
Mild Cognitive Impairment and Mild Dementia: The Role of Ginkgo biloba (EGb 761®)

 ,
, 

 and
and
Abstract
1. Introduction
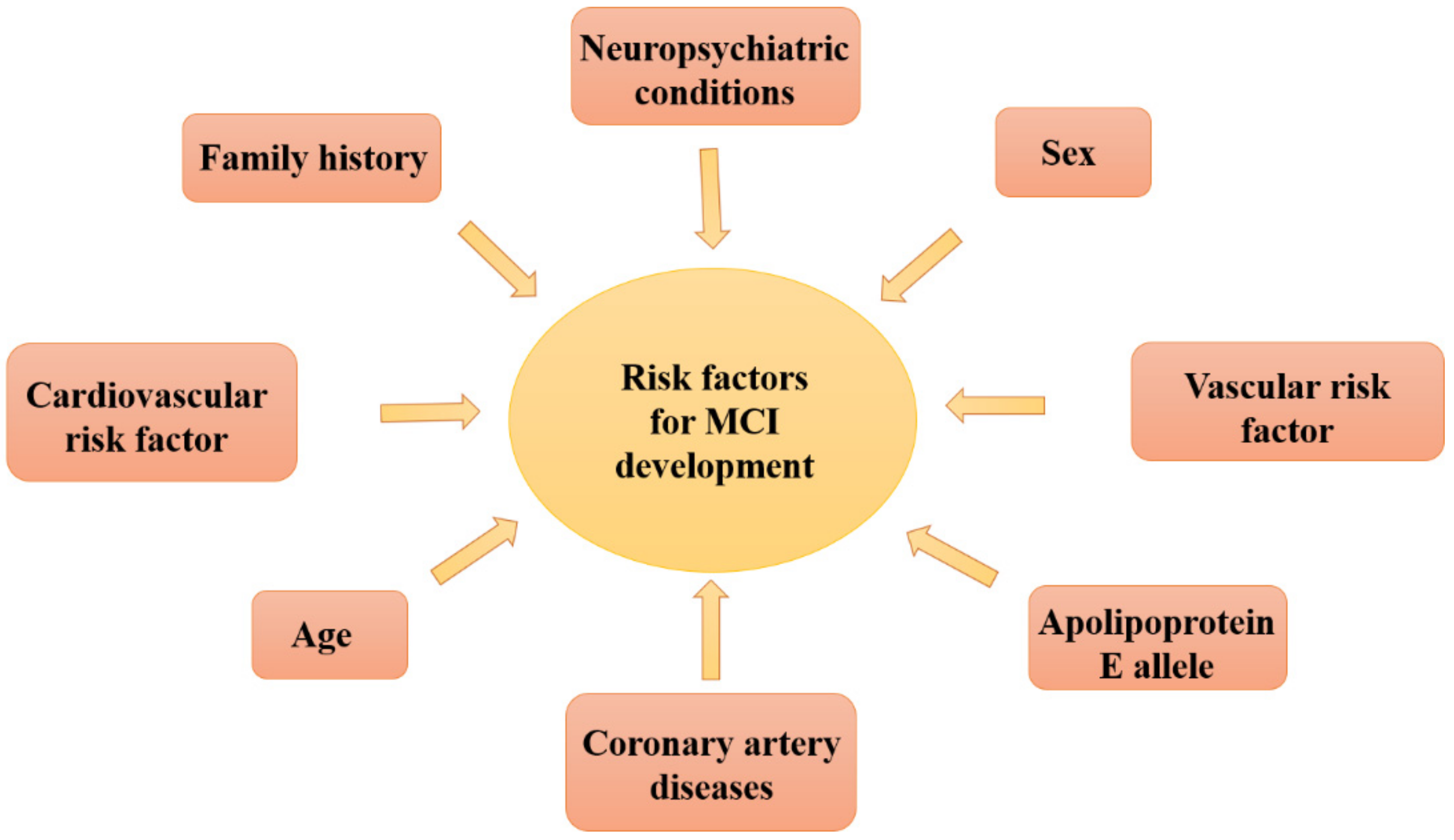
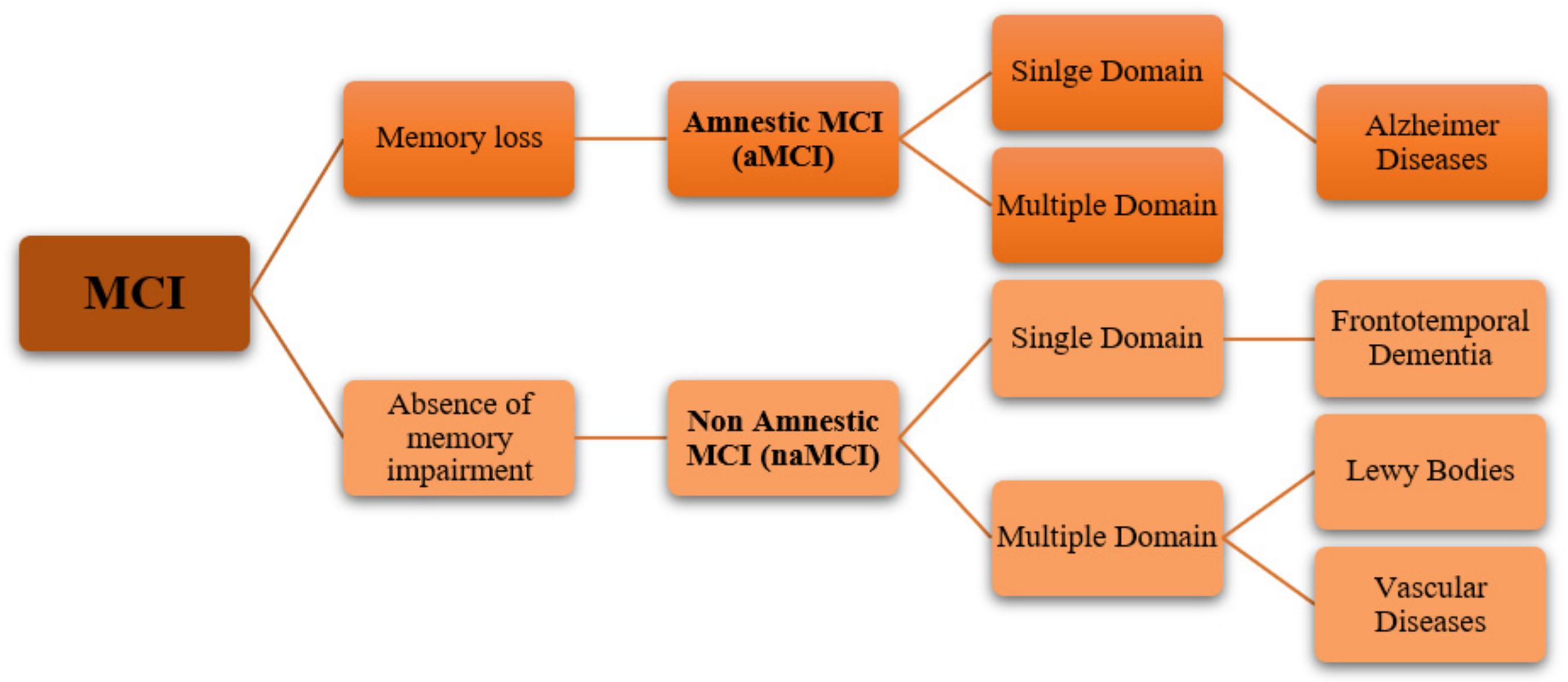
1.1. Mild Cognitive Impairment (MCI) and Mild Dementia: Recent Classification Criteria, Pathogenesis, Therapeutic Aspects
1.2. Therapeutic Approaches in Mild Cognitive Impairment and Mild Dementia
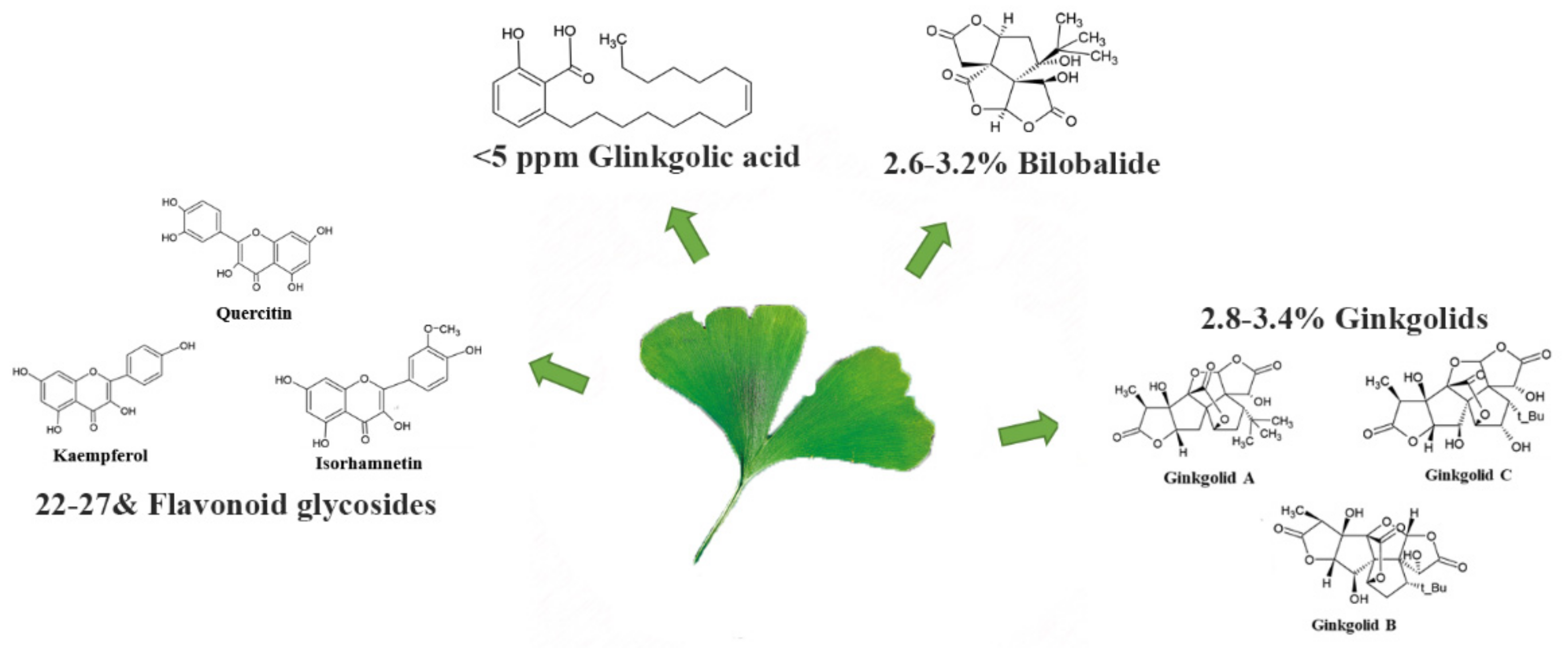
1.3. Ginkgo Biloba: From Traditional Chinese Medicine to Anti-Dementia Drug Based on Scientific Evidence
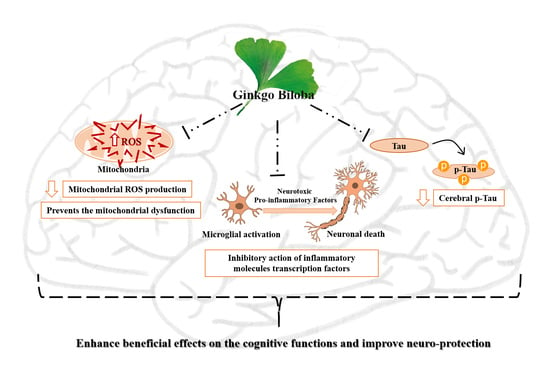
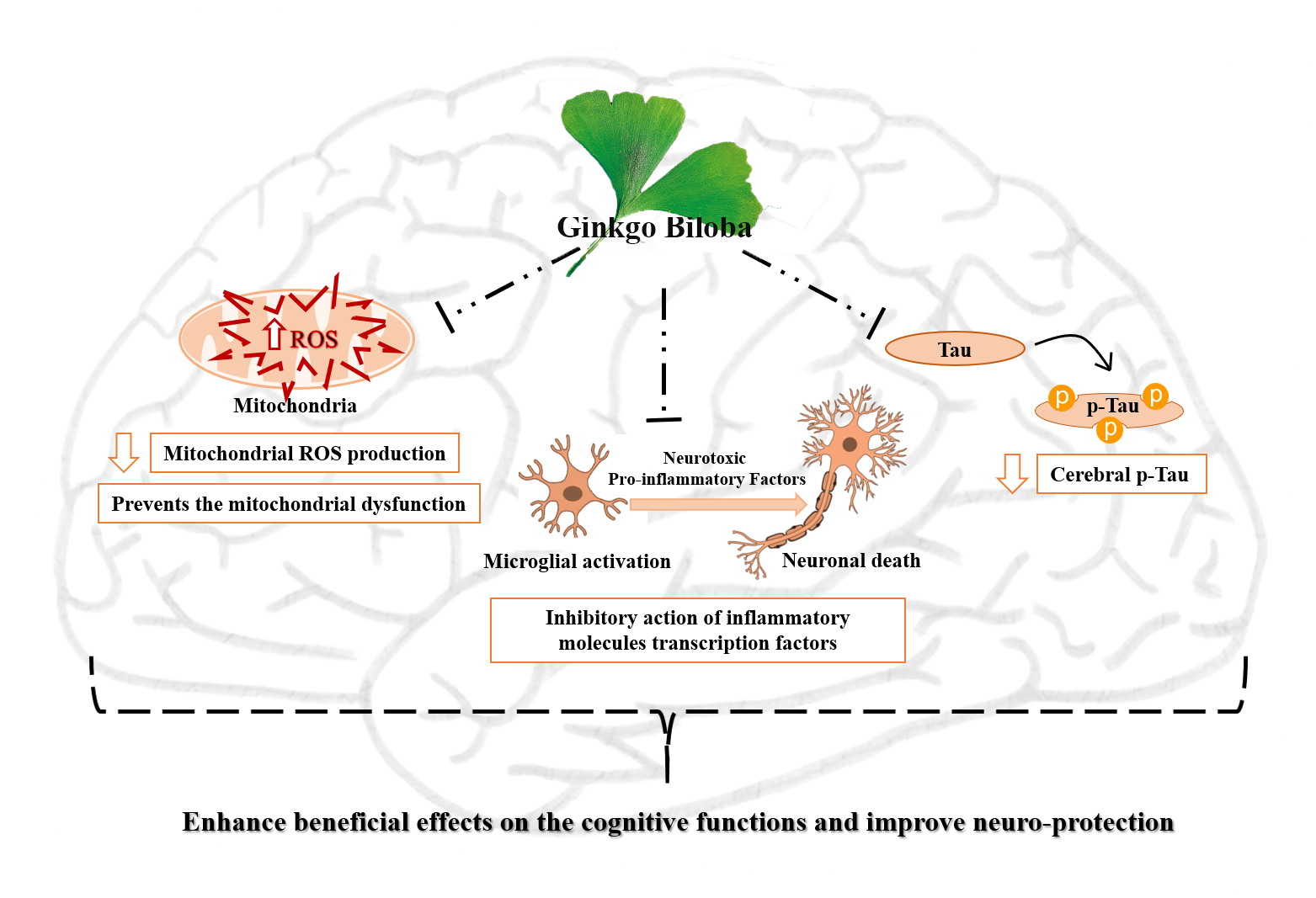
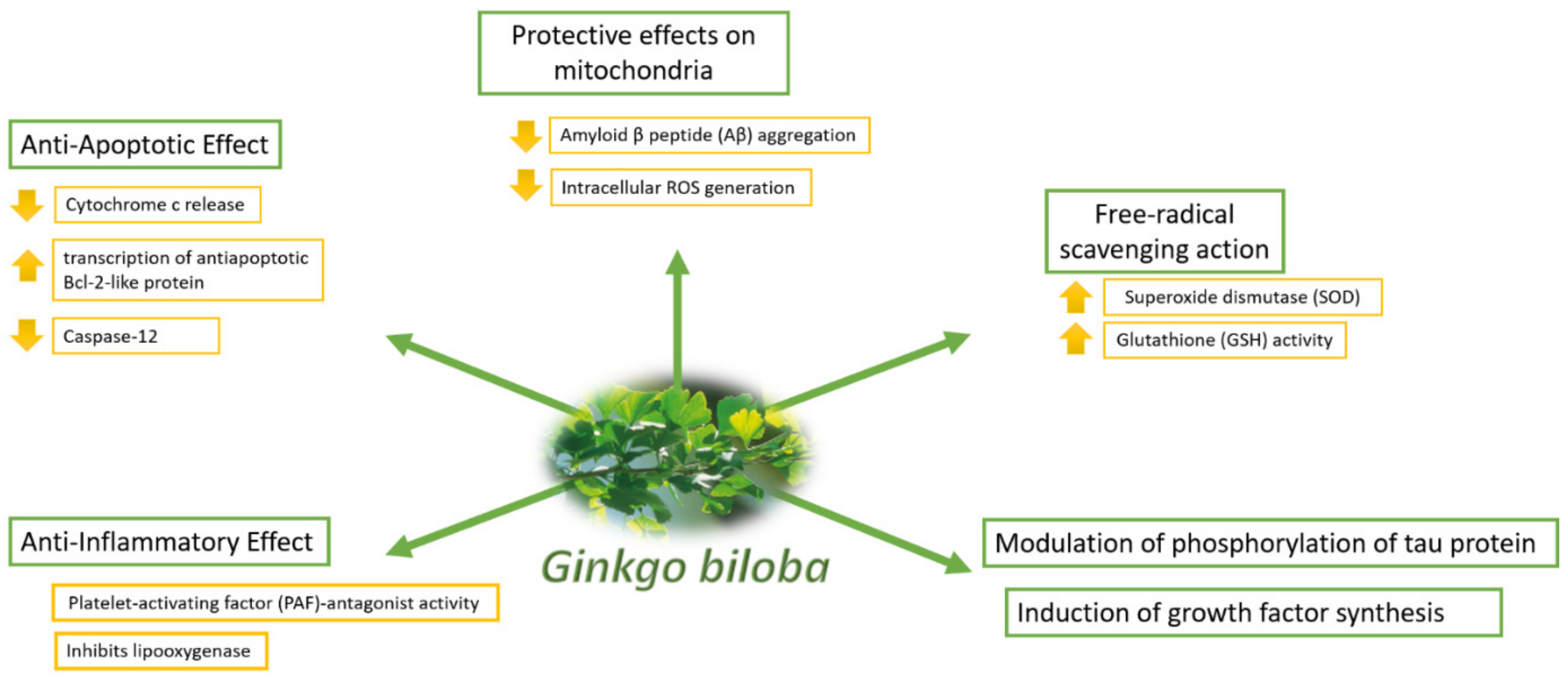
1.3.1. EGb 761® in Basic Research: The Mechanism of Action
1.3.2. EGb 761® in Preclinical and Clinical Dementia: Evidence of Efficacy
1.3.3. EGb 761® in vMCI and Dementia Prevention
1.4. EGb 761® in MCI
1.4.1. EGb 761® Efficacy in Mild and Moderate Dementia with or without Neuropsychiatric Disorders

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Treatment Groups | Results | References |
|---|---|---|---|
| EGb 761® in vMCI, MCI and dementia prevention | |||
| Non-demented patients | EGb 761® or Piracetam and placebo, data collected on cognitive function over a period of twenty years | Patients treated with EGb 761® highlighted a slower cognitive impairment than in Piracetam group. Moreover, EGb 761® patients showed a significant reduction of psychotropic drugs assumption. | [90] |
| Patients with very mild cognitive impairment and low functioning | EGb 761® (240 mg/die) or placebo, for 12 weeks | Patients treated with EGb 761® showed an improvement of memory performances, measured through Wechsler Memory Scale III (human face recognition in pictures) and a significant attention improvement, by using the Vienna Test System Work Performance Series (a computerized math test to keep concentration). | [91] |
| EGb 761® MCI, neurocognitive deficit and dementia | |||
| Patients with amnesic MCI | EGb 761® (240 mg/die) or placebo, for 24 weeks | Patients treated with EGb 761® showed improvement in all the neuropsychiatric symptoms, measured through Neuropsychiatrics Inventory (NPI) sympoms. | [94] |
| Patients with normal cognitive function or MCI | EGb 761® (240 mg/die) or placebo, patients were evaluated every 6 months | This study didn’t demonstrate any significant benefit to prevent dementia development with EGb 761® treatment versus placebo. | [95] |
| Outpatients with mild to moderate dementia (AD or VaD) | EGb 761® (240 mg/die) or placebo, for 24 weeks | Patients treated with EGb 761® demonstrated neuro psychiatric improvement for Neuropsychiatric Inventory (NPI) symptoms. | [96] |
| Outpatients 24-week with mild to moderate dementia (Alzheimer’s disease or vascular dementia) associated with neuropsychiatric symptoms | EGb 761® (240 mg/die) or placebo, for 24 weeks | Treatment with EGb 761® led to a significant and clinically relevant improvement in patients’ cognition, psychopathology, functional measures and quality of life. | [97] |
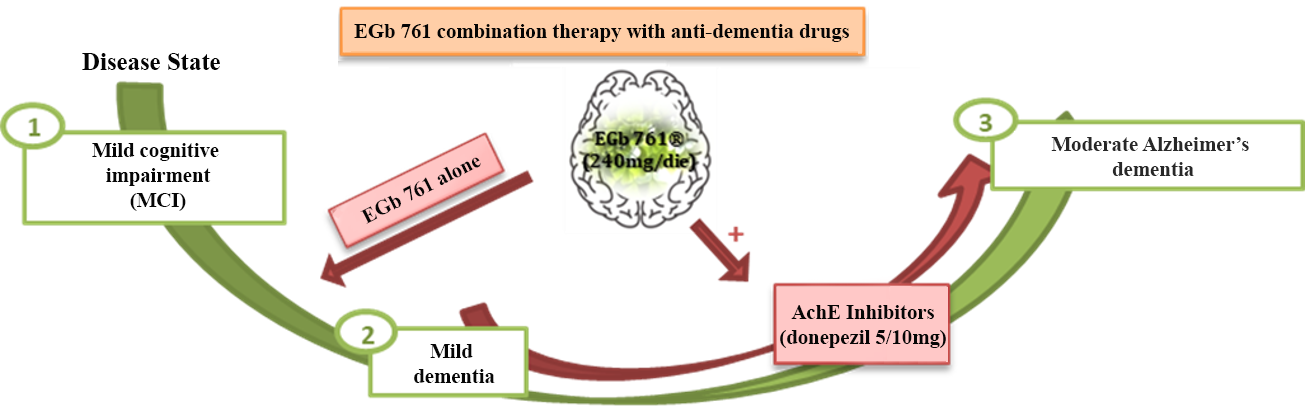
1.4.2. EGb 761® Efficacy and Combined (AChEIs and EGb 761® Association) or Compared (AChEIs versus EGb 761®) Therapy in Mild or Moderate Dementia
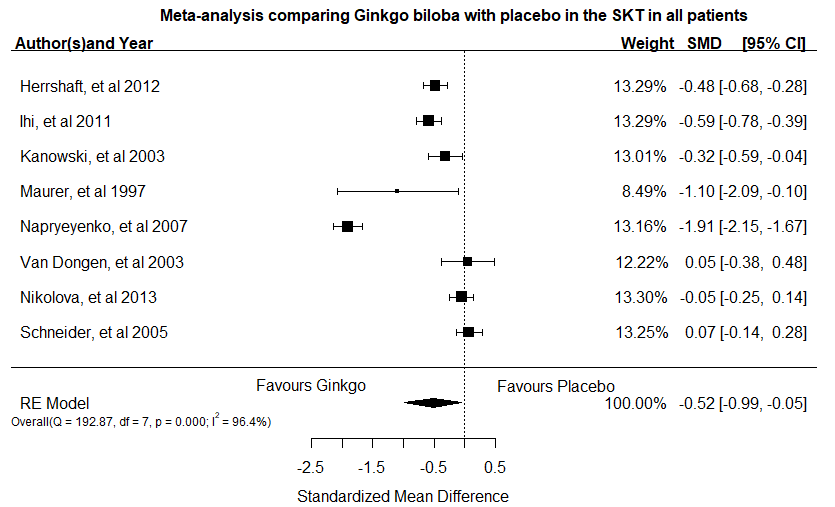
1.4.3. EGb 761® Efficacy Verified through RCTs Meta-Analysis in MCI, Mild and Moderate Dementia with or without Behavior Deficits
| Meta-Analysis Studies (Inclusion Criteria) | Treatment Groups | Results | References |
|---|---|---|---|
| Patients affected by dementia, associated with psycho-behavioral deficits | EGb 761® (240 mg/die) or placebo | Patients treated with EGb 761® showed benefits on cognitive decline stabilization or slowing down, on ADL and neuro psychiatric deficit for MCI, Alzheimer’s and dementia (with/without neuropsychiatric problems) patients. | [44] |
| Patients with a diagnosis of AD, VaD, or mixed dementia | EGb 761® (120 mg/die) or EGb 761® (240 mg/die) or placebo | EGb 761® (240 mg/die; best dosage) has been demonstrated efficacy on cognitive functions, including significant neuropsychiatric deficits in patients with dementia. | [15] |
| Patients with AD or AD + VaD patients | EGb 761® (120 mg/die) or EG b761® (240 mg/die) or placebo | Patients treated with EGb 761® (240 mg/die) showed benefits versus placebo for cognitive deficits, through Syndrom–Kurztest [SKT] analysis. | [104] |
| Patients with the diagnosis of AD, VaD or mixed dementia with behavioral and psychological symptoms (BPSD) | EGb 761® (240 mg/die) or placebo | EGb 761® ginkgo biloba extract (240 mg/die) improved the patients’ cognitive performance, BPSD, functional abilities and general condition. | [105] |
| Patients with MCI and dementia (AD, VaD or AD + VaD, mixed dementia) | EGb 761® (240 mg/die) or placebo | EGb 761® showed benefit versus placebo for cognition, behavior and activities of daily living in patients with MCI and dementia. | [106] |
| Patients with dementia (probable AD, VaD or AD +CVD) | EGb 761® (240 mg/die) or placebo | EGb 761® improved neuro-psychiatric symptoms, in AD, VaD or AD + CVD patients, except for delirium, hallucination and euphoria. | [107] |
2. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jongsiriyanyong, S.; Limpawattana, P. Mild Cognitive Impairment in Clinical Practice: A Review Article. Am. J. Alzheimers Dis. Dement. 2018, 33, 500–507. [Google Scholar] [CrossRef]
- Bondi, M.W.; Edmonds, E.C.; Salmon, D.P. Alzheimer’s Disease: Past, Present, and Future. J. Int. Neuropsychol. Soc. 2017, 23, 818–831. [Google Scholar] [CrossRef]
- Ma, L. Depression, Anxiety, and Apathy in Mild Cognitive Impairment: Current Perspectives. Front. Aging Neurosci. 2020, 12, 9. [Google Scholar] [CrossRef]
- Vlachos, G.S.; Scarmeas, N. Dietary interventions in mild cognitive impairment and dementia. Dialog. Clin. Neurosci. 2019, 21, 69–82. [Google Scholar]
- McGrattan, A.M.; McEvoy, C.T.; McGuinness, B.; McKinley, M.C.; Woodside, J.V. Effect of dietary interventions in mild cognitive impairment: A systematic review. Br. J. Nutr. 2018, 120, 1388–1405. [Google Scholar] [CrossRef] [PubMed]
- Olivera-Pueyo, J.; Pelegrin-Valero, C. Dietary supplements for cognitive impairment. Actas Esp. Psiquiatr. 2017, 45, 37–47. [Google Scholar] [PubMed]
- Ilari, S.; Giancotti, L.A.; Lauro, F.; Dagostino, C.; Gliozzi, M.; Malafoglia, V.; Sansone, L.; Palma, E.; Tafani, M.; Russo, M.A.; et al. Antioxidant modulation of sirtuin 3 during acute inflammatory pain: The ROS control. Pharmacol. Res. 2020, 157, 104851. [Google Scholar] [CrossRef] [PubMed]
- Lauro, F.; Giancotti, L.A.; Ilari, S.; Dagostino, C.; Gliozzi, M.; Morabito, C.; Malafoglia, V.; Raffaeli, W.; Muraca, M.; Goffredo, B.M.; et al. Inhibition of Spinal Oxidative Stress by Bergamot Polyphenolic Fraction Attenuates the Development of Morphine Induced Tolerance and Hyperalgesia in Mice. PLoS ONE 2016, 11, e0156039. [Google Scholar] [CrossRef] [PubMed]
- Lauro, F.; Ilari, S.; Giancotti, L.A.; Ventura, C.A.; Morabito, C.; Gliozzi, M.; Malafoglia, V.; Palma, E.; Paolino, D.; Mollace, V.; et al. Pharmacological effect of a new idebenone formulation in a model of carrageenan-induced inflammatory pain. Pharmacol. Res. 2016, 111, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Ilari, S.; Giancotti, L.A.; Lauro, F.; Gliozzi, M.; Malafoglia, V.; Palma, E.; Tafani, M.; Russo, M.A.; Tomino, C.; Fini, M.; et al. Natural Antioxidant Control of Neuropathic Pain-Exploring the Role of Mitochondrial SIRT3 Pathway. Antioxidants 2020, 9, 1103. [Google Scholar] [CrossRef]
- Liu, H.; Ye, M.; Guo, H. An Updated Review of Randomized Clinical Trials Testing the Improvement of Cognitive Function of Ginkgo biloba Extract in Healthy People and Alzheimer’s Patients. Front. Pharmacol. 2019, 10, 1688. [Google Scholar] [CrossRef]
- Ramassamy, C.; Longpre, F.; Christen, Y. Ginkgo biloba extract (EGb 761) in Alzheimer’s disease: Is there any evidence? Curr. Alzheimer Res. 2007, 4, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Bonassi, S.; Prinzi, G.; Lamonaca, P.; Russo, P.; Paximadas, I.; Rasoni, G.; Rossi, R.; Ruggi, M.; Malandrino, S.; Sanchez-Flores, M.; et al. Clinical and genomic safety of treatment with Ginkgo biloba L. leaf extract (IDN 5933/Ginkgoselect(R)Plus) in elderly: A randomised placebo-controlled clinical trial [GiBiEx]. BMC Complement. Altern. Med. 2018, 18, 22. [Google Scholar] [CrossRef]
- Singh, S.K.; Srivastav, S.; Castellani, R.J.; Plascencia-Villa, G.; Perry, G. Neuroprotective and Antioxidant Effect of Ginkgo biloba Extract Against AD and Other Neurological Disorders. Neurotherapeutics 2019, 16, 666–674. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, S.; Schlaefke, S. Efficacy and tolerability of Ginkgo biloba extract EGb 761(R) in dementia: A systematic review and meta-analysis of randomized placebo-controlled trials. Clin. Interv. Aging 2014, 9, 2065–2077. [Google Scholar] [CrossRef]
- Meng, M.; Ai, D.; Sun, L.; Xu, X.; Cao, X. EGb 761 inhibits Abeta1-42-induced neuroinflammatory response by suppressing P38 MAPK signaling pathway in BV-2 microglial cells. Neuroreport 2019, 30, 434–440. [Google Scholar] [CrossRef]
- D’Amelio, M.; Rossini, P.M. Brain excitability and connectivity of neuronal assemblies in Alzheimer’s disease: From animal models to human findings. Prog. Neurobiol. 2012, 99, 42–60. [Google Scholar] [CrossRef]
- Fernandez-Perez, E.J.; Gallegos, S.; Armijo-Weingart, L.; Araya, A.; Riffo-Lepe, N.O.; Cayuman, F.; Aguayo, L.G. Changes in neuronal excitability and synaptic transmission in nucleus accumbens in a transgenic Alzheimer’s disease mouse model. Sci. Rep. 2020, 10, 19606. [Google Scholar] [CrossRef]
- Campora, M.; Francesconi, V.; Schenone, S.; Tasso, B.; Tonelli, M. Journey on Naphthoquinone and Anthraquinone Derivatives: New Insights in Alzheimer’s Disease. Pharmaceuticals 2021, 14, 33. [Google Scholar] [CrossRef] [PubMed]
- Dugger, B.N.; Dickson, D.W. Pathology of Neurodegenerative Diseases. Cold Spring Harb. Perspect. Biol. 2017, 9, a028035. [Google Scholar] [CrossRef]
- Matej, R.; Tesar, A.; Rusina, R. Alzheimer’s disease and other neurodegenerative dementias in comorbidity: A clinical and neuropathological overview. Clin. Biochem. 2019, 73, 26–31. [Google Scholar] [CrossRef]
- Rossini, P.M.; Di Iorio, R.; Granata, G.; Miraglia, F.; Vecchio, F. From Mild Cognitive Impairment to Alzheimer’s Disease: A New Perspective in the “Land” of Human Brain Reactivity and Connectivity. J. Alzheimers Dis. 2016, 53, 1389–1393. [Google Scholar] [CrossRef]
- Costa, A.; Bak, T.; Caffarra, P.; Caltagirone, C.; Ceccaldi, M.; Collette, F.; Crutch, S.; Della Sala, S.; Demonet, J.F.; Dubois, B.; et al. The need for harmonisation and innovation of neuropsychological assessment in neurodegenerative dementias in Europe: Consensus document of the Joint Program for Neurodegenerative Diseases Working Group. Alzheimers Res. Ther. 2017, 9, 27. [Google Scholar] [CrossRef]
- Lam, C.L.M.; Yiend, J.; Lee, T.M.C. Imaging and neuropsychological correlates of white matter lesions in different subtypes of Mild Cognitive Impairment: A systematic review. NeuroRehabilitation 2017, 41, 189–204. [Google Scholar] [CrossRef]
- Guan, H.; Liu, T.; Jiang, J.; Tao, D.; Zhang, J.; Niu, H.; Zhu, W.; Wang, Y.; Cheng, J.; Kochan, N.A.; et al. Classifying MCI Subtypes in Community-Dwelling Elderly Using Cross-Sectional and Longitudinal MRI-Based Biomarkers. Front. Aging Neurosci. 2017, 9, 309. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, Y.; Takano, H.; Sakata, M.; Maruo, K.; Nakagome, K.; Matsuda, H. Discrete effect of each mild behavioural impairment category on dementia conversion or cognitive decline in patients with mild cognitive impairment. Psychogeriatrics 2019, 19, 591–600. [Google Scholar] [CrossRef]
- Wahlman, C.; Doyle, T.M.; Little, J.W.; Luongo, L.; Janes, K.; Chen, Z.; Esposito, E.; Tosh, D.K.; Cuzzocrea, S.; Jacobson, K.A.; et al. Chemotherapy-induced pain is promoted by enhanced spinal adenosine kinase levels through astrocyte-dependent mechanisms. Pain 2018, 159, 1025–1034. [Google Scholar] [CrossRef]
- Langa, K.M.; Levine, D.A. The diagnosis and management of mild cognitive impairment: A clinical review. JAMA 2014, 312, 2551–2561. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C. Mild Cognitive Impairment. Continuum 2016, 22, 404–418. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.C.; Price, J.L. Pathologic correlates of nondemented aging, mild cognitive impairment, and early-stage Alzheimer’s disease. J. Mol. Neurosci. 2001, 17, 101–118. [Google Scholar] [CrossRef]
- Sanford, A.M. Mild Cognitive Impairment. Clin. Geriatr. Med. 2017, 33, 325–337. [Google Scholar] [CrossRef]
- Khachaturian, Z. The five-five, ten-ten plan for Alzheimer’s disease. Neurobiol. Aging 1992, 13, 197–198. [Google Scholar] [CrossRef]
- Karakaya, T.; Fusser, F.; Schroder, J.; Pantel, J. Pharmacological Treatment of Mild Cognitive Impairment as a Prodromal Syndrome of Alzheimer s Disease. Curr. Neuropharmacol. 2013, 11, 102–108. [Google Scholar] [CrossRef]
- Vanacore, N.; Bianchi, C.; Da Cas, R.; Rossi, M. Use of antiparkinsonian drugs in the Umbria Region. Neurol. Sci. 2003, 24, 221–222. [Google Scholar] [CrossRef] [PubMed]
- Ibach, B.; Haen, E. Acetylcholinesterase inhibition in Alzheimer’s Disease. Curr. Pharm. Des. 2004, 10, 231–251. [Google Scholar] [CrossRef] [PubMed]
- Algin, D.I.; Atalay, S.D.; Ozkan, S.; Adapinar, D.O.; Sivrioz, I.A. Memantine improves semantic memory in patients with amnestic mild cognitive impairment: A single-photon emission computed tomography study. J. Int. Med. Res. 2017, 45, 2053–2064. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Barbagallo, M. Nutritional prevention of cognitive decline and dementia. Acta Biomed. 2018, 89, 276–290. [Google Scholar] [CrossRef] [PubMed]
- Caesar, W. Of Ginkgo EGb on GBL—A long path to rational phytopharmacy. Pharm. Unserer Zeit 2009, 38, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.W.; Chen, J.Y.; Ouyang, D.; Lu, J.H. Quercetin in Animal Models of Alzheimer’s Disease: A Systematic Review of Preclinical Studies. Int. J. Mol. Sci. 2020, 21, 493. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Liu, J.; Wu, F.; Yew, D.T. Ginkgo biloba extract in Alzheimer’s disease: From action mechanisms to medical practice. Int. J. Mol. Sci. 2010, 11, 107–123. [Google Scholar] [CrossRef] [PubMed]
- DeFeudis, F.V. Ginkgo Biloba Extract (EGb 761): From Chemistry to the Clinic; Ullstein Medical: Berlin, Germany, 1998. [Google Scholar]
- Gardner, C.D.; Taylor-Piliae, R.E.; Kiazand, A.; Nicholus, J.; Rigby, A.J.; Farquhar, J.W. Effect of Ginkgo biloba (EGb 761) on treadmill walking time among adults with peripheral artery disease: A randomized clinical trial. J. Cardiopulm. Rehabil. Prev. 2008, 28, 258–265. [Google Scholar] [CrossRef]
- Tan, M.S.; Yu, J.T.; Tan, C.C.; Wang, H.F.; Meng, X.F.; Wang, C.; Jiang, T.; Zhu, X.C.; Tan, L. Efficacy and adverse effects of ginkgo biloba for cognitive impairment and dementia: A systematic review and meta-analysis. J. Alzheimers Dis. 2015, 43, 589–603. [Google Scholar] [CrossRef] [PubMed]
- Cave, A.E.; Chang, D.H.; Munch, G.W.; Steiner, G.Z. Efficacy of Cognition Support Formula(R) on cognitive function in older adults with subjective cognitive impairment: A protocol for a 26-week, randomised, double-blind, placebo-controlled trial. Trials 2019, 20, 345. [Google Scholar] [CrossRef]
- Kandiah, N.; Ong, P.A.; Yuda, T.; Ng, L.L.; Mamun, K.; Merchant, R.A.; Chen, C.; Dominguez, J.; Marasigan, S.; Ampil, E.; et al. Treatment of dementia and mild cognitive impairment with or without cerebrovascular disease: Expert consensus on the use of Ginkgo biloba extract, EGb 761((R)). CNS Neurosci. Ther. 2019, 25, 288–298. [Google Scholar] [CrossRef]
- Liu, L.; Zhang, C.; Kalionis, B.; Wan, W.; Murthi, P.; Chen, C.; Li, Y.; Xia, S. EGb761 protects against Abeta1-42 oligomer-induced cell damage via endoplasmic reticulum stress activation and Hsp70 protein expression increase in SH-SY5Y cells. Exp. Gerontol. 2016, 75, 56–63. [Google Scholar] [CrossRef]
- Smith, J.V.; Luo, Y. Elevation of oxidative free radicals in Alzheimer’s disease models can be attenuated by Ginkgo biloba extract EGb 761. J. Alzheimers Dis. 2003, 5, 287–300. [Google Scholar] [CrossRef]
- ESCOP; Phytotherapy (ESCOP). ESCOP Monographs: The Scientific Foundation for Herbal Medicinal Products; European Scientific Cooperative on Phytotherapy: Yasit, UK, 2003. [Google Scholar]
- Bone, K.; Mills, S. Principles and Practice of Phytotherapy—E-Book: Modern Herbal Medicine; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Haramaki, N.; Aggarwal, S.; Kawabata, T.; Droy-Lefaix, M.T.; Packer, L. Effects of natural antioxidant ginkgo biloba extract (EGB 761) on myocardial ischemia-reperfusion injury. Free Radic. Biol. Med. 1994, 16, 789–794. [Google Scholar] [CrossRef]
- Bridi, R.; Crossetti, F.P.; Steffen, V.M.; Henriques, A.T. The antioxidant activity of standardized extract of Ginkgo biloba (EGb 761) in rats. Phytother. Res. 2001, 15, 449–451. [Google Scholar] [CrossRef] [PubMed]
- Eckert, A.; Keil, U.; Kressmann, S.; Schindowski, K.; Leutner, S.; Leutz, S.; Muller, W.E. Effects of EGb 761 Ginkgo biloba extract on mitochondrial function and oxidative stress. Pharmacopsychiatry 2003, 36 (Suppl. 1) (Suppl. 1), S15–S23. [Google Scholar] [CrossRef]
- Jiang, X.; Nie, B.; Fu, S.; Hu, J.; Yin, L.; Lin, L.; Wang, X.; Lu, P.; Xu, X.M. EGb761 protects hydrogen peroxide-induced death of spinal cord neurons through inhibition of intracellular ROS production and modulation of apoptotic regulating genes. J. Mol. Neurosci. 2009, 38, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Mozet, C.; Martin, H.; Welt, K.; Engel, C.; Fitzl, G. The effect of Ginkgo biloba extract (EGb 761) on parameters of oxidative stress in different regions of aging rat brains after acute hypoxia. Aging Clin. Exp. Res. 2011, 23, 255–263. [Google Scholar] [CrossRef]
- Sastre, J.; Millan, A.; De La Asuncion, J.G.; Pla, R.; Juan, G.; Pallardo, F.V.; O’Connor, E.; Martin, J.A.; Droy-Lefaix, M.-T.; Viña, J. A Ginkgo biloba extract (EGb 761) prevents mitochondrial aging by protecting against oxidative stress. Free Radic. Biol. Med. 1998, 24, 298–304. [Google Scholar] [CrossRef]
- Abdel-Kader, R.; Hauptmann, S.; Keil, U.; Scherping, I.; Leuner, K.; Eckert, A.; Muller, W.E. Stabilization of mitochondrial function by Ginkgo biloba extract (EGb 761). Pharmacol. Res. 2007, 56, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Muller, W.E.; Heiser, J.; Leuner, K. Effects of the standardized Ginkgo biloba extract EGb 761(R) on neuroplasticity. Int. Psychogeriatr. 2012, 24 (Suppl. S1) (Suppl. S1), S21–S24. [Google Scholar] [CrossRef]
- Kumar, A.; Singh, A. A review on mitochondrial restorative mechanism of antioxidants in Alzheimer’s disease and other neurological conditions. Front. Pharmacol. 2015, 6, 206. [Google Scholar] [CrossRef] [PubMed]
- Leuner, K.; Hauptmann, S.; Abdel-Kader, R.; Scherping, I.; Keil, U.; Strosznajder, J.B.; Eckert, A.; Muller, W.E. Mitochondrial dysfunction: The first domino in brain aging and Alzheimer’s disease? Antioxid. Redox Signal. 2007, 9, 1659–1675. [Google Scholar] [CrossRef] [PubMed]
- Muller, W.E.; Eckert, A.; Eckert, G.P.; Fink, H.; Friedland, K.; Gauthier, S.; Hoerr, R.; Ihl, R.; Kasper, S.; Moller, H.J. Therapeutic efficacy of the Ginkgo special extract EGb761((R)) within the framework of the mitochondrial cascade hypothesis of Alzheimer’s disease. World J. Biol. Psychiatry 2019, 20, 173–189. [Google Scholar] [CrossRef]
- Janssens, D.; Michiels, C.; Delaive, E.; Eliaers, F.; Drieu, K.; Remacle, J. Protection of hypoxia-induced ATP decrease in endothelial cells by ginkgo biloba extract and bilobalide. Biochem. Pharmacol. 1995, 50, 991–999. [Google Scholar] [CrossRef]
- Eckert, A.; Keil, U.; Scherping, I.; Hauptmann, S.; Muller, W.E. Stabilization of mitochondrial membrane potential and improvement of neuronal energy metabolism by Ginkgo biloba extract EGb 761. Ann. N. Y. Acad. Sci. 2005, 1056, 474–485. [Google Scholar] [CrossRef]
- Rhein, V.; Giese, M.; Baysang, G.; Meier, F.; Rao, S.; Schulz, K.L.; Hamburger, M.; Eckert, A. Ginkgo biloba extract ameliorates oxidative phosphorylation performance and rescues abeta-induced failure. PLoS ONE 2010, 5, e12359. [Google Scholar] [CrossRef] [PubMed]
- Baliutyte, G.; Trumbeckaite, S.; Baniene, R.; Borutaite, V.; Toleikis, A. Effects of standardized extract of Ginkgo biloba leaves EGb761 on mitochondrial functions: Mechanism(s) of action and dependence on the source of mitochondria and respiratory substrate. J. Bioenerg. Biomembr. 2014, 46, 493–501. [Google Scholar] [CrossRef]
- Liu, X.; Hao, W.; Qin, Y.; Decker, Y.; Wang, X.; Burkart, M.; Schotz, K.; Menger, M.D.; Fassbender, K.; Liu, Y. Long-term treatment with Ginkgo biloba extract EGb 761 improves symptoms and pathology in a transgenic mouse model of Alzheimer’s disease. Brain Behav. Immun. 2015, 46, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Wan, W.; Zhang, C.; Danielsen, M.; Li, Q.; Chen, W.; Chan, Y.; Li, Y. EGb761 improves cognitive function and regulates inflammatory responses in the APP/PS1 mouse. Exp. Gerontol. 2016, 81, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Gargouri, B.; Carstensen, J.; Bhatia, H.S.; Huell, M.; Dietz, G.P.H.; Fiebich, B.L. Anti-neuroinflammatory effects of Ginkgo biloba extract EGb761 in LPS-activated primary microglial cells. Phytomedicine 2018, 44, 45–55. [Google Scholar] [CrossRef]
- Ahlemeyer, B.; Mowes, A.; Krieglstein, J. Inhibition of serum deprivation- and staurosporine-induced neuronal apoptosis by Ginkgo biloba extract and some of its constituents. Eur. J. Pharmacol. 1999, 367, 423–430. [Google Scholar] [CrossRef]
- Schindowski, K.; Leutner, S.; Kressmann, S.; Eckert, A.; Muller, W.E. Age-related increase of oxidative stress-induced apoptosis in mice prevention by Ginkgo biloba extract (EGb761). J. Neural Transm. 2001, 108, 969–978. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Smith, J.V.; Paramasivam, V.; Burdick, A.; Curry, K.J.; Buford, J.P.; Khan, I.; Netzer, W.J.; Xu, H.; Butko, P. Inhibition of amyloid-beta aggregation and caspase-3 activation by the Ginkgo biloba extract EGb761. Proc. Natl. Acad. Sci. USA 2002, 99, 12197–12202. [Google Scholar] [CrossRef]
- Colciaghi, F.; Borroni, B.; Zimmermann, M.; Bellone, C.; Longhi, A.; Padovani, A.; Cattabeni, F.; Christen, Y.; Di Luca, M. Amyloid precursor protein metabolism is regulated toward alpha-secretase pathway by Ginkgo biloba extracts. Neurobiol. Dis. 2004, 16, 454–460. [Google Scholar] [CrossRef]
- Blasko, I.; Kemmler, G.; Krampla, W.; Jungwirth, S.; Wichart, I.; Jellinger, K.; Tragl, K.H.; Fischer, P. Plasma amyloid beta protein 42 in non-demented persons aged 75 years: Effects of concomitant medication and medial temporal lobe atrophy. Neurobiol. Aging 2005, 26, 1135–1143. [Google Scholar] [CrossRef]
- Longpre, F.; Garneau, P.; Christen, Y.; Ramassamy, C. Protection by EGb 761 against beta-amyloid-induced neurotoxicity: Involvement of NF-kappaB, SIRT1, and MAPKs pathways and inhibition of amyloid fibril formation. Free Radic. Biol. Med. 2006, 41, 1781–1794. [Google Scholar] [CrossRef]
- Shi, C.; Zhao, L.; Zhu, B.; Li, Q.; Yew, D.T.; Yao, Z.; Xu, J. Protective effects of Ginkgo biloba extract (EGb761) and its constituents quercetin and ginkgolide B against beta-amyloid peptide-induced toxicity in SH-SY5Y cells. Chem. Biol. Interact. 2009, 181, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Wan, W.B.; Cao, L.; Liu, L.M.; Kalionis, B.; Chen, C.; Tai, X.T.; Li, Y.M.; Xia, S.J. EGb761 provides a protective effect against Abeta1-42 oligomer-induced cell damage and blood-brain barrier disruption in an in vitro bEnd.3 endothelial model. PLoS ONE 2014, 9, e113126. [Google Scholar] [CrossRef]
- Xie, H.; Wang, J.R.; Yau, L.F.; Liu, Y.; Liu, L.; Han, Q.B.; Zhao, Z.; Jiang, Z.H. Quantitative analysis of the flavonoid glycosides and terpene trilactones in the extract of Ginkgo biloba and evaluation of their inhibitory activity towards fibril formation of beta-amyloid peptide. Molecules 2014, 19, 4466–4478. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Zhang, Y.; Tomic, I.; Hao, W.; Menger, M.D.; Liu, C.; Fassbender, K.; Liu, Y. Ginkgo biloba Extract EGb 761 and Its Specific Components Elicit Protective Protein Clearance Through the Autophagy-Lysosomal Pathway in Tau-Transgenic Mice and Cultured Neurons. J. Alzheimers Dis. 2018, 65, 243–263. [Google Scholar] [CrossRef] [PubMed]
- Fehske, C.J.; Leuner, K.; Muller, W.E. Ginkgo biloba extract (EGb761) influences monoaminergic neurotransmission via inhibition of NE uptake, but not MAO activity after chronic treatment. Pharmacol. Res. 2009, 60, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Yoshitake, T.; Yoshitake, S.; Kehr, J. The Ginkgo biloba extract EGb 761(R) and its main constituent flavonoids and ginkgolides increase extracellular dopamine levels in the rat prefrontal cortex. Br. J. Pharmacol. 2010, 159, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Beck, S.M.; Ruge, H.; Schindler, C.; Burkart, M.; Miller, R.; Kirschbaum, C.; Goschke, T. Effects of Ginkgo biloba extract EGb 761(R) on cognitive control functions, mental activity of the prefrontal cortex and stress reactivity in elderly adults with subjective memory impairment—A randomized double-blind placebo-controlled trial. Hum. Psychopharmacol. 2016, 31, 227–242. [Google Scholar] [CrossRef]
- Tchantchou, F.; Xu, Y.; Wu, Y.; Christen, Y.; Luo, Y. EGb 761 enhances adult hippocampal neurogenesis and phosphorylation of CREB in transgenic mouse model of Alzheimer’s disease. FASEB J. 2007, 21, 2400–2408. [Google Scholar] [CrossRef] [PubMed]
- Tchantchou, F.; Lacor, P.N.; Cao, Z.; Lao, L.; Hou, Y.; Cui, C.; Klein, W.L.; Luo, Y. Stimulation of neurogenesis and synaptogenesis by bilobalide and quercetin via common final pathway in hippocampal neurons. J. Alzheimers Dis. 2009, 18, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Kasper, S.; Bancher, C.; Eckert, A.; Forstl, H.; Frolich, L.; Hort, J.; Korczyn, A.D.; Kressig, R.W.; Levin, O.; Palomo, M.S.M. Management of mild cognitive impairment (MCI): The need for national and international guidelines. World J. Biol. Psychiatry 2020, 21, 579–594. [Google Scholar] [CrossRef]
- Massoud, F.; Leger, G.C. Pharmacological treatment of Alzheimer disease. Can. J. Psychiatry 2011, 56, 579–588. [Google Scholar] [CrossRef]
- Baskys, A.; Hou, A.C. Vascular dementia: Pharmacological treatment approaches and perspectives. Clin. Interv. Aging 2007, 2, 327–335. [Google Scholar] [CrossRef]
- Boxer, A.L.; Gold, M.; Feldman, H.; Boeve, B.F.; Dickinson, S.L.; Fillit, H.; Ho, C.; Paul, R.; Pearlman, R.; Sutherland, M.; et al. New directions in clinical trials for frontotemporal lobar degeneration: Methods and outcome measures. Alzheimers Dement. 2020, 16, 131–143. [Google Scholar] [CrossRef]
- Hershey, L.A.; Coleman-Jackson, R. Pharmacological Management of Dementia with Lewy Bodies. Drugs Aging 2019, 36, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Young, J.J.; Balachandran, S.; Garg, G.; Balasubramaniam, M.; Gupta, A.; Tampi, D.J.; Tampi, R.R. Personality and the risk factors for developing behavioral and psychological symptoms of dementia: A narrative review. Neurodegener. Dis. Manag. 2019, 9, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Amieva, H.; Meillon, C.; Helmer, C.; Barberger-Gateau, P.; Dartigues, J.F. Ginkgo biloba extract and long-term cognitive decline: A 20-year follow-up population-based study. PLoS ONE 2013, 8, e52755. [Google Scholar] [CrossRef] [PubMed]
- Grass-Kapanke, B.; Busmane, A.; Lasmanis, A.; Hoerr, R.; Kaschel, R. Effects of Ginkgo biloba special extract EGb761(R) in very mild cognitive impairment (vMCI). Neurosci. Med. 2011, 2, 48–56. [Google Scholar] [CrossRef]
- Vellas, B.; Coley, N.; Ousset, P.J.; Berrut, G.; Dartigues, J.F.; Dubois, B.; Grandjean, H.; Pasquier, F.; Piette, F.; Robert, P.; et al. Long-term use of standardised Ginkgo biloba extract for the prevention of Alzheimer’s disease (GuidAge): A randomised placebo-controlled trial. Lancet Neurol. 2012, 11, 851–859. [Google Scholar] [CrossRef]
- Scherrer, B.; Andrieu, S.; Ousset, P.J.; Berrut, G.; Dartigues, J.F.; Dubois, B.; Pasquier, F.; Piette, F.; Robert, P.; Touchon, J.; et al. Analysing Time to Event Data in Dementia Prevention Trials: The Example of the GuidAge Study of EGb761. J. Nutr. Health Aging 2015, 19, 1009–1011. [Google Scholar] [CrossRef] [PubMed]
- Gavrilova, S.I.; Preuss, U.W.; Wong, J.W.; Hoerr, R.; Kaschel, R.; Bachinskaya, N.; Group, G.I.S. Efficacy and safety of Ginkgo biloba extract EGb 761 in mild cognitive impairment with neuropsychiatric symptoms: A randomized, placebo-controlled, double-blind, multi-center trial. Int. J. Geriatr. Psychiatry 2014, 29, 1087–1095. [Google Scholar] [CrossRef]
- DeKosky, S.T.; Williamson, J.D.; Fitzpatrick, A.L.; Kronmal, R.A.; Ives, D.G.; Saxton, J.A.; Lopez, O.L.; Burke, G.; Carlson, M.C.; Fried, L.P.; et al. Ginkgo biloba for prevention of dementia: A randomized controlled trial. JAMA 2008, 300, 2253–2262. [Google Scholar] [CrossRef]
- Ihl, R.; Bachinskaya, N.; Korczyn, A.D.; Vakhapova, V.; Tribanek, M.; Hoerr, R.; Napryeyenko, O.; Group, G.S. Efficacy and safety of a once-daily formulation of Ginkgo biloba extract EGb 761 in dementia with neuropsychiatric features: A randomized controlled trial. Int. J. Geriatr. Psychiatry 2011, 26, 1186–1194. [Google Scholar] [CrossRef]
- Herrschaft, H.; Nacu, A.; Likhachev, S.; Sholomov, I.; Hoerr, R.; Schlaefke, S. Ginkgo biloba extract EGb 761(R) in dementia with neuropsychiatric features: A randomised, placebo-controlled trial to confirm the efficacy and safety of a daily dose of 240 mg. J. Psychiatr. Res. 2012, 46, 716–723. [Google Scholar] [CrossRef]
- Yancheva, S.; Ihl, R.; Nikolova, G.; Panayotov, P.; Schlaefke, S.; Hoerr, R.; Group, G.S. Ginkgo biloba extract EGb 761(R), donepezil or both combined in the treatment of Alzheimer’s disease with neuropsychiatric features: A randomised, double-blind, exploratory trial. Aging Ment. Health 2009, 13, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Canevelli, M.; Adali, N.; Kelaiditi, E.; Cantet, C.; Ousset, P.J.; Cesari, M.; Group, I.D. Effects of Gingko biloba supplementation in Alzheimer’s disease patients receiving cholinesterase inhibitors: Data from the ICTUS study. Phytomedicine 2014, 21, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Rapp, M.; Burkart, M.; Kohlmann, T.; Bohlken, J. Similar treatment outcomes with Ginkgo biloba extract EGb 761 and donepezil in Alzheimer’s dementia in very old age: A retrospective observational study. Int. J. Clin. Pharmacol. Ther. 2018, 56, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Mazza, M.; Capuano, A.; Bria, P.; Mazza, S. Ginkgo biloba and donepezil: A comparison in the treatment of Alzheimer’s dementia in a randomized placebo-controlled double-blind study. Eur. J. Neurol. 2006, 13, 981–985. [Google Scholar] [CrossRef]
- Birks, J.; Grimley, E.V.; Van Dongen, M. Ginkgo biloba for cognitive impairment and dementia. Cochrane Database Syst. Rev. 2002, 4, 1–19. [Google Scholar] [CrossRef]
- Birks, J.; Evans, J.G. Ginkgo biloba for cognitive impairment and dementia. Cochrane Database Syst. Rev. 2009, 1, CD003120. [Google Scholar] [CrossRef] [PubMed]
- Hashiguchi, M.; Ohta, Y.; Shimizu, M.; Maruyama, J.; Mochizuki, M. Meta-analysis of the efficacy and safety of Ginkgo biloba extract for the treatment of dementia. J. Pharm. Health Care Sci. 2015, 1, 14. [Google Scholar] [CrossRef]
- Von Gunten, A.; Schlaefke, S.; Uberla, K. Efficacy of Ginkgo biloba extract EGb 761((R)) in dementia with behavioural and psychological symptoms: A systematic review. World J. Biol. Psychiatry 2016, 17, 622–633. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.F.; Huang, L.B.; Zhong, Y.B.; Zhou, Q.H.; Wang, H.L.; Zheng, G.Q.; Lin, Y. An Overview of Systematic Reviews of Ginkgo biloba Extracts for Mild Cognitive Impairment and Dementia. Front. Aging Neurosci. 2016, 8, 276. [Google Scholar] [CrossRef] [PubMed]
- Savaskan, E.; Mueller, H.; Hoerr, R.; von Gunten, A.; Gauthier, S. Treatment effects of Ginkgo biloba extract EGb 761(R) on the spectrum of behavioral and psychological symptoms of dementia: Meta-analysis of randomized controlled trials. Int. Psychogeriatr. 2018, 30, 285–293. [Google Scholar] [CrossRef]
- Knopman, D.S.; Petersen, R.C. Mild cognitive impairment and mild dementia: A clinical perspective. Mayo Clin. Proc. 2014, 89, 1452–1459. [Google Scholar] [CrossRef] [PubMed]
- Kanowski, S.; Hoerr, R. Ginkgo biloba extract EGb 761 in dementia: Intent-to-treat analyses of a 24-week, multi-center, double-blind, placebo-controlled, randomized trial. Pharmacopsychiatry 2003, 36, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Maurer, K.; Ihl, R.; Dierks, T.; Frolich, L. Clinical efficacy of Ginkgo biloba special extract EGb 761 in dementia of the Alzheimer type. J. Psychiatr. Res. 1997, 31, 645–655. [Google Scholar] [CrossRef]
- Napryeyenko, O.; Borzenko, I.; Group, G.-N.S. Ginkgo biloba special extract in dementia with neuropsychiatric features. A randomised, placebo-controlled, double-blind clinical trial. Arzneimittelforschung 2007, 57, 4–11. [Google Scholar] [CrossRef]
- Van Dongen, M.; van Rossum, E.; Kessels, A.; Sielhorst, H.; Knipschild, P. Ginkgo for elderly people with dementia and age-associated memory impairment: A randomized clinical trial. J. Clin. Epidemiol. 2003, 56, 367–376. [Google Scholar] [CrossRef]
- Nikolova, G.; Yancheva, S.; Raychev, I.; Hoerr, R.; PLAGIN Study Group. Ginkgo biloba extract in dementia: A 22-week randomised, placebo-controlled, double-blind trial. Bulg. Neurol. 2013, 14, 139–143. [Google Scholar]
- Schneider, L.S.; DeKosky, S.T.; Farlow, M.R.; Tariot, P.N.; Hoerr, R.; Kieser, M. A randomized, double-blind, placebo-controlled trial of two doses of Ginkgo biloba extract in dementia of the Alzheimer’s type. Curr. Alzheimer Res. 2005, 2, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Open Med. 2009, 3, e123–e130. [Google Scholar] [PubMed]
- Halil, M.; Cankurtaran, M.; Yavuz, B.B.; Ozkayar, N.; Ulger, Z.; Dede, D.S.; Shorbagi, A.; Buyukasik, Y.; Haznedaroglu, I.C.; Arogul, S. No alteration in the PFA-100 in vitro bleeding time induced by the Ginkgo biloba special extract, EGb 761, in elderly patients with mild cognitive impairment. Blood Coagul. Fibrinolysis 2005, 16, 349–353. [Google Scholar] [CrossRef]
- Sollier, C.B.D.; Caplain, H.; Drouet, L. No alteration in platelet function or coagulation induced by EGb761 in a controlled study. Clin. Lab. Haematol. 2003, 25, 251–253. [Google Scholar] [CrossRef] [PubMed]
- Wolf, H.R. Does Ginkgo biloba special extract EGb 761 provide additional effects on coagulation and bleeding when added to acetylsalicylic acid 500 mg daily? Drugs R D 2006, 7, 163–172. [Google Scholar] [CrossRef]






| Dementia | Diagnosis | References |
|---|---|---|
| Mild cognitive impairment (MCI) | Neuropsychological syndrome characterized by emerging cognitive impairment | [84] |
| Alzheimer’s disease (AD) | Neurodegenerative disorder characterized by loss of neurons and synapses in the cerebral cortex and certain subcortical regions. | [85] |
| Vascular dementia (VaD) | Cognitive dysfunctions resulting from brain tissue death due to ischemia caused by vascular disease. | [86] |
| Frontotemporal lobar degeneration (FTLD) | Neurodegenerative disorders characterized by progressive changes in behavior, personality. | [87] |
| Dementia with Lewy bodies (DLB) | Several cognitive, behavioral and neurological symptoms characterized by memory loss, hallucinations, rapid eye movement | [88] |
| Behavioral and psychological and symptoms of dementia” (BPSD) | Neuropsychiatric symptoms and behavioral manifestations (apathy, depression, aggression agitation) associated with dementia. | [89] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomino, C.; Ilari, S.; Solfrizzi, V.; Malafoglia, V.; Zilio, G.; Russo, P.; Proietti, S.; Marcolongo, F.; Scapagnini, G.; Muscoli, C.; et al. Mild Cognitive Impairment and Mild Dementia: The Role of Ginkgo biloba (EGb 761®). Pharmaceuticals 2021, 14, 305. https://doi.org/10.3390/ph14040305
Tomino C, Ilari S, Solfrizzi V, Malafoglia V, Zilio G, Russo P, Proietti S, Marcolongo F, Scapagnini G, Muscoli C, et al. Mild Cognitive Impairment and Mild Dementia: The Role of Ginkgo biloba (EGb 761®). Pharmaceuticals. 2021; 14(4):305. https://doi.org/10.3390/ph14040305
Chicago/Turabian StyleTomino, Carlo, Sara Ilari, Vincenzo Solfrizzi, Valentina Malafoglia, Guglielmo Zilio, Patrizia Russo, Stefania Proietti, Federica Marcolongo, Giovanni Scapagnini, Carolina Muscoli, and et al. 2021. "Mild Cognitive Impairment and Mild Dementia: The Role of Ginkgo biloba (EGb 761®)" Pharmaceuticals 14, no. 4: 305. https://doi.org/10.3390/ph14040305
APA StyleTomino, C., Ilari, S., Solfrizzi, V., Malafoglia, V., Zilio, G., Russo, P., Proietti, S., Marcolongo, F., Scapagnini, G., Muscoli, C., & Rossini, P. M. (2021). Mild Cognitive Impairment and Mild Dementia: The Role of Ginkgo biloba (EGb 761®). Pharmaceuticals, 14(4), 305. https://doi.org/10.3390/ph14040305