
Treatments for Ocular Diseases in Pregnancy and Breastfeeding: A Narrative Review
 , , , , and
, , , , and 
Abstract
1. Introduction
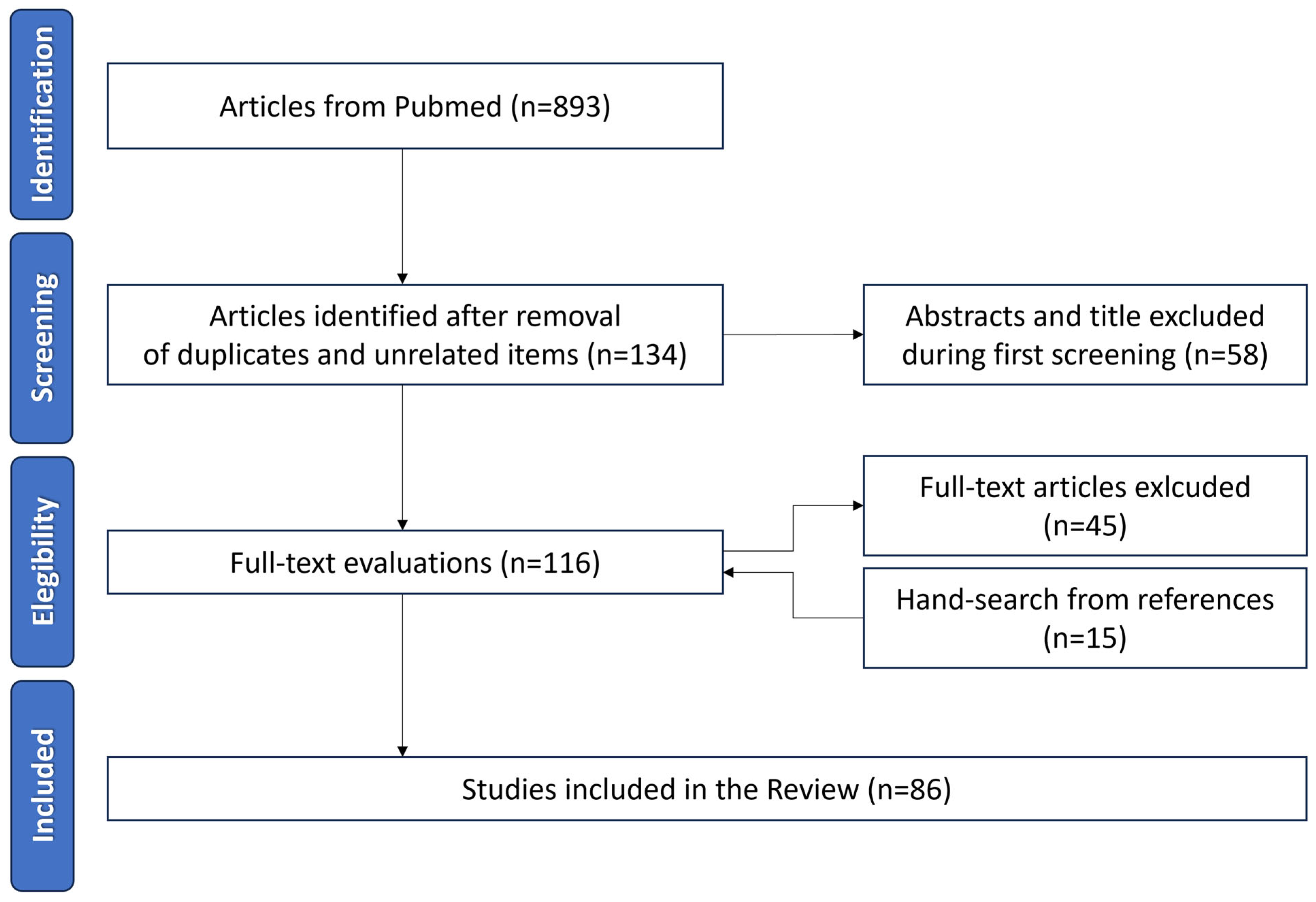
2. Materials and Methods
3. Ocular Drug Delivery
4. Anti-Infective Medications
4.1. Antibiotics
4.2. Antimycotics
4.3. Antivirals
4.4. Antiamoebic
5. Antihistamines
6. Anti-Inflammatory Medications
6.1. Corticosteroids
6.2. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
6.3. Other Immunosuppressive and Anti-Inflammatory Drugs
7. Mydriatics
8. Ocular Anti-Hypertensive Medications
8.1. Beta-Blockers
8.2. Prostaglandin Analogs
8.3. Alpha Agonist
8.4. Carbonic Anhydrase Inhibitors
9. Tear Substitutes
10. Anesthetics
11. Anti-VEGF Injection
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McKiever, M.; Frey, H.; Costantine, M.M. Challenges in Conducting Clinical Research Studies in Pregnant Women. J Pharmacokinet. Pharmacodyn. 2020, 47, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Syme, M.R.; Paxton, J.W.; Keelan, J.A. Drug Transfer and Metabolism by the Human Placenta. Clin Pharmacokinet. 2004, 43, 487–514. [Google Scholar] [CrossRef] [PubMed]
- Blehar, M.C.; Spong, C.; Grady, C.; Goldkind, S.F.; Sahin, L.; Clayton, J.A. Enrolling Pregnant Women: Issues in Clinical Research. Women’s Health Issues 2013, 23, e39–e45. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Amin, M.M.; Sayed, S. Ocular Drug Delivery: A Comprehensive Review. AAPS PharmSciTech 2023, 24, 66. [Google Scholar] [CrossRef] [PubMed]
- Ghate, D.; Edelhauser, H.F. Ocular Drug Delivery. Expert Opin. Drug Deliv. 2006, 3, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.B.; Holmes, A.P.; Eiland, L.S. The Influence of the Food and Drug Administration Pregnancy and Lactation Labeling Rule on Drug Information Resources. Ann. Pharmacother. 2021, 55, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Ramoz, L.L.; Patel-Shori, N.M. Recent Changes in Pregnancy and Lactation Labeling: Retirement of Risk Categories. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2014, 34, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Pernia, S.; DeMaagd, G. The New Pregnancy and Lactation Labeling Rule. Pharm. Ther. 2016, 41, 713–715. [Google Scholar]
- Byrne, J.J.; Saucedo, A.M.; Spong, C.Y. Evaluation of Drug Labels Following the 2015 Pregnancy and Lactation Labeling Rule. JAMA Netw. Open 2020, 3, e2015094. [Google Scholar] [CrossRef]
- Samples, J.R.; Meyer, S.M. Use of Ophthalmic Medications in Pregnant and Nursing Women. Am. J. Ophthalmol. 1988, 106, 616–623. [Google Scholar] [CrossRef]
- Thomseth, V.; Cejvanovic, V.; Jimenez-Solem, E.; Petersen, K.M.; Poulsen, H.E.; Andersen, J.T. Exposure to Topical Chloramphenicol during Pregnancy and the Risk of Congenital Malformations: A Danish Nationwide Cohort Study. Acta Ophthalmol. 2015, 93, 651–653. [Google Scholar] [CrossRef]
- Reali, A.; Ximenes, A.; Cuzzolin, L.; Fanos, V. Antibiotic Therapy in Pregnancy and Lactation. J. Chemother. 2005, 17, 123–130. [Google Scholar] [CrossRef]
- American Academy of Pediatrics Committee on Drugs. The Transfer of Drugs and Other Chemicals Into Human Milk. Pediatrics 2001, 108, 776–789. [Google Scholar] [CrossRef]
- Yefet, E.; Schwartz, N.; Chazan, B.; Salim, R.; Romano, S.; Nachum, Z. The Safety of Quinolones and Fluoroquinolones in Pregnancy: A Meta-Analysis. BJOG 2018, 125, 1069–1076. [Google Scholar] [CrossRef]
- Niebyl, J.R. Antibiotics and Other Anti-Infective Agents in Pregnancy and Lactation. Am. J. Perinatol. 2003, 20, 405–414. [Google Scholar] [CrossRef]
- Cottreau, J.M.; Barr, V.O. A Review of Antiviral and Antifungal Use and Safety during Pregnancy. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2016, 36, 668–678. [Google Scholar] [CrossRef]
- Czeizel, A.E.; Kazy, Z.; Vargha, P. A Case-Control Teratological Study of Vaginal Natamycin Treatment during Pregnancy. Reprod. Toxicol. 2003, 17, 387–391. [Google Scholar] [CrossRef]
- Stone, K.M.; Reiff-Eldridge, R.; White, A.D.; Cordero, J.F.; Brown, Z.; Alexander, E.R.; Andrews, E.B. Pregnancy Outcomes Following Systemic Prenatal Acyclovir Exposure: Conclusions from the International Acyclovir Pregnancy Registry, 1984–1999. Birth Defects Res. Part A Clin. Mol. Teratol. 2004, 70, 201–207. [Google Scholar] [CrossRef]
- Pasternak, B. Use of Acyclovir, Valacyclovir, and Famciclovir in the First Trimester of Pregnancy and the Risk of Birth Defects. JAMA 2010, 304, 859. [Google Scholar] [CrossRef]
- Chou, T.; Hong, B. Ganciclovir Ophthalmic Gel 0.15% for the Treatment of Acute Herpetic Keratitis: Background, Effectiveness, Tolerability, Safety, and Future Applications. Ther. Clin. Risk Manag. 2014, 10, 665–681. [Google Scholar] [CrossRef]
- Sahin, A.; Hamrah, P. Acute Herpetic Keratitis: What Is the Role for Ganciclovir Ophthalmic Gel? Ophthalmol. Eye Dis. 2012, 4, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Concillado, M.; Lund-Andersen, H.; Mathiesen, E.R.; Larsen, M. Dexamethasone Intravitreal Implant for Diabetic Macular Edema During Pregnancy. Am. J. Ophthalmol. 2016, 165, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, D.; El-Asrar, A.A.; McCluskey, P. Treatment of Severe Inflammatory Eye Disease in Patients of Reproductive Age and during Pregnancy. Ocul. Immunol. Inflamm. 2012, 20, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Ofori, B.; Oraichi, D.; Blais, L.; Rey, E.; Bérard, A. Risk of Congenital Anomalies in Pregnant Users of Non-Steroidal Anti-Inflammatory Drugs: A Nested Case-Control Study. Birth Defects Res. B Dev. Reprod. Toxicol. 2006, 77, 268–279. [Google Scholar] [CrossRef]
- Auer, M.; Brezinka, C.; Eller, P.; Luze, K.; Schweigmann, U.; Schwärzler, P. Prenatal Diagnosis of Intrauterine Premature Closure of the Ductus Arteriosus Following Maternal Diclofenac Application. Ultrasound Obstet. Gynecol. 2004, 23, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Arruti, N.; Rebollo, A.; Mezquita, G.; Alcaine, A.; Andonegui, J. Use of ocular drugs in pregnancy. An. Sist. Sanit. Navar. 2013, 36, 479–487. [Google Scholar] [CrossRef]
- Chawla, S.; Chaudhary, T.; Aggarwal, S.; Maiti, G.D.; Jaiswal, K.; Yadav, J. Ophthalmic Considerations in Pregnancy. Med. J. Armed Forces India 2013, 69, 278–284. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Finn, A.P.; Vajzovic, L. Chapter 11—Treatment of Diabetic Retinopathy in Pregnancy. In Current Management of Diabetic Retinopathy; Baumal, C.R., Duker, J.S., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 115–121. ISBN 978-0-323-48452-7. [Google Scholar]
- Razeghinejad, M.R.M.; Masoumpour, M.M.; Eghbal, M.H.M.; Myers, J.S.M.; Moster, M.R.M. Glaucoma Surgery in Pregnancy: A Case Series and Literature Review. Iran. J. Med. Sci. 2016, 41, 437–445. [Google Scholar]
- Sharma, S.; Wuntakal, R.; Anand, A.; Sharma, T.K.; Downey, G. Pregnancy and the Eye. Obstet. Gynaecol. 2006, 8, 141–146. [Google Scholar] [CrossRef][Green Version]
- Madadi, P.; Koren, G.; Freeman, D.J.; Oertel, R.; Campbell, R.J.; Trope, G.E. Timolol Concentrations in Breast Milk of a Woman Treated for Glaucoma: Calculation of Neonatal Exposure. J. Glaucoma 2008, 17, 329–331. [Google Scholar] [CrossRef]
- Coppens, G.; Stalmans, I.; Zeyen, T. Glaucoma Medication during Pregnancy and Nursing. Bull. Soc. Belge Ophtalmol. 2010, 314, 33–36. [Google Scholar]
- Drake, S.C.; Vajaranant, T.S. Evidence-Based Approaches to Glaucoma Management During Pregnancy and Lactation. Curr. Ophthalmol. Rep. 2016, 4, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Korsch, E.; Grote, A.; Seybold, M.; Soditt, V. Systemic Adverse Effects of Topical Treatment with Brimonidine in an Infant with Secondary Glaucoma. Eur. J. Pediatr. 1999, 158, 685. [Google Scholar] [CrossRef] [PubMed]
- Razeghinejad, M.R. Glaucoma Medications in Pregnancy. Oman J. Ophthalmol. 2018, 11, 195–199. [Google Scholar] [CrossRef]
- Merlob, P.; Litwin, A.; Mor, N. Possible Association between Acetazolamide Administration during Pregnancy and Metabolic Disorders in the Newborn. Eur. J. Obstet. Gynecol. Reprod. Biol. 1990, 35, 85–88. [Google Scholar] [CrossRef]
- Söderman, P.; Hartvig, P.; Fagerlund, C. Acetazolamide Excretion into Human Breast Milk. Br. J. Clin. Pharmacol. 1984, 17, 599–600. [Google Scholar] [CrossRef]
- Hashimoto, Y.; Yamana, H.; Michihata, N.; Shigemi, D.; Ishimaru, M.; Matsui, H.; Yasunaga, H.; Aihara, M. Eye Drops for Dry Eye Disease during Pregnancy and Adverse Neonatal Outcomes: High-Dimensional Propensity Score Analyses. Ophthalmic Epidemiol. 2022, 29, 384–393. [Google Scholar] [CrossRef]
- Razeghinejad, M.R.; Tania Tai, T.Y.; Fudemberg, S.J.; Katz, L.J. Pregnancy and glaucoma. Surv. Ophthalmol. 2011, 56, 324–335. [Google Scholar] [CrossRef]
- Zeisler, J.A.; Gaarder, T.D.; De Mesquita, S.A. Lidocaine Excretion in Breast Milk. Drug Intell. Clin. Pharm. 1986, 20, 691–693. [Google Scholar] [CrossRef]
- Ortega, D.; Viviand, X.; Lorec, A.M.; Gamerre, M.; Martin, C.; Bruguerolle, B. Excretion of Lidocaine and Bupivacaine in Breast Milk Following Epidural Anesthesia for Cesarean Delivery. Acta Anaesthesiol. Scand. 1999, 43, 394–397. [Google Scholar] [CrossRef]
- Almawi, W.Y.; Saldanha, F.L.; Mahmood, N.A.; Al-Zaman, I.; Sater, M.S.; Mustafa, F.E. Relationship between VEGFA Polymorphisms and Serum VEGF Protein Levels and Recurrent Spontaneous Miscarriage. Hum. Reprod. 2013, 28, 2628–2635. [Google Scholar] [CrossRef] [PubMed]
- Polizzi, S.; Mahajan, V.B. Intravitreal Anti-VEGF Injections in Pregnancy: Case Series and Review of Literature. J. Ocul. Pharmacol. Ther. 2015, 31, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Avery, R.L.; Castellarin, A.A.; Steinle, N.C.; Dhoot, D.S.; Pieramici, D.J.; See, R.; Couvillion, S.; Nasir, M.A.; Rabena, M.D.; Le, K.; et al. Systemic Pharmacokinetics Following Intravitreal Injections of Ranibizumab, Bevacizumab or Aflibercept in Patients with Neovascular AMD. Br. J. Ophthalmol. 2014, 98, 1636–1641. [Google Scholar] [CrossRef] [PubMed]
- Petrou, P.; Georgalas, I.; Giavaras, G.; Anastasiou, E.; Ntana, Z.; Petrou, C. Early Loss of Pregnancy after Intravitreal Bevacizumab Injection. Acta Ophthalmol. 2009, 88, e136. [Google Scholar] [CrossRef] [PubMed]
- Sakai, T.; Mori, C.; Ohtsu, F. Potential Safety Signal of Pregnancy Loss with Vascular Endothelial Growth Factor Inhibitor Intraocular Injection: A Disproportionality Analysis Using the Food and Drug Administration Adverse Event Reporting System. Front. Pharmacol. 2022, 13, 1063625. [Google Scholar] [CrossRef]
- Gaudana, R.; Ananthula, H.K.; Parenky, A.; Mitra, A.K. Ocular Drug Delivery. AAPS J. 2010, 12, 348–360. [Google Scholar] [CrossRef]
- Schopf, L.R.; Popov, A.M.; Enlow, E.M.; Bourassa, J.L.; Ong, W.Z.; Nowak, P.; Chen, H. Topical Ocular Drug Delivery to the Back of the Eye by Mucus-Penetrating Particles. Transl. Vis. Sci. Technol. 2015, 4, 11. [Google Scholar] [CrossRef]
- Kowalski, R.P.; Nayyar, S.V.; Romanowski, E.G.; Jhanji, V. Anti-Infective Treatment and Resistance Is Rarely Problematic with Eye Infections. Antibiotics 2022, 11, 204. [Google Scholar] [CrossRef]
- Ramsay, E.; del Amo, E.M.; Toropainen, E.; Tengvall-Unadike, U.; Ranta, V.-P.; Urtti, A.; Ruponen, M. Corneal and Conjunctival Drug Permeability: Systematic Comparison and Pharmacokinetic Impact in the Eye. Eur. J. Pharm. Sci. 2018, 119, 83–89. [Google Scholar] [CrossRef]
- Varela-Fernández, R.; Díaz-Tomé, V.; Luaces-Rodríguez, A.; Conde-Penedo, A.; García-Otero, X.; Luzardo-Álvarez, A.; Fernández-Ferreiro, A.; Otero-Espinar, F. Drug Delivery to the Posterior Segment of the Eye: Biopharmaceutic and Pharmacokinetic Considerations. Pharmaceutics 2020, 12, 269. [Google Scholar] [CrossRef]
- Lam, R.F.; Lai, J.S.M.; Ng, J.S.K.; Rao, S.K.; Law, R.W.K.; Lam, D.S.C. Topical Chloramphenicol for Eye Infections. Hong Kong Med. J. 2002, 8, 44–47. [Google Scholar]
- Nahum, G.G.; Uhl, K.; Kennedy, D.L. Antibiotic Use in Pregnancy and Lactation. Obstet. Gynecol. 2006, 107, 1120–1138. [Google Scholar] [CrossRef]
- Amstey, M.S. Chloramphenicol Therapy in Pregnancy. Clin. Infect. Dis. 2000, 30, 237. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hammerschlag, M.R.; Cummings, C.; Roblin, P.M.; Williams, T.H.; Delke, I. Efficacy of Neonatal Ocular Prophylaxis for the Prevention of Chlamydial and Gonococcal Conjunctivitis. N. Engl. J. Med. 1989, 320, 769–772. [Google Scholar] [CrossRef]
- Cabrera-Aguas, M.; Khoo, P.; Watson, S.L. Infectious Keratitis: A Review. Clin. Exp. Ophthalmol. 2022, 50, 543–562. [Google Scholar] [CrossRef] [PubMed]
- Reginatto, P.; Agostinetto, G.D.J.; Fuentefria, R.D.N.; Marinho, D.R.; Pizzol, M.D.; Fuentefria, A.M. Eye Fungal Infections: A Mini Review. Arch. Microbiol. 2023, 205, 236. [Google Scholar] [CrossRef] [PubMed]
- Behrens-Baumann, W. Topical Antimycotics in Ophthalmology. Ophthalmologica 1997, 211, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, P.; Patil, A.; Majumdar, S. Challenges in the Polyene- and Azole-Based Pharmacotherapy of Ocular Fungal Infections. J. Ocul. Pharmacol. Ther. 2019, 35, 6–22. [Google Scholar] [CrossRef]
- Kaur, I.P.; Kakkar, S. Topical Delivery of Antifungal Agents. Expert Opin. Drug Deliv. 2010, 7, 1303–1327. [Google Scholar] [CrossRef]
- Srinivasan, M. Fungal Keratitis. Curr. Opin. Ophthalmol. 2004, 15, 321–327. [Google Scholar] [CrossRef]
- Sahay, P.; Singhal, D.; Nagpal, R.; Maharana, P.K.; Farid, M.; Gelman, R.; Sinha, R.; Agarwal, T.; Titiyal, J.S.; Sharma, N. Pharmacologic Therapy of Mycotic Keratitis. Surv. Ophthalmol. 2019, 64, 380–400. [Google Scholar] [CrossRef] [PubMed]
- Padberg, S. Anti-Infective Agents. In Drugs During Pregnancy and Lactation; Elsevier: Amsterdam, The Netherlands, 2015; pp. 115–176. [Google Scholar]
- Gonul, S.; Gedik, S.; Ozturk, B.T.; Bakbak, B.; Koktekir, B.E.; Okudan, S.; Dagı, H.T. Postoperative Fungal Endophthalmitis Caused by Trichosporon Asahii Treated with Voriconazole. Arq. Bras. Oftalmol. 2015, 78, 252–254. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Thilagaraj, S.; Zahari, M.; Sarojini, K.; Qamarruddin, F.A. Trichosporon Endophthalmitis Following Cataract Surgery: A Case Report. Cureus 2023, 15, e34067. [Google Scholar] [CrossRef] [PubMed]
- Sigera, L.S.M.; Denning, D.W. Flucytosine and Its Clinical Usage. Ther. Adv. Infect. Dis. 2023, 10, 204993612311613. [Google Scholar] [CrossRef]
- Schardein, J.L.; Hentz, D.L.; Petrere, J.A.; Fitzgerald, J.E.; Kurtz, S.M. The Effect of Vidarabine on the Development of the Offspring of Rats, Rabbits, and Monkeys. Teratology 1977, 15, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Itoi, M. Teratogenicities of Ophthalmic Drugs. Arch. Ophthalmol. 1975, 93, 46. [Google Scholar] [CrossRef]
- Wilhelmus, K.R. Antiviral Treatment and Other Therapeutic Interventions for Herpes Simplex Virus Epithelial Keratitis. Cochrane Database Syst. Rev. 2015, 1, CD002898. [Google Scholar] [CrossRef]
- Al-Badr, A.A.; Ajarim, T.D.S. Ganciclovir. Profiles Drug Subst Excip Relat Methodol. 2018, 43, 1–208. [Google Scholar]
- Contejean, A.; Leruez-Ville, M.; Treluyer, J.-M.; Tsatsaris, V.; Ville, Y.; Charlier, C.; Chouchana, L. Assessing the Risk of Adverse Pregnancy Outcomes and Birth Defects Reporting in Women Exposed to Ganciclovir or Valganciclovir during Pregnancy: A Pharmacovigilance Study. J. Antimicrob. Chemother. 2023, 78, 1265–1269. [Google Scholar] [CrossRef]
- Bouten, M.; Elsheikha, H.M. Diagnosis and Management of Acanthamoeba Keratitis: A Continental Approach. Parasitologia 2022, 2, 167–197. [Google Scholar] [CrossRef]
- Marciano-Cabral, F.; Puffenbarger, R.; Cabral, G.A. The Increasing Importance of Acanthamoeba Infections. J. Eukaryot Microbiol. 2000, 47, 29–36. [Google Scholar] [CrossRef]
- Mazzotta, P.; Loebstein, R.; Koren, G. Treating Allergic Rhinitis in Pregnancy. Drug Saf. 1999, 20, 361–375. [Google Scholar] [CrossRef] [PubMed]
- Kar, S.; Krishnan, A.; Preetha, K.; Mohankar, A. A Review of Antihistamines Used during Pregnancy. J. Pharmacol. Pharmacother. 2012, 3, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Holland, E.J.; Fingeret, M.; Mah, F.S. Use of Topical Steroids in Conjunctivitis: A Review of the Evidence. Cornea 2019, 38, 1062–1067. [Google Scholar] [CrossRef] [PubMed]
- Haydinger, C.D.; Ferreira, L.B.; Williams, K.A.; Smith, J.R. Mechanisms of Macular Edema. Front. Med. 2023, 10, 1128811. [Google Scholar] [CrossRef] [PubMed]
- Gaballa, S.A.; Kompella, U.B.; Elgarhy, O.; Alqahtani, A.M.; Pierscionek, B.; Alany, R.G.; Abdelkader, H. Corticosteroids in Ophthalmology: Drug Delivery Innovations, Pharmacology, Clinical Applications, and Future Perspectives. Drug Deliv. Transl. Res. 2021, 11, 866–893. [Google Scholar] [CrossRef]
- Chiam, N.P.Y.; Lim, L.L.P. Uveitis and Gender: The Course of Uveitis in Pregnancy. J. Ophthalmol. 2014, 2014, 401915. [Google Scholar] [CrossRef]
- Fung, A.T.; Tran, T.; Lim, L.L.; Samarawickrama, C.; Arnold, J.; Gillies, M.; Catt, C.; Mitchell, L.; Symons, A.; Buttery, R.; et al. Local Delivery of Corticosteroids in Clinical Ophthalmology: A Review. Clin. Exp. Ophthalmol. 2020, 48, 366–401. [Google Scholar] [CrossRef]
- Chi, C.C.; Wang, S.-H.; Wojnarowska, F.; Kirtschig, G.; Davies, E.; Bennett, C. Safety of Topical Corticosteroids in Pregnancy. Cochrane Database Syst. Rev. 2015, 2015, CD007346. [Google Scholar] [CrossRef]
- Ballard, P.D.; Hearney, E.F.; Smith, M.B. Comparative Teratogenicity of Selected Glucocorticoids Applied Ocularly in Mice. Teratology 1977, 16, 175–180. [Google Scholar] [CrossRef]
- Frier, E.M.; Lin, C.; Reynolds, R.M.; Allegaert, K.; Been, J.V.; Fraser, A.; Gissler, M.; Einarsdóttir, K.; Florian, L.; Jacobsson, B.; et al. Consortium for the Study of Pregnancy Treatments (Co-OPT): An International Birth Cohort to Study the Effects of Antenatal Corticosteroids. PLoS ONE 2023, 18, e0282477. [Google Scholar] [CrossRef] [PubMed]
- Chi, C.C.; Mayon-White, R.T.; Wojnarowska, F.T. Safety of Topical Corticosteroids in Pregnancy: A Population-Based Cohort Study. J. Investig. Dermatol. 2011, 131, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.Y.; Kwok, A.K.H.; Chung, K.L. Use of Ophthalmic Medications during Pregnancy. Hong Kong Med. J. 2004, 10, 191–195. [Google Scholar] [PubMed]
- Hashimoto, Y.; Michihata, N.; Yamana, H.; Shigemi, D.; Morita, K.; Matsui, H.; Yasunaga, H.; Aihara, M. Ophthalmic Corticosteroids in Pregnant Women with Allergic Conjunctivitis and Adverse Neonatal Outcomes: Propensity Score Analyses. Am. J. Ophthalmol. 2020, 220, 91–101. [Google Scholar] [CrossRef]
- Degenring, R.F.; Jonas, J.B. Serum Levels of Triamcinolone Acetonide after Intravitreal Injection. Am. J. Ophthalmol. 2004, 137, 1142–1143. [Google Scholar] [CrossRef]
- Chang-Lin, J.-E.; Attar, M.; Acheampong, A.A.; Robinson, M.R.; Whitcup, S.M.; Kuppermann, B.D.; Welty, D. Pharmacokinetics and Pharmacodynamics of a Sustained-Release Dexamethasone Intravitreal Implant. Investig. Opthalmol. Vis. Sci. 2011, 52, 80. [Google Scholar] [CrossRef]
- Juthani, V.V.; Clearfield, E.; Chuck, R.S. Non-Steroidal Anti-Inflammatory Drugs versus Corticosteroids for Controlling Inflammation after Uncomplicated Cataract Surgery. Cochrane Database Syst. Rev. 2017, 7, CD010516. [Google Scholar] [CrossRef]
- Farkouh, A.; Frigo, P.; Czejka, M. Systemic Side Effects of Eye Drops: A Pharmacokinetic Perspective. Clin. Ophthalmol. 2016, 10, 2433–2441. [Google Scholar] [CrossRef]
- Antonucci, R.; Zaffanello, M.; Puxeddu, E.; Porcella, A.; Cuzzolin, L.; Pilloni, M.D.; Fanos, V. Use of Non-Steroidal Anti-Inflammatory Drugs in Pregnancy: Impact on the Fetus and Newborn. Curr. Drug Metab. 2012, 13, 474–490. [Google Scholar] [CrossRef]
- Shinomiya, K.; Kajima, M.; Tajika, H.; Shiota, H.; Nakagawa, R.; Saijyou, T. Renal Failure Caused by Eyedrops Containing Phenylephrine in a Case of Retinopathy of Prematurity. J. Med. Investig. 2003, 50, 203–206. [Google Scholar]
- Qureshi, I.A. Intraocular Pressure and Pregnancy: A Comparison between Normal and Ocular Hypertensive Subjects. Arch Med. Res. 1997, 28, 397–400. [Google Scholar] [PubMed]
- Horven, I.; Gjonnaess, H. Corneal Indentation Pulse and Intraocular Pressure in Pregnancy. Arch. Ophthalmol. 1974, 91, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Patil, A.D.; Ellabban, A.A.; Patil, D.B.; Yorston, D.; Williamson, T.H.; Laidlaw, D.A.; Vize, C.J.; Hingorani, M.; Morris, E.P. Ocular Manifestations of Pregnancy and Labour: From the Innocuous to the Sight Threatening. Obstet. Gynaecol. 2020, 22, 217–226. [Google Scholar] [CrossRef]
- Rubin, P.C. Current Concepts: Beta-Blockers in Pregnancy. N. Engl. J. Med. 1981, 305, 1323–1326. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.-D.; Hu, C.-C.; Lin, H.-C. Antiglaucoma Medications during Pregnancy and the Risk of Low Birth Weight: A Population-Based Study. Br. J. Ophthalmol. 2009, 93, 1283–1286. [Google Scholar] [CrossRef] [PubMed]
- Netland, P.A.; Tanna, A.P. Glaucoma Medical Therapy: Principles and Management; Kugler Publications: Amsterdam, The Netherlands, 2020; ISBN 9062999328. [Google Scholar]
- Rowe, J.A.; Hattenhauer, M.G.; Herman, D.C. Adverse Side Effects Associated with Latanoprost. Am. J. Ophthalmol. 1997, 124, 683–685. [Google Scholar] [CrossRef]
- Alm, A. Latanoprost in the Treatment of Glaucoma. Clin. Ophthalmol. 2014, 8, 1967–1985. [Google Scholar] [CrossRef]
- Thomas, R.; Parikh, R.; Sood, D.; Vijaya, L.; Sekhar, G.C.; Sood, N.N.; Baskaran, M.; Prasad, K.K. Efficacy and Safety of Latanoprost for Glaucoma Treatment: A Three-Month Multicentric Study in India. Indian J. Ophthalmol. 2005, 53, 23–30. [Google Scholar] [CrossRef]
- Johnson, S.M.; Martinez, M.; Freedman, S. Management of Glaucoma in Pregnancy and Lactation. Surv. Ophthalmol. 2001, 45, 449–454. [Google Scholar] [CrossRef]
- De Santis, M.; De Lucchese, A.; Carducci, B.; Cavaliere, A.F.; De Santis, L.; Merola, A.; Straface, G.; Caruso, A. Latanoprost Exposure in Pregnancy. Am. J. Ophthalmol. 2004, 138, 305–306. [Google Scholar] [CrossRef]
- Carlsen, J.O.; Zabriskie, N.A.; Kwon, Y.H.; Barbe, M.E.; Scott, W.E. Apparent Central Nervous System Depression in Infants after the Use of Topical Brimonidine. Am. J. Ophthalmol. 1999, 128, 255–256. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, T.J.; Kooner, K.S. Clinical Pathways in Glaucoma; Thieme: New York, NY, USA, 2001; ISBN 0865779198. [Google Scholar]
- Gotovac, M.; Kastelan, S.; Lukenda, A. Eye and Pregnancy. Coll. Antropol. 2013, 37 (Suppl. S1), 189–193. [Google Scholar]
- Soma-Pillay, P.; Nelson-Piercy, C.; Tolppanen, H.; Mebazaa, A. Physiological Changes in Pregnancy. Cardiovasc. J. Afr. 2016, 27, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Ibraheem, W.A.; Ibraheem, A.B.; Tjani, A.M.; Oladejo, S.; Adepoju, S.; Folohunso, B. Tear Film Functions and Intraocular Pressure Changes in Pregnancy. Afr. J. Reprod. Health 2015, 19, 118–122. [Google Scholar] [PubMed]
- Nkiru, Z.N.; Stella, O.; Udeh, N.; Polycarp, U.A.; Daniel, C.N.; Ifeoma, R.E. Dry Eye Disease: A Longitudinal Study among Pregnant Women in Enugu, South East, Nigeria. Ocul. Surf. 2019, 17, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Fujinaga, M.; Mazze, R.I. Reproductive and Teratogenic Effects of Lidocaine in Sprague-Dawley Rats. Anesthesiology 1986, 65, 626–632. [Google Scholar] [CrossRef]
- Dryden, R.M.; Lo, M.W. Breast Milk Lidocaine Levels in Tumescent Liposuction. Plast. Reconstr. Surg. 2000, 105, 2267–2268. [Google Scholar] [CrossRef]
- Mazzuca, D.; Demarinis, G.; Della Corte, M.; Caputo, F.; Caruso, A.; Pallocci, M.; Marsella, L.T.; Tatti, F.; Pintor, E.S.; Mangoni, L.; et al. Intravitreal Injection Planning during COVID-19 Pandemic: A Retrospective Study of Two Tertiary University Centers in Italy. Healthcare 2023, 11, 287. [Google Scholar] [CrossRef]
- Cordero Coma, M.; Sobrin, L.; Onal, S.; Christen, W.; Foster, C.S. Intravitreal Bevacizumab for Treatment of Uveitic Macular Edema. Ophthalmology 2007, 114, 1574.e1–1579.e1. [Google Scholar] [CrossRef]
- Avery, R.L.; Pearlman, J.; Pieramici, D.J.; Rabena, M.D.; Castellarin, A.A.; Nasir, M.A.; Giust, M.J.; Wendel, R.; Patel, A. Intravitreal Bevacizumab (Avastin) in the Treatment of Proliferative Diabetic Retinopathy. Ophthalmology 2006, 113, 1695.e6–1705.e6. [Google Scholar] [CrossRef]
- Traversi, C.; Nuti, E.; Marigliani, D.; Cevenini, G.; Balestrazzi, A.; Martone, G.; Caporossi, T.; Tosi, G.M. Forty-Two-Month Outcome of Intravitreal Bevacizumab in Myopic Choroidal Neovascularization. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, N. Role of Vascular Endothelial Growth Factor in Regulation of Physiological Angiogenesis. Am. J. Physiol. Cell Physiol. 2001, 280, C1358–C1366. [Google Scholar] [CrossRef] [PubMed]
- Galazios, G.; Papazoglou, D.; Tsikouras, P.; Kolios, G. Vascular Endothelial Growth Factor Gene Polymorphisms and Pregnancy. J. Matern. Fetal Neonatal Med. 2009, 22, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Gómez Ledesma, I.; de Santiago Rodríguez, M.Á.; Follana Neira, I.; León Garrigosa, F. Membrana Neovascular y Embarazo. Tratamiento Con Bevacizumab. Arch. Soc. Esp. Oftalmol. 2012, 87, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, L.; Kelly, S.P.; Glenn, A.; Williams, C.P.R.; McKibbin, M. Intravitreal Bevacizumab Injection in Unrecognised Early Pregnancy. Eye 2014, 28, 492–494. [Google Scholar] [CrossRef] [PubMed]
- Rosen, E.; Rubowitz, A.; Ferencz, J.R. Exposure to Verteporfin and Bevacizumab Therapy for Choroidal Neovascularization Secondary to Punctate Inner Choroidopathy during Pregnancy. Eye 2009, 23, 1479. [Google Scholar] [CrossRef] [PubMed]
- Tarantola, R.M.; Folk, J.C.; Boldt, H.C.; Mahajan, V.B. Intravitreal Bevacizumab during Pregnancy. Retina 2010, 30, 1405–1411. [Google Scholar] [CrossRef]
- Introini, U.; Casalino, G.; Cardani, A.; Scotti, F.; Finardi, A.; Candiani, M.; Bandello, F. Intravitreal Bevacizumab for a Subfoveal Myopic Choroidal Neovascularization in the First Trimester of Pregnancy. J. Ocul. Pharmacol. Ther. 2012, 28, 553–555. [Google Scholar] [CrossRef]
- Sarhianaki, A.; Katsimpris, A.; Petropoulos, I.; Livieratou, A.; Theoulakis, P.; Katsimpris, J. Intravitreal Administration of Ranibizumab for Idiopathic Choroidal Neovascularization in a Pregnant Woman. Klin. Monatsblätter Augenheilkd. 2012, 229, 451–453. [Google Scholar] [CrossRef]
- Jouve, L.; Akesbi, J.; Nordmann, J.-P. Safety and Efficacy of Ranibizumab for Pregnant Women in Idiopathic Choroidal Neovascularization. Acta Ophthalmol. 2015, 93, e597–e598. [Google Scholar] [CrossRef]
- Akkaya, S. Early Miscarriage Occurring Six Days After Intravitreal Ranibizumab Injection. Med. Hypothesis Discov. Innov. Ophthalmol. 2019, 8, 69–72. [Google Scholar] [PubMed]
- Schmidt-Erfurth, U.; Lang, G.E.; Holz, F.G.; Schlingemann, R.O.; Lanzetta, P.; Massin, P.; Gerstner, O.; Bouazza, A.S.; Shen, H.; Osborne, A.; et al. Three-Year Outcomes of Individualized Ranibizumab Treatment in Patients with Diabetic Macular Edema. Ophthalmology 2014, 121, 1045–1053. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Eye | Disease | Pregnancy | ||
|---|---|---|---|---|
| “eye” OR “ophthalmology” OR “eye drops” OR “ocular diseases” OR “ocular drugs” OR “ocular medication” | AND | “glaucoma” OR “uveitis” OR “ocular infection” OR “conjunctivitis” OR “keratitis” OR “retinopathy” OR “diabetic retinopathy” OR “maculopathy” OR “mydriatics” OR “anti-inflammatory” OR “ocular anesthesia” | AND | “pregnancy” OR “breastfeeding” OR lactation” OR “fetal risk” |
| Drug Family | Drug | Admin. | Ref. | Toxicity in Pregnancy | Recommendation | Ref. | Toxicity in Lactation | Recommendation |
|---|---|---|---|---|---|---|---|---|
| Anti-Infective Medications | ||||||||
| Antibiotics | Polymyxin B | Topical | [10] | Studied in systemic administration: no congenital defects. Possible nephrotoxicity. | Probably Safe | [10] | Studied in systemic administration: None | Safe |
| Chloramphenicol | Topical | [11] | No congenital defects. | Safe | [10] | Vomiting, meteorism. | Contraindicated | |
| Erythromycin | Topical | [10] | Studied in systemic administration: no congenital defects. Possible hepatoxicity. | Probably Safe | [12,13] | Studied in systemic administration- | Safe | |
| Fluoroquinolones | Topical | [14] | Studied in systemic administration: no congenital defects. Mechanism of action based on alterations of DNA synthesis. | Caution | N/A | N/A | Caution | |
| Tetracyclines | Topical | [15] | Studied in systemic administration: color alteration of deciduous teeth; bone growth inhibition. | Caution | [12] | Studied in systemic administration: color alterations in deciduous teeth; bone growth inhibition. | Caution | |
| Antimycotics | Amphotericin B | Topical | [16] | No congenital defects | Safe | [16] | No adverse effects. | Safe |
| Voriconazole | Topical | [16] | Animal studies: Teratogenic. | Contraindicated | N/A | N/A | Contraindicated | |
| 5-fluorocytosine | Systemic | [16] | Animal studies: Teratogenic. | Contraindicated | [16] | N/A | Contraindicated | |
| Natamycin | Topical | [17] | Studied in vaginal administration: No congenital defects. | Caution | N/A | N/A | Caution | |
| Antivirals | Acyclovir | Topical | [18,19] | No congenital defects. | Safe | N/A | N/A | Probably Safe |
| Ganciclovir | Topical | N/A | N/A | Contraindicated | [20,21] | Animal studies: adverse effects on the offspring. | Contraindicated | |
| Antimoebic | Biguanides and diamidines | Systemic | N/A | N/A | Contraindicated | N/A | N/A | Contraindicated |
| Antihistamines | ||||||||
| Antihistamines | Systemic/ Topical | N/A | N/A | Contraindicated | N/A | N/A | Contraindicated | |
| Anti-inflammatory Medications | ||||||||
| Corticosteroids | Dexamethasone | Intravitreal | [22] | No congenital defects. More evidence is required | Contraindicated | N/A | N/A | Contraindicated |
| Prednisone | Topical | [23] | No congenital defects. 10–13% cross the placenta. | Caution | [23] | No adverse effects. | Probably Safe | |
| Immunosuppressive | Methotrexate and alkylating agents | Systemic | [23] | Teratogenic. | Contraindicated | N/A | N/A | Contraindicated |
| Azathioprine and cyclosporin | Systemic/Topical | N/A | N/A | Caution | N/A | N/A | Caution | |
| NSAIDs | Ibuprofen, naproxen and indomethacin | Topical | [24,25] | Avoid early and in third trimester of pregnancy | Contraindicated | [13] | No adverse effects | Safe |
| Mydriatics | ||||||||
| Parasympatholytic | Tropicamide | Topical | [26] | Not recommended in 1st trimester | Probably Safe | N/A | N/A | Probably Safe |
| Atropine and homatropine | Topical | [27,28] | Studied in systemic administration: Minor fetal malformations. | Caution | N/A | N/A | Caution | |
| Sympathomimetic | Phenylephrine | Topical | [27] | Generally considered safe. Not recommended in 1st trimester. Case report of renal failure. Studied in systemic administration: Minor fetal malformations. | Caution | N/A | N/A | Caution |
| Ocular Anti-Hypertensive Medications | ||||||||
| Beta-blockers | Topical | [29,30] | Suspend 2–3 days before delivery or keep newborns under observation | Safe | [31] | No adverse effects | Safe | |
| Prostaglandin analogues | Topical | [32] | Theoretically increase uterine tone and induce premature labor; unlikely with ophthalmic dosage | Caution | [33] | No evidence to support the use | Caution | |
| 2-adrenergic agonists | Topical | [34] | Animal studies: No congenital defects. To be discontinued before labor. | Safe | [35] | Risk of apnea or hypotension | Contraindicated | |
| Carbonic anhydrase inhibitors | Topical | [36] | N/A | Contraindicated | [37] | N/A | Contraindicated | |
| Tear Substitutes | ||||||||
| Hyaluronate 0.1–0.3% | Topical | [38] | No congenital defects | Safe | N/A | N/A | Safe | |
| Diquafosol | Topical | [38] | No congenital defects | Safe | N/A | N/A | Safe | |
| Anesthetics | ||||||||
| Lidocaine, prilocaine and editocaine | Local | [39] | No congenital defects | Probably Safe | [40] | No adverse effects. | Probably Safe | |
| Bupivacaine and mepivacaine | Local | [29] | Fetal bradycardia. | Caution | [41] | No adverse effects for bupivacaine | Probably Safe | |
| Others | Topical | N/A | N/A | Contraindicated | N/A | N/A | Contraindicated | |
| Anti-VEGF Injections | ||||||||
| Ranibizumab | Intravitreal | [42] | Minimal effect on plasma VEGF, 1 case report of miscarriage during first week of pregnancy. | Caution | N/A | N/A | Probably Safe | |
| Bavacizumab | Intravitreal | [43,44,45] | Several cases of miscarriage, 1 case of pre-eclampsia | Contraindicated | N/A | N/A | Contraindicated | |
| Aflibercept | Intravitreal | [46] | N/A | Contraindicated | N/A | N/A | Contraindicated | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demarinis, G.; Tatti, F.; Taloni, A.; Giugliano, A.V.; Panthagani, J.; Myerscough, J.; Peiretti, E.; Giannaccare, G. Treatments for Ocular Diseases in Pregnancy and Breastfeeding: A Narrative Review. Pharmaceuticals 2023, 16, 1433. https://doi.org/10.3390/ph16101433
Demarinis G, Tatti F, Taloni A, Giugliano AV, Panthagani J, Myerscough J, Peiretti E, Giannaccare G. Treatments for Ocular Diseases in Pregnancy and Breastfeeding: A Narrative Review. Pharmaceuticals. 2023; 16(10):1433. https://doi.org/10.3390/ph16101433
Chicago/Turabian StyleDemarinis, Giuseppe, Filippo Tatti, Andrea Taloni, Antonio Valentino Giugliano, Jesse Panthagani, James Myerscough, Enrico Peiretti, and Giuseppe Giannaccare. 2023. "Treatments for Ocular Diseases in Pregnancy and Breastfeeding: A Narrative Review" Pharmaceuticals 16, no. 10: 1433. https://doi.org/10.3390/ph16101433
APA StyleDemarinis, G., Tatti, F., Taloni, A., Giugliano, A. V., Panthagani, J., Myerscough, J., Peiretti, E., & Giannaccare, G. (2023). Treatments for Ocular Diseases in Pregnancy and Breastfeeding: A Narrative Review. Pharmaceuticals, 16(10), 1433. https://doi.org/10.3390/ph16101433