
Somatostatin Analogue Therapy in MEN1-Related Pancreatic Neuroendocrine Tumors from Evidence to Clinical Practice: A Systematic Review

 , ,
, , 
Abstract
1. Introduction
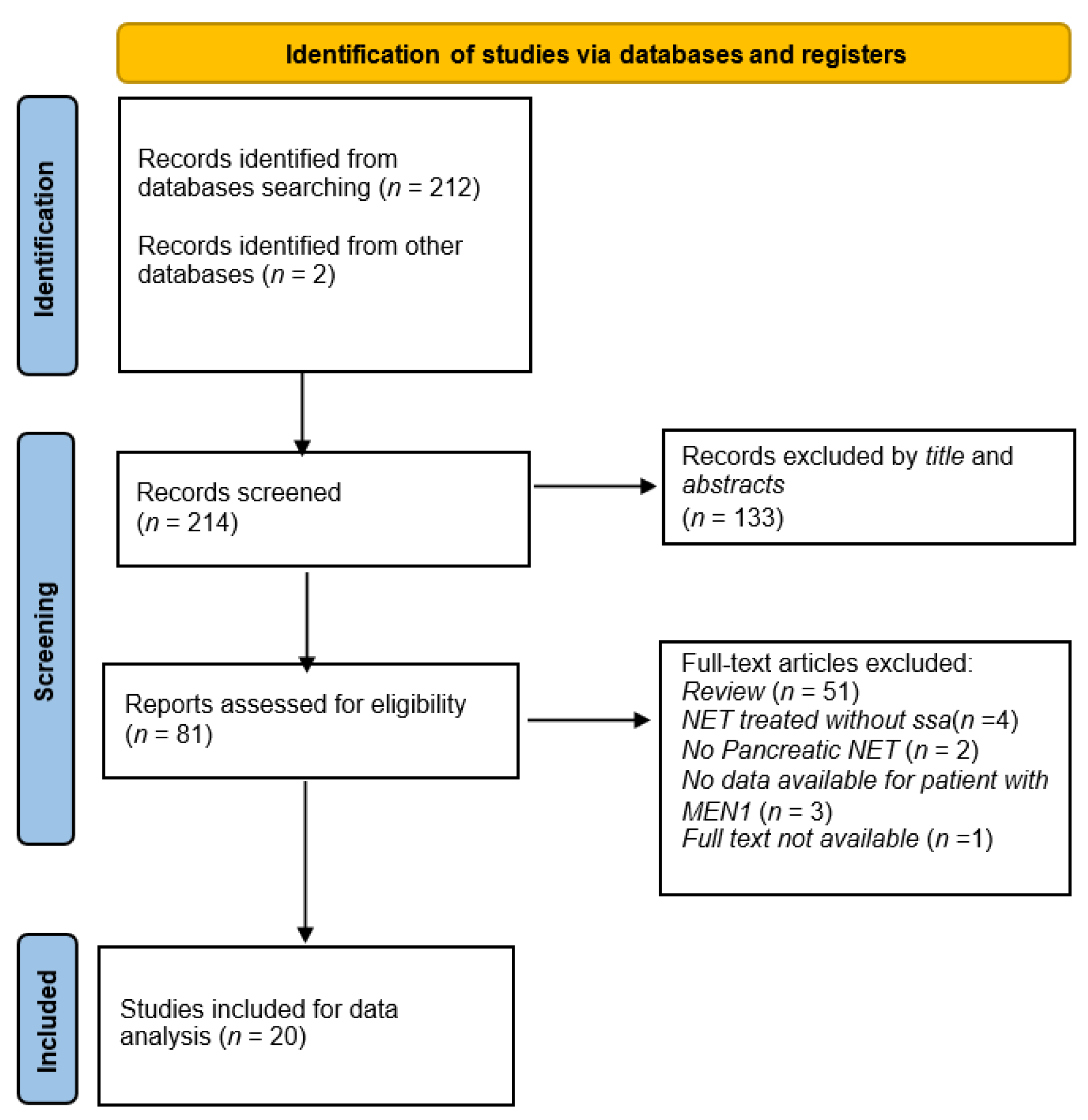
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
- Published papers including data regarding efficacy and safety of SSA in patients with pNENs in the context of MEN1syndrome;
- English language;
- Study design: prospective, retrospective, mixed prospective/retrospective trials, and case-report.
2.3. Study Selection and Data Extraction
3. Results
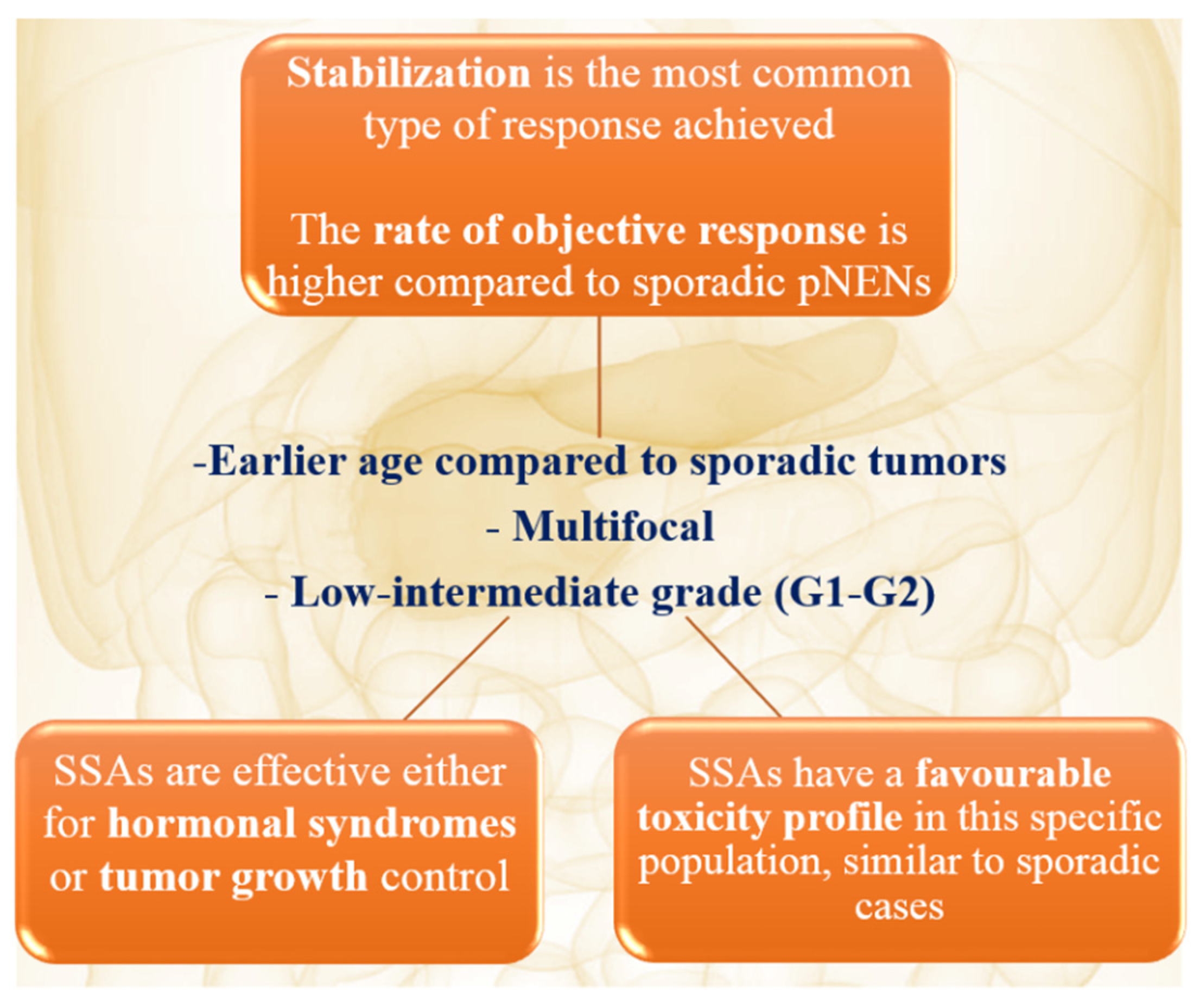
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lewis, M.A. Hereditary Syndromes in Neuroendocrine Tumors. Curr. Treat. Options Oncol. 2020, 21, 50. [Google Scholar] [CrossRef]
- Faggiano, A.; Ferolla, P.; Grimaldi, F.; Campana, D.; Manzoni, M.; Davì, M.V.; Bianchi, A.; Valcavi, R.; Papini, E.; Giuffrida, D.; et al. Natural history of gastro-entero-pancreatic and thoracic neuroendocrine tumors. Data from a large prospective and retrospective Italian epidemiological study: The NET management study. J. Endocrinol. Investig. 2012, 35, 817–823. [Google Scholar]
- Ramundo, V.; Milone, F.; Severino, R.; Savastano, S.; Di Somma, C.; Vuolo, L.; De Luca, L.; Lombardi, G.; Colao, A.; Faggiano, A. Clinical and Prognostic Implications of the Genetic Diagnosis of Hereditary NET Syndromes in Asymptomatic Patients. Horm. Metab. Res. 2011, 43, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Falchetti, A. Genetics of multiple endocrine neoplasia type 1 syndrome: What’s new and what’s old. F1000Research 2017, 6, Faculty Rev-73. [Google Scholar] [CrossRef]
- Anlauf, M.; Garbrecht, N.; Bauersfeld, J.; Schmitt, A.; Henopp, T.; Komminoth, P.; Heitz, P.U.; Perren, A.; Klöppel, G. Hereditary neuroendocrine tumors of the gastroenteropancreatic system. Virchows Archiv 2007, 451, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Larsson, C.; Skogseid, B.; Oberg, K.; Nakamura, Y.; Nordenskjöld, M. Multiple endocrine neoplasia type 1 gene maps to chromosome 11 and is lost in insulinoma. Nature 1988, 332, 85–87. [Google Scholar] [CrossRef] [PubMed]
- Iyer, S.; Agarwal, S.K. Epigenetic regulation in the tumorigenesis of MEN1-associated endocrine cell types. J. Mol. Endocrinol. 2018, 61, R13–R24. [Google Scholar] [CrossRef] [PubMed]
- Brandi, M.L.; Gagel, R.F.; Angeli, A.; Bilezikian, J.P.; Beck-Peccoz, P.; Bordi, C.; Conte-Devolx, B.; Falchetti, A.; Gheri, R.G.; Libroia, A.; et al. Guidelines for diagnosis and therapy of MEN type 1 and type 2. J. Clin. Endocrinol. Metab. 2001, 86, 5658–5671. [Google Scholar] [CrossRef] [PubMed]
- Brandi, M.L.; Agarwal, S.K.; Perrier, N.D.; Lines, K.E.; Valk, G.D.; Thakker, R.V. Multiple Endocrine Neoplasia Type 1: Latest Insights. Endocr. Rev. 2021, 42, 133–170. [Google Scholar] [CrossRef]
- Thakker, R.V.; Newey, P.J.; Walls, G.V.; Bilezikian, J.; Dralle, H.; Ebeling, P.R.; Melmed, S.; Sakurai, A.; Tonelli, F.; Brandi, M.L. Clinical Practice Guidelines for Multiple Endocrine Neoplasia Type 1 (MEN1). J. Clin. Endocrinol. Metab. 2012, 97, 2990–3011. [Google Scholar] [CrossRef]
- Pieterman, C.R.C.; Vriens, M.R.; Dreijerink, K.; Van Der Luijt, R.B.; Valk, G.D. Care for patients with multiple endocrine neoplasia type 1: The current evidence base. Fam. Cancer 2010, 10, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Goudet, P.; Dalac, A.; Le Bras, M.; Cardot-Bauters, C.; Niccoli, P.; Lévy-Bohbot, N.; Du Boullay, H.; Bertagna, X.; Ruszniewski, P.; Borson-Chazot, F.; et al. MEN1 Disease Occurring Before 21 Years Old: A 160-Patient Cohort Study from the Groupe d’étude des Tumeurs Endocrines. J. Clin. Endocrinol. Metab. 2015, 100, 1568–1577. [Google Scholar] [CrossRef] [PubMed]
- Anlauf, M.; Perren, A.; Klöppel, G. Endocrine Precursor Lesions and Microadenomas of the Duodenum and Pancreas with and without MEN1: Criteria, Molecular Concepts and Clinical Significance. Pathobiology 2007, 74, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Yates, C.J.; Newey, P.J.; Thakker, R.V. Challenges and controversies in management of pancreatic neuroendocrine tumours in patients with MEN1. Lancet Diabetes Endocrinol. 2015, 3, 895–905. [Google Scholar] [CrossRef]
- Goudet, P.; Murat, A.; Binquet, C.; Cardot-Bauters, C.; Costa, A.; Ruszniewski, P.; Niccoli, P.; Ménégaux, F.; Chabrier, G.; Borson-Chazot, F.; et al. Risk Factors and Causes of Death in MEN1 Disease. A GTE (Groupe d’Etude des Tumeurs Endocrines) Cohort Study Among 758 Patients. World J. Surg. 2010, 34, 249–255. [Google Scholar] [CrossRef]
- Harper, S.; Harrison, B. First surgery for pancreatic neuroendocrine tumours in a patient with MEN1: Enucleation versus disease-modifying surgery. Clin. Endocrinol. 2015, 83, 618–621. [Google Scholar] [CrossRef]
- Agarwal, S.K. Multiple endocrine neoplasia type 1. Front. Horm. Res. 2013, 41, 1–15. [Google Scholar]
- Dogliotti, L.; Tampellini, M.; Stivanello, M.; Gorzegno, G.; Fabiani, L. The clinical management of neuroendocrine tumors with long-acting repeatable (LAR) octreotide: Comparison with standard subcutaneous octreotide therapy. Ann. Oncol. 2001, 12 (Suppl. S2), S105–S109. [Google Scholar] [CrossRef]
- Pavel, M.; O’Toole, D.; Costa, F.; Capdevila, J.; Gross, D.; Kianmanesh, R.; Krenning, E.; Knigge, U.; Salazar, R.; Pape, U.F.; et al. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology 2016, 103, 172–185. [Google Scholar] [CrossRef]
- De Herder, W.W. When and How to Use Somatostatin Analogues. Endocrinol. Metab. Clin. N. Am. 2018, 47, 549–555. [Google Scholar] [CrossRef]
- Rinke, A.; Müller, H.-H.; Schade-Brittinger, C.; Klose, K.-J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.-F.; Bläker, M.; et al. Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients with Metastatic Neuroendocrine Midgut Tumors: A Report from the PROMID Study Group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef]
- Caplin, M.E.; Pavel, M.; Ćwikła, J.B.; Phan, A.T.; Raderer, M.; Sedláčková, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Anti-tumour effects of lanreotide for pancreatic and intestinal neuroendocrine tumours: The CLARINET open-label extension study. Endocr.-Relat. Cancer 2016, 23, 191–199. [Google Scholar] [CrossRef]
- Öberg, K.E.; Reubi, J.; Kwekkeboom, D.J.; Krenning, E.P. Role of Somatostatins in Gastroenteropancreatic Neuroendocrine Tumor Development and Therapy. Gastroenterology 2010, 139, 742–753.e1. [Google Scholar] [CrossRef]
- Öberg, K.; Kvols, L.; Caplin, M.; Fave, G.D.; de Herder, W.; Rindi, G.; Ruszniewski, P.; Woltering, E.A.; Wiedenmann, B. Consensus report on the use of somatostatin analogs for the management of neuroendocrine tumors of the gastroenteropancreatic system. Ann. Oncol. 2004, 15, 966–973. [Google Scholar] [CrossRef]
- Panzuto, F.; Di Fonzo, M.; Iannicelli, E.; Sciuto, R.; Maini, C.L.; Capurso, G.; Milione, M.; Cattaruzza, M.S.; Falconi, M.; David, V.; et al. Long-term clinical outcome of somatostatin analogues for treatment of progressive, metastatic, well-differentiated entero-pancreatic endocrine carcinoma. Ann. Oncol. 2006, 17, 461–466. [Google Scholar] [CrossRef]
- Ryan, P.; McBride, A.; Ray, D.; Pulgar, S.; Ramirez, R.A.; Elquza, E.; Favaro, J.P.; Dranitsaris, G. Lanreotide vs octreotide LAR for patients with advanced gastroenteropancreatic neuroendocrine tumors: An observational time and motion analysis. J. Oncol. Pharm. Pract. 2018, 25, 1425–1433. [Google Scholar] [CrossRef] [PubMed]
- Ricci, S.; Antonuzzo, A.; Galli, L.; Ferdeghini, M.; Bodei, L.; Orlandini, C.; Conte, P. Octreotide acetate long-acting release in patients with metastatic neuroendocrine tumors pretreated with lanreotide. Ann. Oncol. 2000, 11, 1127–1130. [Google Scholar] [CrossRef] [PubMed]
- Diamantopoulos, L.; Laskaratos, F.-M.; Kalligeros, M.; Shah, R.; Navalkissoor, S.; Gnanasegaran, G.; Banks, J.; Smith, J.; Jacobs, B.; Galanopoulos, M.; et al. Antiproliferative Effect of Above-Label Doses of Somatostatin Analogs for the Management of Gastroenteropancreatic Neuroendocrine Tumors. Neuroendocrinology 2021, 111, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Yoo, C.; Hwang, H.-S.; Hong, S.-M.; Kim, K.-P.; Kim, S.Y.; Hong, Y.-S.; Kim, T.W.; Ryoo, B.-Y. Efficacy and safety of lanreotide in Korean patients with metastatic, well-differentiated gastroenteropancreatic-neuroendocrine tumors: A retrospective analysis. Investig. New Drugs 2019, 37, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Caplin, M.E.; Pavel, M.; Ruszniewski, P. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N. Engl. J. Med. 2014, 371, 1556–1557. [Google Scholar] [CrossRef] [PubMed]
- Kemm, M.H.; Manly, C.D.; Hoang, T.D.; Mai, V.Q.; Shakir, M.K.M. Octreotide Use in a Patient with MEN-1 Syndrome and Multifocal Pancreatic Neuroendocrine Tumors: A Case Report and Review of the Literature. Case Rep. Gastrointest. Med. 2019, 2019, 1–6. [Google Scholar] [CrossRef]
- Marciello, F.; Di Somma, C.; Del Prete, M.; Marotta, V.; Ramundo, V.; Carratù, A.; Roseto, C.D.L.D.; Camera, L.; Colao, A.; Faggiano, A. Combined biological therapy with lanreotide autogel and cabergoline in the treatment of MEN-1-related insulinomas. Endocrine 2014, 46, 678–681. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yamaguchi, M.; Yamada, Y.; Hosokawa, Y.; Iwamoto, R.; Tamba, S.; Ihara, A.; Yamamoto, K.; Hoshida, Y.; Matsuzawa, Y. Long-Term Suppressive Effect of Octreotide on Progression of Metastatic Gastrinoma with Multiple Endocrine Neoplasia Type 1: Seven-Year Follow up. Intern. Med. 2010, 49, 1557–1563. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Daniels, L.M.; Khalili, M.; Morano, W.F.; Simoncini, M.; Mapow, B.C.; Leaf, A.; Bowne, W.B. Case report: Optimal tumor cytoreduction and octreotide with durable disease control in a patient with MEN-1 and Zollinger-Ellison syndrome—Over a decade of follow-up. World J. Surg. Oncol. 2019, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tomassetti, P.; Migliori, M.; Caletti, G.C.; Fusaroli, P.; Corinaldesi, R.; Gullo, L. Treatment of Type II Gastric Carcinoid Tumors with Somatostatin Analogues. N. Engl. J. Med. 2000, 343, 551–554. [Google Scholar] [CrossRef] [PubMed]
- Ohno, A.; Fujimori, N.; Miki, M.; Oono, T.; Igarashi, H.; Matsuda, R.; Koga, Y.; Oda, Y.; Ohtsuka, T.; Nakamura, M.; et al. Collision of a pancreatic ductal adenocarcinoma and a pancreatic neuroendocrine tumor associated with multiple endocrine neoplasm type 1. Clin. J. Gastroenterol. 2021, 14, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.E.; Vogel, O.H.; Lopes, M.B.S.; Chang, S.D.; Katznelson, L. Ectopic Acromegaly due to A Pancreatic Neuroendocrine Tumor Producing Growth Hormone-Releasing Hormone. Endocr. Pract. 2011, 17, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Massironi, S.; Rossi, R.; Ferrero, S.; Cavalcoli, F.; Spampatti, M.; Conte, D.; Corbetta, S.; Peracchi, M. An esophageal gastrointestinal stromal tumor in a patient with MEN1-related pancreatic gastrinoma: An unusual association and review of the literature. J. Cancer Res. Ther. 2014, 10, 443. [Google Scholar] [CrossRef] [PubMed]
- Shiihara, M.; Izumo, W.; Higuchi, R.; Yazawa, T.; Uemura, S.; Furukawa, T.; Yamamoto, M. A case of long-survival insulinoma with multiple neuroendocline tumour type 1 controlled by multimodal therapy. J. Surg. Case Rep. 2017, 2017, rjx244. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Li, Y.; Su, X.; Tan, H. Type 2 gastric neuroendocrine tumor: Report of one case. Transl. Gastroenterol. Hepatol. 2016, 1, 88. [Google Scholar] [CrossRef]
- Sala, E.; Ferrante, E.; Verrua, E.; Malchiodi, E.; Mantovani, G.; Filopanti, M.; Ferrero, S.; Pietrabissa, A.; Vanoli, A.; La Rosa, S.; et al. Growth hormone-releasing hormone-producing pancreatic neuroendocrine tumor in a multiple endocrine neoplasia type 1 family with an uncommon phenotype. Eur. J. Gastroenterol. Hepatol. 2013, 25, 858–862. [Google Scholar] [CrossRef] [PubMed]
- Cioppi, F.; Cianferotti, L.; Masi, L.; Giusti, F.; Brandi, M.L. The LARO-MEN1 study: A longitudinal clinical experience with octreotide Long-Acting Release in patients with Multiple Endocrine Neoplasia type 1 Syndrome. Clin. Cases Min. Bone Metab. 2017, 14, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.R.; Greenaway, T.M.; Parameswaran, V.; Shepherd, J.J. Octreotide improves biochemical, radiologic, and symptomatic indices of gastroenteropancreatic neoplasia in patients with multiple endocrine neoplasia type 1 (MEN-1). Implications for an integrated model of MEN-1 tumorigenesis. Cancer 1999, 86, 2154–2159. [Google Scholar] [CrossRef]
- Faggiano, A.; Modica, R.; Calzo, F.L.; Camera, L.; Napolitano, V.; Altieri, B.; De Cicco, F.; Bottiglieri, F.; Sesti, F.; Badalamenti, G.; et al. Lanreotide Therapy vs Active Surveillance in MEN1-Related Pancreatic Neuroendocrine Tumors < 2 Centimeters. J. Clin. Endocrinol. Metab. 2020, 105, 78–84. [Google Scholar]
- Shojamanesh, H.; Gibril, F.; Louie, A.; Ojeaburu, J.V.; Bashir, S.; Abou-Saif, A.; Jensen, R.T. Prospective study of the antitumor efficacy of long-term octreotide treatment in patients with progressive metastatic gastrinoma. Cancer 2002, 94, 331–343. [Google Scholar] [CrossRef] [PubMed]
- Ferolla, P.; Faggiano, A.; Grimaldi, F.; Ferone, D.; Scarpelli, G.; Ramundo, V.; Severino, R.; Bellucci, M.C.; Camera, L.M.; Lombardi, G.; et al. Shortened interval of long-acting octreotide administration is effective in patients with well-differentiated neuroendocrine carcinomas in progression on standard doses. J. Endocrinol. Investig. 2012, 35, 326–331. [Google Scholar]
- Ito, T.; Honma, Y.; Hijioka, S.; Kudo, A.; Fukutomi, A.; Nozaki, A.; Kimura, Y.; Motoi, F.; Isayama, H.; Komoto, I.; et al. Phase II study of lanreotide autogel in Japanese patients with unresectable or metastatic well-differentiated neuroendocrine tumors. Investig. New Drugs 2017, 35, 499–508. [Google Scholar] [CrossRef]
- Ramundo, V.; Del Prete, M.; Marotta, V.; Marciello, F.; Camera, L.; Napolitano, V.; De Luca, L.; Circelli, L.; Colantuoni, V.; Di Sarno, A.; et al. Impact of long-acting octreotide in patients with early-stage MEN1-related duodeno-pancreatic neuroendocrine tumours. Clin. Endocrinol. 2014, 80, 850–855. [Google Scholar] [CrossRef]
- Oleinikov, K.; Uri, I.; Jacob, H.; Epshtein, J.; Benson, A.; Ben-Haim, S.; Atlan, K.; Tal, I.; Meirovitz, A.; Maimon, O.; et al. Long-term outcomes in MEN-1 patients with pancreatic neuroendocrine neoplasms: An Israeli specialist center experience. Endocrine 2020, 68, 222–229. [Google Scholar] [CrossRef]
- Faggiano, A.; Carratù, A.C.; Guadagno, E.; Tafuto, S.; Tatangelo, F.; Riccardi, F.; Mocerino, C.; Palmieri, G.; Damiano, V.; Siciliano, R.; et al. Somatostatin analogues according to Ki67 index in neuroendocrine tumours: An observational retrospective-prospective analysis from real life. Oncotarget 2016, 7, 5538–5547. [Google Scholar] [CrossRef]
- Ducreux, M.; Ruszniewski, P.; Chayvialle, J.A.; Blumberg, J.; Cloarec, D.; Michel, H.; Raymond, J.M.; Dupas, J.L.; Gouerou, H.; Jian, R.; et al. The antitumoral effect of the long-acting somatostatin analog lanreotide in neuroendocrine tumors. Am. J. Gastroenterol. 2000, 95, 3276–3281. [Google Scholar] [CrossRef] [PubMed]
- Wymenga, A.; Eriksson, B.; Salmela, P.; Jacobsen, M.; Van Cutsem, E.; Fiasse, R.; Välimäki, M.; Renstrup, J.; De Vries, E.; Öberg, K. Efficacy and Safety of Prolonged-Release Lanreotide in Patients with Gastrointestinal Neuroendocrine Tumors and Hormone-Related Symptoms. J. Clin. Oncol. 1999, 17, 1111. [Google Scholar] [CrossRef] [PubMed]
- Lamberti, G.; Faggiano, A.; Brighi, N.; Tafuto, S.; Ibrahim, T.; Brizzi, M.P.; Pusceddu, S.; Albertelli, M.; Massironi, S.; Panzuto, F.; et al. Nonconventional Doses of Somatostatin Analogs in Patients with Progressing Well-Differentiated Neuroendocrine Tumor. J. Clin. Endocrinol. Metab. 2020, 105, 194–200. [Google Scholar] [CrossRef]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Al-Salameh, A.; Cadiot, G.; Calender, A.; Goudet, P.; Chanson, P. Clinical aspects of multiple endocrine neoplasia type 1. Nat. Rev. Endocrinol. 2021, 17, 207–224. [Google Scholar] [CrossRef]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Klöppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef]
- Bertherat, J.; Tenenbaum, F.; Perlemoine, K.; Videau, C.; Alberini, J.L.; Richard, B.; Dousset, B.; Bertagna, X.; Epelbaum, J. Somatostatin Receptors 2 and 5 Are the Major Somatostatin Receptors in Insulinomas: An in Vivo and in Vitro Study. J. Clin. Endocrinol. Metab. 2003, 88, 5353–5360. [Google Scholar] [CrossRef][Green Version]
- Theodoropoulou, M.; Stalla, G.K. Somatostatin receptors: From signaling to clinical practice. Front. Neuroendocrinol. 2013, 34, 228–252. [Google Scholar] [CrossRef]
- Qian, Z.R.; Li, T.; Ter-Minassian, M.; Yang, J.; Chan, J.A.; Brais, L.K.; Masugi, Y.; Thiaglingam, A.; Brooks, N.; Nishihara, R.; et al. Association Between Somatostatin Receptor Expression and Clinical Outcomes in Neuroendocrine Tumors. Pancreas 2016, 45, 1386–1393. [Google Scholar] [CrossRef]
- Okuwaki, K.; Kida, M.; Mikami, T.; Yamauchi, H.; Imaizumi, H.; Miyazawa, S.; Iwai, T.; Takezawa, M.; Saegusa, M.; Watanabe, M.; et al. Clinicopathologic characteristics of pancreatic neuroendocrine tumors and relation of somatostatin receptor type 2A to outcomes. Cancer 2013, 119, 4094–4102. [Google Scholar] [CrossRef]
- Gomes-Porras, M.; Cárdenas, J.J.; Álvarez-Escolá, C. Somatostatin Analogs in Clinical Practice: A Review. Int. J. Mol. Sci. 2020, 21, 1682. [Google Scholar] [CrossRef] [PubMed]
- Kidd, M.; Modlin, I.M.; Bodei, L.; Drozdov, I. Decoding the Molecular and Mutational Ambiguities of Gastroenteropancreatic Neuroendocrine Neoplasm Pathobiology. Cell. Mol. Gastroenterol. Hepatol. 2015, 1, 131–153. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | n = 105 (100%) |
|---|---|
| Gender | |
| Data available | 41 (40%) |
| Men | 17 (41.5%) |
| Women | 24 (58.5%) |
| NA | 64 (61.0%) |
| Median age | 44 years (18–73) |
| Functioning NEN | |
| Data available | 83 (79%) |
| Yes | 31 (37.3%) |
| No | 52 (62.7%) |
| NA | 22 (21%) |
| Type of syndrome in functioning NEN | |
| Data available | 29 (27.6%) |
| Gastrinoma | 19 (65.6%) |
| Glucagonoma | 6 (20.7%) |
| Insulinoma | 2 (6.9%) |
| Somatostatinoma | 1 (3.4%) |
| Gastrinoma + insulinoma | 1 (3.4%) |
| NA | 76 (72.4%) |
| Stage | |
| Data available | 92 (87.6%) |
| I | 73 (79.3%) |
| II | 5 (5.4%) |
| III | 0 (0.0%) |
| IV | 14 (15.2%) |
| NA | 13 (12.4%) |
| Number of pancreatic nodules | |
| Data available | 64 (60.9%) |
| 1 | 25 (39.1%) |
| >1 | 39 (60.9%) |
| NA | 41 (39.0%) |
| Grade | |
| Data available | 29 (27.6%) |
| 1 | 10 (34.5%) |
| 2 | 19 (65.5%) |
| NA | 76 (72.4%) |
| Median Ki67 index (%) | |
| 2 (1–8) | |
| MEN1 manifestations | |
| Data available | 33 (31.5%) |
| Hyperparathyroidism | 15 (45.5%) |
| Pituitary adenoma | 1 (3.0%) |
| Hyperparathyroidism and pituitary adenoma | 17 (51.5%) |
| NA | 72 (68.6%) |
| Surgery | |
| Data available | 54 (51.4%) |
| Yes | 23 (42.6%) |
| No | 31 (57.4%) |
| NA | 51 (48.6%) |
| Short-acting SSA therapy | |
| Yes | 24 (22.9%) |
| No | 81 (77.1%) |
| Octreotide LAR | |
| Yes | 73 (69.5%) |
| No | 32 (30.5%) |
| Lanreotide LAR | |
| Yes | 28 (26.7%) |
| No | 77 (73.3%) |
| Response to SSA therapy | |
| Data available | 78 (74.2%) |
| SD | 59 (75.6%) |
| PR | 7 (9.0%) |
| CR | 3 (3.8%) |
| PD | 9 (11.5%) |
| NA | 27 (25.7%) |
| Side effects to SSA therapy | |
| No | 95 (90.4%) |
| Gallstones | 6 (5.7%) |
| Hyperglycaemia | 2 (1.9%) |
| Gastrointestinal (nausea, diarrhea) | 1 (0.9%) |
| Pain | 1 (0.9%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Salvia, A.; Sesti, F.; Grinzato, C.; Mazzilli, R.; Tarsitano, M.G.; Giannetta, E.; Faggiano, A. Somatostatin Analogue Therapy in MEN1-Related Pancreatic Neuroendocrine Tumors from Evidence to Clinical Practice: A Systematic Review. Pharmaceuticals 2021, 14, 1039. https://doi.org/10.3390/ph14101039
La Salvia A, Sesti F, Grinzato C, Mazzilli R, Tarsitano MG, Giannetta E, Faggiano A. Somatostatin Analogue Therapy in MEN1-Related Pancreatic Neuroendocrine Tumors from Evidence to Clinical Practice: A Systematic Review. Pharmaceuticals. 2021; 14(10):1039. https://doi.org/10.3390/ph14101039
Chicago/Turabian StyleLa Salvia, Anna, Franz Sesti, Chiara Grinzato, Rossella Mazzilli, Maria Grazia Tarsitano, Elisa Giannetta, and Antongiulio Faggiano. 2021. "Somatostatin Analogue Therapy in MEN1-Related Pancreatic Neuroendocrine Tumors from Evidence to Clinical Practice: A Systematic Review" Pharmaceuticals 14, no. 10: 1039. https://doi.org/10.3390/ph14101039
APA StyleLa Salvia, A., Sesti, F., Grinzato, C., Mazzilli, R., Tarsitano, M. G., Giannetta, E., & Faggiano, A. (2021). Somatostatin Analogue Therapy in MEN1-Related Pancreatic Neuroendocrine Tumors from Evidence to Clinical Practice: A Systematic Review. Pharmaceuticals, 14(10), 1039. https://doi.org/10.3390/ph14101039