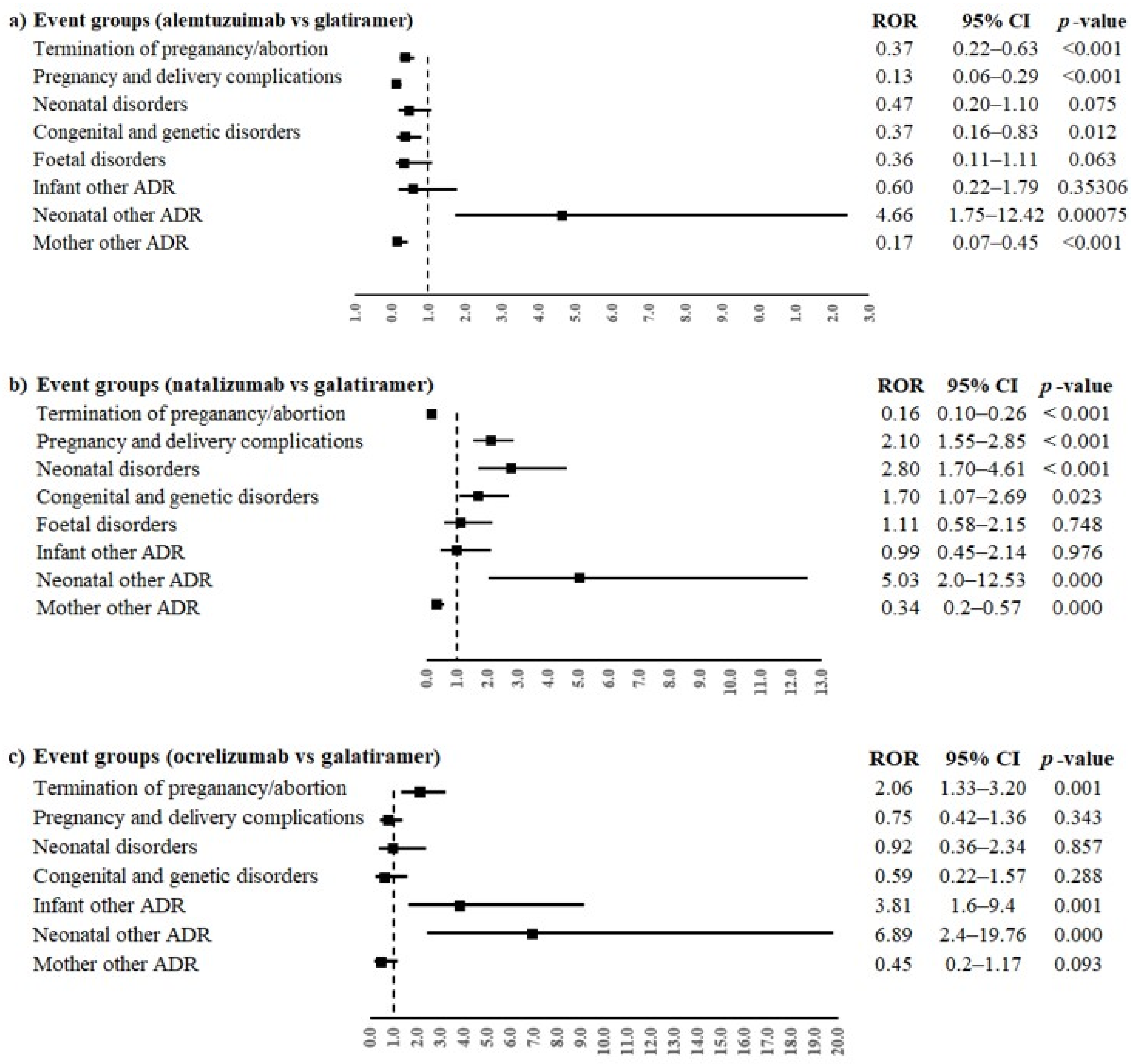
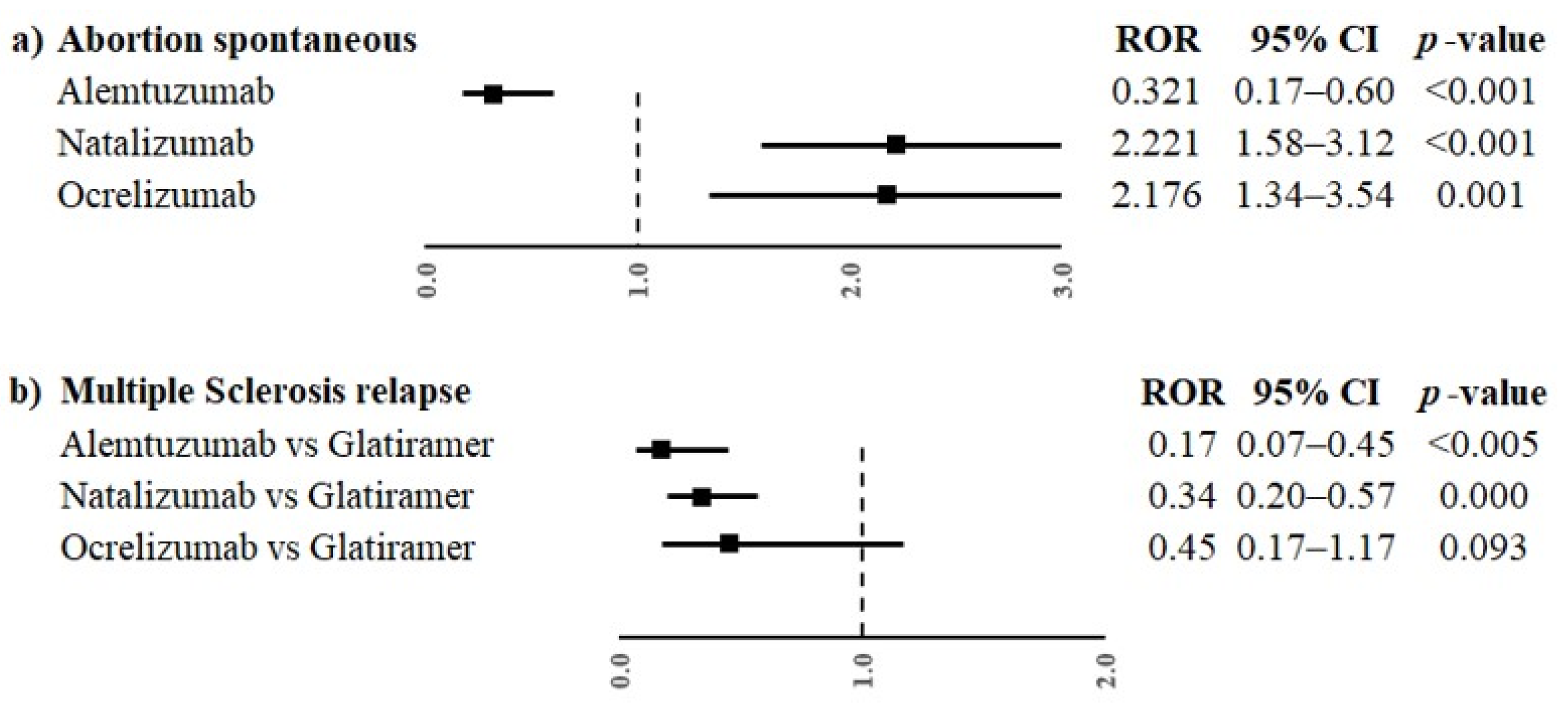
2.2. Reporting Odds Ratio (ROR)
3. Discussion
Strengths and Limits
4. Materials and Methods
4.1. Data Source
4.2. Data Retrieval
4.3. Data Analyses
4.4. Disproportionality Analyses
4.5. Compliance with Ethical Standards
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamaita, R.; Melo, C.; Laranjeira, C.; Barquero, P.; Gomes, J.; Silva-Filho, A. Multiple Sclerosis in Pregnancy and Its Role in Female Fertility: A Systematic Review. JBRA Assist. Reprod. 2021, 25, 493. [Google Scholar] [CrossRef] [PubMed]
- Ben-Zacharia, A.B. Therapeutics for Multiple Sclerosis Symptoms. Mt. Sinai J. Med. A J. Transl. Pers. Med. 2011, 78, 176–191. [Google Scholar] [CrossRef] [PubMed]
- Olsson, T.; Barcellos, L.F.; Alfredsson, L. Interactions between Genetic, Lifestyle and Environmental Risk Factors for Multiple Sclerosis. Nat. Rev. Neurol. 2016, 13, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Harbo, H.F.; Gold, R.; Tintora, M. Sex and Gender Issues in Multiple Sclerosis. Ther. Adv. Neurol. Disord. 2013, 6, 237. [Google Scholar] [CrossRef] [PubMed]
- Villaverde-González, R. Updated Perspectives on the Challenges of Managing Multiple Sclerosis During Pregnancy. Degener. Neurol. Neuromuscul. Dis. 2022, 12, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Dahl, J.; Myhr, K.M.; Daltveit, A.K.; Gilhus, N.E. Pregnancy, Delivery and Birth Outcome in Different Stages of Maternal Multiple Sclerosis. J. Neurol. 2008, 255, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Van Der Kop, M.L.; Pearce, M.S.; Dahlgren, L.; Synnes, A.; Sadovnick, D.; Sayao, A.L.; Tremlett, H. Neonatal and Delivery Outcomes in Women with Multiple Sclerosis. Ann. Neurol. 2011, 70, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Lu, E.; Zhao, Y.; Zhu, F.; Van Der Kop, M.L.; Synnes, A.; Dahlgren, L.; Sadovnick, A.D.; Sayao, A.L.; Tremlett, H. Birth Hospitalization in Mothers with Multiple Sclerosis and Their Newborns. Neurology 2013, 80, 447–452. [Google Scholar] [CrossRef]
- Birk, K.; Smeltzer, S.C.; Rudick, R. Pregnancy and Multiple Sclerosis. Semin. Neurol. 1988, 8, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Airas, L.; Kaaja, R. Pregnancy and Multiple Sclerosis. Obstet. Med. 2012, 5, 94. [Google Scholar] [CrossRef]
- Varytė, G.; Zakarevičienė, J.; Ramašauskaitė, D.; Laužikienė, D.; Arlauskienė, A. Pregnancy and Multiple Sclerosis: An Update on the Disease Modifying Treatment Strategy and a Review of Pregnancy’s Impact on Disease Activity. Medicina 2020, 56, 49. [Google Scholar] [CrossRef] [PubMed]
- Simone, I.L.; Tortorella, C.; Ghirelli, A. Influence of Pregnancy in Multiple Sclerosis and Impact of Disease-Modifying Therapies. Front. Neurol. 2021, 12, 697974. [Google Scholar] [CrossRef]
- Alroughani, R.; Akhtar, S.; Zeineddine, M.; EL Kouzi, Y.; El Ayoubi, N.K.; Ahmed, S.F.; Behbehani, R.; Khoury, S.J.; Al-Hashel, J.Y.; Yamout, B.I. Risk of Relapses during Pregnancy among Multiple Sclerosis Patients. Mult. Scler. Relat. Disord. 2019, 34, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, A. European and American Guidelines for Multiple Sclerosis Treatment. Neurol. Ther. 2018, 7, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Lu, E.; Wang, B.W.; Guimond, C.; Synnes, A.; Sadovnick, D.; Tremlett, H. Disease-Modifying Drugs for Multiple Sclerosis in Pregnancy: A Systematic Review. Neurology 2012, 79, 1130–1135. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Geissbühler, Y.; Sabidó, M.; Turkson, M.; Wahlich, C.; Morris, J.K. A Systematic Review and Meta-Analyses of Pregnancy and Fetal Outcomes in Women with Multiple Sclerosis: A Contribution from the IMI2 ConcePTION Project. J. Neurol. 2020, 267, 2721. [Google Scholar] [CrossRef] [PubMed]
- Hellwig, K.; Tokic, M.; Thiel, S.; Esters, N.; Spicher, C.; Timmesfeld, N.; Ciplea, A.I.; Gold, R.; Langer-Gould, A. Multiple Sclerosis Disease Activity and Disability Following Discontinuation of Natalizumab for Pregnancy. JAMA Netw. Open 2022, 5, E2144750. [Google Scholar] [CrossRef] [PubMed]
- Portaccio, E.; Annovazzi, P.; Ghezzi, A.; Zaffaroni, M.; Moiola, L.; Martinelli, V.; Lanzillo, R.; Morra, V.B.; Rinaldi, F.; Gallo, P.; et al. Pregnancy Decision-Making in Women with Multiple Sclerosis Treated with Natalizumab: I: Fetal Risks. Neurology 2018, 90, e823–e831. [Google Scholar] [CrossRef]
- Smith, A.L.; Cohen, J.A.; Ontaneda, D.; Rensel, M. Pregnancy and Multiple Sclerosis: Risk of Unplanned Pregnancy and Drug Exposure in Utero. Mult. Scler. J. Exp. Transl. Clin. 2019, 5, 1744. [Google Scholar] [CrossRef]
- MacDonald, S.C.; McElrath, T.F.; Hernández-Díaz, S. Use and Safety of Disease-Modifying Therapy in Pregnant Women with Multiple Sclerosis. Pharmacoepidemiol. Drug Saf. 2019, 28, 556–560. [Google Scholar] [CrossRef]
- Howard, T.B.; Tassinari, M.S.; Feibus, K.B.; Mathis, L.L. Monitoring for Teratogenic Signals: Pregnancy Registries and Surveillance Methods. Am. J. Med. Genet. C Semin. Med. Genet. 2011, 157C, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Mascolo, A.; di Mauro, G.; Fraenza, F.; Gaio, M.; Zinzi, A.; Pentella, C.; Rossi, F.; Capuano, A.; Sportiello, L. Maternal, Fetal and Neonatal Outcomes among Pregnant Women Receiving COVID-19 Vaccination: The Preg-Co-Vax Study. Front. Immunol. 2022, 13, 965171. [Google Scholar] [CrossRef] [PubMed]
- Krajnc, N.; Bsteh, G.; Berger, T.; Mares, J.; Hartung, H.P. Monoclonal Antibodies in the Treatment of Relapsing Multiple Sclerosis: An Overview with Emphasis on Pregnancy, Vaccination, and Risk Management. Neurotherapeutics 2022, 19, 753–773. [Google Scholar] [CrossRef] [PubMed]
- Orthmann-Murphy, J.L.; Calabresi, P.A. Therapeutic Application of Monoclonal Antibodies in Multiple Sclerosis. Clin. Pharmacol. Ther. 2017, 101, 52–64. [Google Scholar] [CrossRef]
- Carlson, A.K.; Ontaneda, D.; Rensel, M.R.; Cohen, J.A.; Kunchok, A. Reproductive Issues and Multiple Sclerosis: 20 Questions. Clevel. Clin. J. Med. 2023, 90, 235–243. [Google Scholar] [CrossRef]
- Varytė, G.; Arlauskienė, A.; Ramašauskaitė, D. Pregnancy and Multiple Sclerosis: An Update. Curr. Opin. Obstet. Gynecol. 2021, 33, 378–383. [Google Scholar] [CrossRef] [PubMed]
- European Medicine Agency. Annex I Summary of Product Characteristics. In Tysabri (Natalizumab); European Medicine Agency: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Food and Drug Administration. Highlights of Prescribing Information. In Copaxone (Glatiramer Acetate Injection); Food and Drug Administration: Silver Spring, MD, USA, 2022. [Google Scholar]
- Giannini, M.; Portaccio, E.; Ghezzi, A.; Hakiki, B.; Pastò, L.; Razzolini, L.; Piscolla, E.; De Giglio, L.; Pozzilli, C.; Paolicelli, D.; et al. Pregnancy and Fetal Outcomes after Glatiramer Acetate Exposure in Patients with Multiple Sclerosis: A Prospective Observational Multicentric Study. BMC Neurol. 2012, 12, 124. [Google Scholar] [CrossRef] [PubMed]
- Tillaut, H.; Degrémont, A.; Kerbrat, S.; Roux, J.; Le Page, E.; Mainguy, C.; Duros, S.; Polard, E.; Leray, E. Pregnancy in Women with Multiple Sclerosis in France from 2010 to 2015: Incidence, Outcomes, and Exposure to Disease-Modifying Therapies. Mult. Scler. 2022, 28, 778–789. [Google Scholar] [CrossRef]
- Duchesneau, E.D.; Kinlaw, A.C.; Jonsson Funk, M.; Pate, V.; Lund, J.L. Trends in the Use of Disease-Modifying Therapies among Reproductive-Aged Women with Multiple Sclerosis in the United States from 2010 to 2019. Pharmacoepidemiol. Drug Saf. 2022, 31, 481–487. [Google Scholar] [CrossRef]
- Sandberg-Wollheim, M.; Neudorfer, O.; Grinspan, A.; Weinstock-Guttman, B.; Haas, J.; Izquierdo, G.; Riley, C.; Ross, A.P.; Baruch, P.; Drillman, T.; et al. Pregnancy Outcomes from the Branded Glatiramer Acetate Pregnancy Database. Int. J. MS Care 2018, 20, 9–14. [Google Scholar] [CrossRef]
- European Medicine Agency. Annex I Summary of Product Characteristics. In Lemtrada (Alemtuzumab); European Medicine Agency: Amsterdam, The Netherlands, 2006. [Google Scholar]
- European Medicine Agency. Annex I Summary of Product Characteristics. In Ocrevus (Ocrelizumab); European Medicine Agency: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Valeria, R.C.; Roberta, L.; Francesco, S.; Marcello, M.; Antonio, C.; Vincenzo, B.M. Pregnancy Outcomes in Alemtuzumab Treated Women with Multiple Sclerosis: A Case Series. Neurol. Sci. 2021, 42, 3427–3430. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Achiron, A.; Celius, E.G.; Chambers, C.; Derwenskus, J.; Devonshire, V.; Hellwig, K.; Hutton, G.J.; McCombe, P.; Moore, M.; et al. Pregnancy Outcomes and Postpartum Relapse Rates in Women with RRMS Treated with Alemtuzumab in the Phase 2 and 3 Clinical Development Program over 16 Years. Mult. Scler. Relat. Disord. 2020, 43, 102146. [Google Scholar] [CrossRef] [PubMed]
- European Medicine Agency. Guideline on Good Pharmacovigilance Practices (GVP)–Product- or Population-Specific Considerations III: Pregnant and Breastfeeding Women; European Medicine Agency: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Hellwig, K.; Verdun di Cantogno, E.; Sabidó, M. A Systematic Review of Relapse Rates during Pregnancy and Postpartum in Patients with Relapsing Multiple Sclerosis. Ther. Adv. Neurol. Disord. 2021, 14, 1012. [Google Scholar] [CrossRef] [PubMed]
- Zanghì, A.; D’Amico, E.; Callari, G.; Chisari, C.G.; Borriello, G.; Grimaldi, L.M.E.; Patti, F. Pregnancy and the Postpartum Period in Women with Relapsing-Remitting Multiple Sclerosis Treated with Old and New Disease-Modifying Treatments: A Real-World Multicenter Experience. Front. Neurol. 2020, 11, 499730. [Google Scholar] [CrossRef] [PubMed]
- Thiel, S.; Ciplea, A.I.; Gold, R.; Hellwig, K. The German Multiple Sclerosis and Pregnancy Registry: Rationale, Objective, Design, and First Results. Ther. Adv. Neurol. Disord. 2021, 14, 4956. [Google Scholar] [CrossRef] [PubMed]
- Bsteh, G.; Hegen, H.; Riedl, K.; Altmann, P.; Di Pauli, F.; Ehling, R.; Zulehner, G.; Rommer, P.; Leutmezer, F.; Deisenhammer, F.; et al. Estimating Risk of Multiple Sclerosis Disease Reactivation in Pregnancy and Postpartum: The VIPRiMS Score. Front. Neurol. 2022, 12, 766956. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, M.A.; Sorbara, E.E.; Battaglia, A.; Cicala, G.; Rizzo, V.; Spina, E.; Cutroneo, P.M. Adverse Drug Reactions with Drugs Used in Multiple Sclerosis: An Analysis from the Italian Pharmacovigilance Database. Front. Pharmacol. 2022, 13, 808370. [Google Scholar] [CrossRef]
- Gitman, V.; Stavropoulos, A.; Saenz, V.; Pasquarelli, N.; Zecevic, D.; Devonshire, V. Pregnancy Outcomes of Women with Multiple Sclerosis Treated with Ocrelizumab in Canada: A Descriptive Analysis of Real-World Data. Mult. Scler. Relat. Disord. 2022, 62, 103792. [Google Scholar] [CrossRef]
- Risch, H.A.; Weiss, N.S.; Aileen Clarke, E.; Miller, A.B. Risk Factors for Spontaneous Abortion and Its Recurrence. Am. J. Epidemiol. 1988, 128, 420–430. [Google Scholar] [CrossRef]
- Nguyen, A.L.; Havrdova, E.K.; Horakova, D.; Izquierdo, G.; Kalincik, T.; van der Walt, A.; Terzi, M.; Alroughani, R.; Duquette, P.; Girard, M.; et al. Incidence of Pregnancy and Disease-Modifying Therapy Exposure Trends in Women with Multiple Sclerosis: A Contemporary Cohort Study. Mult. Scler. Relat. Disord. 2019, 28, 235–243. [Google Scholar] [CrossRef]
- Godano, E.; Barra, F.; Allodi, A.; Ferraiolo, A.; Laroni, A.; Novi, G.; Mancardi, G.L.; Gustavino, C.; Arioni, C. Erythropoietin Therapy in a Case of Neonatal Anemia after Exposure to Natalizumab throughout Pregnancy. Ital. J. Pediatr. 2021, 47, 69. [Google Scholar] [CrossRef] [PubMed]
- Proschmann, U.; Haase, R.; Inojosa, H.; Akgün, K.; Ziemssen, T. Drug and Neurofilament Levels in Serum and Breastmilk of Women with Multiple Sclerosis Exposed to Natalizumab During Pregnancy and Lactation. Front. Immunol. 2021, 12, 715195. [Google Scholar] [CrossRef] [PubMed]
- Mahzari, M.; Arnaout, A.; Freedman, M.S. Alemtuzumab Induced Thyroid Disease in Multiple Sclerosis: A Review and Approach to Management. Can. J. Neurol. Sci. 2015, 42, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Hammerstad, S.S.; Celius, E.G.; Husby, H.; Sørensen, I.M.; Norheim, I.E. Management of Severe Graves’ Hyperthyroidism in Pregnancy Following Immune Reconstitution Therapy in Multiple Sclerosis. J. Endocr. Soc. 2021, 5, bvab044. [Google Scholar] [CrossRef] [PubMed]
- Berger, T.; Elovaara, I.; Fredrikson, S.; McGuigan, C.; Moiola, L.; Myhr, K.M.; Oreja-Guevara, C.; Stoliarov, I.; Zettl, U.K. Alemtuzumab Use in Clinical Practice: Recommendations from European Multiple Sclerosis Experts. CNS Drugs 2017, 31, 33–50. [Google Scholar] [CrossRef] [PubMed]
- De Lima Kaminski, V.; Michita, R.T.; Ellwanger, J.H.; Veit, T.D.; Schuch, J.B.; dos Riesgo, R.S.; Roman, T.; Chies, J.A.B. Exploring Potential Impacts of Pregnancy-Related Maternal Immune Activation and Extracellular Vesicles on Immune Alterations Observed in Autism Spectrum Disorder. Heliyon 2023, 9, e15593. [Google Scholar] [CrossRef] [PubMed]
- Siracusano, M.; Carloni, E.; Riccioni, A.; Ferrara, M.; Scoppola, C.; Arturi, L.; Niolu, C.; Marfia, G.A.; Mazzone, L. Maternal Multiple Sclerosis and Offspring’s Cognitive and Behavioral Development: What Do We Know until Now? Children 2022, 9, 1716. [Google Scholar] [CrossRef] [PubMed]
- Carta, A.; Zarbo, I.R.; Scoppola, C.; Pisuttu, G.; Conti, M.; Melis, M.C.; De Martino, F.; Serra, A.; Biancu, M.A.; Guerini, F.R.; et al. Maternal Multiple Sclerosis Is Not a Risk Factor for Neurodevelopmental Disorders in Offspring. Mult. Scler. J. Exp. Transl. Clin. 2021, 7, 7301. [Google Scholar] [CrossRef]
- Proschmann, U.; Akgün, K.; Ziemssen, T. Reader Response: Pregnancy Decision-Making in Women with Multiple Sclerosis Treated with Natalizumab: I: Fetal Risks. Neurology 2018, 91, 849–850. [Google Scholar] [CrossRef]
- Sportiello, L.; Capuano, A. It Is the Time to Change the Paradigms of Pregnant and Breastfeeding Women in Clinical Research! Front. Pharmacol. 2023, 14, 1113557. [Google Scholar] [CrossRef]
- European Medicine Agency. Committee for Medicinal Products for Human Use (CHMP). Guideline on the Exposure to Medicinal Products During Pregnancy: Need for Post-Authorisation Data; European Medicine Agency: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Ruggiero, R.; Stelitano, B.; Fraenza, F.; di Mauro, G.; Scavone, C.; Sportiello, L.; Rafaniello, C.; Di Napoli, R.; Danesi, R.; Del Re, M.; et al. Neurological Manifestations Related to Immune Checkpoint Inhibitors: Reverse Translational Research by Using the European Real-World Safety Data. Front. Oncol. 2022, 12, 824511. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Event Groups | Glatiramer (n = 201) | Alemtuzumab (n = 100) | Natalizumab (n = 839) | Ocrelizumab (n = 96) | Total (n = 1236) |
|---|---|---|---|---|---|
| Child age group | |||||
| Foetus | 2 (1.0) | 3 (3.0) | 5 (0.6) | 5 (5.2) | 15 (1.2) |
| Neonate (0–1 m) | 13 (6.5) | 8 (8.0) | 107 (12.8) | 7 (7.3) | 135 (10.9) |
| Infant (2 m–2 y) | 6 (3.0) | 4 (4.0) | 25 (3.0) | 3 (3.1) | 38 (3.1) |
| Mother age group | |||||
| 12–17 Years | 1 (0.5) | 0 (0) | 2 (0.2) | 0 (0) | 3 (0.2) |
| 18–64 Years | 126 (62.7) | 72 (72.0) | 481 (57.3) | 40 (41.7) | 719 (58.2) |
| Not specified age group | |||||
| Not specified | 53 (26.4) | 13 (13.0) | 219 (26.1) | 41 (42.7) | 326 (26.4) |
| Baby sex | |||||
| Female | 6 (3.0) | 8 (8.0) | 35 (4.2) | 4 (4.2) | 53 (4.3) |
| Male | 12 (6.0) | 4 (4.0) | 45 (5.4) | 8 (8.3) | 69 (5.6) |
| Not specified | 3 (1.5) | 3 (3.0) | 57 (6.8) | 3 (3.1) | 66 (5.3) |
| Type of reporting | |||||
| Spontaneous | 201 (100.02) | 100 (100.0) | 839 (100.0) | 96 (100.0) | 1236 (100.0) |
| Not spontaneous | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Primary source qualification | |||||
| Healthcare professional | 117 (58.2) | 84 (84.0) | 766 (91.3) | 84 (87.5) | 1051 (85.0) |
| Non-healthcare professional | 84 (41.8) | 16 (16.0) | 73 (8.7) | 12 (12.5) | 185 (15.0) |
| Primary source country | |||||
| European economic area | 145 (72.1) | 67 (67.0) | 529 (63.1) | 41 (42.7) | 782 (63.3) |
| Non-European economic area | 56 (27.9) | 33 (33.0) | 310 (36.9) | 55 (57.3) | 454 (36.7) |
| Seriousness | |||||
| Not serious | 36 (17.9) | 31 (31.0) | 168 (20.0) | 15 (15.6) | 250 (20.2) |
| Serious | 165 (82.1) | 69 (69.0) | 671 (80.0) | 81 (84.4) | 986 (79.8) |
| Type of exposure | |||||
| Maternal/Foetal exposure during pregnancy or transplacental route | 180 (89.6) | 39 (39.0) | 770 (91.8) | 59 (61.5) | 1048 (84.8) |
| Exposure via breast milk/during breast feeding or transmammary route | 6 (3.0) | 3 (3.0) | 22 (2.6) | 3 (3.1) | 34 (2.8) |
| Maternal/Drug exposure before pregnancy | 4 (2.0) | 22 (22.0) | - | 20 (20.8) | 46 (3.7) |
| Maternal/Foetal exposure timing unspecified or transplacental route | - | 4 (4.0) | 2 (0.2) | 7 (7.3) | 13 (1.0) |
| Not specified | 11 (5.4) | 32 (32.0) | 45 (5.4) | 7 (7.3) | 95 (7.7) |
| Suspect drug(s) other than DMT | |||||
| 0 | 150 (74.6) | 85 (85.0) | 604 (72.0) | 82 (85.4) | 921 (74.6) |
| 1 | 28 (13.9) | 6 (6.0) | 178 (21.2) | 8 (8.3) | 220 (17.8) |
| 2 | 16 (8.0) | 4 (4.0) | 46 (5.5) | 6 (6.3) | 72 (5.8) |
| 3 | 1 (0.5) | 3 (3.0) | 6 (0.7) | 0 (0) | 10 (0.8) |
| ≥4 | 6 (3.0) | 2 (2.0) | 5 (0.6) | 0 (0) | 13 (1.1) |
| Concomitant drug(s) | |||||
| 1 | 10 (5.0) | 7 (7.0) | 49 (5.8) | 5 (5.2) | 71 (5.7) |
| 2 | 8 (4.0) | 3 (3.0) | 36 (4.3) | 11 (11.5) | 58 (4.7) |
| 3 | 4 (2.0) | 4 (4.0) | 21 (2.5) | 1 (1.0) | 30 (2.4) |
| 4 | 1 (0.5) | 4 (4.0) | 12 (1.4) | 3 (3.1) | 20 (1.6) |
| ≥5 | 4 (2.0) | 10 (10.0) | 24 (2.9) | 6 (6.3) | 44 (3.6) |
| Not reported | 174 (86.6) | 72 (72.0) | 697 (83.1) | 70 (72.9) | 1013 (82.0) |
| Event Groups | Glatiramer (n = 720) | Alemtuzumab (n = 666) | Natalizumab (n = 1943) | Ocrelizumab (n = 261) | Total (n = 3590) § * |
|---|---|---|---|---|---|
| Maternal other ADRs | 254 (35.3) | 501 (75.2) | 204 (10.5) | 69 (26.4) | 1028 (28.6) |
| Multiple sclerosis relapse | 30 (4.2) | 5 (0.7) | 28 (1.4) | 5 (1.9) | 68 (1.9) |
| Haemorrhage | 2 (0.3) | 2 (0.3) | 8 (0.4) | 3 (1.1) | 15 (0.4) |
| Anaemia | 4 (0.6) | 2 (0.3) | 7 (0.4) | - | 13 (0.4) |
| Dyspnoea | 4 (0.6) | 7 (1.1) | 1 (0.1) | 1 (0.4) | 13 (0.4) |
| Termination of pregnancy and risk of abortion | 55 (7.6) | 20 (3.0) | 266 (13.7) | 38 (14.6) | 379 (10.6) |
| Abortion spontaneous | 42 (5.8) | 13 (2.0) | 235 (12.1) | 31 (11.9) | 321 (8.9) |
| Abortion | 6 (0.8) | 2 (0.3) | 8 (0.4) | - | 16 (0.4) |
| Abortion missed | 3 (0.4) | - | 6 (0.3) | 3 (1.1) | 12 (0.3) |
| Foetal death | 1 (0.1) | 1 (0.2) | 2 (0.1) | 2 (0.8) | 6 (0.2) |
| Pregnancy, labour and delivery complications and risk factors (excl abortions and stillbirth) | 54 (7.5) | 7 (1.1) | 284 (14.6) | 15 (5.7) | 360 (10.0) |
| Caesarean section | 13 (1.8) | - | 93 (4.8) | - | 106 (2.9) |
| Premature delivery | 2 (0.3) | - | 35 (1.8) | 3 (1.1) | 40 (1.1) |
| Gestational diabetes | 6 (0.8) | 1 (0.2) | 8 (0.4) | 3 (1.1) | 18 (0.5) |
| Pre-eclampsia | 1 (0.1) | - | 16 (0.8) | - | 17 (0.5) |
| Neonatal disorders | 18 (2.5) | 8 (1.2) | 130 (6.7) | 6 (2.3) | 162 (4.5) |
| Premature baby | 5 (0.7) | 1 (0.2) | 52 (2.7) | 4 (1.5) | 62 (1.7) |
| Low birth weight baby | 1 (0.1) | - | 24 (1.2) | - | 25 (0.7) |
| Anaemia neonatal | - | - | 16 (0.8) | 1 (0.4) | 17 (0.5) |
| Jaundice neonatal | 1 (0.1) | - | 5 (0.3) | - | 6 (0.2) |
| Congenital, familial and genetic disorders | 23 (3.2) | 8 (1.2) | 103 (5.3) | 5 (1.9) | 139 (3.9) |
| Trisomy 21 | - | - | 6 (0.3) | 1 (0.4) | 7 (0.2) |
| Atrial septal defect | 2 (0.3) | 1 (0.2) | 3 (0.2) | - | 6 (0.2) |
| Ventricular septal defect | 1 (0.1) | - | 4 (0.2) | - | 5 (0.1) |
| Talipes | - | - | 4 (0.2) | - | 4 (0.1) |
| Neonatal other ADRs | 3 (0.4) | 18 (2.7) | 56 (2.9) | 12 (4.6) | 89 (2.5) |
| Thrombocytopaenia | - | - | 9 (0.5) | - | 9 (0.3) |
| Anaemia | - | - | 4 (0.2) | - | 4 (0.1) |
| Platelet count decreased | - | - | 3 (0.2) | - | 3 (0.1) |
| Anti-thyroid antibody positive | - | 2 (0.3) | - | - | 2 (0.06) |
| Foetal disorders | 12 (1.7) | 4 (0.6) | 36 (1.9) | 1 (0.4) | 53 (1.5) |
| Foetal growth restriction | 5 (0.7) | 3 (0.5) | 10 (0.5) | 1 (0.4) | 19 (0.5) |
| Foetal heart rate abnormal | 2 (0.3) | - | 5 (0.3) | - | 7 (0.2) |
| Foetal malformation | 2 (0.3) | - | 5 (0.3) | - | 7 (0.2) |
| Foetal distress syndrome | - | - | 4 (0.2) | - | 4 (0.1) |
| Infant other ADRs | 9 (1.3) | 5 (0.8) | 20 (7.7) | 10 (3.8) | 44 (1.2) |
| Anaemia | - | - | 3 (0.2) | - | 3 (0.1) |
| Autism spectrum disorder | - | - | 3 (0.2) | - | 3 (0.1) |
| COVID-19 | 2 (0.3) | - | - | 1 (0.4) | 3 (0.1) |
| Blood thyroid-stimulating hormone decreased | - | 2 (0.3) | - | - | 2 (0.1) |
| Foetal other ADRs | - | 6 (0.9) | - | 4 (1.5) | 10 (0.3) |
| Bladder dilatation | - | - | - | 1 (0.4) | 1 (0.0) |
| Cerebral calcification | - | 1 (0.2) | - | - | 1 (0.0) |
| Cerebral cyst | - | 1 (0.2) | - | - | 1 (0.0) |
| Cerebral ventricle dilatation | - | 1 (0.2) | - | - | 1 (0.0) |
| Glatiramer (n = 720) | Alemtuzumab (n = 666) | Natalizumab (n = 1943) | Ocrelizumab (n = 261) | Total (n = 3590) | |
|---|---|---|---|---|---|
| Seriousness | |||||
| Results in death | 2 (0.3) | 1 (0.2) | 67 (3.4) | 8 (3.1) | 78 (2.2) |
| Life threatening | 1 (0.1) | 3 (0.5) | 10 (0.5) | 0 (0) | 14 (0.4) |
| Caused/prolonged hospitalisation | 141 (19.6) | 99 (14.9) | 334 (17.2) | 27 (10.3) | 601 (16.7) |
| Disabling | 4 (0.6) | 0 (0) | 0 (0) | 0 (0) | 4 (0.1) |
| Congenital anomaly | 22 (3.1) | 3 (0.5) | 171 (8.8) | 7 (2.7) | 203 (5.7) |
| Other medically important condition | 341 (47.4) | 330 (49.5) | 978 (50.3) | 89 (34.1) | 1738 (48.4) |
| Not serious | 209 (29.0) | 230 (34.5) | 383 (19.7) | 130 (49.8) | 952 (26.5) |
| Outcome | |||||
| Recovered/Resolved | 108 (15.0) | 64 (9.6) | 1117 (57.5) | 37 (14.2) | 1326 (36.9) |
| Recovering/Resolving | 14 (1.9) | 21 (3.2) | 9 (0.5) | 0 (0) | 44 (1.2) |
| Recovered/Resolved with sequelae | 9 (1.3) | 0 (0) | 11 (0.6) | 2 (0.8) | 22 (0.6) |
| Not recovered/not resolved | 45 (6.3) | 231 (34.7) | 109 (5.6) | 11 (4.2) | 396 (11.0) |
| Fatal | 2 (0.3) | 1 (0.2) | 67 (3.4) | 8 (3.1) | 78 (2.2) |
| Unknown | 542 (75.3) | 349 (52.4) | 630 (32.4) | 203 (77.8) | 1724 (48.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sportiello, L.; Di Napoli, R.; Balzano, N.; Mascolo, A.; Ruggiero, R.; Di Costanzo, L.; Monaco, D.; Maniscalco, G.T.; Capuano, A. Disease-Modifying Therapies (DMTs) in Pregnant and Lactating Women with Multiple Sclerosis: Analysis of Real-World Data from EudraVigilance Database. Pharmaceuticals 2023, 16, 1566. https://doi.org/10.3390/ph16111566
Sportiello L, Di Napoli R, Balzano N, Mascolo A, Ruggiero R, Di Costanzo L, Monaco D, Maniscalco GT, Capuano A. Disease-Modifying Therapies (DMTs) in Pregnant and Lactating Women with Multiple Sclerosis: Analysis of Real-World Data from EudraVigilance Database. Pharmaceuticals. 2023; 16(11):1566. https://doi.org/10.3390/ph16111566
Chicago/Turabian StyleSportiello, Liberata, Raffaella Di Napoli, Nunzia Balzano, Annamaria Mascolo, Rosanna Ruggiero, Luigi Di Costanzo, Davida Monaco, Giorgia Teresa Maniscalco, and Annalisa Capuano. 2023. "Disease-Modifying Therapies (DMTs) in Pregnant and Lactating Women with Multiple Sclerosis: Analysis of Real-World Data from EudraVigilance Database" Pharmaceuticals 16, no. 11: 1566. https://doi.org/10.3390/ph16111566
APA StyleSportiello, L., Di Napoli, R., Balzano, N., Mascolo, A., Ruggiero, R., Di Costanzo, L., Monaco, D., Maniscalco, G. T., & Capuano, A. (2023). Disease-Modifying Therapies (DMTs) in Pregnant and Lactating Women with Multiple Sclerosis: Analysis of Real-World Data from EudraVigilance Database. Pharmaceuticals, 16(11), 1566. https://doi.org/10.3390/ph16111566