Trends in Antidepressants Use in Spain between 2015 and 2018: Analyses from a Population-Based Registry Study with Reference to Driving

 ,
,  ,
, 

Abstract
:1. Introduction
2. Experimental Section
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kim, M.J.; Kim, N.; Shin, D.; Rhee, S.J.; Park, C.H.K.; Kim, H.; Cho, S.J.; Lee, J.W.; Kim, E.Y.; Yang, B.; et al. The epidemiology of antidepressant use in South Korea: Does short-term antidepressant use affect the relapse and recurrence of depressive episodes? PLoS ONE 2019, 14, e0222791. [Google Scholar] [CrossRef]
- Carvalho, A.F.; Sharma, M.S.; Brunoni, A.R.; Vieta, E.; Fava, G.A. The Safety, Tolerability and Risks Associated with the Use of Newer Generation Antidepressant Drugs: A Critical Review of the Literature. Psychother. Psychosom. 2016, 85, 270–288. [Google Scholar] [CrossRef]
- Hill, L.L.; Lauzon, V.L.; Winbrock, E.L.; Li, G.; Chihuri, S.; Lee, K.C. Depression, antidepressants and driving safety. Inj. Epidemiol. 2017, 4, 10. [Google Scholar] [CrossRef] [Green Version]
- Lahera, G.; Andrade-González, N.; Gasull, V.; Pagés-Lluyot, J.R.; Roca, M. [The public perception of depression in Spain]. An. Sist. Sanit. Navar. 2019, 42, 31–39. [Google Scholar] [PubMed] [Green Version]
- Wingen, M.; Ramaekers, J.G.; Schmitt, J.A.J. Driving impairment in depressed patients receiving long-term antidepressant treatment. Psychopharmacology 2006, 188, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Van der Sluiszen, N.N.J.J.M.; Wingen, M.; Vermeeren, A.; Vinckenbosch, F.; Jongen, S.; Ramaekers, J.G. Driving performance of depressed patients who are untreated or receive long-term antidepressant (SSRI/SNRI) treatment. Pharmacopsychiatry 2017, 50, 182–188. [Google Scholar] [CrossRef]
- Ménard, I.; Korner-Bitensky, N.; Dobbs, B.; Casacalenda, N.; Beck, P.R.; Dippsych, C.M.; Gélinas, I.; Molnar, F.J.; Naglie, G. Canadian psychiatrists’ current attitudes, practices, and knowledge regarding fitness to drive in individuals with mental illness: a cross-Canada survey. Can. J. Psychiatry Rev. Can. Psychiatr. 2006, 51, 836–846. [Google Scholar] [CrossRef] [Green Version]
- Brunnauer, A.; Laux, G. The effects of most commonly prescribed second generation antidepressants on driving ability: A systematic review: 70th Birthday Prof. Riederer. J. Neural Transm. Vienna Austria 1996 2013, 120, 225–232. [Google Scholar] [CrossRef]
- Brunnauer, A.; Buschert, V.; Fric, M.; Distler, G.; Sander, K.; Segmiller, F.; Zwanzger, P.; Laux, G. Driving performance and psychomotor function in depressed patients treated with agomelatine or venlafaxine. Pharmacopsychiatry 2015, 48, 65–71. [Google Scholar] [CrossRef]
- Ravera, S.; Ramaekers, J.G.; de Jong-van den Berg, L.T.W.; de Gier, J.J. Are selective serotonin reuptake inhibitors safe for drivers? What is the evidence? Clin. Ther. 2012, 34, 1070–1083. [Google Scholar] [CrossRef]
- WHO. Collaborating Centre for Drug Statistics Methodology—ATC/DDD Index 2020. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 23 February 2020).
- Ivers, T.; White, N.D. Potentially Driver-Impairing Medications: Risks and Strategies for Injury Prevention. Am. J. Lifestyle Med. 2016, 10, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Trindade, E.; Menon, D.; Topfer, L.A.; Coloma, C. Adverse effects associated with selective serotonin reuptake inhibitors and tricyclic antidepressants: a meta-analysis. CMAJ Can. Med. Assoc. J. J. Assoc. Medicale Can. 1998, 159, 1245–1252. [Google Scholar]
- Brunnauer, A.; Laux, G. Driving under the influence of antidepressants: A systematic review and update of the evidence of experimental and controlled clinical studies. Pharmacopsychiatry 2017, 50, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Ray, W.A.; Fought, R.L.; Decker, M.D. Psychoactive drugs and the risk of injurious motor vehicle crashes in elderly drivers. Am. J. Epidemiol. 1992, 136, 873–883. [Google Scholar] [CrossRef]
- Leveille, S.G.; Buchner, D.M.; Koepsell, T.D.; McCloskey, L.W.; Wolf, M.E.; Wagner, E.H. Psychoactive medications and injurious motor vehicle collisions involving older drivers. Epidemiol. Camb. Mass 1994, 5, 591–598. [Google Scholar] [CrossRef]
- Iwamoto, K.; Takahashi, M.; Nakamura, Y.; Kawamura, Y.; Ishihara, R.; Uchiyama, Y.; Ebe, K.; Noda, A.; Noda, Y.; Yoshida, K.; et al. The effects of acute treatment with paroxetine, amitriptyline, and placebo on driving performance and cognitive function in healthy Japanese subjects: a double-blind crossover trial. Hum. Psychopharmacol. 2008, 23, 399–407. [Google Scholar] [CrossRef]
- Bramness, J.G.; Skurtveit, S.; Neutel, C.I.; Mørland, J.; Engeland, A. Minor increase in risk of road traffic accidents after prescriptions of antidepressants: a study of population registry data in Norway. J. Clin. Psychiatry 2008, 69, 1099–1103. [Google Scholar] [CrossRef]
- Barbone, F.; McMahon, A.D.; Davey, P.G.; Morris, A.D.; Reid, I.C.; McDevitt, D.G.; MacDonald, T.M. Association of road-traffic accidents with benzodiazepine use. Lancet Lond. Engl. 1998, 352, 1331–1336. [Google Scholar] [CrossRef]
- Ravera, S.; Monteiro, S.P.; de Gier, J.J.; van der Linden, T.; Gómez-Talegón, T.; Álvarez, F.J. A European approach to categorizing medicines for fitness to drive: outcomes of the DRUID project. Br. J. Clin. Pharmacol. 2012, 74, 920–931. [Google Scholar] [CrossRef] [Green Version]
- Tamblyn, R.; Bates, D.W.; Buckeridge, D.L.; Dixon, W.; Forster, A.J.; Girard, N.; Haas, J.; Habib, B.; Kurteva, S.; Li, J.; et al. Multinational comparison of new antidepressant use in older adults: A cohort study. BMJ Open 2019, 9, e027663. [Google Scholar] [CrossRef]
- Arthur, A.; Savva, G.M.; Barnes, L.E.; Borjian-Boroojeny, A.; Dening, T.; Jagger, C.; Matthews, F.E.; Robinson, L.; Brayne, C. Cognitive function and ageing studies collaboration changing prevalence and treatment of depression among older people over two decades. Br. J. Psychiatry J. Ment. Sci. 2019, 1–6. [Google Scholar]
- Agencia Española del Medicamento y Productos Sanitarios. INFORME DE UTILIZACIÓN DE MEDICAMENTOS U/AD/V1/14012015. Utilización de Medicamentos Antidepresivos en España Durante el Periodo 2000–2013. 2015. Available online: https://www.cofm.es/recursos/doc/portal/2015/04/24/informe-de-utilizacion-de-medicamentos-de-la-agencia-espanola-de-medicamentos-y-.pdf (accessed on 3 April 2020).
- Gutierrez-Abejón, E.; Herrera-Gómez, F.; Criado-Espegel, P.; Alvarez, F.J. Use of driving-impairing medicines by a Spanish population: a population-based registry study. BMJ Open 2017, 7, e017618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera-Gómez, F.; Gutierrez-Abejón, E.; Criado-Espegel, P.; Álvarez, F.J. The problem of benzodiazepine use and its extent in the driver population: a population-based registry study. Front. Pharmacol. 2018, 9, 408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera-Gómez, F.; Gutierrez-Abejón, E.; Álvarez, F.J. Antipsychotics in the general population and the driver population: comparisons from a population-based registry study. Int. Clin. Psychopharmacol. 2019, 34, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Gómez, F.; Gutierrez-Abejón, E.; Ayestarán, I.; Criado-Espegel, P.; Álvarez, F.J. The trends in opioid use in castile and leon, Spain: A population-based registry analysis of dispensations in 2015 to 2018. J. Clin. Med. 2019, 8, 2148. [Google Scholar] [CrossRef] [Green Version]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M. RECORD working committee the REporting of studies conducted using observational routinely-collected health data (RECORD) statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef]
- Rapoport, M.J.; Zagorski, B.; Seitz, D.; Herrmann, N.; Molnar, F.; Redelmeier, D.A. At-fault motor vehicle crash risk in elderly patients treated with antidepressants. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2011, 19, 998–1006. [Google Scholar] [CrossRef]
- Mamdani, M.; Rapoport, M.; Shulman, K.I.; Herrmann, N.; Rochon, P.A. Mental health-related drug utilization among older adults: prevalence, trends, and costs. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2005, 13, 892–900. [Google Scholar] [CrossRef]
- Montagnier, D.; Barberger-Gateau, P.; Jacqmin-Gadda, H.; Dartigues, J.-F.; Rainfray, M.; Pérès, K.; Lechevallier-Michel, N.; Fourrier-Réglat, A. Evolution of prevalence of depressive symptoms and antidepressant use between 1988 and 1999 in a large sample of older French people: Results from the personnes agées quid study. J. Am. Geriatr. Soc. 2006, 54, 1839–1845. [Google Scholar] [CrossRef]
- Reynolds, K.; Pietrzak, R.H.; El-Gabalawy, R.; Mackenzie, C.S.; Sareen, J. Prevalence of psychiatric disorders in U.S. older adults: findings from a nationally representative survey. World Psychiatry Off. J. World Psychiatr. Assoc. WPA 2015, 14, 74–81. [Google Scholar] [CrossRef] [Green Version]
- Fournier, J.-P.; Wilchesky, M.; Patenaude, V.; Suissa, S. Concurrent use of benzodiazepines and antidepressants and the risk of motor vehicle accident in older drivers: A nested case-control study. Neurol. Ther. 2015, 4, 39–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wickens, C.M.; Mann, R.E.; Stoduto, G.; Ialomiteanu, A.; Smart, R.G.; Rehm, J. The impact of probable anxiety and mood disorder on self-reported collisions: a population study. J. Affect. Disord. 2013, 145, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Orriols, L.; Queinec, R.; Philip, P.; Gadegbeku, B.; Delorme, B.; Moore, N.; Suissa, S.; Lagarde, E. CESIR Research Group Risk of injurious road traffic crash after prescription of antidepressants. J. Clin. Psychiatry 2012, 73, 1088–1094. [Google Scholar] [CrossRef]
- Gebara, M.A.; Lipsey, K.L.; Karp, J.F.; Nash, M.C.; Iaboni, A.; Lenze, E.J. Cause or effect? Selective serotonin reuptake inhibitors and falls in older adults: A systematic review. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2015, 23, 1016–1028. [Google Scholar] [CrossRef] [Green Version]
- Verster, J.C.; van de Loo, A.J.A.E.; Roth, T. Mirtazapine as positive control drug in studies examining the effects of antidepressants on driving ability. Eur. J. Pharmacol. 2015, 753, 252–256. [Google Scholar] [CrossRef]
- Ramaekers, J.G. Antidepressants and driver impairment: empirical evidence from a standard on-the-road test. J. Clin. Psychiatry 2003, 64, 20–29. [Google Scholar] [CrossRef]
- Ravera, S.; van Rein, N.; de Gier, J.J.; de Jong-van den Berg, L.T.W. Road traffic accidents and psychotropic medication use in The Netherlands: a case-control study. Br. J. Clin. Pharmacol. 2011, 72, 505–513. [Google Scholar] [CrossRef] [Green Version]
- Fischer, B.; Fidalgo, T.; Varatharajan, T. Reflections on pollini et al. (2017)-Implications for interventions for driving while using psychotropic medications with impairment risk. J. Stud. Alcohol Drugs 2017, 78, 814–816. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Antidepressant | Population Using Antidepressants % (95CI) | Drivers Using Antidepressants % (95CI) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Yearly Use | Daily Use | Type of Use | Yearly Use | Daily Use | Type of Use | |||||
| Acute | Subacute | Chronic | Acute | Subacute | Chronic | |||||
| Total Antidepressants | ||||||||||
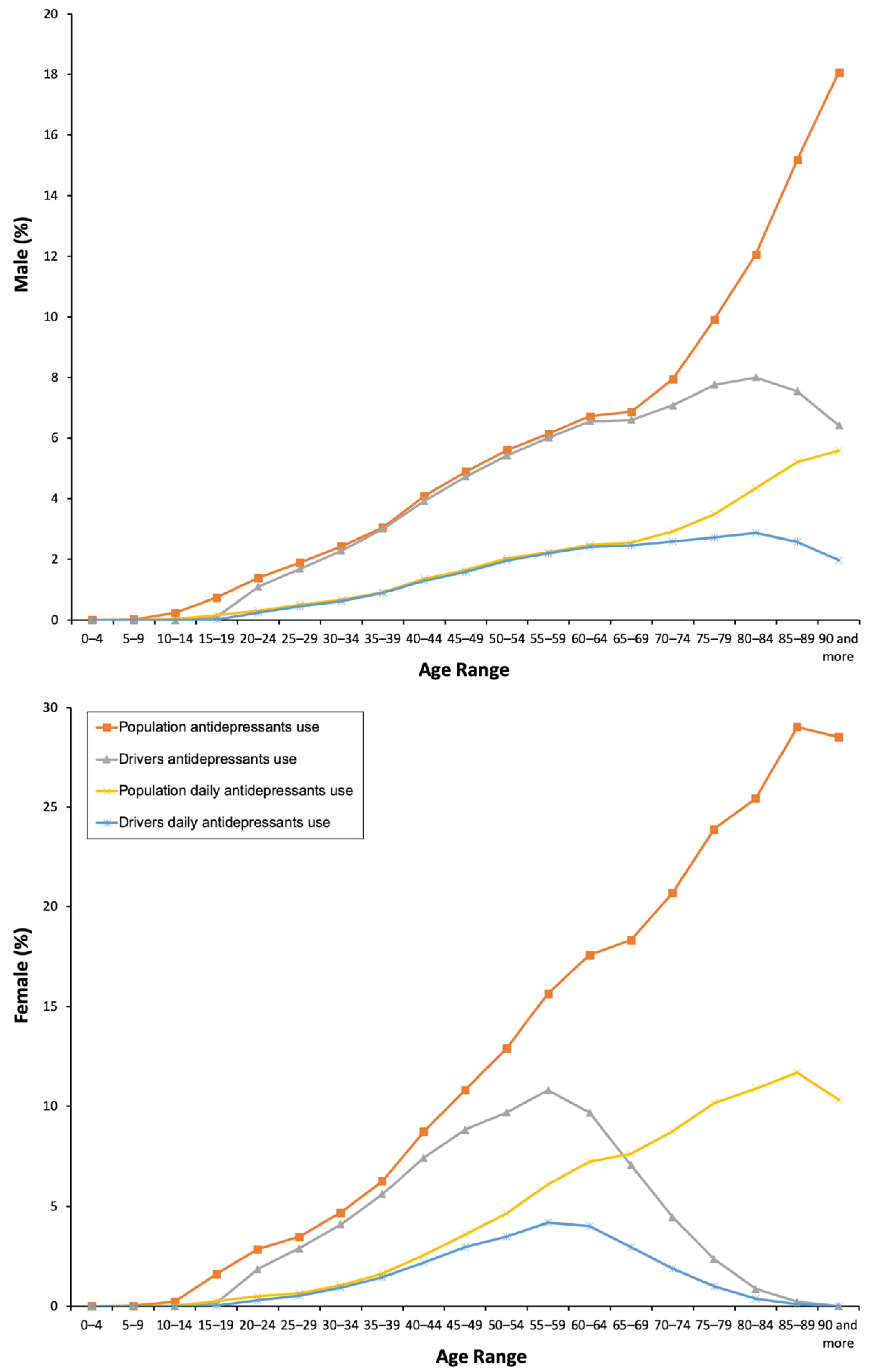
| TOTAL | 8.56 (8.52–8.59) | 3.15 (3.13–3.17) | 0.05 (0.04–0.06) | 0.23 (0.22–0.24) | 8.28 (8.25–8.32) | 5.66 (5.62–5.70) | 1.93 (1.91–1.95) | 0.04 (0.03–0.05) | 0.21 (0.20–0.21) | 5.41 (5.37–5.44) |
| Male | 4.87 (4.83–4.91) | 1.68 (1.65–1.70) | 0.03 (0.02–0.04) | 0.15 (0.14–0.15) | 4.70 (4.66–4.74) | 4.83 (4.78–4.87) | 1.68 (1.65–1.70) | 0.03 (0.02–0.04) | 0.16 (0.15–0.16) | 4.64 (4.60–4.69) |
| Female | 12.12 (12.06–12.17) | 4.57 (4.54–4.61) | 0.07 (0.06–0.08) | 0.31 (0.30–0.32) | 11.74 (11.68–11.80) | 6.90 (6.83–6.96) | 2.31 (2.27–2.35) | 0.07 (0.06–0.08) | 0.16 (0.15–0.17) | 4.64 (4.59–4.70) |
| Χ² = 1325.124; p = 0.001 | Χ² = 4531.330; p = 0.001 | Χ² = 32.612; p = 0.013 | Χ² = 76.08; p = 0.001 | Χ² = 7024.208; p=0.001 | Χ² = 14360.161; p = 0.001 | Χ² = 14615.499; p = 0.001 | Χ² = 1160.409; p = 0.001 | Χ² = 6083.759; p = 0.001 | Χ² = 43897.32; p = 0.001 | |
| Non-selective monoamine reuptake inhibitors | ||||||||||
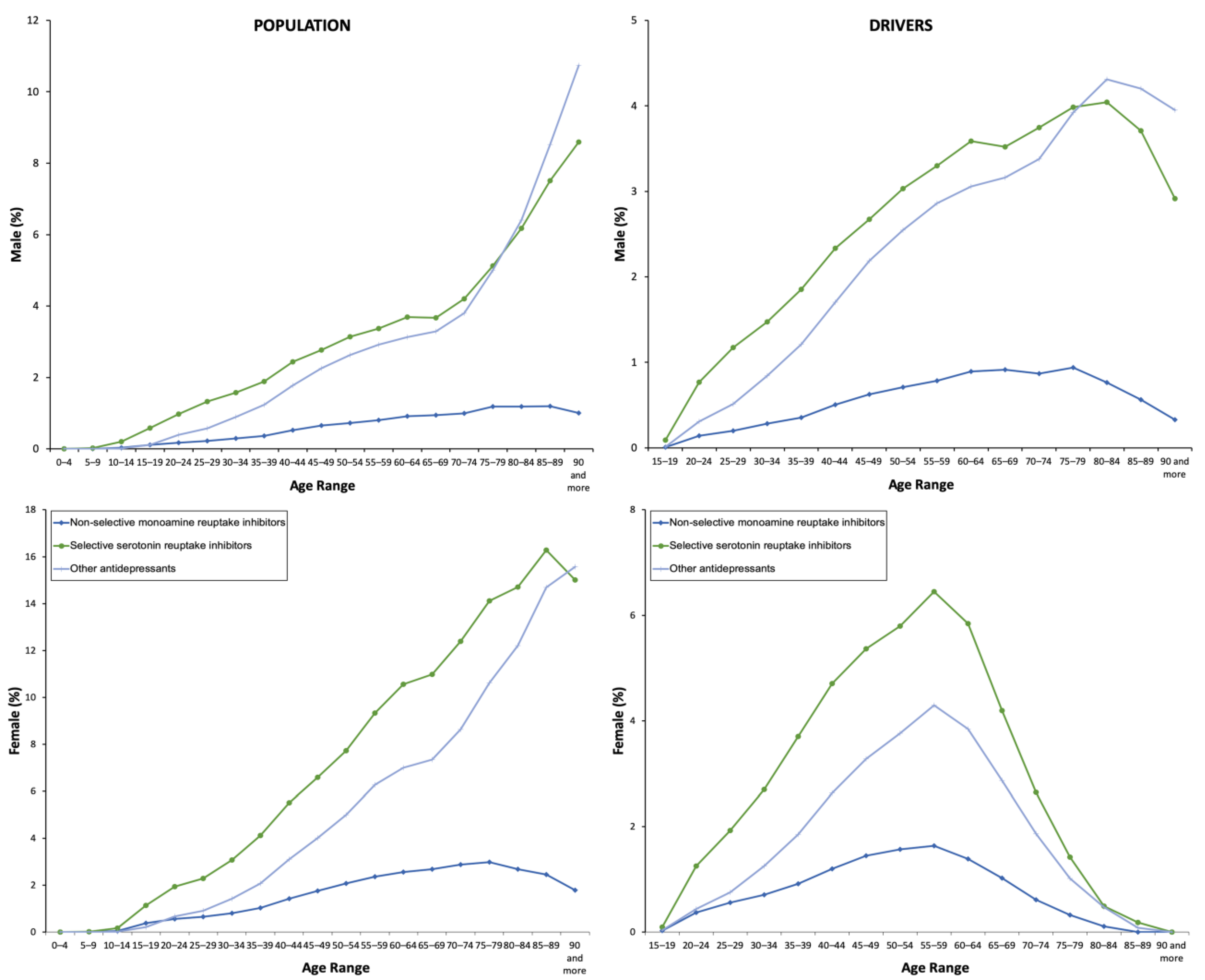
| TOTAL | 1.11 (1.10–1.13) | 0.05 (0.04–0.05) | 0.17 (0.16–0.17) | 0.30 (0.29–0.31) | 0.64 (0.63–0.65) | 0.80 (0.70–0.90) | 0.04 (0.03–0.05) | 0.14 (0.13–0.15) | 0.24 (0.24–0.25) | 0.42 (0.41–0.43) |
| Male | 0.58 (0.57–0.59) | 0.03 (0.03–0.04) | 0.08 (0.08–0.09) | 0.16 (0.15–0.17) | 0.34 (0.32–0.35) | 0.61 (0.59–0.63) | 0.04 (0.03–0.05) | 0.09 (0.08–0.10) | 0.17 (0.16–0.18) | 0.35 (0.34–0.36) |
| Female | 1.63 (1.61–1.65) | 0.06 (0.05–0.06) | 0.25 (0.24–0.26) | 0.44 (0.43–0.45) | 0.94 (0.92–0.96) | 1.10 (0.99–1.12) | 0.03 (0.02–0.04) | 0.21 (0.2–0.22) | 0.35 (0.34–0.37) | 0.53 (0.51–0.55) |
| Χ² = 48.521; p = 0.001 | Χ² = 306.885; p = 0.001 | Χ² = 36.373; p = 0.004 | Χ² = 51.54; p = 0.001 | Χ² = 392.684; p = 0.001 | Χ² = 1837.676; p = 0.001 | Χ² = 113.888; p = 0.023 | Χ² = 1149.338; p = 0.013 | Χ² = 2029.683; p = 0.001 | Χ² = 3326.979; p = 0.001 | |
| Selective serotonin reuptake inhibitors | ||||||||||
| TOTAL | 4.99 (4.96–5.02) | 2.22 (2.20–2.24) | - | 0.23 (0.22–0.24) | 4.76 (4.73–4.79) | 3.32 (3.29–3.35) | 1.33 (1.31–1.35) | - | 0.19 (0.18–0.20) | 3.13 (3.10–3.16) |
| Male | 2.69 (2.66–2.72) | 1.16 (1.14–1.18) | - | 0.30 (0.29–0.31) | 0.64 (0.63–0.66) | 2.69 (2.65–2.72) | 1.14 (1.12–1.16) | - | 0.14 (0.13–0.15) | 2.55 (2.51–2.58) |
| Female | 7.22 (7.17–7.26) | 3.24 (3.21–3.27) | - | 0.32 (0.31–0.33) | 6.90 (6.85–6.94) | 4.26 (4.21–4.32) | 1.62 (1.59–1.65) | - | 0.26 (0.25–0.27) | 4.00 (3.95–4.05) |
| Χ² = 1009.602; p = 0.001 | Χ² = 2947.450; p = 0.001 | - | Χ² = 114.15; p = 0.001 | Χ² = 4329.346; p = 0.001 | Χ² = 6700.641; p = 0.001 | Χ² = 10488.675; p = 0.001 | - | Χ² = 1231.407; p = 0.001 | Χ² = 23530.089; p = 0.001 | |
| Other antidepressants | ||||||||||
| TOTAL | 3.71 (3.69–3.74) | 0.97 (0.96–0.99) | - | 0.43 (0.42–0.44) | 3.28 (3.26–3.3) | 2.36 (2.34–2.39) | 0.62 (0.61–0.63) | - | 0.31 (0.30–0.32) | 2.05 (2.03–2.07) |
| Male | 2.31 (2.28–2.34) | 0.54 (0.53–0.55) | - | 0.29 (0.28–0.30) | 2.02 (1.99–2.04) | 2.24 (2.21–2.27) | 0.56 (0.54–0.57) | - | 0.29 (0.28–0.30) | 1.95 (1.93–1.98) |
| Female | 5.07 (5.03–5.11) | 1.39 (1.37–1.41) | - | 0.56 (0.55–0.57) | 4.51 (4.47–4.54) | 2.54 (2.50–2.58) | 0.71 (0.69–0.73) | - | 0.35 (0.33–0.36) | 2.19 (2.15–2.23) |
| Χ² = 661.836; p = 0.001 | Χ² = 1423.581; p = 0.001 | - | Χ² = 98.22; p = 0.001 | Χ² = 3157.1; p = 0.001 | Χ² = 5506.160; p = 0.001 | Χ² = 4202.911; p = 0.001 | - | Χ² = 2613.557; p = 0.001 | Χ² = 16278.972; p = 0.001 | |
| ATC Code | Description | Population % (95CI) | Drivers % (95CI) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Yearly Use | Daily Use | Yearly Use | Daily Use | ||||||
| Male | Female | Male | Female | Male | Female | Male | Female | ||
| N05B | Ansyolitics | 53.65 (53.36–53.94) | 60.80 (60.51–61.09) | 61.21 (60.52–61.89) | 69.3 (68.91–69.68) | 55.22 (54.75–55.7) | 61.89 (61.42–62.37) | 62.75 (61.97–63.53) | 71.85 (71.09–72.60) |
| Χ² = 1026.420; p = 0.001 | Χ² = 845.748; p = 0.001 | Χ² = 6479.230; p = 0.001 | Χ² = 2593.569; p = 0.001 | ||||||
| N02A | Opioids | 20.84 (20.5–21.17) | 28.61 (28.38–28.84) | 20.77 (20.20–21.34) | 31.76 (31.37–32.15) | 20.53 (20.14–20.91) | 23.33 (22.92–23.74) | 20.43 (19.78–21.08) | 26.49 (25.75–27.23) |
| Χ² = 399.964, p = 0.001 | Χ² = 378.297, p = 0.001 | Χ² = 3344.400, p = 0.001 | Χ² = 1178.273, p = 0.001 | ||||||
| N02B | Other analgesics and antipiretics | 16.15 (15.84–16.45) | 20.59 (20.39–20.8) | 15.96 (15.45–16.47) | 22.53 (22.18–22.88) | 15.40 (15.06–15.74) | 16 (15.64–16.35) | 15.08 (14.50–15.66) | 17.67 (17.03–18.31) |
| Χ² = 229.200, p = 0.001 | Χ² = 201.621, p = 0.001 | Χ² = 2612.735, p = 0.001 | Χ² = 939.163, p = 0.001 | ||||||
| N05C | Hypnotics and Sedatives | 17.33 (17.01–17.64) | 17.16 (16.97–17.36) | 18.63 (18.08–19.18) | 19.81 (19.48–20.14) | 16.97 (16.61–17.33) | 14.64 (14.30–14.98) | 18.56 (17.93–19.19) | 18.85 (18.19–19.50) |
| Χ² = 235.223, p = 0.001 | Χ² = 188.963, p = 0.001 | Χ² = 2087.480, p = 0.001 | Χ² = 835.451, p = 0.001 | ||||||
| N03A | Antiepileptics | 19.14 (18.82–19.47) | 16.28 (16.09–16.47) | 24.48 (23.88–25.08) | 20.93 (20.59–21.27) | 20.24 (19.86–20.62) | 17.67 (17.30–18.04) | 26.30 (25.59–27.01) | 25.58 (24.84–26.31) |
| Χ² = 362.380, p = 0.001 | Χ² = 359.500, p = 0.001 | Χ² = 1878.187, p = 0.001 | Χ² = 775.130, p = 0.001 | ||||||
| N05A | Antipsychotics | 20.73 (20.40–21.06) | 15.43 (15.25–15.62) | 29.39 (28.75–30.03) | 20.20 (19.86–20.53) | 20.71 (20.32–21.09) | 13.44 (13.11–13.77) | 30.76 (30.02–31.51) | 20.96 (20.27–21.64) |
| Χ² = 1082.860, p = 0.001 | Χ² = 876.871, p = 0.001 | Χ² = 1435.496, p = 0.001 | Χ² = 610.888, p = 0.001 | ||||||
| Average of Driving Impairing Medicines. Population Antidepressants Use | 2.74 ± 1.14 | 2.76 ± 1.18 | 2.86 ± 1.12 | 2.92 ± 1.23 | 2.73 ± 1.31 | 2.59 ± 1.37 | 2.89 ± 1.35 | 2.88 ± 1.43 | |
| t = −2.951; p = 0.003 | t = −7.255; p = 0.001 | t = 20.608; p = 0.001 | t = 1.150; p = 0.250 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez-Abejón, E.; Herrera-Gómez, F.; Criado-Espegel, P.; Álvarez, F.J. Trends in Antidepressants Use in Spain between 2015 and 2018: Analyses from a Population-Based Registry Study with Reference to Driving. Pharmaceuticals 2020, 13, 61. https://doi.org/10.3390/ph13040061
Gutiérrez-Abejón E, Herrera-Gómez F, Criado-Espegel P, Álvarez FJ. Trends in Antidepressants Use in Spain between 2015 and 2018: Analyses from a Population-Based Registry Study with Reference to Driving. Pharmaceuticals. 2020; 13(4):61. https://doi.org/10.3390/ph13040061
Chicago/Turabian StyleGutiérrez-Abejón, Eduardo, Francisco Herrera-Gómez, Paloma Criado-Espegel, and F. Javier Álvarez. 2020. "Trends in Antidepressants Use in Spain between 2015 and 2018: Analyses from a Population-Based Registry Study with Reference to Driving" Pharmaceuticals 13, no. 4: 61. https://doi.org/10.3390/ph13040061
APA StyleGutiérrez-Abejón, E., Herrera-Gómez, F., Criado-Espegel, P., & Álvarez, F. J. (2020). Trends in Antidepressants Use in Spain between 2015 and 2018: Analyses from a Population-Based Registry Study with Reference to Driving. Pharmaceuticals, 13(4), 61. https://doi.org/10.3390/ph13040061