
Cross-Validation of a Multiplex LC-MS/MS Method for Assaying mAbs Plasma Levels in Patients with Cancer: A GPCO-UNICANCER Study

 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Results
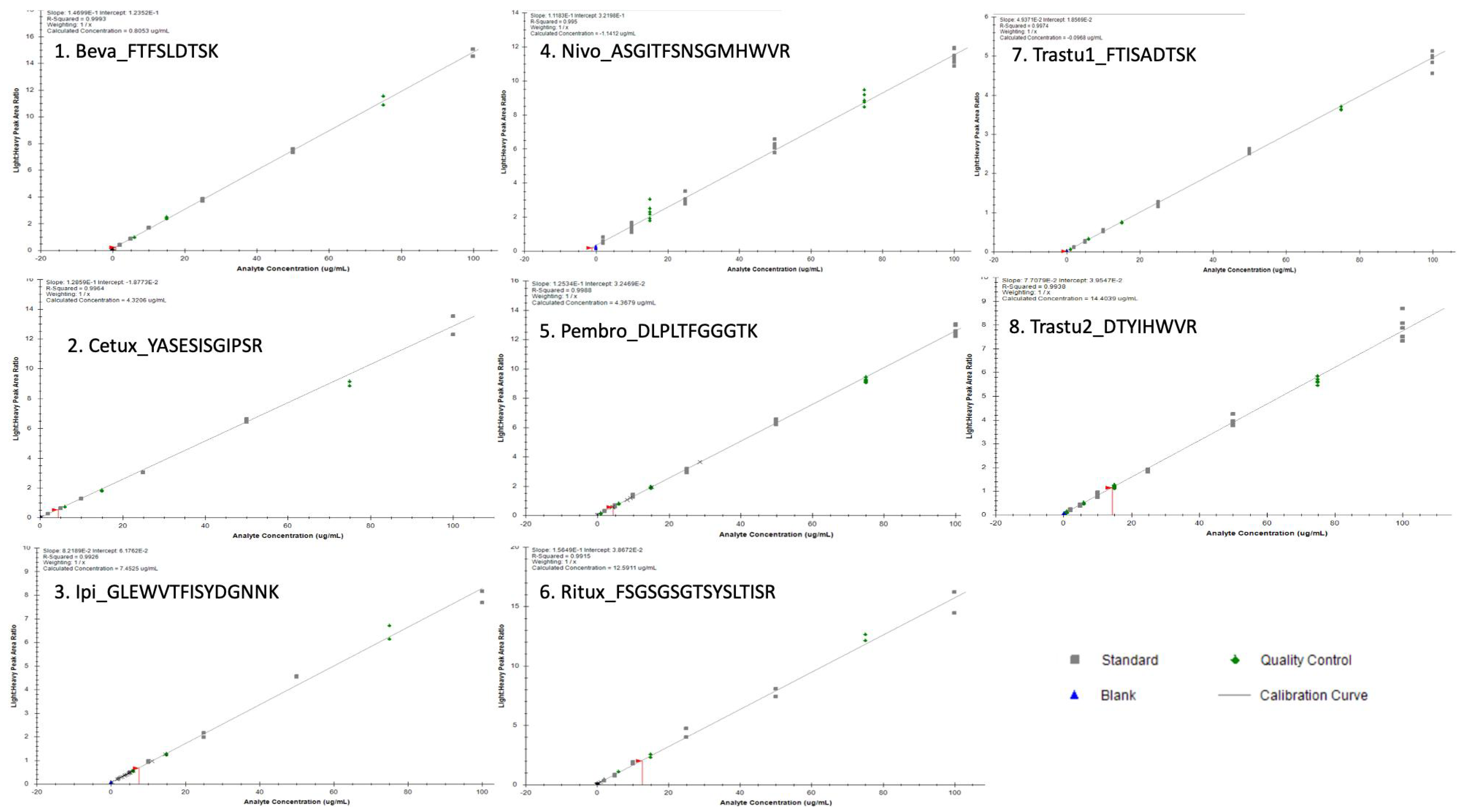
2.1. Validation
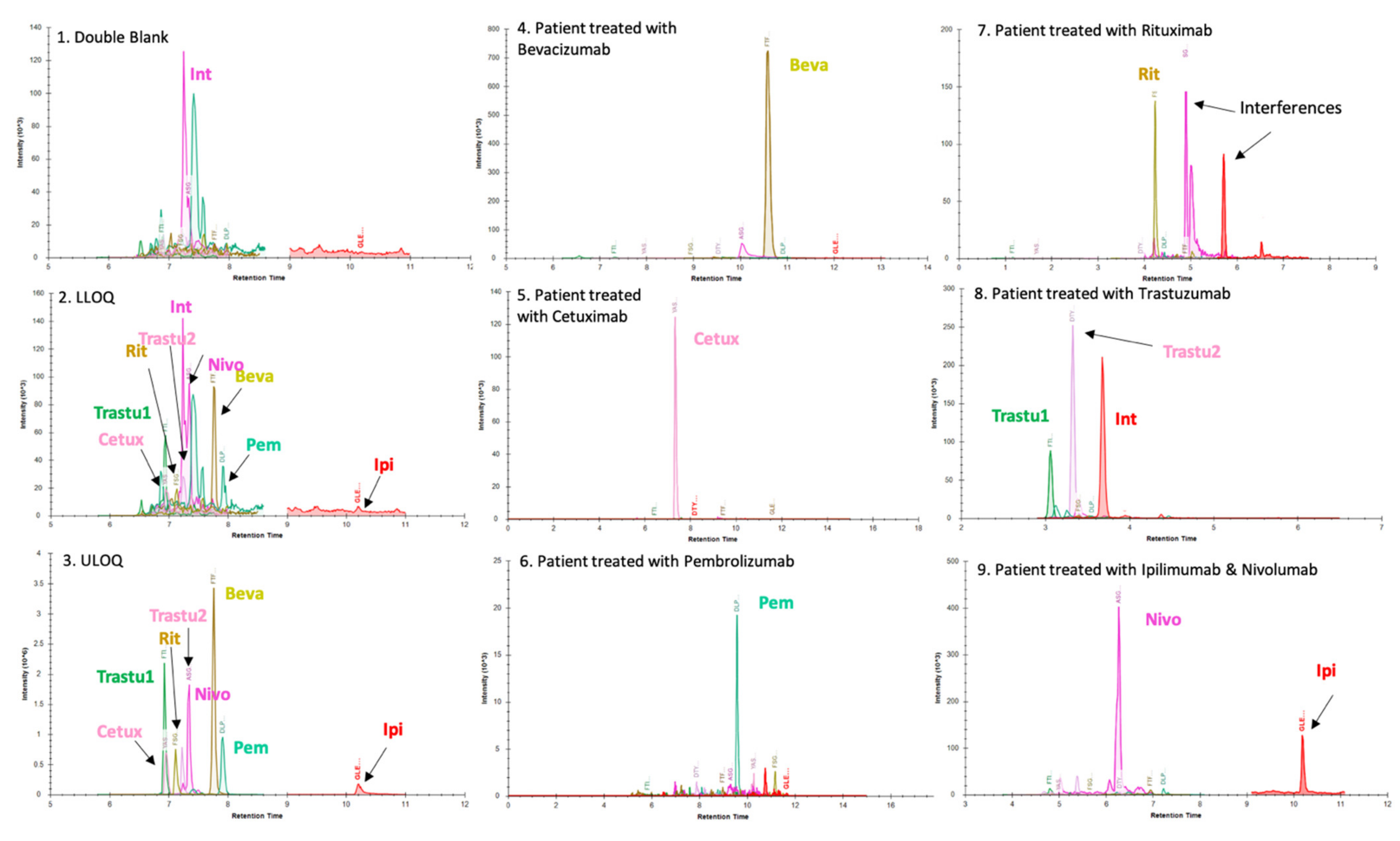
2.1.1. Chromatograms
2.1.2. Accuracy and Precision
2.1.3. Dilution Effect
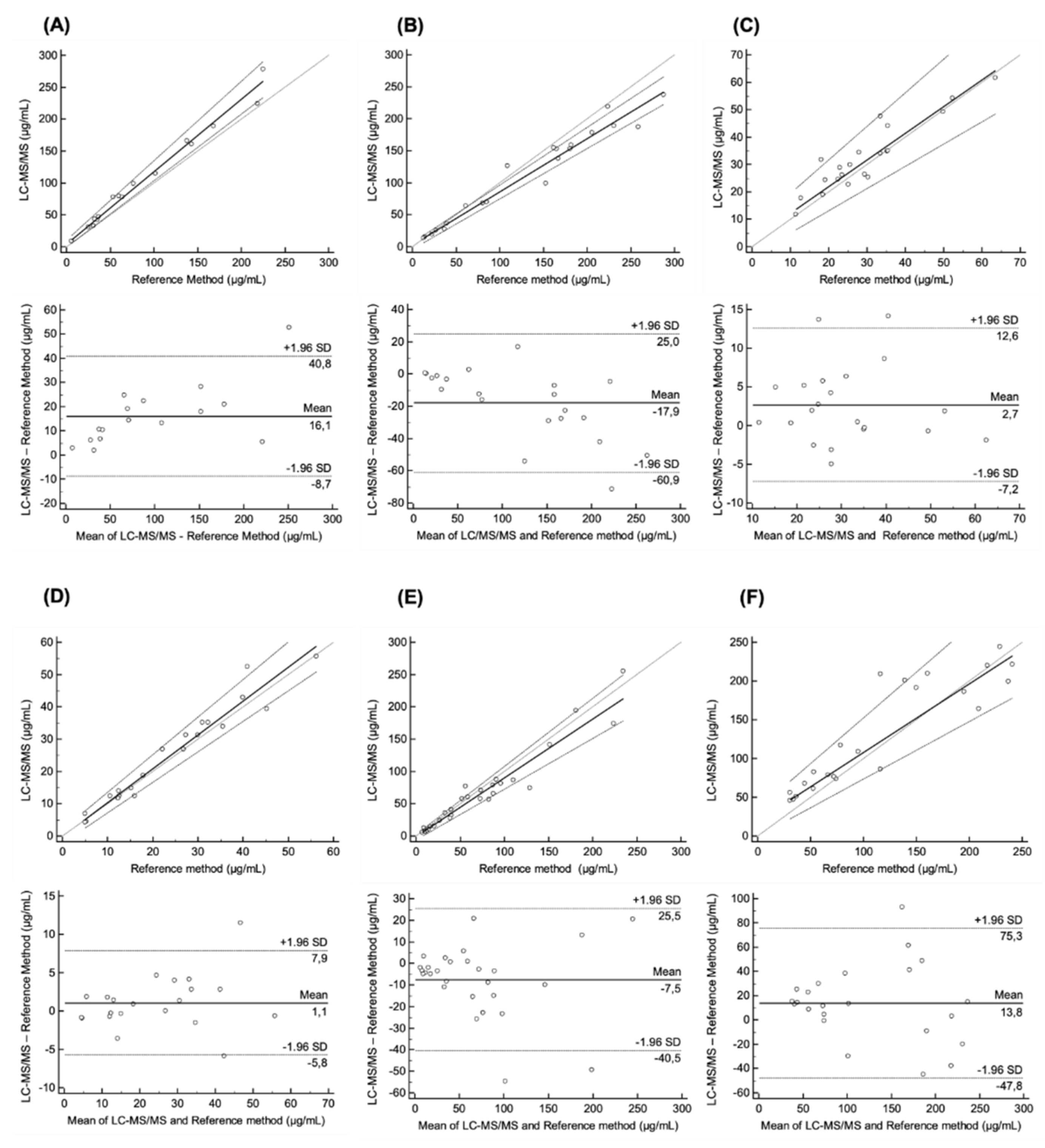
2.2. Comparison of mAbs Levels with LC–MS/MS Method versus References Methods
3. Discussion
4. Materials and Methods
4.1. Reagents and Consumables
4.2. Calibration Curve and Internal Quality Control Preparation
4.2.1. Sample Preparation with mAbXmise Kit
4.2.2. Selection of Peptides for Quantification
4.2.3. Chromatographic and Mass Spectrometric Conditions and Instrumentation
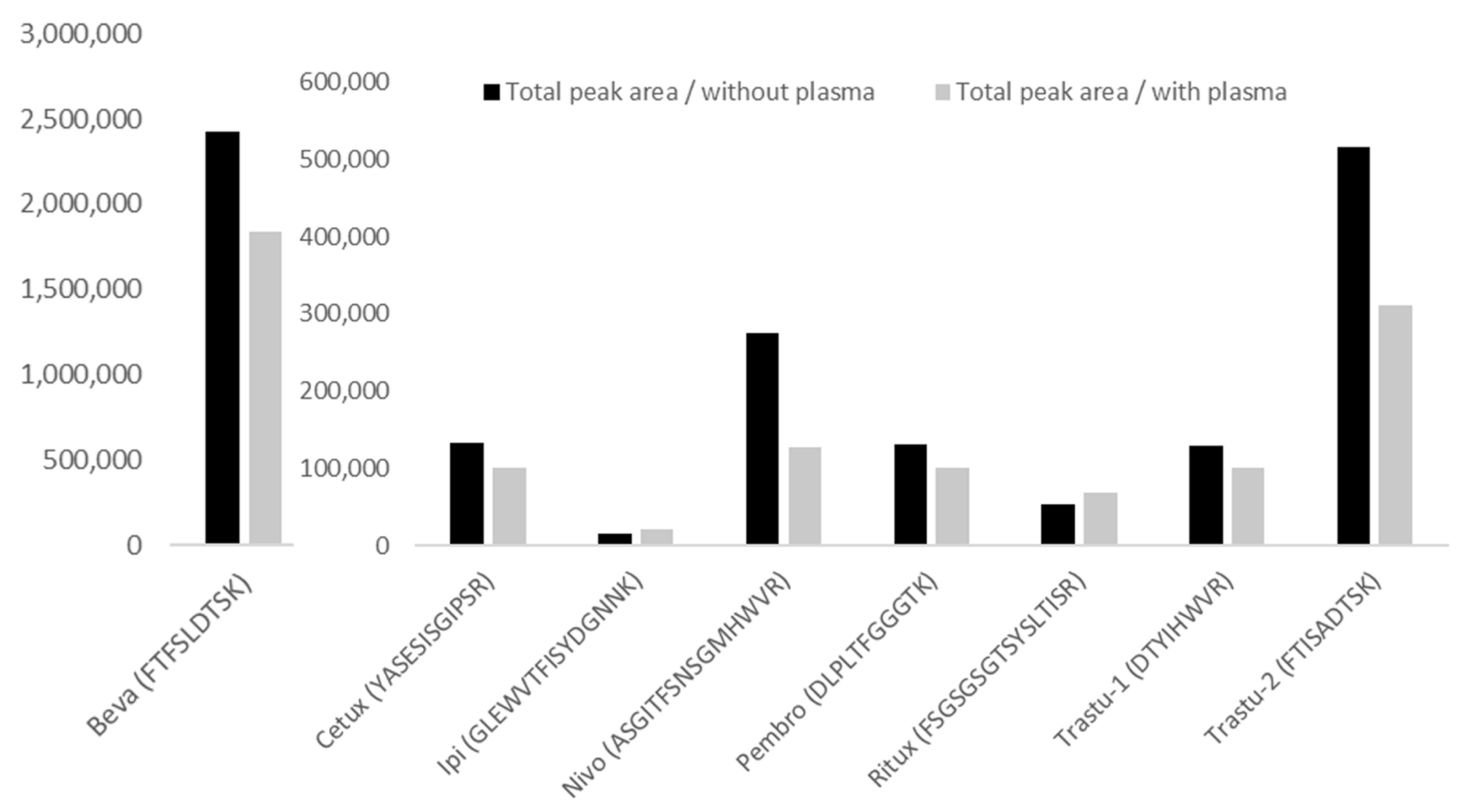
4.2.4. Selectivity, Carry-Over and Matrix Effect
4.2.5. Method Validation
4.2.6. Cross Validation
4.2.7. Statistical Analysis
4.2.8. Ethic Committee Approval
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Caulet, M.; Lecomte, T.; Bouché, O.; Rollin, J.; Gouilleux-Gruart, V.; Azzopardi, N.; Léger, J.; Borg, C.; Douillard, J.-Y.; Manfredi, S.; et al. Bevacizumab Pharmacokinetics Influence Overall and Progression-Free Survival in Metastatic Colorectal Cancer Patients. Clin. Pharmacokinet. 2016, 55, 1381–1394. [Google Scholar] [CrossRef]
- Igarashi, T.; Kobayashi, Y.; Ogura, M.; Kinoshita, T.; Ohtsu, T.; Sasaki, Y.; Morishima, Y.; Murate, T.; Kasai, M.; Uike, N.; et al. IDEC-C2B8 Study Group in Japan, Factors affecting toxicity, response and progression-free survival in relapsed patients with indolent B-cell lymphoma and mantle cell lymphoma treated with rituximab: A Japanese phase II study. Ann. Oncol. 2002, 13, 928–943. [Google Scholar] [CrossRef]
- Tobinai, K.; Igarashi, T.; Itoh, K.; Kobayashi, Y.; Taniwaki, M.; Ogura, M.; Kinoshita, T.; Hotta, T.; Aikawa, K.; Tsushita, K.; et al. IDEC-C2B8 Japan Study Group, Japanese multicenter phase II and pharmacokinetic study of rituximab in relapsed or refractory patients with aggressive B-cell lymphoma. Ann. Oncol. 2004, 15, 821–830. [Google Scholar] [CrossRef]
- Becher, F.; Ciccolini, J.; Imbs, D.-C.; Marin, C.; Fournel, C.; Dupuis, C.; Fakhry, N.; Pourroy, B.; Ghettas, A.; Pruvost, A.; et al. A simple and rapid LC-MS/MS method for therapeutic drug monitoring of cetuximab: A GPCO-UNICANCER proof of concept study in head-and-neck cancer patients. Sci. Rep. 2017, 7, 2714. [Google Scholar] [CrossRef] [PubMed]
- Azzopardi, N.; Lecomte, T.; Ternant, D.; Boisdron-Celle, M.; Piller, F.; Morel, A.; Gouilleux-Gruart, V.; Vignault-Desvignes, C.; Watier, H.; Gamelin, E.; et al. Cetuximab pharmacokinetics influences progression-free survival of metastatic colorectal cancer patients. Clin. Cancer Res. 2011, 17, 6329–6337. [Google Scholar] [CrossRef] [Green Version]
- Paci, A.; Desnoyer, A.; Delahousse, J.; Blondel, L.; Maritaz, C.; Chaput, N.; Mir, O.; Broutin, S. Pharmacokinetic/pharmacodynamic relationship of therapeutic monoclonal antibodies used in oncology: Part 1, monoclonal antibodies, antibody-drug conjugates and bispecific T-cell engagers. Eur. J. Cancer 2020, 128, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Desnoyer, A.; Broutin, S.; Delahousse, J.; Maritaz, C.; Blondel, L.; Mir, O.; Chaput, N.; Paci, A. Pharmacokinetic/pharmacodynamic relationship of therapeutic monoclonal antibodies used in oncology: Part 2, immune checkpoint inhibitor antibodies. Eur. J. Cancer 2020, 128, 119–128. [Google Scholar] [CrossRef]
- Fleisher, B.; Ait-Oudhia, S. A retrospective examination of the US Food and Drug Administration’s clinical pharmacology reviews of oncology biologics for potential use of therapeutic drug monitoring. OncoTargets Ther. 2018, 11, 113–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, Y.; Roy, A.; Masson, E.; Chen, T.-T.; Humphrey, R.; Weber, J.S. Exposure-response relationships of the efficacy and safety of ipilimumab in patients with advanced melanoma. Clin. Cancer Res. 2013, 19, 3977–3986. [Google Scholar] [CrossRef] [Green Version]
- Wolchok, J.D.; Neyns, B.; Linette, G.; Negrier, S.; Lutzky, J.; Thomas, L.; Waterfield, W.; Schadendorf, D.; Smylie, M.; Guthrie, T.; et al. Ipilimumab monotherapy in patients with pretreated advanced melanoma: A randomised, double-blind, multicentre, phase 2, dose-ranging study. Lancet Oncol. 2010, 11, 155–164. [Google Scholar] [CrossRef]
- Ascierto, P.A.; del Vecchio, M.; Robert, C.; Mackiewicz, A.; Chiarion-Sileni, V.; Arance, A.; Lebbé, C.; Bastholt, L.; Hamid, O.; Rutkowski, P.; et al. Ipilimumab 10 mg/kg versus ipilimumab 3 mg/kg in patients with unresectable or metastatic melanoma: A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2017, 18, 611–622. [Google Scholar] [CrossRef]
- Chatterjee, M.S.; Elassaiss-Schaap, J.; Lindauer, A.; Turner, D.C.; Sostelly, A.; Freshwater, T.; Mayawala, K.; Ahamadi, M.; Stone, J.A.; de Greef, R.; et al. Population Pharmacokinetic/Pharmacodynamic Modeling of Tumor Size Dynamics in Pembrolizumab-Treated Advanced Melanoma. CPT Pharmacomet. Syst. Pharmacol. 2017, 6, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Freshwater, T.; Kondic, A.; Ahamadi, M.; Li, C.H.; de Greef, R.; de Alwis, D.; Stone, J.A. Evaluation of dosing strategy for pembrolizumab for oncology indications. J. Immunother. Cancer 2017, 5, 43. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Yu, J.; Liu, C.; Liu, J.; Subramaniam, S.; Zhao, H.; Blumenthal, G.M.; Turner, D.C.; Li, C.; Ahamadi, M.; et al. Time dependent pharmacokinetics of pembrolizumab in patients with solid tumor and its correlation with best overall response. J. Pharmacokinet. Pharmacodyn. 2017, 44, 403–414. [Google Scholar] [CrossRef] [PubMed]
- Le Louedec, F.; Leenhardt, F.; Marin, C.; Chatelut, É.; Evrard, A.; Ciccolini, J. Cancer Immunotherapy Dosing: A Pharmacokinetic/Pharmacodynamic Perspective. Vaccines 2020, 8, 632. [Google Scholar] [CrossRef] [PubMed]
- Ratain, M.J.; Goldstein, D.A. Time Is Money: Optimizing the Scheduling of Nivolumab. J. Clin. Oncol. 2018, JCO1800045. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Masson, E.; Dai, D.; Parker, S.M.; Berman, D.; Roy, A. Model-based clinical pharmacology profiling of ipilimumab in patients with advanced melanoma. Br. J. Clin. Pharmacol. 2014, 78, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Kato, R.; Ikarashi, D.; Matsuura, T.; Maekawa, S.; Kato, Y.; Kanehira, M.; Takata, R.; Tokuyama, R.; Tamai, K.; Harigai, N.; et al. Analyses of Nivolumab Exposure and Clinical Safety Between 3-mg/kg Dosing and 240-mg Flat Dosing in Asian Patients with Advanced Renal Cell Carcinoma in the Real-World Clinical Setting. Transl. Oncol. 2020, 13, 100771. [Google Scholar] [CrossRef]
- Cosson, V.F.; Ng, V.W.; Lehle, M.; Lum, B.L. Population pharmacokinetics and exposure-response analyses of trastuzumab in patients with advanced gastric or gastroesophageal junction cancer. Cancer Chemother. Pharmacol. 2014, 73, 737–747. [Google Scholar] [CrossRef]
- Pluim, D.; Ros, W.; van Bussel, M.T.J.; Brandsma, D.; Beijnen, J.H.; Schellens, J.H.M. Enzyme linked immunosorbent assay for the quantification of nivolumab and pembrolizumab in human serum and cerebrospinal fluid. J. Pharm. Biomed. Anal. 2019, 164, 128–134. [Google Scholar] [CrossRef]
- Berinstein, N.L.; Grillo-López, A.J.; White, C.A.; Bence-Bruckler, I.; Maloney, D.; Czuczman, M.; Green, D.; Rosenberg, J.; McLaughlin, P.; Shen, D. Association of serum Rituximab (IDEC-C2B8) concentration and anti-tumor response in the treatment of recurrent low-grade or follicular non-Hodgkin’s lymphoma. Ann. Oncol. 1998, 9, 995–1001. [Google Scholar] [CrossRef]
- Iwamoto, N.; Takanashi, M.; Shimada, T.; Sasaki, J.; Hamada, A. Comparison of Bevacizumab Quantification Results in Plasma of Non-small Cell Lung Cancer Patients Using Bioanalytical Techniques Between LC-MS/MS, ELISA, and Microfluidic-based Immunoassay. AAPS J. 2019, 21, 101. [Google Scholar] [CrossRef] [PubMed]
- Suárez, I.; Salmerón-García, A.; Cabeza, J.; Capitán-Vallvey, L.F.; Navas, N. Development and use of specific ELISA methods for quantifying the biological activity of bevacizumab, cetuximab and trastuzumab in stability studies. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2016, 1032, 155–164. [Google Scholar] [CrossRef]
- Truffot, A.; Jourdil, J.-F.; Seitz-Polski, B.; Malvezzi, P.; Brglez, V.; Stanke-Labesque, F.; Gautier-Veyret, E. Simultaneous quantification of rituximab and eculizumab in human plasma by liquid chromatography-tandem mass spectrometry and comparison with rituximab ELISA kits. Clin. Biochem. 2021, 87, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Schokker, S.; Fusetti, F.; Bonardi, F.; Molenaar, R.J.; Mathôt, R.A.A.; van Laarhoven, H.W.M. Development and validation of an LC-MS/MS method for simultaneous quantification of co-administered trastuzumab and pertuzumab. mAbs 2020, 12, 1795492. [Google Scholar] [CrossRef]
- Ternant, D.; Cézé, N.; Lecomte, T.; Degenne, D.; Duveau, A.-C.; Watier, H.; Dorval, E.; Paintaud, G. An enzyme-linked immunosorbent assay to study bevacizumab pharmacokinetics. Ther. Drug Monit. 2010, 32, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Millet, A.; Lebert, D.; Picard, G.; You, B.; Ceruse, P.; Guitton, J. Determination of Cetuximab in Plasma by Liquid Chromatography-High-Resolution Mass Spectrometry Orbitrap with a Stable Labeled 13C,15N-Cetuximab Internal Standard. Ther. Drug Monit. 2019, 41, 467–475. [Google Scholar] [CrossRef]
- Millet, A.; Khoudour, N.; Bros, P.; Lebert, D.; Picard, G.; Machon, C.; Goldwasser, F.; Blanchet, B.; Guitton, J. Quantification of nivolumab in human plasma by LC-MS/HRMS and LC-MS/MS, comparison with ELISA. Talanta 2021, 224, 121889. [Google Scholar] [CrossRef]
- Millet, A.; Khoudour, N.; Guitton, J.; Lebert, D.; Goldwasser, F.; Blanchet, B.; Machon, C. Analysis of pembrolizumab in human plasma by LC-MS/HRMS. Method validation and comparison with ELISA. Biomedecines 2021, 9, 621. [Google Scholar] [CrossRef]
- Millet, A.; Khoudour, N.; Lebert, D.; Machon, C.; Terrier, B.; Blanchet, B.; Guitton, J. Development, Validation, and Comparison of Two Mass Spectrometry Methods (LC-MS/HRMS and LC-MS/MS) for the Quantification of Rituximab in Human Plasma. Molecules 2021, 26, 1383. [Google Scholar] [CrossRef] [PubMed]
- Willeman, T.; Jourdil, J.-F.; Gautier-Veyret, E.; Bonaz, B.; Stanke-Labesque, F. A multiplex liquid chromatography tandem mass spectrometry method for the quantification of seven therapeutic monoclonal antibodies: Application for adalimumab therapeutic drug monitoring in patients with Crohn’s disease. Anal. Chim. Acta 2019, 1067, 63–70. [Google Scholar] [CrossRef]
- Centanni, M.; Moes, D.J.A.R.; Trocóniz, I.F.; Ciccolini, J.; van Hasselt, J.G.C. Clinical Pharmacokinetics and Pharmacodynamics of Immune Checkpoint Inhibitors. Clin. Pharmacokinet. 2019, 58, 835–857. [Google Scholar] [CrossRef] [Green Version]
- Chatelut, E.; le Louedec, F.; Milano, G. Setting the Dose of Checkpoint Inhibitors: The Role of Clinical Pharmacology. Clin. Pharmacokinet. 2020, 59, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Chatelut, E.; Hendrikx, J.J.M.A.; Martin, J.; Ciccolini, J.; Moes, D.J.A.R. Unraveling the complexity of therapeutic drug monitoring for monoclonal antibody therapies to individualize dose in oncology. Pharmacol. Res. Perspect. 2021, 9, e00757. [Google Scholar] [CrossRef] [PubMed]
- Basak, E.A.; Koolen, S.L.W.; Hurkmans, D.P.; Schreurs, M.W.J.; Bins, S.; Hoop, E.O.; Wijkhuijs, A.J.M.; den Besten, I.; Sleijfer, S.; Debets, R.; et al. Correlation between nivolumab exposure and treatment outcomes in non-small-cell lung cancer. Eur. J. Cancer 2019, 109, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Bellesoeur, A.; Ollier, E.; Allard, M.; Hirsch, L.; Boudou-Rouquette, P.; Arrondeau, J.; Thomas-Schoemann, A.; Tiako, M.; Khoudour, N.; Chapron, J.; et al. Is there an Exposure-Response Relationship for Nivolumab in Real-World NSCLC Patients? Cancers 2019, 11, 1784. [Google Scholar] [CrossRef] [Green Version]
- Turner, D.C.; Kondic, A.G.; Anderson, K.M.; Robinson, A.G.; Garon, E.B.; Riess, J.W.; Jain, L.; Mayawala, K.; Kang, J.; Ebbinghaus, S.W.; et al. Pembrolizumab Exposure-Response Assessments Challenged by Association of Cancer Cachexia and Catabolic Clearance. Clin. Cancer Res. 2018, 24, 5841–5849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keizer, R.J.; Huitema, A.D.R.; Schellens, J.H.M.; Beijnen, J.H. Clinical pharmacokinetics of therapeutic monoclonal antibodies. Clin. Pharmacokinet. 2010, 49, 493–507. [Google Scholar] [CrossRef] [PubMed]
- Irie, K.; Okada, A.; Yamasaki, Y.; Kokan, C.; Hata, A.; Kaji, R.; Fukushima, K.; Sugioka, N.; Okada, Y.; Katakami, N.; et al. An LC-MS/MS Method for Absolute Quantification of Nivolumab in Human Plasma: Application to Clinical Therapeutic Drug Monitoring. Ther. Drug Monit. 2018, 40, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.-H.; Liao, H.-W.; Shao, Y.-Y.; Lu, Y.-S.; Lin, C.-H.; Tsai, I.-L.; Kuo, C.-H. Development of a general method for quantifying IgG-based therapeutic monoclonal antibodies in human plasma using protein G purification coupled with a two internal standard calibration strategy using LC-MS/MS. Anal. Chim. Acta 2018, 1019, 93–102. [Google Scholar] [CrossRef]
- Peer, C.J.; Goldstein, D.A.; Goodell, J.C.; Nguyen, R.; Figg, W.D.; Ratain, M.J. Opportunities for using in silico-based extended dosing regimens for monoclonal antibody immune checkpoint inhibitors. Br. J. Clin. Pharmacol. 2020, 86, 1769–1777. [Google Scholar] [CrossRef] [PubMed]
- Basak, E.A.; Wijkhuijs, A.J.M.; Mathijssen, R.H.J.; Koolen, S.L.W.; Schreurs, M.W.J. Development of an Enzyme-Linked Immune Sorbent Assay to Measure Nivolumab and Pembrolizumab Serum Concentrations. Ther. Drug Monit. 2018, 40, 596–601. [Google Scholar] [CrossRef] [PubMed]
- Ohuchi, M.; Yagishita, S.; Taguchi, K.; Goto, Y.; Fukahori, M.; Enoki, Y.; Shimada, T.; Yamaguchi, M.; Matsumoto, K.; Hamada, A. Use of an alternative signature peptide during development of a LC-MS/MS assay of plasma nivolumab levels applicable for multiple species. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2021, 1162, 122489. [Google Scholar] [CrossRef]
- Iwamoto, N.; Shimada, T.; Terakado, H.; Hamada, A. Validated LC-MS/MS analysis of immune checkpoint inhibitor Nivolumab in human plasma using a Fab peptide-selective quantitation method: Nano-surface and molecular-orientation limited (nSMOL) proteolysis. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2016, 1023–1024, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sureda, M.; Mata, J.J.; Catalán, A.; Escudero, V.; Martínez-Navarro, E.; Rebollo, J. Therapeutic drug monitoring of nivolumab in routine clinical practice. A pilot study. Farm Hosp. 2020, 44, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Puszkiel, A.; Noé, G.; Boudou-Rouquette, P.; Cossec, C.L.; Arrondeau, J.; Giraud, J.-S.; Thomas-Schoemann, A.; Alexandre, J.; Vidal, M.; Goldwasser, F.; et al. Development and validation of an ELISA method for the quantification of nivolumab in plasma from non-small-cell lung cancer patients. J. Pharm. Biomed. Anal. 2017, 139, 30–36. [Google Scholar] [CrossRef]
- EMEA. Bioanalytical Method Validation, European Medicines Agency—Commission. 2018. Available online: https://www.ema.europa.eu/en/bioanalytical-method-validation (accessed on 19 February 2019).
- Carr, S.A.; Abbatiello, S.E.; Ackermann, B.L.; Borchers, C.; Domon, B.; Deutsch, E.W.; Grant, R.P.; Hoofnagle, A.N.; Hüttenhain, R.; Koomen, J.M.; et al. Targeted Peptide Measurements in Biology and Medicine: Best Practices for Mass Spectrometry-based Assay Development Using a Fit-for-Purpose Approach. Mol. Cell Proteom. 2014, 13, 907–917. [Google Scholar] [CrossRef] [Green Version]
- Kverneland, A.H.; Enevold, C.; Donia, M.; Bastholt, L.; Svane, I.M.; Nielsen, C.H. Development of anti-drug antibodies is associated with shortened survival in patients with metastatic melanoma treated with ipilimumab. Oncoimmunology 2018, 7, e1424674. [Google Scholar] [CrossRef]
- Passing, H.; Bablok, W. Comparison of several regression procedures for method comparison studies and determination of sample sizes. Application of linear regression procedures for method comparison studies in Clinical Chemistry, Part II. J. Clin. Chem. Clin. Biochem. 1984, 22, 431–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bults, P.; Bischoff, R.; Bakker, H.; Gietema, J.A.; van de Merbel, N.C. LC-MS/MS-Based Monitoring of In Vivo Protein Biotransformation: Quantitative Determination of Trastuzumab and Its Deamidation Products in Human Plasma. Anal. Chem. 2016, 88, 1871–1877. [Google Scholar] [CrossRef] [PubMed]
- Vialaret, J.; Broutin, S.; Pugnier, C.; Santelé, S.; Jaffuel, A.; Barnes, A.; Tiers, L.; Pelletier, L.; Lehmann, S.; Paci, A.; et al. What sample preparation should be chosen for targeted MS monoclonal antibody quantification in human serum? Bioanalysis 2018, 10, 723–735. [Google Scholar] [CrossRef] [PubMed]
- Shibata, K.; Naito, T.; Okamura, J.; Hosokawa, S.; Mineta, H.; Kawakami, J. Simple and rapid LC-MS/MS method for the absolute determination of cetuximab in human serum using an immobilized trypsin. J. Pharm. Biomed. Anal. 2017, 146, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.J. Regression analysis. Lancet 1986, 1, 908–909. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Within-Run | Between-Run | ||||||
|---|---|---|---|---|---|---|---|
| Nominal Concentration (µg/mL) | Level | Mean Calculated Concentration (µg/mL) | Intra-Day Precision a (%, n = 6) | Intra-Day Accuracy (%, n = 6) | Mean Calculated Concentration (µg/mL) | Inter-Day Precision a (%, D = 4, n = 16) | Inter-Day Accuracy (%, D = 4, n = 16) |
| BevacizumabFTFSLDTSK | |||||||
| 2 | LLOQ | 2.1 | 3.4 | 103.0 | 2.0 | 1.5 | 101.2 |
| 6 | Low IQC | 6.3 | 3.1 | 105.1 | 6.2 | 3.3 | 102.8 |
| 15 | Mid IQC | 15.5 | 1.8 | 103.1 | 15.8 | 1.7 | 105.4 |
| 75 | High IQC | 75.4 | 1.1 | 100.5 | 75.7 | 1.0 | 100.9 |
| Cetuximab YASESGIPSR | |||||||
| 2 | LLOQ | 2.0 | 1.4 | 102.0 | 2.0 | 4.6 | 98.6 |
| 6 | Low IQC | 6.2 | 1.9 | 104.0 | 6.1 | 3.4 | 102.5 |
| 15 | Mid IQC | 15.2 | 1.9 | 101.0 | 15.4 | 1.7 | 102.4 |
| 75 | High IQC | 73.8 | 0.9 | 98.4 | 74.1 | 1.1 | 98.8 |
| Ipilimumab GLEWVTFISYDGNNK | |||||||
| 2 | LLOQ | 2.2 | 3.4 | 111.1 * | 2.0 | 11.5 | 99.4 ** |
| 6 | Low IQC | 6.2 | 14.6 | 102.7 | 6.0 | 7.2 | 100.0 ** |
| 15 | Mid IQC | 14.5 | 12.2 | 97.0 | 14.4 | 2.4 | 96.0 ** |
| 75 | High IQC | 81.3 | 3.9 | 108.0 | 78.7 | 5.2 | 105.0 ** |
| Nivolumab ASGITFSNSGMHWVR | |||||||
| 2 | LLOQ | 2.1 | 6.5 | 103.0 | 2.0 | 12.4 | 100.1 |
| 6 | Low IQC | 5.4 | 6.5 | 90.1 | 5.79 | 13.1 | 96.5 |
| 15 | Mid IQC | 14.1 | 7.7 | 94.0 | 15.6 | 7.3 | 104.0 |
| 75 | High IQC | 74.2 | 2.8 | 99.0 | 74.2 | 1.2 | 99.0 |
| Pembrolizumab DLPLTFGGGTK | |||||||
| 2 | LLOQ | 1.9 | 4.2 | 95.7 | 1.9 | 2.1 | 93.0 |
| 6 | Low IQC | 6.0 | 2.1 | 100.4 | 6.1 | 4.4 | 100.7 |
| 15 | Mid IQC | 14.9 | 1.4 | 99.3 | 15.4 | 2.5 | 102.3 |
| 75 | High IQC | 73.1 | 1.5 | 97.5 | 74.8 | 1.6 | 100.0 |
| Rituximab FSGSGSGTSYSLTISR | |||||||
| 2 | LLOQ | 2.0 | 6.9 | 100.5 | 2.1 | 4.6 | 106.8 |
| 6 | Low IQC | 6.5 | 5.4 | 107.8 | 6.4 | 2.1 | 106.0 |
| 15 | Mid IQC | 16.1 | 3.8 | 107.5 | 16.1 | 1.8 | 107.1 |
| 75 | High IQC | 77.5 | 4.0 | 103.3 | 77.5 | 1.8 | 103.3 |
| Trastuzumab DTYIHWVR | |||||||
| 2 | LLOQ | 2.0 | 7.6 | 98.9 | 2.1 | 5.2 | 103.4 |
| 6 | Low IQC | 5.7 | 3.8 | 95.4 | 6.1 | 5.9 | 101.4 |
| 15 | Mid IQC | 14.9 | 5.1 | 99.2 | 15.5 | 4.2 | 103.2 |
| 75 | High IQC | 72.4 | 2.7 | 96.5 | 74.0 | 1.7 | 98.7 |
| Trastuzumab FTISADTSK | |||||||
| 2 | LLOQ | 1.9 | 3.1 | 93.4 | 1.8 | 8.1 | 91.3 |
| 6 | Low IQC | 6.2 | 2.0 | 103.1 | 6.0 | 4.2 | 99.6 |
| 15 | Mid IQC | 15.0 | 1.1 | 100.0 | 14.9 | 2.3 | 99.6 |
| 75 | High IQC | 74.8 | 1.0 | 99.7 | 73.3 | 1.9 | 97.8 |
| Passing-Bablok | Bland–Altman Absolute Differences | |||
|---|---|---|---|---|
| Parameters | Slope (95% CI) | Intercept (95% CI) | Cusum Test (p-Value) | Bias (95% LOA) |
| Bevacizumab LC–MS/MS vs. ELISA Reference Method [26] (n = 16) | 1.132 (1.043; 1.242) | 4.16 (−1.41; 10.35) | 0.58 | 16.1 (−8.7; 40.8) |
| Cetuximab LC–MS/MS vs. LC–MS/MS Reference Method [27] (n = 21) | 0.829 (0.788; 0.900) | −2.72 (−4.53; 6.20) | 0.72 | −17.9 (−60.9; 25.0) |
| Nivolumab LC–MS/MS vs. LC–MS/MS Reference Method [28] (n = 21) | 0.970 (0.811; 1.221) | 2.59 (−3.05; 7.37) | 0.72 | 2.7 (−7.2; 12.6) |
| Pembrolizumab LS–MS/MS vs. LC–MS/MS Reference Method [29] (n = 21) | 1.049 (0.947;1.159) | −0.19 (−2.34; 2.04) | 0.72 | 1.1 (−5.8; 7.9) |
| Rituximab LS–MS/MS vs. LC–MS/MS Reference Method [30] (n = 28) | 0.909 (0.784; 1.054) | −1.30 (−5.82; 1.92) | 0.89 | −7.5 (−40.5; 25.5) |
| Trastuzumab LS–MS/M/S vs. LC–MS/MS Reference Method [31] (n = 23) | 0.884 (0.740; 1.178) | 19.42 (−0.23; 32.47) | 0.78 | 13.8 (−47.8; 75.3) |
| Monoclonal Antibody | Peptide Sequence | Q1 m/z | Charge Parent Ion | Q3 m/z | Fragment Ion |
|---|---|---|---|---|---|
| Bevacizumab | FTFSLDTSK | 523.263664 | 2+ | 797.404 | y7+ |
| 650.336 | y6+ | ||||
| 563.304 | y5+ | ||||
| 450.219 | y4+ | ||||
| 335.193 | y3+ | ||||
| FTFSLDTS [13C6,15N2] K | 527.270764 | 805.418 | y7+ | ||
| 658.350 | y6+ | ||||
| 571.318 | y5+ | ||||
| 458.234 | y4+ | ||||
| 343.207 | y3+ | ||||
| Cetuximab | YASESISGIPSR | 633.819866 | 2+ | 1103.569 | y11+ |
| 1032.532 | y10+ | ||||
| 816.457393 | y8+ | ||||
| YASESISGIPS [13C6,15N4] R | 638.824001 | 1113.577 | y11+ | ||
| 1042.540 | y10+ | ||||
| 826.466 | y8+ | ||||
| Ipilimumab | GLEWVTFISYDGNNK | 871.922851 | 2+ | 1257.611 | y11+ |
| 1158.543 | y10+ | ||||
| 1057.495 | y9+ | ||||
| 910.426 | y8+ | ||||
| 797.342 | y7+ | ||||
| 710.310 | y6+ | ||||
| 547.247 | y5+ | ||||
| GLEWVTFISYDGNN [13C6,15N2] K | 875.929951 | 1265.625 | y11+ | ||
| 1166.557 | y10+ | ||||
| 1065.509 | y9+ | ||||
| 918.441 | y8+ | ||||
| 805.357 | y7+ | ||||
| 718.325 | y6+ | ||||
| 555.261 | y5+ | ||||
| Nivolumab | ASGITFSNSGMHWVR | 550.599946 | 3+ | 1073.495 | y9+ |
| 986.462 | y8+ | ||||
| 872.420 | y7+ | ||||
| 785.387 | y6+ | ||||
| 661.309 | y112+ | ||||
| ASGITFSNSGMHWV [13C6,15N4] R | 553.936036 | 1083.503 | y9+ | ||
| 996.471 | y8+ | ||||
| 882.428 | y7+ | ||||
| 795.396 | y6+ | ||||
| 666.313 | y112+ | ||||
| Pembrolizumab | DLPLTFGGGTK | 553.298038 | 2+ | 877.478 | y9+ |
| 780.425 | y8+ | ||||
| 566.293 | y6+ | ||||
| 419.225 | y5+ | ||||
| DLPLTFGGGT [13C6,15N2] K | 557.305138 | 885.4920 | y9+ | ||
| 788.439 | y8+ | ||||
| 574.307 | y6+ | ||||
| 427.239 | y5+ | ||||
| Rituximab | FSGSGSGTSYSLTISR | 803.889009 | 2+ | 1084.563 | y10+ |
| 1027.542 | y9+ | ||||
| 926.494 | y8+ | ||||
| 839.462 | y7+ | ||||
| FSGSGSGTSYSLTIS [13C6,15N4] R | 808.893143 | 1094.572 | y10+ | ||
| 1037.550 | y9+ | ||||
| 936.502 | y8+ | ||||
| 849.470 | y7+ | ||||
| Trastuzumab | DTYIHWVR | 545.27744 | 2+ | 873.473 | y6+ |
| 710.410 | y5+ | ||||
| 597.326 | y4+ | ||||
| 460.267 | y3+ | ||||
| 630.288 | b5+ | ||||
| 816.368 | b6+ | ||||
| DTYIHWV [13C6,15N4] R | 550.281575 | 883.481 | y6+ | ||
| 720.418 | y5+ | ||||
| 607.334 | y4+ | ||||
| 470.275 | y3+ | ||||
| 630.288 | b5+ | ||||
| 816.368 | b6+ | ||||
| FTISADTSK | 485.248014 | 2+ | 822.420 | y8+ | |
| 608.289 | y6+ | ||||
| 521.257 | y5+ | ||||
| 450.219 | y4+ | ||||
| FTISADTS [13C6,15N2] K | 489.255114 | 830.435 | y8+ | ||
| 616.303 | y6+ | ||||
| 529.271 | y5+ | ||||
| 458.234 | y4+ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marin, C.; Khoudour, N.; Millet, A.; Lebert, D.; Bros, P.; Thomas, F.; Ternant, D.; Lacarelle, B.; Guitton, J.; Ciccolini, J.; et al. Cross-Validation of a Multiplex LC-MS/MS Method for Assaying mAbs Plasma Levels in Patients with Cancer: A GPCO-UNICANCER Study. Pharmaceuticals 2021, 14, 796. https://doi.org/10.3390/ph14080796
Marin C, Khoudour N, Millet A, Lebert D, Bros P, Thomas F, Ternant D, Lacarelle B, Guitton J, Ciccolini J, et al. Cross-Validation of a Multiplex LC-MS/MS Method for Assaying mAbs Plasma Levels in Patients with Cancer: A GPCO-UNICANCER Study. Pharmaceuticals. 2021; 14(8):796. https://doi.org/10.3390/ph14080796
Chicago/Turabian StyleMarin, Clémence, Nihel Khoudour, Aurélien Millet, Dorothée Lebert, Pauline Bros, Fabienne Thomas, David Ternant, Bruno Lacarelle, Jérôme Guitton, Joseph Ciccolini, and et al. 2021. "Cross-Validation of a Multiplex LC-MS/MS Method for Assaying mAbs Plasma Levels in Patients with Cancer: A GPCO-UNICANCER Study" Pharmaceuticals 14, no. 8: 796. https://doi.org/10.3390/ph14080796
APA StyleMarin, C., Khoudour, N., Millet, A., Lebert, D., Bros, P., Thomas, F., Ternant, D., Lacarelle, B., Guitton, J., Ciccolini, J., & Blanchet, B. (2021). Cross-Validation of a Multiplex LC-MS/MS Method for Assaying mAbs Plasma Levels in Patients with Cancer: A GPCO-UNICANCER Study. Pharmaceuticals, 14(8), 796. https://doi.org/10.3390/ph14080796