
Measuring Lower-Limb Kinematics in Walking: Wearable Sensors Achieve Comparable Reliability to Motion Capture Systems and Smartphone Cameras


Abstract
1. Introduction
2. Methodology
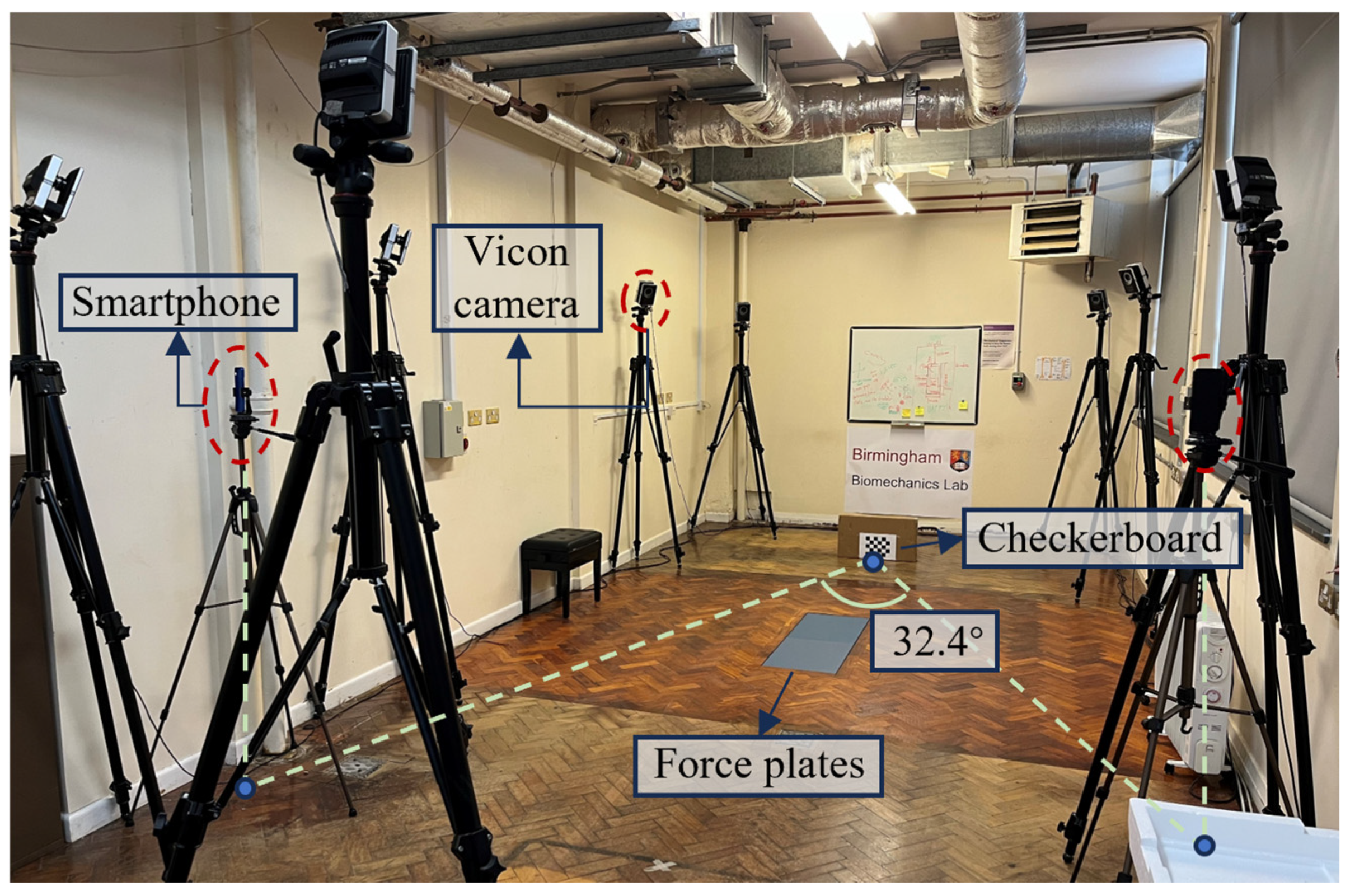
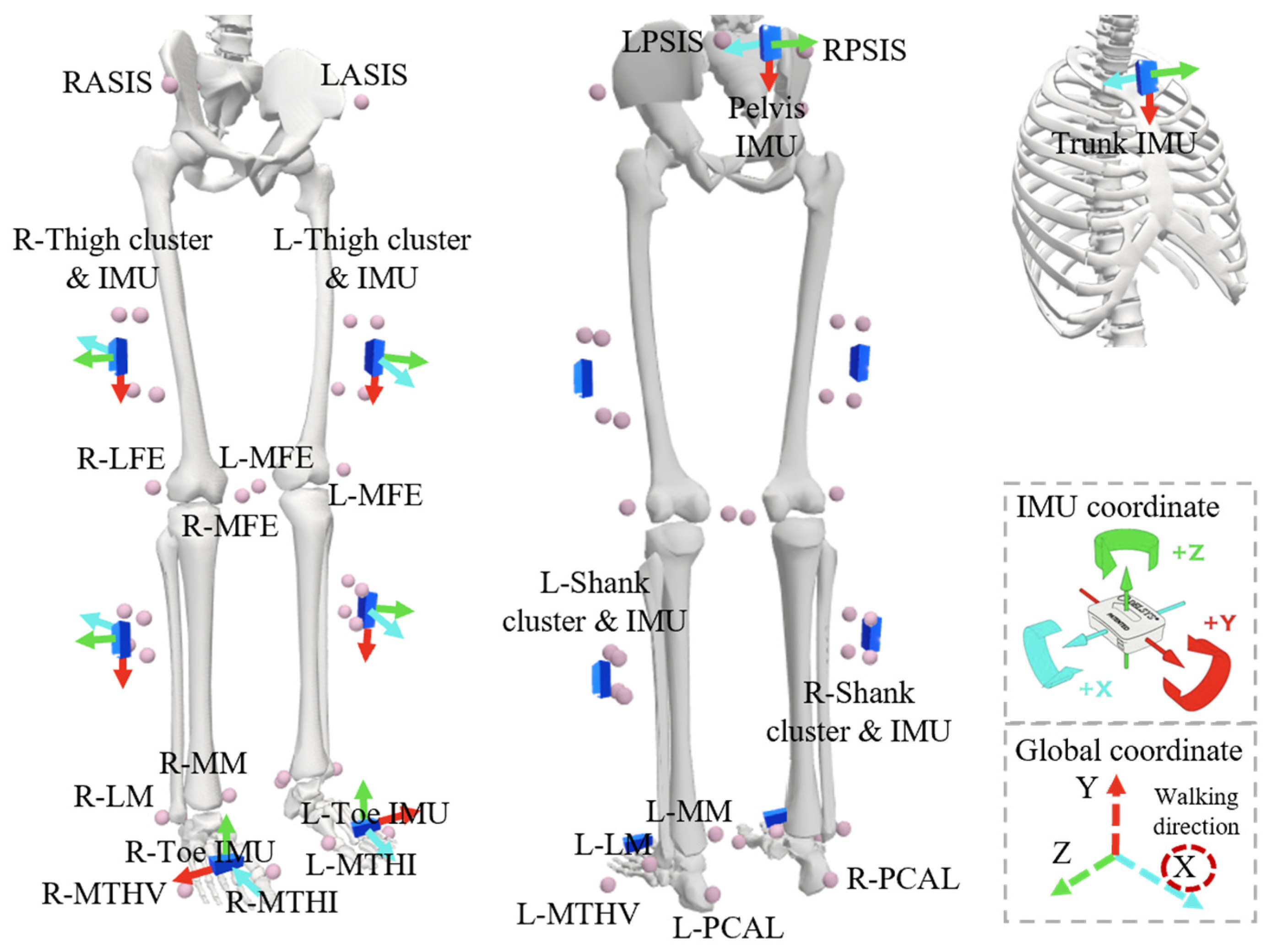
2.1. Experiment Setup
2.2. Data Processing
2.3. Data Analysis
3. Results
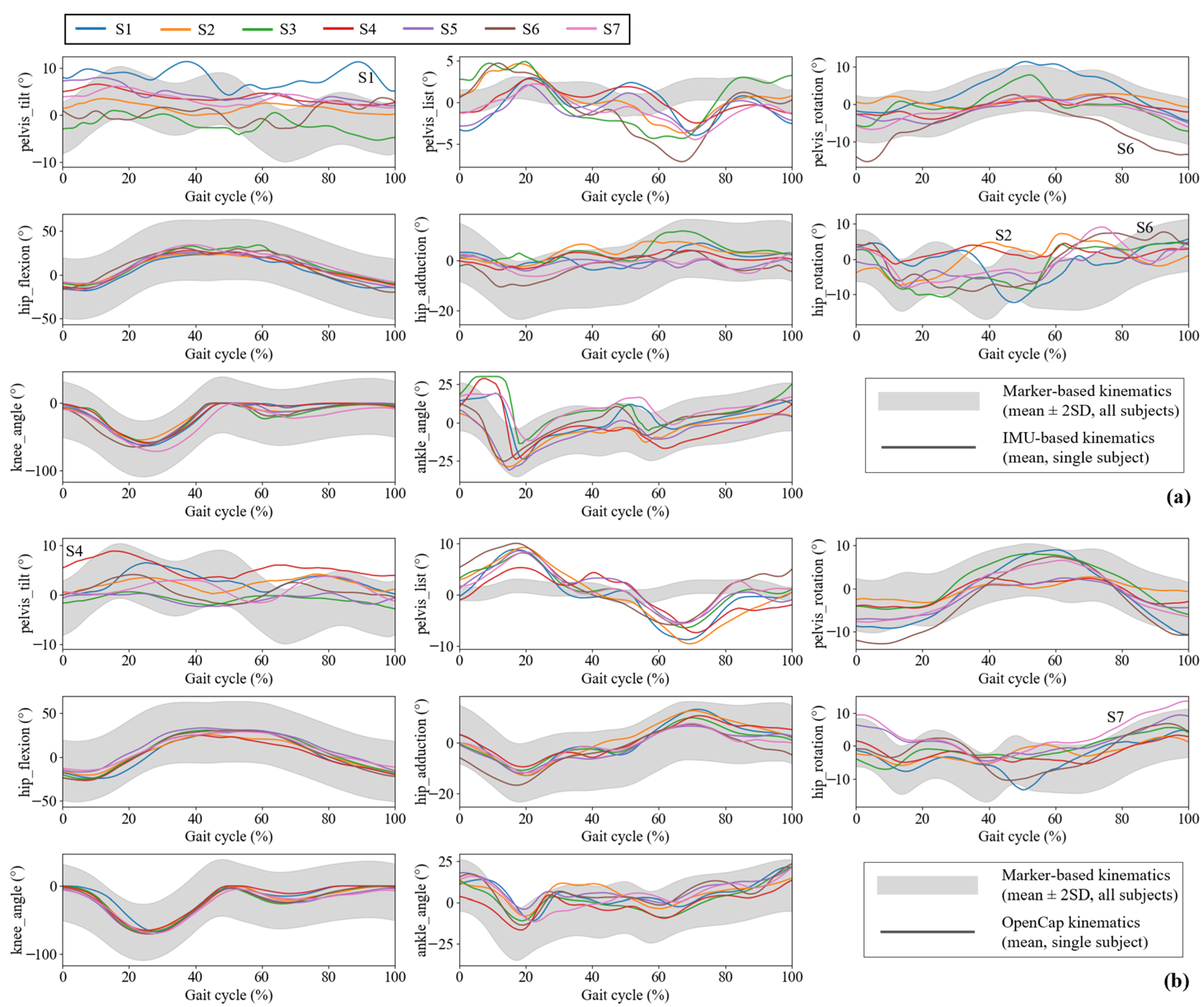
3.1. Accuracy Comparison
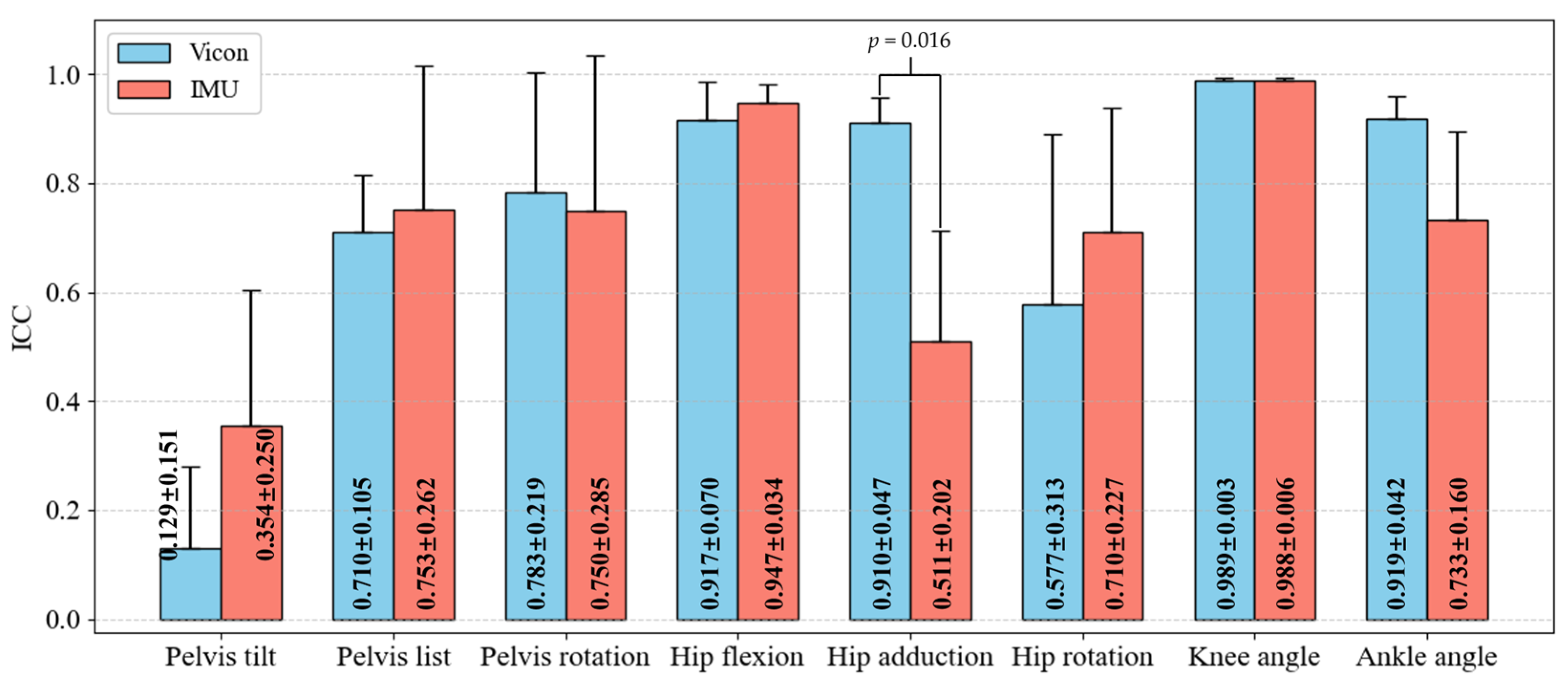
3.2. Inter-Operator Comparison
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yahya, M.; Shah, J.A.; Kadir, K.A.; Yusof, Z.M.; Khan, S.; Warsi, A. Motion capture sensing techniques used in human upper limb motion: A review. Sens. Rev. 2019, 39, 504–511. [Google Scholar] [CrossRef]
- Caicedo, P.E.; Rengifo, C.F.; Rodriguez, L.E.; Sierra, W.A.; Gómez, M.C. Dataset for gait analysis and assessment of fall risk for older adults. Data Brief 2020, 33, 106550. [Google Scholar] [CrossRef]
- Ito, T.; Ota, Y. Comparison of gait analysis between a triaxial accelerometer–based device and an optical motion capture system. Preprints 2020. [Google Scholar]
- Forsyth, L.; Ligeti, A.; Blyth, M.; Clarke, J.; Riches, P. Validity of wearable sensors for total knee arthroplasty (TKA) rehabilitation: A study in younger and older healthy participants. Knee 2024, 51, 292–302. [Google Scholar] [CrossRef]
- Widhalm, K.; Durstberger, S.; Greisberger, A.; Wolf, B.; Putz, P. Validity of assessing level walking with the 2D motion analysis software TEMPLO and reliability of 3D marker application. Sci. Rep. 2024, 14, 1427. [Google Scholar] [CrossRef] [PubMed]
- Asaeda, M.; Kuwahara, W.; Fujita, N.; Yamasaki, T.; Adachi, N. Validity of motion analysis using the Kinect system to evaluate single leg stance in patients with hip disorders. Gait Posture 2018, 62, 458–462. [Google Scholar] [CrossRef]
- Mirek, E.; Rudzińska, M.; Szczudlik, A. The assessment of gait disorders in patients with Parkinson’s disease using the three-dimensional motion analysis system Vicon. Neurol. Neurochir. Pol. 2007, 41, 128–133. [Google Scholar]
- Ida, R.; Kuroyanagi, G.; Ueki, Y.; Murakami, S.; Shiraki, T.; Shimotori, D.; Okamoto, H.; Yamada, K. Total knee arthroplasty improves energy conversion efficiency during walking in patients with knee osteoarthritis. Knee 2025, 53, 42–48. [Google Scholar] [CrossRef]
- Ding, Z.; Güdel, M.; Smith, S.H.L.; Ademefun, R.A.; Bull, A.M.J. A Femoral Clamp to Reduce Soft Tissue Artifact: Accuracy and Reliability in Measuring Three-Dimensional Knee Kinematics During Gait. J. Biomech. Eng. 2020, 142, 044501. [Google Scholar] [CrossRef]
- Zhou, Y.M.; Raman, N.; Proietti, T.; Arnold, J.; Pathak, P.; Pont-Esteban, D.; Nuckols, K.; Rishe, K.; Doshi-Velez, F.; Lin, D.; et al. Estimating Upper Limb Fugl–Meyer Assessment Scores from Reaching Motions Using Wearable Sensors. IEEE J. Biomed. Health Inform. 2025; early access. [Google Scholar]
- Cocco, E.S.; Pournajaf, S.; Romano, P.; Morone, G.; Thouant, C.L.; Buscarini, L.; Manzia, C.M.; Cioeta, M.; Felzani, G.; Infarinato, F.; et al. Comparative analysis of upper body kinematics in stroke, Parkinson’s disease, and healthy subjects: An observational study using IMU–based targeted box and block test. Gait Posture 2024, 114, 69–77. [Google Scholar] [CrossRef]
- Woodman, O.J. An Introduction to Inertial Navigation; Tech. Rep. UCAM-CL-TR-696; University of Cambridge, Computer La-boratory: Cambridge, UK, 2007. [Google Scholar]
- Das, S.S. Simple, inexpensive, accurate calibration of 9 axis Inertial Motion Unit. In Proceedings of the 2019 28th IEEE International Conference on Robot and Human Interactive Communication (RO-MAN), New Delhi, India, 14–18 October 2019; pp. 1–6. [Google Scholar]
- Zhang, Z. Microsoft Kinect Sensor and Its Effect. IEEE Multimed. 2012, 19, 4–10. [Google Scholar] [CrossRef]
- Hadjakos, A. Pianist motion capture with the Kinect depth camera. In Proceedings of the Sound and Music Computing Conference 2012, Copenhagen, Denmark, 11–14 July 2012; pp. 303–310. [Google Scholar]
- Bohannon, R.W.; Harrison, S.; Kinsella-Shaw, J. Reliability and validity of pendulum test measures of spasticity obtained with the Polhemus tracking system from patients with chronic stroke. J. Neuroeng. Rehabil. 2009, 6, 30. [Google Scholar] [CrossRef]
- Park, Y.; Lee, J.; Bae, J. Development of a Wearable Sensing Glove for Measuring the Motion of Fingers Using Linear Potentiometers and Flexible Wires. IEEE Trans. Ind. Inform. 2014, 11, 198–206. [Google Scholar] [CrossRef]
- Bentley, M. Wireless and Visual Hybrid Motion Capture System. U.S. Patent 9,320,957, 26 April 2016. [Google Scholar]
- Uhlrich, S.D.; Falisse, A.; Kidziński, Ł.; Muccini, J.; Ko, M.; Chaudhari, A.S.; Hicks, J.L.; Delp, S.L. OpenCap: Human movement dynamics from smartphone videos. PLoS Comput. Biol. 2023, 19, e1011462. [Google Scholar] [CrossRef] [PubMed]
- Svetek, A.; Morgan, K.; Burland, J.; Glaviano, N.R. Validation of OpenCap on lower extremity kinematics during functional tasks. J. Biomech. 2025, 183, 112602. [Google Scholar] [CrossRef]
- Wang, J.; Xu, W.; Wu, Z.; Zhang, H.; Wang, B.; Zhou, Z.; Wang, C.; Li, K.; Nie, Y. Evaluation of a smartphone-based markerless system to measure lower-limb kinematics in patients with knee osteoarthritis. J. Biomech. 2025, 181, 112529. [Google Scholar] [CrossRef] [PubMed]
- Min, Y.-S.; Jung, T.-D.; Lee, Y.-S.; Kwon, Y.; Kim, H.J.; Kim, H.C.; Lee, J.C.; Park, E. Biomechanical Gait Analysis Using a Smartphone-Based Motion Capture System (OpenCap) in Patients with Neurological Disorders. Bioengineering 2024, 11, 911. [Google Scholar] [CrossRef]
- Nagorna, V.; Mytko, A.; Borysova, O.; Zhyhailova, L.; Achermann, B.; Lorenzetti, S. Biomechanical Analysis: Exploring Gender-Specific Differences in Velocity-Based Strength Training. Sport Sci. Spectr. 2024, 2, 20–26. [Google Scholar] [CrossRef]
- Aminian, K.; Najafi, B. Capturing human motion using body-fixed sensors: Outdoor measurement and clinical applications. Comput. Animat. Virtual Worlds 2004, 15, 79–94. [Google Scholar] [CrossRef]
- Tamir, M.; Oz, G. Real–Time Objects Tracking and Motion Capture in Sports Events. U.S. Patent 20080192116A1, 14 August 2008. [Google Scholar]
- Bregler, C. Motion capture technology for entertainment [in the spotlight]. IEEE Signal Process. Mag. 2007, 24, 156–160. [Google Scholar] [CrossRef]
- Geng, W.; Yu, G. Reuse of motion capture data in animation: A review. In Proceedings of the International Conference on Computational Science and Its Applications, Montreal, Canada, 18–21 May 2003; Springer: Berlin/Heidelberg, Germany; pp. 620–629. [Google Scholar]
- Field, M.; Stirling, D.; Naghdy, F.; Pan, Z. Motion capture in robotics review. In Proceedings of the 2009 IEEE International Conference on Control and Automation, Christchurch, New Zealand, 9–11 December 2009; pp. 1697–1702. [Google Scholar]
- Plantard, P.; Shum, H.P.; Le Pierres, A.-S.; Multon, F. Validation of an ergonomic assessment method using Kinect data in real workplace conditions. Appl. Ergon. 2017, 65, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Valero, E.; Sivanathan, A.; Bosché, F.; Abdel-Wahab, M. Analysis of construction trade worker body motions using a wearable and wireless motion sensor network. Autom. Constr. 2017, 83, 48–55. [Google Scholar] [CrossRef]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Validation of inertial measurement units with an optoelectronic system for whole-body motion analysis. Med. Biol. Eng. Comput. 2017, 55, 609–619. [Google Scholar] [CrossRef]
- Zhang, H.; Song, Y.; Li, C.; Dou, Y.; Wang, D.; Wu, Y.; Chen, X.; Liu, D. Validation of a Wearable System for Lower Extremity Assessment. Orthop. Surg. 2023, 15, 2911–2917. [Google Scholar] [CrossRef] [PubMed]
- Seel, T.; Raisch, J.; Schauer, T. IMU-Based Joint Angle Measurement for Gait Analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef]
- Karatsidis, A.; Jung, M.; Schepers, H.M.; Bellusci, G.; de Zee, M.; Veltink, P.H.; Andersen, M.S. Musculoskeletal model-based inverse dynamic analysis under ambulatory conditions using inertial motion capture. Med. Eng. Phys. 2019, 65, 68–77. [Google Scholar] [CrossRef]
- Bian, Q.; Castellani, M.; Shepherd, D.; Duan, J.; Ding, Z. Gait Intention Prediction Using a Lower-Limb Musculoskeletal Model and Long Short-Term Memory Neural Networks. IEEE Trans. Neural Syst. Rehabil. Eng. 2024, 32, 822–830. [Google Scholar] [CrossRef]
- Di Marco, R.; Rossi, S.; Racic, V.; Cappa, P.; Mazzà, C. Concurrent repeatability and reproducibility analyses of four marker placement protocols for the foot–ankle complex. J. Biomech. 2016, 49, 3168–3176. [Google Scholar] [CrossRef]
- Pataky, T.C. One-dimensional statistical parametric mapping in Python. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 295–301. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Motion Capture Method | Joint Angle MAE (deg) | Joint Torque MAE (%BW×BH) | GRF MAE (%BW) |
|---|---|---|---|
| IMU | 3~7 [31,32,33] | 0.6–1.4 [34] | 12.4% [33] |
| Smartphone cameras [19] | 4.5 | 0.3–1.7 | 1.5–11.1% |
| Joint/Segment | Direction of Movement |
|---|---|
| Pelvis | Tilt |
| List | |
| Rotation | |
| Knee | Flexion |
| Ankle | Flexion |
| Hip | Flexion |
| Adduction | |
| Rotation |
| No. | Age | Height (cm) | Weight (kg) | BMI (kg/m2) |
|---|---|---|---|---|
| 1 | 21 | 161.5 | 79.7 | 30.56 |
| 2 | 38 | 172.0 | 65.4 | 22.11 |
| 3 | 23 | 176.3 | 102.1 | 32.85 |
| 4 | 29 | 170.0 | 51.1 | 17.68 |
| 5 | 22 | 181.8 | 80.1 | 24.24 |
| 6 | 23 | 179.5 | 67.8 | 21.04 |
| 7 | 21 | 176.6 | 79.8 | 25.59 |
| RMSE | r | B | RMSE | r | B | |
| Pelvis Tilt | Pelvis List | |||||
| IMU | 5.49 (2.22) | 0.10 | −5.30, 8.51 | 3.86 (1.52) | 0.08 | −5.12, 4.22 |
| OpenCap | 4.28 (1.47) | 0.26 | −4.13, 6.31 | 5.35 (0.97) | 0.10 | −4.57, 3.81 |
| p-value | 0.013 a | 0.125 | ||||
| Pelvis rotation | Hip flexion | |||||
| IMU | 2.89 (1.75) | 0.85 | −2.17, 5.89 | 5.16 (1.32) | 0.99 | −5.77, 5.02 |
| OpenCap | 2.81 (1.41) | 0.88 | −3.25, 1.37 | 6.16 (2.79) | 0.97 | −7.45, 1.50 |
| p-value | 0.306 | 0.200 | ||||
| Hip adduction | Hip rotation | |||||
| IMU | 6.10 (1.35) | 0.59 | −3.67, 7.52 | 6.09 (1.74) | 0.33 | 0.04, 7.29 |
| OpenCap | 4.06 (0.78) | 0.89 | −3.17, 3.55 | 4.82 (2.30) | 0.73 | −1.57, 8.60 |
| p-value | 0.019 a | 0.009 a | ||||
| Knee angle | Ankle angle | |||||
| IMU | 5.74 (0.80) | 0.99 | 1.94, 5.86 | 7.47 (3.91) | 0.80 | −3.77, 11.23 |
| OpenCap | 7.36 (3.14) | 0.94 | −2.92, 4.66 | 8.20 (3.00) | 0.80 | 1.12, 10.56 |
| p-value | 0.020 a | 0.011 a | ||||
| ICC | ||||||||
|---|---|---|---|---|---|---|---|---|
| Pelvis tilt | Pelvis list | Pelvis rotation | Hip flexion | |||||
| Vicon | IMU | Vicon | IMU | Vicon | IMU | Vicon | IMU | |
| ROM | 0.194 | 0.529 | 0.563 | 0.793 | 0.283 | 0.964 | 0.641 | 0.931 |
| S1 | 0.095 | 0.302 | 0.702 | 0.886 | 0.528 | 0.753 | 0.761 | 0.902 |
| S2 | 0.472 | 0.154 | 0.560 | 0.133 | 0.374 | 0.079 | 0.951 | 0.912 |
| S3 | 0.066 | 0.082 | 0.802 | 0.890 | 0.966 | 0.942 | 0.988 | 0.928 |
| S4 | 0.001 | 0.834 | 0.783 | 0.903 | 0.933 | 0.938 | 0.933 | 0.999 |
| S5 | 0.045 | 0.134 | 0.557 | 0.946 | 0.959 | 0.805 | 0.969 | 0.948 |
| S6 | 0.035 | 0.545 | 0.839 | 0.745 | 0.912 | 0.960 | 0.891 | 0.986 |
| S7 | 0.192 | 0.429 | 0.726 | 0.765 | 0.809 | 0.773 | 0.927 | 0.953 |
| Mean | 0.129 | 0.354 | 0.710 | 0.753 | 0.783 | 0.750 | 0.917 | 0.947 |
| p-value | 0.156 | 0.578 | 0.688 | 0.375 | ||||
| Hip adduction | Hip rotation | Knee angle | Ankle angle | |||||
| Vicon | IMU | Vicon | IMU | Vicon | IMU | Vicon | IMU | |
| ROM | 0.653 | 0.749 | 0.082 | 0.840 | 0.883 | 0.885 | 0.585 | 0.026 |
| S1 | 0.916 | 0.603 | 0.304 | 0.891 | 0.990 | 0.984 | 0.914 | 0.746 |
| S2 | 0.978 | 0.218 | 0.091 | 0.842 | 0.991 | 0.980 | 0.829 | 0.876 |
| S3 | 0.936 | 0.756 | 0.933 | 0.935 | 0.983 | 0.988 | 0.923 | 0.934 |
| S4 | 0.837 | 0.534 | 0.942 | 0.302 | 0.992 | 0.996 | 0.926 | 0.554 |
| S5 | 0.943 | 0.243 | 0.339 | 0.438 | 0.994 | 0.998 | 0.929 | 0.456 |
| S6 | 0.849 | 0.749 | 0.811 | 0.847 | 0.986 | 0.988 | 0.983 | 0.830 |
| S7 | 0.914 | 0.473 | 0.619 | 0.718 | 0.989 | 0.987 | 0.926 | 0.736 |
| Mean | 0.910 | 0.511 | 0.577 | 0.710 | 0.989 | 0.988 | 0.919 | 0.733 |
| p-value | 0.016 a | 0.203 | 0.984 | 0.078 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, P.; Bian, Q.; Kim, J.M.; Alsayed, K.; Ding, Z. Measuring Lower-Limb Kinematics in Walking: Wearable Sensors Achieve Comparable Reliability to Motion Capture Systems and Smartphone Cameras. Sensors 2025, 25, 2899. https://doi.org/10.3390/s25092899
Ma P, Bian Q, Kim JM, Alsayed K, Ding Z. Measuring Lower-Limb Kinematics in Walking: Wearable Sensors Achieve Comparable Reliability to Motion Capture Systems and Smartphone Cameras. Sensors. 2025; 25(9):2899. https://doi.org/10.3390/s25092899
Chicago/Turabian StyleMa, Peiyu, Qingyao Bian, Jin Min Kim, Khalid Alsayed, and Ziyun Ding. 2025. "Measuring Lower-Limb Kinematics in Walking: Wearable Sensors Achieve Comparable Reliability to Motion Capture Systems and Smartphone Cameras" Sensors 25, no. 9: 2899. https://doi.org/10.3390/s25092899
APA StyleMa, P., Bian, Q., Kim, J. M., Alsayed, K., & Ding, Z. (2025). Measuring Lower-Limb Kinematics in Walking: Wearable Sensors Achieve Comparable Reliability to Motion Capture Systems and Smartphone Cameras. Sensors, 25(9), 2899. https://doi.org/10.3390/s25092899