
Response to Anti-PD1/L1 Antibodies in Advanced Urothelial Cancer in the ‘Real-Life’ Setting

 ,
,
Abstract
1. Introduction
2. Results
3. Methods
3.1. Patients
3.2. Endpoints
3.3. Definitions of Response and Toxicity
3.4. Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nanda, R.; Chow, L.Q.M.; Dees, E.C.; Berger, R.; Gupta, S.; Geva, R.; Pusztai, L.; Pathiraja, K.; Aktan, G.; Cheng, J.D.; et al. Pembrolizumab in Patients With Advanced Triple-Negative Breast Cancer: Phase Ib KEYNOTE-012 Study. J. Clin. Oncol. 2016, 34, 2460–2467. [Google Scholar] [CrossRef] [PubMed]
- Pembrolizumab (MK-3475) for Advanced Urothelial Cancer: Updated Results and Biomarker Analysis from KEYNOTE-012. | 2015 ASCO Annual Meeting | Abstracts | Meeting Library. Available online: http://meetinglibrary.asco.org/content/147894-156 (accessed on 2 February 2016).
- Muro, K.; Chung, H.C.; Shankaran, V.; Geva, R.; Catenacci, D.; Gupta, S.; Eder, J.P.; Golan, T.; Le, D.T.; Burtness, B.; et al. Pembrolizumab for patients with PD-L1-positive advanced gastric cancer (KEYNOTE-012): A multicentre, open-label, phase 1b trial. Lancet Oncol. 2016, 17, 717–726. [Google Scholar] [CrossRef]
- Plimack, E.R.; Bellmunt, J.; Gupta, S.; Berger, R.; Chow, L.Q.M.; Juco, J.; Lunceford, J.; Saraf, S.; Perini, R.F.; O’Donnell, P.H. Safety and activity of pembrolizumab in patients with locally advanced or metastatic urothelial cancer (KEYNOTE-012): A non-randomised, open-label, phase 1b study. Lancet Oncol. 2017, 18, 212–220. [Google Scholar] [CrossRef]
- Seiwert, T.Y.; Burtness, B.; Mehra, R.; Weiss, J.; Berger, R.; Eder, J.P.; Heath, K.; McClanahan, T.; Lunceford, J.; Gause, C.; et al. Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-012): An open-label, multicentre, phase 1b trial. Lancet Oncol. 2016, 17, 956–965. [Google Scholar] [CrossRef]
- Rosenberg, J.E.; Hoffman-Censits, J.; Powles, T.; van der Heijden, M.S.; Balar, A.V.; Necchi, A.; Dawson, N.; O’Donnell, P.H.; Balmanoukian, A.; Loriot, Y.; et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: A single-arm, multicentre, phase 2 trial. Lancet 2016, 387, 1909–1920. [Google Scholar] [CrossRef]
- Powles, T.; Durán, I.; Van Der Heijden, M.S.; Loriot, Y.; Vogelzang, N.J.; De Giorgi, U.; Oudard, S.; Retz, M.M.; Castellano, D.; Bamias, A.; et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): A multicentre, open-label, phase 3 randomised controlled trial. Lancet 2018, 391, 748–757. [Google Scholar] [CrossRef]
- Bellmunt, J.; De Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.-L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [PubMed]
- Grivas, P.; Plimack, E.; Balar, A.; Castellano, D.; O’Donnell, P.; Bellmunt, J.; Powles, T.; Hahn, N.; De Wit, R.; Bajorin, D.; et al. Pembrolizumab (pembro) as first-line therapy in cisplatin-ineligible advanced urothelial cancer (UC): Outcomes from KEYNOTE-052 in senior patients (pts) with poor performance status. Ann. Oncol. 2017, 28, v301. [Google Scholar] [CrossRef]
- Bellmunt, J.; Balar, A.; Galsky, M.; Loriot, Y.; Theodore, C.; Pulido, E.G.; Castellano, D.; Retz, M.; Niegisch, G.; Bracarda, S.; et al. IMvigor210: Updated analyses of first-line (1L) atezolizumab (atezo) in cisplatin (cis)-ineligible locally advanced/metastatic urothelial carcinoma (mUC). Ann. Oncol. 2016, 27 (Suppl. 6), vi266–vi295. [Google Scholar] [CrossRef]
- Food and Drug Administration. FDA Limits the Use of Tecentriq and Keytruda for Some Urothelial Cancer Patients. Available online: https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm612484.htm (accessed on 15 August 2022).
- Feld, E.; Harton, J.; Meropol, N.J.; Adamson, B.J.; Cohen, A.; Parikh, R.B.; Galsky, M.D.; Narayan, V.; Christodouleas, J.; Vaughn, D.J.; et al. Effectiveness of First-line Immune Checkpoint Blockade Versus Carboplatin-based Chemotherapy for Metastatic Urothelial Cancer. Eur. Urol. 2019, 76, 524–532. [Google Scholar] [CrossRef]
- Karim, S.; Xu, Y.; Kong, S.; Abdel-Rahman, O.; Quan, M.; Cheung, W. Generalisability of Common Oncology Clinical Trial Eligibility Criteria in the Real World. Clin. Oncol. 2019, 31, e160–e166. [Google Scholar] [CrossRef] [PubMed]
- Simeone, J.C.; Nordstrom, B.L.; Patel, K.; Mann, H.; Klein, A.B.; Horne, L. Treatment patterns and overall survival in metastatic urothelial carcinoma in a real-world, US setting. Cancer Epidemiology 2019, 60, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Khaki, A.R.; Li, A.; Diamantopoulos, L.N.; Bilen, M.A.; Santos, V.; Esther, J.; Morales-Barrera, R.; Devitt, M.; Nelson, A.; Do, C.J.H.; et al. Impact of performance status on treatment outcomes: A real-world study of advanced urothelial cancer treated with immune checkpoint inhibitors. Cancer 2019, 126, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Necchi, A.; Fradet, Y.; Bellmunt, J.; De Wit, R.; Lee, J.-L.; Fong, L.; Vozelgang, N.; Climent, M.; Petrylak, D.; Choueiri, T.; et al. Three-year follow-up from the phase III KEYNOTE-045 trial: Pembrolizumab (Pembro) versus investigator’s choice (paclitaxel, docetaxel, or vinflunine) in recurrent, advanced urothelial cancer (UC). Ann. Oncol. 2019, 30, v366–v367. [Google Scholar] [CrossRef]
- Fishman, M. Commentary: 2-year follow up of pembrolizumab as second-line therapy for advanced urothelial cancer (“KEYNOTE 045”). Transl. Androl. Urol. 2019, 8, 409–413. [Google Scholar] [CrossRef]
- Lista, A.G.D.L.; van Dijk, N.; Rueda, G.D.V.O.D.; Necchi, A.; Lavaud, P.; Morales-Barrera, R.; Gordoa, T.A.; Maroto, P.; Ravaud, A.; Durán, I.; et al. Clinical outcome after progressing to frontline and second-line Anti–PD-1/PD-L1 in advanced urothelial cancer. Eur. Urol. 2020, 77, 269–276. [Google Scholar] [CrossRef]
- Parikh, R.B.; Feld, E.; Galsky, M.D.; Adamson, B.J.; Cohen, A.B.; Baxi, S.S.; Ben Boursi, S.; Christodouleas, J.P.; Vaughn, D.J.; Meropol, N.J.; et al. First-line immune checkpoint inhibitor use in cisplatin-eligible patients with advanced urothelial carcinoma: A secular trend analysis. Futur. Oncol. 2019, 16, 4341–4345. [Google Scholar] [CrossRef]
- Soria, F.; Beleni, A.I.; D’Andrea, D.; Resch, I.; Gust, K.M.; Gontero, P.; Shariat, S.F. Pseudoprogression and hyperprogression during immune checkpoint inhibitor therapy for urothelial and kidney cancer. World J. Urol. 2018, 36, 1703–1709. [Google Scholar] [CrossRef]
- Adashek, J.J.; Kato, S.; Ferrara, R.; Russo, G.L.; Kurzrock, R. Hyperprogression and Immune Checkpoint Inhibitors: Hype or Progress? Oncologist 2020, 25, 94–98. [Google Scholar] [CrossRef]
- Kato, S.; Goodman, A.; Walavalkar, V.; Barkauskas, D.A.; Sharabi, A.; Kurzrock, R. Hyperprogressors after Immunotherapy: Analysis of Genomic Alterations Associated with Accelerated Growth Rate. Clin. Cancer Res. 2017, 23, 4242–4250. [Google Scholar] [CrossRef]
- Champiat, S.; Ferrara, R.; Massard, C.; Besse, B.; Marabelle, A.; Soria, J.-C.; Ferté, C. Hyperprogressive disease: Recognizing a novel pattern to improve patient management. Nat. Rev. Clin. Oncol. 2018, 15, 748–762. [Google Scholar] [CrossRef] [PubMed]
- Denis, M.; Duruisseaux, M.; Brevet, M.; Dumontet, C. How Can Immune Checkpoint Inhibitors Cause Hyperprogression in Solid Tumors? Front. Immunol. 2020, 11, 492. [Google Scholar] [CrossRef] [PubMed]
- Saxman, S.B.; Propert, K.J.; Einhorn, L.H.; Crawford, E.D.; Tannock, I.; Raghavan, D.; Loehrer, P.J.; Trump, D. Long-term follow-up of a phase III intergroup study of cisplatin alone or in combination with methotrexate, vinblastine, and doxorubicin in patients with metastatic urothelial carcinoma: A cooperative group study. J. Clin. Oncol. 1997, 15, 2564–2569. [Google Scholar] [CrossRef]
- Sengeløv, L.; Kamby, C.; Geertsen, P.; Andersen, L.J.; von der Maase, H. Predictive factors of response to cisplatin-based chemotherapy and the relation of response to survival in patients with metastatic urothelial cancer. Cancer Chemother. Pharmacol. 2000, 46, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Heng, D.Y.; Xie, W.; Regan, M.M.; Harshman, L.C.; A Bjarnason, G.; Vaishampayan, U.N.; Mackenzie, M.; Wood, L.; Donskov, F.; Tan, M.-H.; et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: A population-based study. Lancet Oncol. 2013, 14, 141–148. [Google Scholar] [CrossRef]
- Arend, R.; Van Arsdale, A.; Gojayev, A.; Roane, B.M.; Doo, D.; Leath, C.; Goldberg, G.L.; Huang, G. Neutrophilia and mortality in women with uterine carcinosarcoma. Int. J. Gynecol. Cancer 2019, 29, 1258–1263. [Google Scholar] [CrossRef]
- Schernberg, A.; Mezquita, L.; Boros, A.; Botticella, A.; Caramella, C.; Besse, B.; Escande, A.; Planchard, D.; Le Péchoux, C.; Deutsch, E. Neutrophilia as prognostic biomarker in locally advanced stage III lung cancer. PLoS ONE 2018, 13, e0204490. [Google Scholar] [CrossRef]
- Diefenhardt, M.; Hofheinz, R.-D.; Martin, D.; Beißbarth, T.; Arnold, D.; Hartmann, A.; von der Grün, J.; Grützmann, R.; Liersch, T.; Ströbel, P.; et al. Leukocytosis and neutrophilia as independent prognostic immunological biomarkers for clinical outcome in the CAO/ARO/AIO-04 randomized phase 3 rectal cancer trial. Int. J. Cancer 2019, 145, 2282–2291. [Google Scholar] [CrossRef]
- Leibowitz-Amit, R.; Israel, A.; Gal, M.; Atenafu, E.; Symon, Z.; Portnoy, O.; Laufer, M.; Dotan, Z.; Ramon, J.; Avni, D.; et al. Association between the Absolute Baseline Lymphocyte Count and Response to Neoadjuvant Platinum-based Chemotherapy in Muscle-invasive Bladder Cancer. Clin. Oncol. 2016, 28, 790–796. [Google Scholar] [CrossRef]
- Yip, S.M.; Kaiser, J.; Li, H.; North, S.; Heng, D.Y.; Alimohamed, N.S. Real-world Outcomes in Advanced Urothelial Cancer and the Role of Neutrophil to Lymphocyte Ratio. Clin. Genitourin. Cancer 2018, 16, e637–e644. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | N | % | |
|---|---|---|---|
| Sex | Male | 77 | 82 |
| Female | 17 | 18 | |
| Histology | Pure urothelial | 80 | 85 |
| Mixed | 8 | 9 | |
| Predominantly squamous | 4 | 4 | |
| Other | 2 | 2 | |
| Primary site | Bladder | 72 | 77 |
| Upper tract | 16 | 17 | |
| Bladder + Upper tract | 6 | 6 | |
| Sites of metastasis | Visceral (soft tissue in pelvis or metastatic) | 57 | 61 |
| LNs only | 10 | 11 | |
| Bones (with or without other sites) | 27 | 29 | |
| Metastatic at presentation | No | 61 | 65 |
| Yes | 33 | 35 | |
| Definitive treatment | Surgery | 34 | 36 |
| RT | 13 | 14 | |
| Surgery + RT | 2 | 2 | |
| Not applicable/unknown | 44 | 47 | |
| Prior neo-adjuvant/adjuvant chemo | Yes | 28 | 30 |
| No | 66 | 70 | |
| # of previous chemotherapy lines | 0 | 14 | 15 |
| 1 | 57 | 61 | |
| 2 or more | 23 | 24 | |
| ECOG PS | 0/1 | 24 | 25 |
| 2 | 26 | 28 | |
| 3/4 | 44 | 47 | |
| Characteristic | Median | Range | |
| Age (years) | 71.8 | 43.7–95.7 | |
| Hemoglobin (gr/dL) | 10.3 | 7–15.5 | |
| WBC (K/microL) | 7.2 | 2.3–37.3 | |
| Platelets (K/microL) | 235 | 16–668 | |
| Neutrophils (K/microL) | 4.6 | 1.5–35.8 | |
| Lymphocytes (K/microL) | 1.1 | 0.25–6.0 | |
| LDH (IU/L) | 218 | 114–7143 | |
| Alkaline phosphatase (IU/L) | 120 | 37–1993 | |
| Albumin (gr/dL) | 3.5 | 2.1–6.3 | |
| Treatment Characteristics | N | % | |
|---|---|---|---|
| IO type | Pembrolizumab | 67 | 71 |
| Atezolizumab | 19 | 20 | |
| Nivolumab | 3 | 3 | |
| Durvalumab | 1 | 1 | |
| Anti-PD1 + Other | 4 | 4 | |
| Median # of IO cycles | 3 | Range 1–43 | |
| Reasons for discontinuation | Death | 19 | 20 |
| Deterioration (clinical and/or radiological) | 56 | 60 | |
| Complete response | 4 | 4 | |
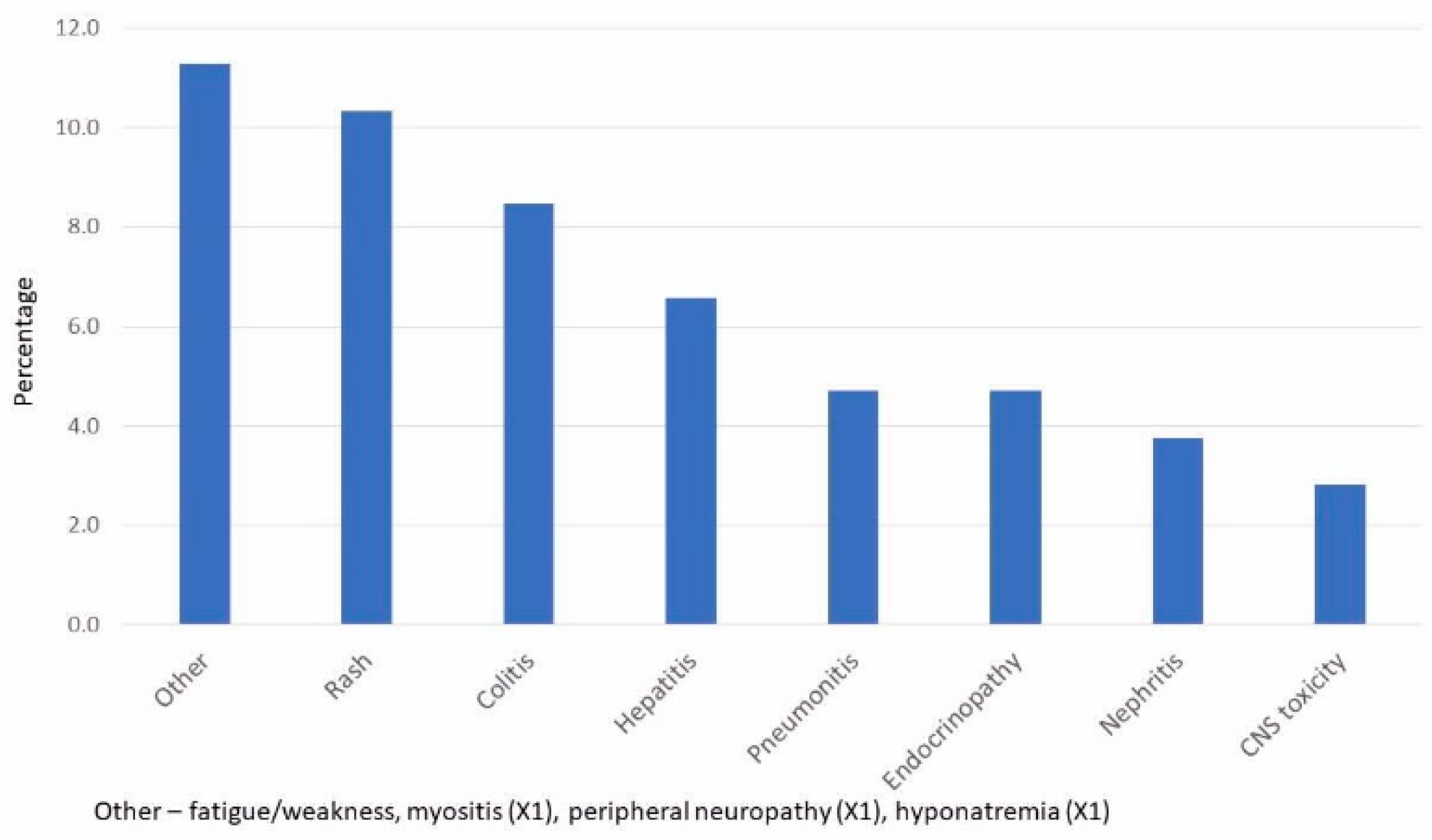
| Toxicity | 7 | 7 | |
| NA-still on treatment | 8 | 9 | |
| Received steroids for toxicity | No | 62 | 66 |
| Yes | 32 | 34 | |
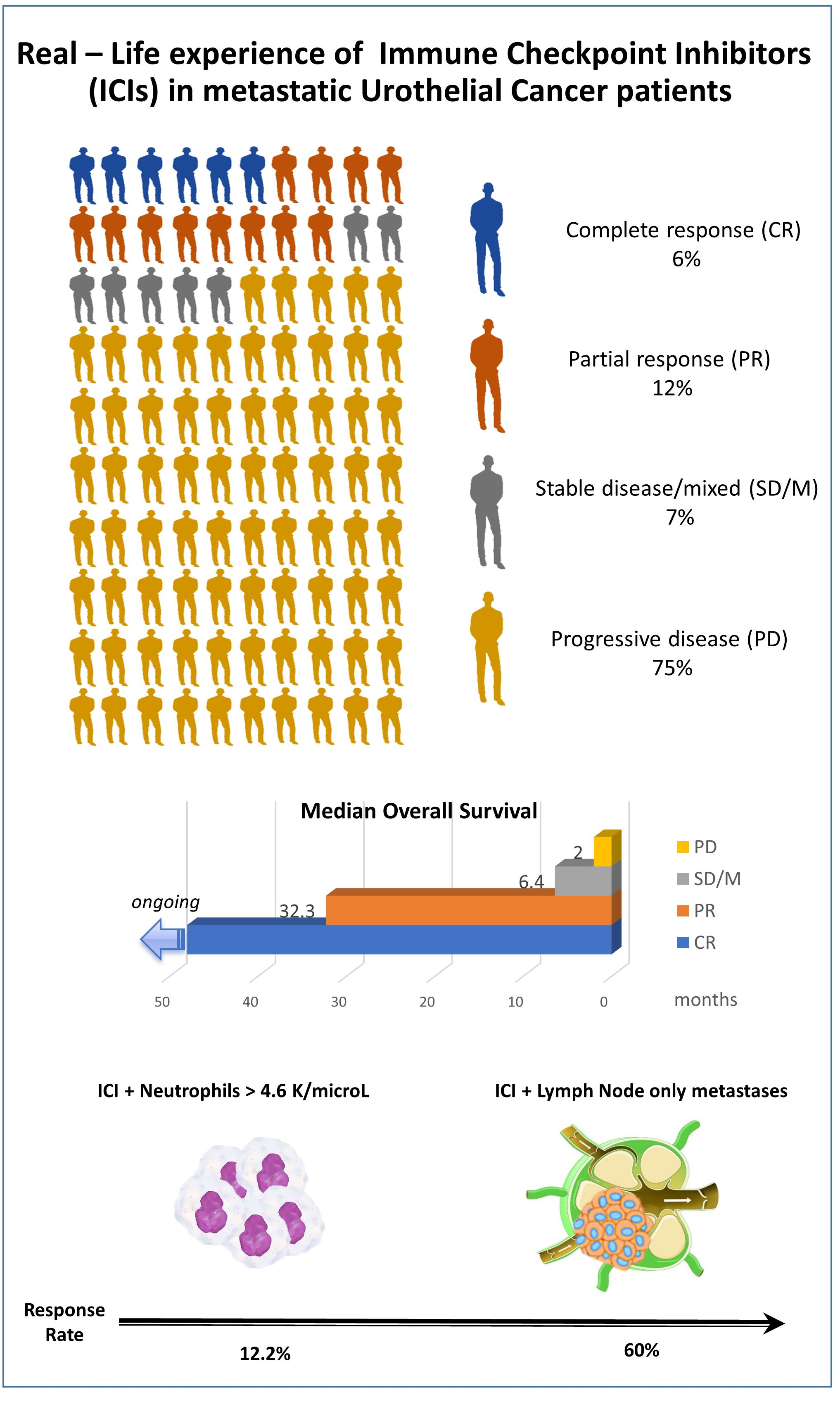
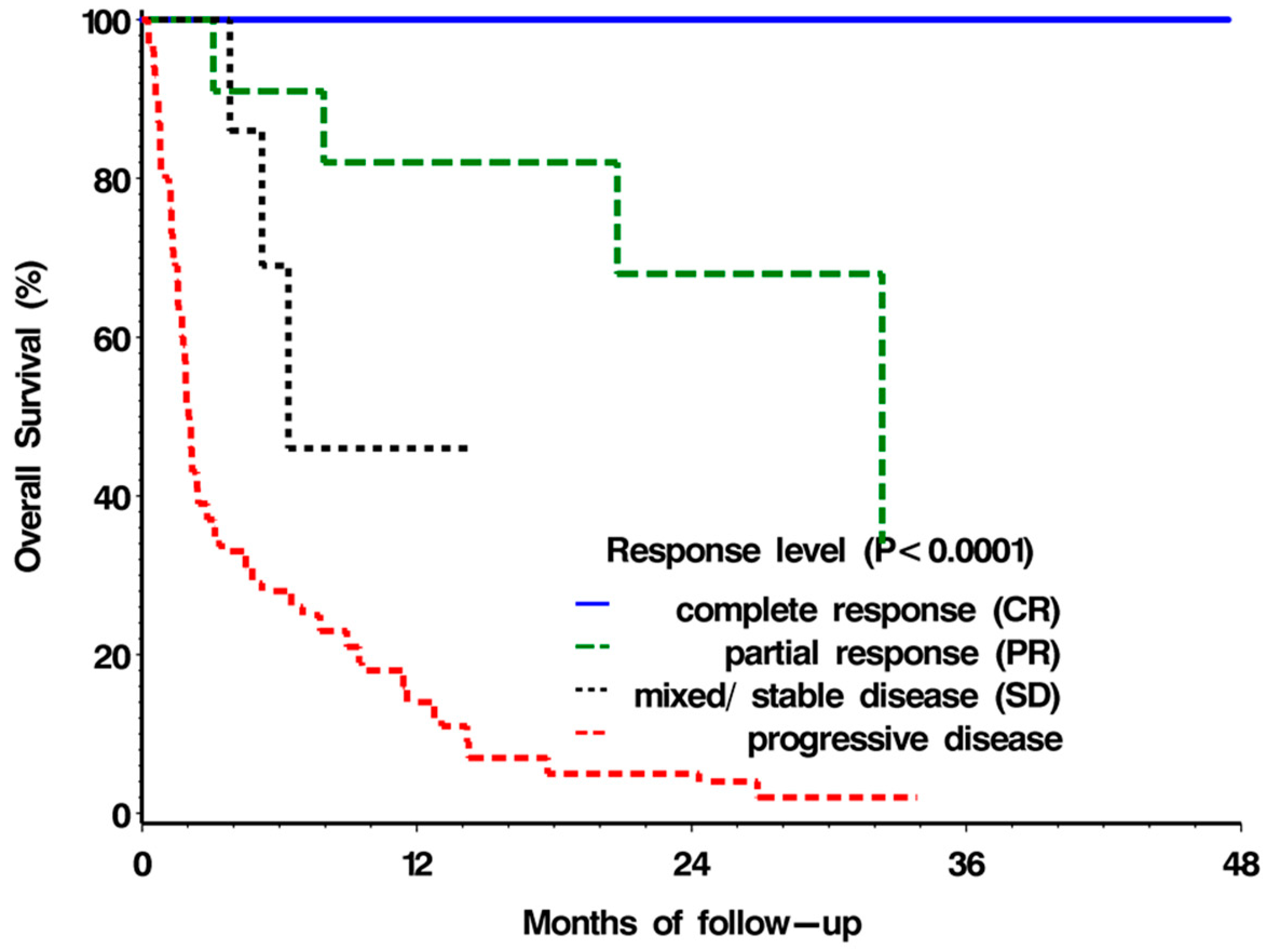
| Response Type | N | % | Median OS (95% CI; Months) |
|---|---|---|---|
| Complete response (CR) | 6 | 6.4 | NR |
| Partial response (PR) | 11 | 11.7 | 32.3 (>7.9) |
| Stable disease (SD)/ mixed response | 7 | 7.4 | 6.4 (>3.8) |
| Progressive Disease (PD) | 70 | 74.5 | 2.0 (1.7–2.5) |
| Level | p-Value | OR | 95% CI | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Worst metastatic Site | node only vs. bone | 0.005 | 15.75 | 2.30 | 107.93 |
| visceral disease vs. bone | 1.82 | 0.36 | 9.13 | ||
| Neutrophil (K/microL) | 0.15 | 0.87 | 0.72 | 1.05 | |
| Neutrophil > 4.6 (K/microL) | Yes vs. No | 0.06 | 0.34 | 0.11 | 1.06 |
| Parameter | Level | p-Value | OR | 95% CI | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Worst metastatic Site | node only vs. bone | 0.007 | 21.6 | 2.6 | 180.0 |
| Neutrophil > 4.6 K/microL | Yes vs. No | 0.054 | 0.28 | 0.08 | 1.02 |
| Clinical Characteristic | Response Rate | 95% CI | |
|---|---|---|---|
| Metastatic site | Visceral | 14.8 | (7–26) |
| Bone | 8.7 | (1–28) | |
| LN only | 60.0 | (26–88) | |
| Neutrophils (K/microL) | >4.6 | 12.2 | (4–26) |
| ≤4.6 | 29.3 | (16–46) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gadot, M.; Arad, I.; Atenafu, E.G.; Levartovsky, M.; Portnoy, O.; Davidson, T.; Schor-Bardach, R.; Berger, R.; Leibowitz, R. Response to Anti-PD1/L1 Antibodies in Advanced Urothelial Cancer in the ‘Real-Life’ Setting. Pharmaceuticals 2022, 15, 1154. https://doi.org/10.3390/ph15091154
Gadot M, Arad I, Atenafu EG, Levartovsky M, Portnoy O, Davidson T, Schor-Bardach R, Berger R, Leibowitz R. Response to Anti-PD1/L1 Antibodies in Advanced Urothelial Cancer in the ‘Real-Life’ Setting. Pharmaceuticals. 2022; 15(9):1154. https://doi.org/10.3390/ph15091154
Chicago/Turabian StyleGadot, Moran, Ido Arad, Eshetu G. Atenafu, Meital Levartovsky, Orith Portnoy, Tima Davidson, Rachel Schor-Bardach, Raanan Berger, and Raya Leibowitz. 2022. "Response to Anti-PD1/L1 Antibodies in Advanced Urothelial Cancer in the ‘Real-Life’ Setting" Pharmaceuticals 15, no. 9: 1154. https://doi.org/10.3390/ph15091154
APA StyleGadot, M., Arad, I., Atenafu, E. G., Levartovsky, M., Portnoy, O., Davidson, T., Schor-Bardach, R., Berger, R., & Leibowitz, R. (2022). Response to Anti-PD1/L1 Antibodies in Advanced Urothelial Cancer in the ‘Real-Life’ Setting. Pharmaceuticals, 15(9), 1154. https://doi.org/10.3390/ph15091154