
Pharmacology and Adverse Events of Emergency-Use Authorized Medication in Moderate to Severe COVID-19



Abstract
:1. Introduction
Chemical Structure and Molecular Properties
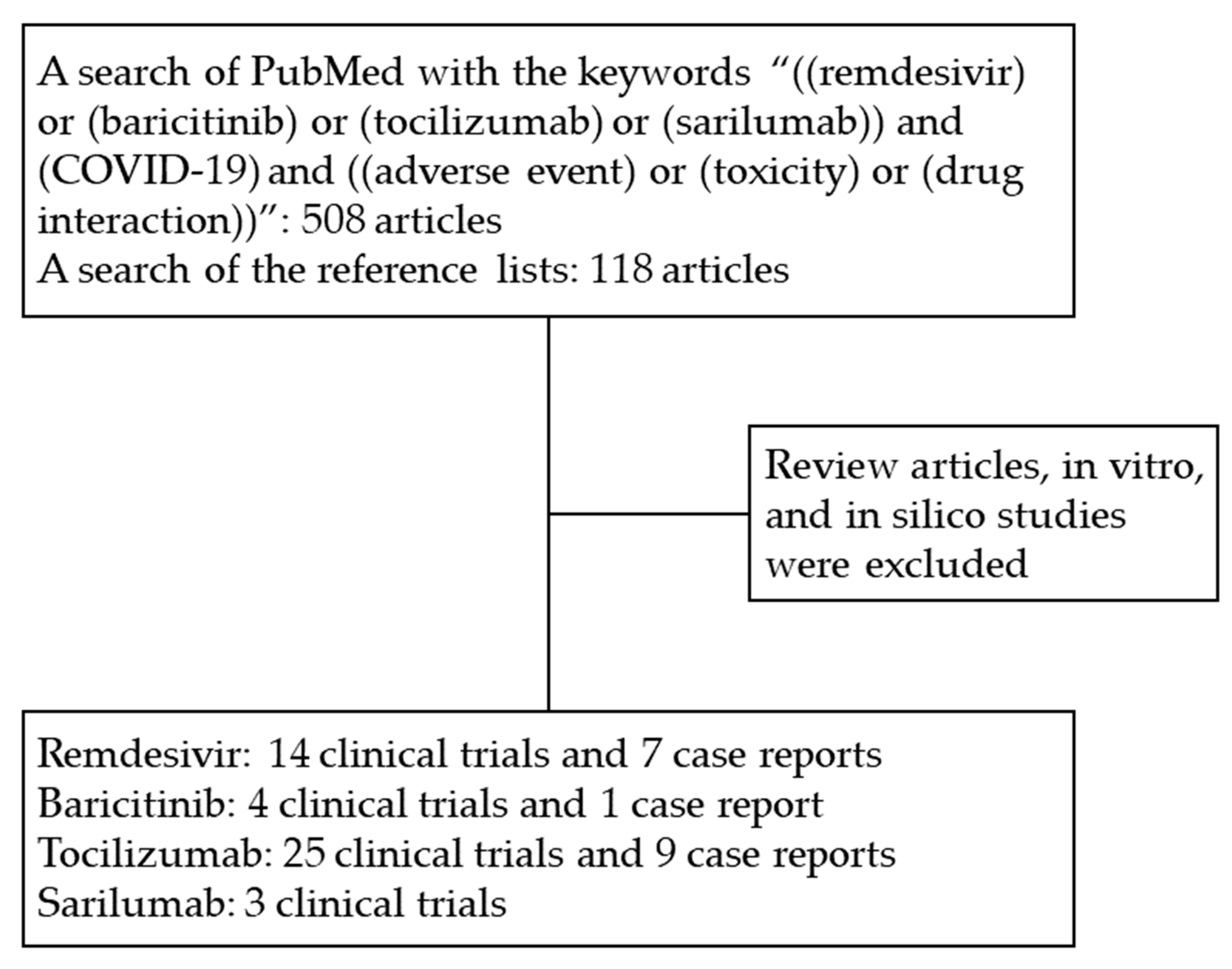
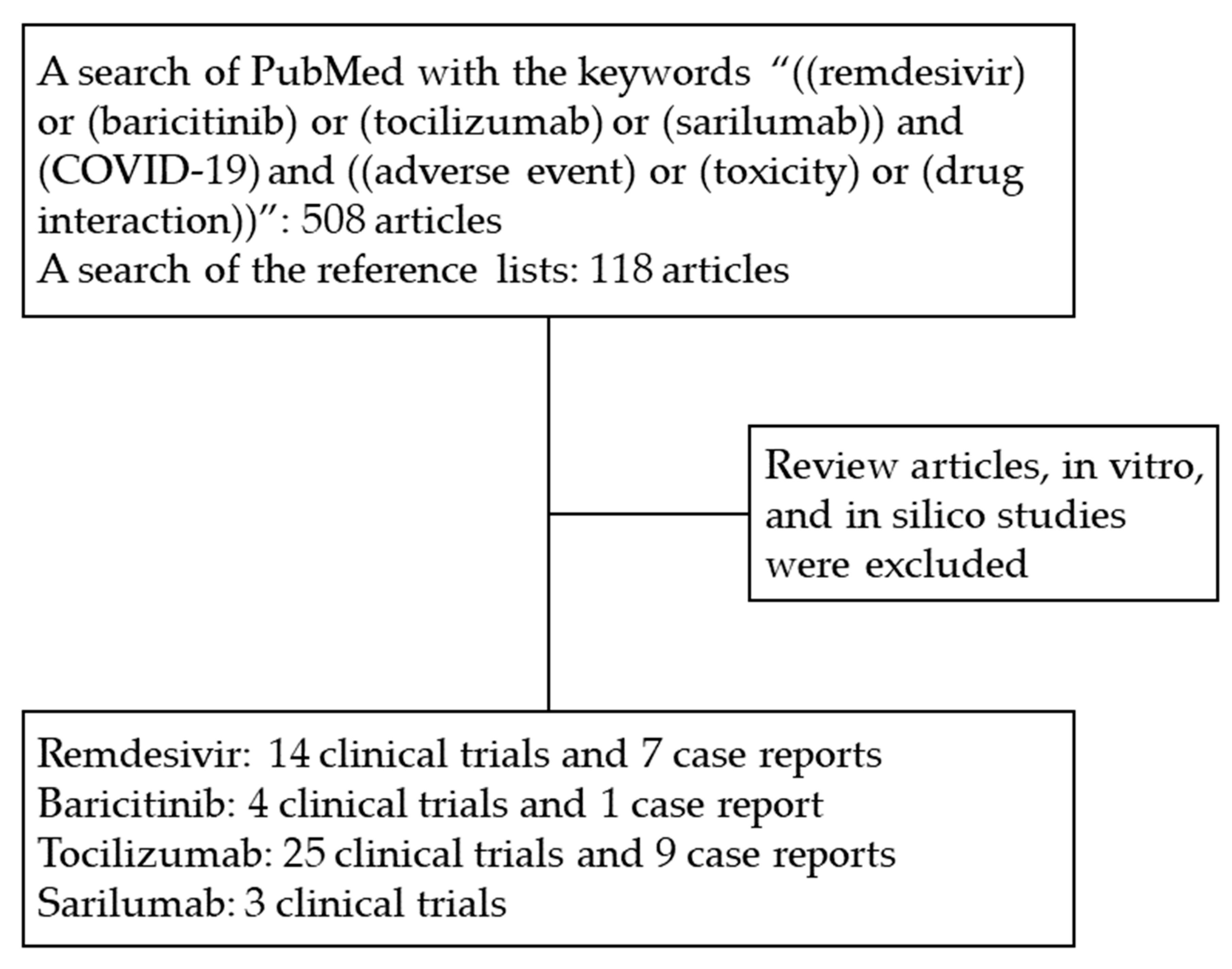
2. Literature Search Strategy
3. Remdesivir
3.1. Indication
3.2. Pharmacokinetics and Mechanism of Action
3.3. Recommended Dosage
3.4. Adverse Events
4. Baricitinib
4.1. Indication
4.2. Pharmacokinetics and Mechanism of Action
4.3. Recommended Dosage
4.4. Adverse Events
5. Tocilizumab
5.1. Indication
5.2. Pharmacokinetics and Mechanism of Action
5.3. Recommended Dosage
5.4. Adverse Events
6. Sarilumab
6.1. Indication
6.2. Pharmacokinetics and Mechanism of Action
6.3. Recommended Dosage
6.4. Adverse Events
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 21 September 2021).
- Roviello, V.; Roviello, G.N. Less COVID-19 deaths in southern and insular Italy explained by forest bathing, Mediterranean environment, and antiviral plant volatile organic compounds. Environ. Chem. Lett. 2021, 1–11. [Google Scholar] [CrossRef]
- Costanzo, M.; De Giglio, M.A.R.; Roviello, G.N. Anti-Coronavirus Vaccines: Past Investigations on SARS-CoV-1 and MERS-CoV, the Approved Vaccines from BioNTech/Pfizer, Moderna, Oxford/AstraZeneca and others under Development Against SARS-CoV-2 Infection. Curr. Med. Chem. 2021. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health (NIH) COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://files.covid19treatmentguidelines.nih.gov/guidelines/covid19treatmentguidelines.pdf (accessed on 17 September 2021).
- Regeneron Pharmaceuticals Inc. Fact Sheet for Healthcare Providers: Emergency Use Authorization (EUA) of Casirivimab and Imdevimab. Available online: https://www.fda.gov/media/145611/download (accessed on 17 September 2021).
- Eli Lilly and Company. Fact Sheet for Healthcare Providers: Emergency Use Authorization (EUA) of Bamlanivimab and Etesevimab. Available online: https://www.fda.gov/media/145802/download (accessed on 17 September 2021).
- GlaxoSmithKline LLC. Fact Sheet for Healthcare Providers: Emergency Use Authorization (EUA) of Sotrovimab. Available online: https://www.fda.gov/media/149534/download (accessed on 17 September 2021).
- The RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- US Food & Drug Administration (FDA). Clinical Memorandum: COVID-19 Convalescent Plasma. Available online: https://www.fda.gov/media/141480/download (accessed on 1 August 2021).
- Gilead Sciences Inc. Full Prescribing Information: Remdesivir, for Intravenous Use. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/214787Orig1s000lbl.pdf (accessed on 1 August 2021).
- Eli Lilly and Company. Fact Sheet for Healthcare Providers: Emergency Use Authorization (EUA) of Baricitinib. Available online: https://www.fda.gov/media/143823/download (accessed on 1 August 2021).
- Genentech Inc. Fact Sheet for Healthcare Providers: Emergency Use Authorization (EUA) of Tocilizumab. Available online: https://www.fda.gov/media/150321/download (accessed on 1 August 2021).
- US Food & Drug Administration (FDA). Memorandum Explaining Basis for Revocation of Emergency Use Authorization for Emergency Use of Chloroquine Phosphate and Hydroxychloroquine Sulfate. Available online: https://www.fda.gov/media/138945/download (accessed on 1 August 2021).
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe COVID-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.W.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Emberson, J.; Palfreeman, A.; Raw, J.; Elmahi, E.; Prudon, B.; et al. Lopinavir–ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef]
- Cattaneo, D.; Pasina, L.; Maggioni, A.P.; Giacomelli, A.; Oreni, L.; Covizzi, A.; Bradanini, L.; Schiuma, M.; Antinori, S.; Ridolfo, A.; et al. Drug–Drug Interactions and Prescription Appropriateness in Patients with COVID-19: A Retrospective Analysis from a Reference Hospital in Northern Italy. Drugs Aging 2020, 37, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef]
- The REMAP-CAP Investigators. Interleukin-6 Receptor Antagonists in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar] [CrossRef] [PubMed]
- Wishart, D.S.; Feunang, Y.D.; Guo, A.C.; Lo, E.J.; Marcu, A.; Grant, J.R.; Sajed, T.; Johnson, D.; Li, C.; Sayeeda, Z.; et al. DrugBank 5.0: A major update to the DrugBank database for 2018. Nucleic Acids Res. 2017, 46, D1074–D1082. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383. [Google Scholar] [CrossRef]
- Abani, O.; Abbas, A.; Abbas, F.; Abbas, M.; Abbasi, S.; Abbass, H.; Abbott, A.; Abdallah, N.; Abdelaziz, A.; Abdelfattah, M.; et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Salama, C.; Han, J.; Yau, L.; Reiss, W.G.; Kramer, B.; Neidhart, J.D.; Criner, G.J.; Kaplan-Lewis, E.; Baden, R.; Pandit, L.; et al. Tocilizumab in Patients Hospitalized with COVID-19 Pneumonia. N. Engl. J. Med. 2021, 384, 20–30. [Google Scholar] [CrossRef]
- Rosas, I.O.; Bräu, N.; Waters, M.; Go, R.C.; Hunter, B.D.; Bhagani, S.; Skiest, D.; Aziz, M.S.; Cooper, N.; Douglas, I.S.; et al. Tocilizumab in Hospitalized Patients with Severe COVID-19 Pneumonia. N. Engl. J. Med. 2021, 384, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- Roche, H.-L.; Sciences, G. A Study to Evaluate the Efficacy and Safety of Remdesivir Plus Tocilizumab Compared With Remdesivir Plus Placebo in Hospitalized Participants With Severe COVID-19 Pneumonia. Available online: https://ClinicalTrials.gov/show/NCT04409262 (accessed on 1 August 2021).
- Della-Torre, E.; Lanzillotta, M.; Campochiaro, C.; Cavalli, G.; De Luca, G.; Tomelleri, A.; Boffini, N.; De Lorenzo, R.; Ruggeri, A.; Rovere-Querini, P.; et al. Respiratory Impairment Predicts Response to IL-1 and IL-6 Blockade in COVID-19 Patients With Severe Pneumonia and Hyper-Inflammation. Front. Immunol. 2021, 12, 675678. [Google Scholar] [CrossRef] [PubMed]
- Lescure, F.-X.; Honda, H.; Fowler, R.A.; Lazar, J.S.; Shi, G.; Wung, P.; Patel, N.; Hagino, O.; Bazzalo, I.J.; Casas, M.M.; et al. Sarilumab in patients admitted to hospital with severe or critical COVID-19: A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir. Med. 2021, 9, 522–532. [Google Scholar] [CrossRef]
- Garcia-Vicuña, R.; Abad-Santos, F.; González-Alvaro, I.; Ramos-Lima, F.; Sanz, J.S. Subcutaneous Sarilumab in hospitalised patients with moderate-severe COVID-19 infection compared to the standard of care (SARCOVID): A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 772. [Google Scholar] [CrossRef] [PubMed]
- Boyapati, A.; Wipperman, M.F.; Ehmann, P.J.; Hamon, S.; Lederer, D.J.; Waldron, A.; Flanagan, J.J.; Karayusuf, E.; Bhore, R.; Nivens, M.C.; et al. Baseline SARS-CoV-2 Viral Load is Associated With COVID-19 Disease Severity and Clinical Outcomes: Post-Hoc Analyses of a Phase 2/3 Trial. J. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- López, R.L.; Fernández, S.C.; Pérez, L.L.; Palacios, A.R.; Fernández-Roldán, M.C.; Alonso, E.A.; Camacho, I.P.; Rodriguez-Baño, J.; Merchante, N.; Olalla, J.; et al. Efficacy and safety of early treatment with sarilumab in hospitalised adults with COVID-19 presenting cytokine release syndrome (SARICOR STUDY): Protocol of a phase II, open-label, randomised, multicentre, controlled clinical trial. BMJ Open 2020, 10, e039951. [Google Scholar] [CrossRef]
- Gilead Sciences Inc. Fact Sheet for Healthcare Providers: Emergency Use Authorization (EUA) of Remdesivir for Hospitalized Pediatric Patients Weighing 3.5 kg to Less than 40 kg or Hospitalized Pediatric Patients Less than 12 Years of Age Weighing at least 3.5 kg. Available online: https://www.fda.gov/media/137566/download (accessed on 1 August 2021).
- Spinner, C.D.; Gottlieb, R.L.; Criner, G.J.; López, J.R.A.; Cattelan, A.M.; Viladomiu, A.S.; Ogbuagu, O.; Malhotra, P.; Mullane, K.M.; Castagna, A.; et al. Effect of Remdesivir vs. Standard Care on Clinical Status at 11 Days in Patients with Moderate COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 1048–1057. [Google Scholar] [CrossRef]
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.; Edwards, K.M.; Gandhi, R.; Gallagher, J.; Muller, W.J.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Infectious Diseases Society of America 2021; Version 5.1.2. Available online: https://www.idsociety.org/practice-guideline/covid-19-Guideline-Treatment-and-Management/ (accessed on 17 September 2021).
- World Health Organization. Therapeutics and COVID-19: Living Guideline. Available online: https://apps.who.int/iris/rest/bitstreams/1354702/retrieve (accessed on 17 September 2021).
- Humeniuk, R.; Mathias, A.; Cao, H.; Osinusi, A.; Shen, G.; Chng, E.; Ling, J.; Vu, A.; German, P. Safety, Tolerability, and Pharmacokinetics of Remdesivir, An Antiviral for Treatment of COVID-19, in Healthy Subjects. Clin. Transl. Sci. 2020, 13, 896–906. [Google Scholar] [CrossRef]
- Borbone, N.; Piccialli, G.; Roviello, G.N.; Oliviero, G. Nucleoside Analogs and Nucleoside Precursors as Drugs in the Fight against SARS-CoV-2 and Other Coronaviruses. Molecules 2021, 26, 986. [Google Scholar] [CrossRef] [PubMed]
- Pettit, N.N.; Pisano, J.; Nguyen, C.T.; Lew, A.K.; Hazra, A.; Sherer, R.; Mullane, K.M. Remdesivir Use in the Setting of Severe Renal Impairment: A Theoretical Concern or Real Risk? Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sörgel, F.; Malin, J.J.; Hagmann, H.; Kinzig, M.; Bilal, M.; Eichenauer, D.A.; Scherf-Clavel, O.; Simonis, A.; El Tabei, L.; Fuhr, U.; et al. Pharmacokinetics of remdesivir in a COVID-19 patient with end-stage renal disease on intermittent haemodialysis. J. Antimicrob. Chemother. 2020, 76, 825–827. [Google Scholar] [CrossRef]
- Buxeda, A.; Arias-Cabrales, C.; Pérez-Sáez, M.J.; Cacho, J.; Pelegrin, S.C.; Melilli, E.; Aladrén, M.J.; Galeano, C.; Lorenzo, I.; Mazuecos, A.; et al. Use and Safety of Remdesivir in Kidney Transplant Recipients With COVID-19. Kidney Int. Rep. 2021, 6, 2305–2315. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Goldman, J.D.; Lye, D.C.B.; Hui, D.S.; Marks, K.M.; Bruno, R.; Montejano, R.; Spinner, C.D.; Galli, M.; Ahn, M.-Y.; Nahass, R.G.; et al. Remdesivir for 5 or 10 Days in Patients with Severe COVID-19. N. Engl. J. Med. 2020, 383. [Google Scholar] [CrossRef] [PubMed]
- ACTIV-3/TICO LY-CoV555 Study Group. A Neutralizing Monoclonal Antibody for Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 905–914. [Google Scholar] [CrossRef]
- Antinori, S.; Cossu, M.V.; Ridolfo, A.L.; Rech, R.; Bonazzetti, C.; Pagani, G.; Gubertini, G.; Coen, M.; Magni, C.; Castelli, A.; et al. Compassionate remdesivir treatment of severe COVID-19 pneumonia in intensive care unit (ICU) and Non-ICU patients: Clinical outcome and differences in post-treatment hospitalisation status. Pharmacol. Res. 2020, 158, 104899. [Google Scholar] [CrossRef] [PubMed]
- WHO Solidarity Trial Consortium. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef]
- Bertolini, A.; Van De Peppel, I.P.; Bodewes, F.A.; Moshage, H.; Fantin, A.; Farinati, F.; Fiorotto, R.; Jonker, J.W.; Strazzabosco, M.; Verkade, H.J.; et al. Abnormal Liver Function Tests in Patients With COVID-19: Relevance and Potential Pathogenesis. Hepatology 2020, 72, 1864–1872. [Google Scholar] [CrossRef]
- Benedetti, C.; Waldman, M.; Zaza, G.; Riella, L.V.; Cravedi, P. COVID-19 and the Kidneys: An Update. Front. Med. 2020, 7, 423. [Google Scholar] [CrossRef]
- Mulangu, S.; Dodd, L.E.; Davey, R.T.; Mbaya, O.T.; Proschan, M.; Mukadi, D.; Manzo, M.L.; Nzolo, D.; Oloma, A.T.; Ibanda, A.; et al. A Randomized, Controlled Trial of Ebola Virus Disease Therapeutics. N. Engl. J. Med. 2019, 381, 2293–2303. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Parker, B.M.; Priyadarshi, V.; Parker, J. Cardiac Adverse Events with Remdesivir in COVID-19 Infection. Cureus 2020, 12, e11132. [Google Scholar] [CrossRef] [PubMed]
- Gubitosa, J.C.; Kakar, P.; Gerula, C.; Nossa, H.; Finkel, D.; Wong, K.; Khatri, M.; Ali, H. Marked Sinus Bradycardia Associated With Remdesivir in COVID-19. JACC Case Rep. 2020, 2, 2260–2264. [Google Scholar] [CrossRef]
- Selvaraj, V.; Bavishi, C.; Patel, S.; Dapaah-Afriyie, K. Complete heart block associated with Remdesivir in COVID-19: A case report. Eur. Hear. J. Case Rep. 2021, 5, ytab200. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.V.; Ferdinandy, P.; Liaudet, L.; Pacher, P. Drug-induced mitochondrial dysfunction and cardiotoxicity. Am. J. Physiol. Circ. Physiol. 2015, 309, H1453–H1467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zipes, D.P.; Libby, P.; Bonow, R.O.; Mann, D.L.; Tomaselli, G.F.; Braunwald, E. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine; Elsevier/Saunders: Philadelphia, PA, USA, 2019. [Google Scholar]
- Hopkins, B.J.; Prokesch, B.C. Anaphylaxis Due to Remdesivir. Antimicrob. Agents Chemother. 2021, 65, e00233-21. [Google Scholar] [CrossRef]
- Van Merendonk, L.N.; Leeuwerik, A.F.; Brok, M.W.J.D.; Hekking, P.-P.W.; Korevaar, D.A.; Jacobs, C.J.; Bet, P.M. Peripheral infiltration of remdesivir in 3 patients with COVID-19: Case series and discussion. Am. J. Health Pharm. 2021. [Google Scholar] [CrossRef] [PubMed]
- Leegwater, E.; Strik, A.; Wilms, E.B.; Bosma, L.B.E.; Burger, D.M.; Ottens, T.H.; van Nieuwkoop, C. Drug-induced Liver Injury in a Patient With Coronavirus Disease 2019: Potential Interaction of Remdesivir With P-Glycoprotein Inhibitors. Clin. Infect. Dis. 2020, 72, 1256–1258. [Google Scholar] [CrossRef]
- Landayan, R.P.; Saint-Felix, S.; Williams, A. Probable Interaction Between Warfarin and the Combination of Remdesivir With Dexamethasone for Coronavirus Disease 2019 (COVID-19) Treatment: A 2 Case Report. J. Pharm. Pract. 2021. [Google Scholar] [CrossRef] [PubMed]
- Teoli, D.; Thompson, V.; Wright, J.; Ho, I.; Vlaminck, B.; Miller, G.; Feely, M. Acute Pain Crisis Caused by Tramadol Remdesivir Drug–Drug Interaction. J. Palliat. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Eli Lilly Canada Inc. Product Monograph Including Patient Medication Information: OLUMIANT®, Baricitinib, Oral Tablets. Available online: http://pi.lilly.com/ca/olumiant-ca-pm.pdf (accessed on 1 August 2021).
- Richardson, P.; Griffin, I.; Tucker, C.; Smith, D.; Oechsle, O.; Phelan, A.; Rawling, M.; Savory, E.; Stebbing, J. Baricitinib as potential treatment for 2019-nCoV acute respiratory disease. Lancet 2020, 395, e30–e31. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.G.; Chen, X.; Lee, F.; Emm, T.; Scherle, P.A.; Lo, Y.; Punwani, N.; Williams, W.V.; Yeleswaram, S. The pharmacokinetics, pharmacodynamics, and safety of baricitinib, an oral JAK 1/2 inhibitor, in healthy volunteers. J. Clin. Pharmacol. 2014, 54, 1354–1361. [Google Scholar] [CrossRef]
- Peng, L.; Xiao, K.; Ottaviani, S.; Stebbing, J.; Wang, Y.-J. A real-world disproportionality analysis of FDA Adverse Event Reporting System (FAERS) events for baricitinib. Expert Opin. Drug Saf. 2020, 19, 1505–1511. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Liang, W.-H.; Zhao, Y.; Liang, H.-R.; Chen, Z.-S.; Li, Y.-M.; Liu, X.-Q.; Chen, R.-C.; Tang, C.-L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [Green Version]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Hasan, J.; Rabbani, R.; Anam, A.M.; Huq, S.M.R.; Polash, M.M.I.; Nessa, S.S.T.; Bachar, S.C. Impact of high dose of baricitinib in severe COVID-19 pneumonia: A prospective cohort study in Bangladesh. BMC Infect. Dis. 2021, 21, 427. [Google Scholar] [CrossRef] [PubMed]
- Markham, A. Baricitinib: First Global Approval. Drugs 2017, 77, 697–704. [Google Scholar] [CrossRef]
- Posada, M.M.; Cannady, E.A.; Payne, C.D.; Zhang, X.; Bacon, J.A.; Pak, Y.A.; Higgins, J.W.; Shahri, N.; Hall, S.D.; Hillgren, K.M. Prediction of Transporter-Mediated Drug-Drug Interactions for Baricitinib. Clin. Transl. Sci. 2017, 10, 509–519. [Google Scholar] [CrossRef]
- Genentech, I. Full Prescribing Information: ACTEMRA®, Tocilizumab, Injection, for Intravenous or Subcutaneous Use. Available online: https://www.gene.com/download/pdf/actemra_prescribing.pdf (accessed on 15 September 2021).
- Abou-Auda, H.S.; Sakr, W. Tocilizumab: A new anti-rheumatic drug. Saudi Pharm. J. 2010, 18, 257–259. [Google Scholar] [CrossRef] [Green Version]
- Veiga, V.C.; Prats, J.A.G.G.; Farias, D.L.C.; Rosa, R.G.; Dourado, L.K.; Zampieri, F.G.; Machado, F.R.; Lopes, R.D.; Berwanger, O.; Azevedo, L.C.P.; et al. Effect of tocilizumab on clinical outcomes at 15 days in patients with severe or critical coronavirus disease 2019: Randomised controlled trial. BMJ 2021, 372, n84. [Google Scholar] [CrossRef] [PubMed]
- Soin, A.S.; Kumar, K.; Choudhary, N.S.; Sharma, P.; Mehta, Y.; Kataria, S.; Govil, D.; Deswal, V.; Chaudhry, D.; Singh, P.K.; et al. Tocilizumab plus standard care versus standard care in patients in India with moderate to severe COVID-19-associated cytokine release syndrome (COVINTOC): An open-label, multicentre, randomised, controlled, phase 3 trial. Lancet Respir. Med. 2021, 9, 511–521. [Google Scholar] [CrossRef]
- Hermine, O.; Mariette, X.; Tharaux, P.-L.; Resche-Rigon, M.; Porcher, R.; Ravaud, P.; Bureau, S.; Dougados, M.; Tibi, A.; CORIMUNO-19 Collaborative Group; et al. Effect of Tocilizumab vs. Usual Care in Adults Hospitalized With COVID-19 and Moderate or Severe Pneumonia. JAMA Intern. Med. 2021, 181, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Salvarani, C.; Dolci, G.; Massari, M.; Merlo, D.F.; Cavuto, S.; Savoldi, L.; Bruzzi, P.; Boni, F.; Braglia, L.; Turrà, C.; et al. Effect of Tocilizumab vs. Standard Care on Clinical Worsening in Patients Hospitalized With COVID-19 Pneumonia: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 24–31. [Google Scholar] [CrossRef]
- Perrone, F.; Piccirillo, M.C.; Ascierto, P.A.; Salvarani, C.; Parrella, R.; Marata, A.M.; Popoli, P.; Ferraris, L.; Marrocco-Trischitta, M.M.; Ripamonti, D.; et al. Tocilizumab for patients with COVID-19 pneumonia. The single-arm TOCIVID-19 prospective trial. J. Transl. Med. 2020, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Fu, B.; Peng, Z.; Yang, D.; Han, M.; Li, M.; Yang, Y.; Yang, T.; Sun, L.; Li, W.; et al. Tocilizumab in patients with moderate or severe COVID-19: A randomized, controlled, open-label, multicenter trial. Front. Med. 2021, 15, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.H.; Frigault, M.J.; Serling-Boyd, N.J.; Fernandes, A.D.; Harvey, L.; Foulkes, A.S.; Horick, N.K.; Healy, B.C.; Shah, R.; Bensaci, A.M.; et al. Efficacy of Tocilizumab in Patients Hospitalized with COVID-19. N. Engl. J. Med. 2020, 383, 2333–2344. [Google Scholar] [CrossRef]
- Malekzadeh, R.; Abedini, A.; Mohsenpour, B.; Sharifipour, E.; Ghasemian, R.; Javad-Mousavi, S.A.; Khodashahi, R.; Darban, M.; Kalantari, S.; Abdollahi, N.; et al. Subcutaneous tocilizumab in adults with severe and critical COVID-19: A prospective open-label uncontrolled multicenter trial. Int. Immunopharmacol. 2020, 89, 107102. [Google Scholar] [CrossRef]
- Zhao, H.; Zhu, Q.; Zhang, C.; Li, J.; Wei, M.; Qin, Y.; Chen, G.; Wang, K.; Yu, J.; Wu, Z.; et al. Tocilizumab combined with favipiravir in the treatment of COVID-19: A multicenter trial in a small sample size. Biomed. Pharmacother. 2020, 133. [Google Scholar] [CrossRef]
- Roumier, M.; Paule, R.; Vallée, A.; Rohmer, J.; Ballester, M.; Brun, A.-L.; Cerf, C.; Chabi, M.-L.; Chinet, T.; Colombier, M.-A.; et al. Tocilizumab for Severe Worsening COVID-19 Pneumonia: A Propensity Score Analysis. J. Clin. Immunol. 2020, 41, 303–314. [Google Scholar] [CrossRef] [PubMed]
- West, T.A.; Malik, S.; Nalpantidis, A.; Tran, T.; Cannon, C.; Bhonagiri, D.; Chan, K.; Cheong, E.; Cheong, J.W.S.; Cheung, W.; et al. Tocilizumab for severe COVID-19 pneumonia: Case series of 5 Australian patients. Int. J. Rheum. Dis. 2020, 23, 1030–1039. [Google Scholar] [CrossRef]
- Taramasso, L.; Vena, A.; Bovis, F.; Portunato, F.; Mora, S.; Dentone, C.; Delfino, E.; Mikulska, M.; Giacobbe, D.R.; De Maria, A.; et al. Higher Mortality and Intensive Care Unit Admissions in COVID-19 Patients with Liver Enzyme Elevations. Microorganisms 2020, 8, 2010. [Google Scholar] [CrossRef] [PubMed]
- Mehta, M.; Purpura, L.J.; McConville, T.H.; Neidell, M.J.; Anderson, M.R.; Bernstein, E.J.; Dietz, D.E.; Laracy, J.; Gunaratne, S.H.; Miller, E.H.; et al. What about tocilizumab? A retrospective study from a NYC Hospital during the COVID-19 outbreak. PLoS ONE 2021, 16, e0249349. [Google Scholar] [CrossRef] [PubMed]
- Sernicola, A.; Carnicelli, G.; Di Fraia, M.; Chello, C.; Furlan, C.; Muharremi, R.; Paolino, G.; Grieco, T. ‘Toxic erythema’ and eosinophilia associated with tocilizumab therapy in a COVID-19 patient. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e368–e370. [Google Scholar] [CrossRef] [PubMed]
- Dastan, F.; Saffaei, A.; Haseli, S.; Marjani, M.; Moniri, A.; Abtahian, Z.; Abedini, A.; Kiani, A.; Seifi, S.; Jammati, H.; et al. Promising effects of tocilizumab in COVID-19: A non-controlled, prospective clinical trial. Int. Immunopharmacol. 2020, 88, 106869. [Google Scholar] [CrossRef] [PubMed]
- Bruzzese, V.; Lazzarino, A.I. The paradoxical effect of IL-6 and implications for the use of Tocilizumab in COVID-19 patients. Med. Hypotheses 2020, 144, 110284. [Google Scholar] [CrossRef] [PubMed]
- Galván-Román, J.M.; Rodríguez-García, S.C.; Roy-Vallejo, E.; Marcos-Jiménez, A.; Sánchez-Alonso, S.; Fernández-Díaz, C.; Alcaraz-Serna, A.; Mateu-Albero, T.; Rodríguez-Cortes, P.; Sánchez-Cerrillo, I.; et al. IL-6 serum levels predict severity and response to tocilizumab in COVID-19: An observational study. J. Allergy Clin. Immunol. 2020, 147, 72–80.e8. [Google Scholar] [CrossRef] [PubMed]
- Pettit, N.N.; Nguyen, C.T.; Mutlu, G.M.; Wu, D.; Kimmig, L.; Pitrak, D.; Pursell, K. Late onset infectious complications and safety of tocilizumab in the management of COVID-19. J. Med. Virol. 2020, 93, 1459–1464. [Google Scholar] [CrossRef]
- Podlasin, R.B.; Kowalska, J.D.; Pihowicz, A.; Wojtycha-Kwaśnica, B.; Thompson, M.; Dyda, T.; Czeszko-Paprocka, H.; Horban, A. How to follow-up a patient who received tocilizumab in severe COVID-19: A case report. Eur. J. Med. Res. 2020, 25, 1–6. [Google Scholar] [CrossRef]
- Bruce-Hickman, D.; Sajeed, S.M.; Pang, Y.H.; Seow, C.S.; Chen, W.; Kansal, M.G. Bowel ulceration following tocilizumab administration in a COVID-19 patient. BMJ Open Gastroenterol. 2020, 7, e000484. [Google Scholar] [CrossRef]
- Martínez-López-De-Castro, N.; Samartín-Ucha, M.; Paradela-Carreiro, A.; Pérez-Landeiro, A.; Inaraja-Bobo, M.T.; Álvarez-Payero, M.; Castro-Núñez, I.; García-Beloso, N.; Robles-Torres, D.; López-López, A.; et al. Real-world prevalence and consequences of potential drug-drug interactions in the first-wave COVID-19 treatments. J. Clin. Pharm. Ther. 2020, 46, 724–730. [Google Scholar] [CrossRef]
- Oguz, E.G.; Atilgan, K.G.; Cimen, S.G.; Sahin, H.; Selen, T.; Ebinc, F.A.; Cimen, S.; Ayli, M.D. COVID-19 infection in a kidney transplant recipient—special emphasis on pharmacokinetic interactions: A case report. World J. Transplant. 2020, 10, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Bishara, D.; Kalafatis, C.; Taylor, D. Emerging and experimental treatments for COVID-19 and drug interactions with psychotropic agents. Ther. Adv. Psychopharmacol. 2020, 10, 2045125320935306. [Google Scholar] [CrossRef] [PubMed]
- Sanofi-Aventis Canada Inc. Product Monograph Including Patient Medication Information: KEVZARA®, Sarilumab, Solution for subcutaneous Injection. Available online: https://products.sanofi.ca/en/Kevzara-en.pdf (accessed on 1 August 2021).
- Benfield, T.; Hospital, H.U. Efficacy and Safety of Novel Treatment Options for Adults with COVID-19 Pneumonia. Available online: https://ClinicalTrials.gov/show/NCT04345289 (accessed on 1 August 2021).
- Barrett, L.; Nova Scotia Health Authority; Dalhousie University. Treatment of Moderate to Severe Coronavirus Disease (COVID-19) in Hospitalized Patients; Canada, 2020. Available online: https://clinicaltrials.gov/ct2/show/NCT04321993 (accessed on 1 August 2021).
- Sivapalasingam, S.; Lederer, D.J.; Bhore, R.; Hajizadeh, N.; Criner, G.; Hossain, R.; Mahmood, A.; Giannelou, A.; Somersan-Karakaya, S.; O’Brien, M.; et al. A Randomized Placebo-Controlled Trial of Sarilumab in Hospitalized Patients with COVID-19. medRxiv 2021. [Google Scholar] [CrossRef]

{kind=link}
| Drugs | Type | Chemical Formula | Average Weight | US FDA Labeled Indication Other Than COVID-19 | Possible Mechanisms in Treatment of COVID-19 |
|---|---|---|---|---|---|
| Remdesivir | Small Molecule | C27H35N6O8P | 602.6 Da | None | The nucleotide analogue inhibit viral nucleotide synthesis to stop viral replication. |
| Baricitinib | Small Molecule | C16H17N7O2S | 371.4 Da | 1. Rheumatoid arthritis (moderate to severe) | The JAK inhibitor blocks JAK-STAT signaling pathway and inflammatory response. |
| Tocilizumab | Monoclonal antibody | C6428H9976N1720O2018S42 | 148,000.0 Da | 1. Cytokine release syndrome 2. Juvenile rheumatoid arthritis 3. Lung disease with systemic sclerosis 4. Rheumatoid arthritis (moderate to severe) 5. Systemic onset juvenile chronic arthritis 6. Temporal arteritis | The IL-6 receptor antagonist inhibit IL-6 signaling pathway and inflammatory response. |
| Sarilumab | Monoclonal antibody | C6388H9918N1718O1998S44 | 150,000.0 Da | 1. Rheumatoid arthritis (moderate to severe) | The IL-6 receptor antagonist inhibit IL-6 signaling pathway and inflammatory response. |
| Drugs | Trial Names | Trial Sites | Inclusion Criteria | Patient Numbers | Dosage | Efficacy | Safety |
|---|---|---|---|---|---|---|---|
| Remdesivir | ACTT-1 [20] | The United States (45 sites), Denmark (8), the United Kingdom (5), Greece (4), Germany (3), Korea (2), Mexico (2), Spain (2), Japan (1), and Singapore (1) | Adults who were hospitalized with COVID-19 and had evidence of lower respiratory tract infection | 541 assigned to the remdesivir group and 521 to the placebo group | Remdesivir was administered intravenously as a 200-mg loading dose on day 1, followed by a 100-mg maintenance dose administered daily on days 2 through 10 or until hospital discharge or death | Remdesivir was superior to placebo in shortening the time to recovery; the mortality rates were 6.7% with remdesivir and 11.9% with placebo by day 15 (HR, 0.55; 95% CI, 0.36 to 0.83) and 11.4% with remdesivir and 15.2% with placebo by day 29 (HR, 0.73; 95% CI, 0.52 to 1.03) | Serious adverse events were reported in 131 of the 532 patients who received remdesivir (24.6%) and in 163 of the 516 patients who received placebo (31.6%) |
| Baricitinib | ACTT-2 [17] | The United States (55 sites), Singapore (4), South Korea (2), Mexico (2), Japan (1), Spain (1), the United Kingdom (1), and Denmark (1) | Adults with COVID-19 who received remdesivir (≤10 days) and either baricitinib (≤14 days) or placebo (control) | 515 assigned to combination treatment and 518 to control | Baricitinib was administered as a 4-mg daily dose for 14 days or until hospital discharge. | Baricitinib plus remdesivir was superior to remdesivir alone in reducing recovery time; the 28-day mortality was 5.1% in the combination group and 7.8% in the control group (HR, 0.65; 95% CI, 0.39 to 1.09) | Serious adverse events were less frequent in the combination group than in the control group (16.0% vs. 21.0%), as were new infections (5.9% vs. 11.2%), under the recommendation of venous thromboembolism prophylaxis |
| Tocilizumab | RECOVERY [21] | The United Kingdom | Adults with COVID-19 who had hypoxia (oxygen saturation <92% on air or requiring oxygen therapy) and evidence of systemic inflammation (C-reactive protein >=75 mg/L) | 2022 randomly allocated to tocilizumab and 2094 to usual care | Tocilizumab was given intravenously as a dose of 400–800 mg, followed by either a second dose 12–24 h later or not | Tocilizumab was superior to placebo in discharge from hospital within 28 days (57% vs. 50%); patients allocated tocilizumab were less likely to reach the composite endpoint of invasive mechanical ventilation or death (35% vs. 42%; RR 0.84; 95% CI 0.77–0.92) | There were three reports of serious adverse reactions believed to be related to tocilizumab: one each of otitis externa, Staphylococcus aureus bacteremia, and lung abscess, all of which resolved with standard treatment |
| Tocilizumab | EMPACTA [22] | The United States (45 sites), Brazil (6), Peru (5), South Africa (3), Kenya (2), Mexico (2) | Adults with COVID-19 who were confirmed by a positive polymerase-chain-reaction test and radiographic imaging | 249 randomly allocated to tocilizumab and 128 to placebo | Tocilizumab was given intravenously as one or two doses of 8 mg per kilogram of body weight (maximum of 800 mg) | Tocilizumab was superior to placebo in the cumulative percentage of receiving mechanical ventilation or death by day 28 (12.0% vs. 19.3%; HR, 0.56; 95% CI, 0.33 to 0.97); there was no significant difference in death from any cause by day 28 (10.4% vs. 8.6%) | Serious adverse events occurred in 38 of 250 patients (15.2%) in the tocilizumab group and 25 of 127 patients (19.7%) in the placebo group |
| Tocilizumab | COVACTA [23] | The United States (23 sites), France (7), Spain (7), the United Kingdom (7), Canada (4), Denmark (4), Germany (4), Netherlands (4), Italy (2) | Adults with COVID-19 who had blood oxygen saturation of 93% or less or a ratio of the arterial oxygen partial pressure to fractional inspired oxygen of less than 300 mmHg | 294 randomly allocated to tocilizumab and 144 to placebo | Tocilizumab was given intravenously as one a dose of 8 mg per kilogram of body weight, followed by either a second dose 8–24 h later or not | The use of tocilizumab did not result in significantly better clinical status at 28 days; mortality at day 28 was 19.7% in the tocilizumab group and 19.4% in the placebo group | Serious adverse events occurred in 103 of 295 patients (34.9%) in the tocilizumab group and in 55 of 143 patients (38.5%) in the placebo group |
| Tocilizumab | REMDACTA [24] | The United States (41 sites), Spain (9), Brazil (8), Russian Federation (5) | Patients with COVID-19 requiring more than 6 L/min supplemental oxygen to maintain oxygen saturation >93% who received remdesivir (10 days) and either tocilizumab (1 day) or placebo (control) | 649 enrolled | Tocilizumab was given intravenously as one dose | Ongoing | Ongoing |
| Drugs | Possible Mechanisms | Indications for the Treatment of COVID-19 | Routes of Administration | Recommended Dosage | Related Adverse Events |
|---|---|---|---|---|---|
| Remdesivir | Nucleotide analogue; inhibit viral nucleotide synthesis to stop viral replication. | Approved by the US FDA in hospitalized patients aged ≥12 years and weighing ≥40 kg; granted an EUA by the US FDA in hospitalized patients aged <12 years and weighing ≥3.5 kg. | Intravenous. | A single loading dose of 200 mg followed by once-daily maintenance doses of 100 mg for 5 to 10 days or until hospital discharge. | Alterations in liver function studies, increased serum levels of creatinine, atrioventricular block, and anaphylaxis. |
| Baricitinib | JAK inhibitor; blocks JAK-STAT signaling pathway and inflammatory response. | Granted an EUA by the US FDA in combination with remdesivir in hospitalized patients aged ≥2 years requiring supplemental oxygen, invasive mechanical ventilation, or extracorporeal membrane oxygenation. | Oral. | 4 mg in patients aged over 9 years and 2 mg aged under 9 years once daily for 14 days or until hospital discharge. | Thromboembolism, secondary infections, and hypersensitivity reaction. |
| Tocilizumab | IL-6 receptor antagonist; inhibit IL-6 signaling pathway. | Granted an EUA by the US FDA in hospitalized patients aged ≥2 years receiving systemic corticosteroids and requiring supplemental oxygen, non-invasive or invasive mechanical ventilation, or extracorporeal membrane oxygenation. | Intravenous. | First dose: a single loading dose of 8 mg/kg in patients over 30 kg, and 12 mg/kg in patients under 30 kg (max. 800 mg). Second dose: another single loading dose at least 8 h later if not improved. | Alteration in liver function studies, neutropenia, secondary infections, and allergic reactions. |
| Sarilumab | IL-6 receptor antagonist; inhibit IL-6 signaling pathway. | Under investigational use. | Subcutaneous or intravenous. | A single loading dose of 200 mg subcutaneously or 200 to 800 mg intravenously. | Alteration in liver function studies, neutropenia, secondary infection, and allergic reaction. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, J.-Y.; Mao, Y.-C.; Liu, P.-Y.; Lai, K.-L. Pharmacology and Adverse Events of Emergency-Use Authorized Medication in Moderate to Severe COVID-19. Pharmaceuticals 2021, 14, 955. https://doi.org/10.3390/ph14100955
Hsu J-Y, Mao Y-C, Liu P-Y, Lai K-L. Pharmacology and Adverse Events of Emergency-Use Authorized Medication in Moderate to Severe COVID-19. Pharmaceuticals. 2021; 14(10):955. https://doi.org/10.3390/ph14100955
Chicago/Turabian StyleHsu, Jen-Yu, Yan-Chiao Mao, Po-Yu Liu, and Kuo-Lung Lai. 2021. "Pharmacology and Adverse Events of Emergency-Use Authorized Medication in Moderate to Severe COVID-19" Pharmaceuticals 14, no. 10: 955. https://doi.org/10.3390/ph14100955
APA StyleHsu, J.-Y., Mao, Y.-C., Liu, P.-Y., & Lai, K.-L. (2021). Pharmacology and Adverse Events of Emergency-Use Authorized Medication in Moderate to Severe COVID-19. Pharmaceuticals, 14(10), 955. https://doi.org/10.3390/ph14100955