

Challenging Behaviors in Children with Nonverbal Autism: A Questionnaire to Guide the Design of a Wearable Device for Biomarker Recording

 , , ,
, , ,
Abstract
Highlights
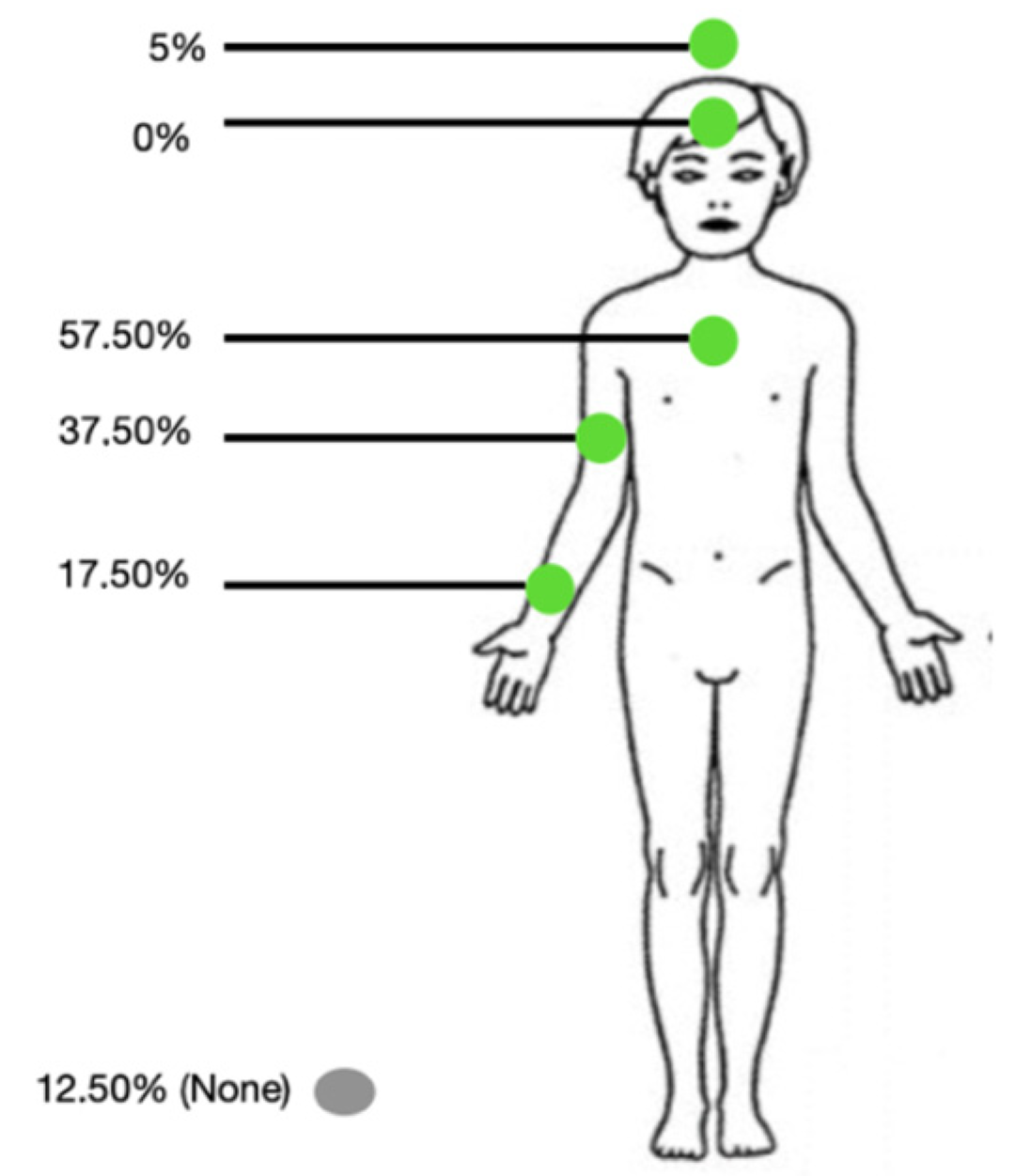
- A total of 67.5% of respondents support a wearable stress detection device for nmvASD children, preferably integrated into clothing, placed on the trunk, and be wireless.
- These findings guide the development of tailored tools to improve behavioral management in this population.
Abstract
1. Introduction
1.1. Sensory Particularities
1.2. Behavioral Issues
1.3. Stress Biomarkers
1.4. Wearable Devices for Children with ASD
2. Materials and Methods
3. Results
3.1. Population
3.2. Sensitivity

{kind=link}
| Type of Contact | Location | Always | Often | Sometimes | Rarely | Not at all | N/A * |
|---|---|---|---|---|---|---|---|
| Light brief touch (like a stroke) | Trunk | 50% | 20% | 20% | 7.5% | 0% | 2.5% |
| Arm | 27.5% | 35% | 27.5% | 7.5% | 0% | 2.5% | |
| Wrist | 42.5% | 27.5% | 20% | 7.5% | 2.5% | 0% | |
| Head | 37.5% | 22.5% | 27.5% | 10% | 2.5% | 0% | |
| Forehead | 37.5% | 30% | 17.5% | 7.5% | 5% | 2.5% | |
| Light sustained touch (like giving a hug) | Trunk | 25% | 30% | 32.5% | 7.5% | 2.5% | 2.5% |
| Arm | 22.5% | 15% | 20% | 22.5% | 10% | 10% | |
| Wrist | 32.5% | 25% | 27.5% | 10% | 0% | 5% | |
| Head | 32.5% | 15% | 35% | 10% | 5% | 2.5% | |
| Forehead | 25% | 25% | 25% | 10% | 5% | 10% | |
| Pressure touch (like putting a plaster) | Trunk | 17.5% | 15% | 15% | 25% | 7.5% | 20% |
| Arm | 22.5% | 15% | 20% | 22.5% | 10% | 10% | |
| Wrist | 20% | 15% | 20% | 15% | 17.5% | 12.5% | |
| Head | 17.5% | 5% | 25% | 17.5% | 22.5% | 12.5% | |
| Forehead | 10% | 12.5% | 20% | 25% | 17.5% | 15% | |
| Light sustained touch with an object (like clothing friction) | Trunk | 70% | 20% | 2.5% | 2.5% | 5% | 0% |
| Arm | 60% | 22.5% | 10% | 2.5% | 2.5% | 2.5% | |
| Wrist | 57.5% | 20% | 10% | 2.5% | 2.5% | 2.5% | |
| Head | 37.5% | 17.5% | 15% | 22.5% | 22.5% | 0% | |
| Forehead | 42.5% | 20% | 5% | 17.5% | 17.5% | 2.5% | |
| Moving contact (like applying a cream) | Trunk | 30% | 27.5% | 20% | 10% | 5% | 7.5% |
| Arm | 37.5% | 25% | 15% | 10% | 5% | 7.5% | |
| Wrist | 27.5% | 30% | 20% | 10% | 5% | 7.5% | |
| Head | 22.5% | 20% | 22.5% | 17.5% | 10% | 7.5% | |
| Forehead | 25% | 22.5% | 17.5% | 20% | 7.5% | 7.5 | |
| Contact with a liquid substance (water) | Trunk | 80% | 7.5% | 7.5% | 2.5% | 0% | 2.5% |
| Arm | 77.5% | 15% | 7.5% | 0% | 0% | 0% | |
| Wrist | 80% | 12.5% | 7.5% | 0% | 0% | 0% | |
| Head | 57.5% | 17.5% | 7.5% | 12.5% | 5% | 0% | |
| Forehead | 62.5% | 17.5% | 10% | 7.5% | 2.5% | 0% |
3.3. Emotions
3.4. Wereable Device
3.5. Technical Parameters
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASD | Autism Spectrum Disorder |
| nmvASD | Non or Minimally Verbal Autism |
| ABA | Applied Behavior Analysis |
| PECS | Picture Exchange Communication System |
| EIBI | Early Intensive Behavioral Intervention |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders |
| HR | Heart Rate |
| HRV | Heart Rate Variation |
| GSR | Galvanic Skin Response |
| EDA | Electrodermal Activity |
| EEG | Electroencephalogram |
| ECG | Electrocardiogram |
Appendix A. Inclusion Criteria
| Inclusion Criteria |
| ASD diagnosed by an expert in child psychiatry Aged 3 years to 17 years 11 months |
| Severe language impairment: non or minimally verbal |
References
- American Psychiatric Association (Ed.) Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Text Revision; American Psychiatric Publishing: Washington, DC, USA, 2022. [Google Scholar]
- Kim, Y.S.; Leventhal, B.L.; Koh, Y.-J.; Fombonne, E.; Laska, E.; Lim, E.-C.; Cheon, K.-A.; Kim, S.-J.; Kim, Y.-K.; Lee, H.; et al. Prevalence of Autism Spectrum Disorders in a Total Population Sample. Am. J. Psychiatry 2011, 168, 904–912. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, J.; Fombonne, E.; Scorah, J.; Ibrahim, A.; Durkin, M.S.; Saxena, S.; Yusuf, A.; Shih, A.; Elsabbagh, M. Global Prevalence of Autism: A Systematic Review Update. Autism Res. 2022, 15, 778–790. [Google Scholar] [PubMed]
- Fombonne, E. Editorial: Is Autism Overdiagnosed? J. Child Psychol. Psychiatry 2023, 64, 711–714. [Google Scholar]
- Lundström, S.; Taylor, M.; Larsson, H.; Lichtenstein, P.; Kuja-Halkola, R.; Gillberg, C. Perceived Child Impairment and the ‘Autism Epidemic’. J. Child Psychol. Psychiatry 2021, 63, 591–598. [Google Scholar]
- Taylor, M.J.; Rosenqvist, M.A.; Larsson, H.; Gillberg, C.; D’Onofrio, B.M.; Lichtenstein, P.; Lundström, S. Etiology of Autism Spectrum Disorders and Autistic Traits Over Time. JAMA Psychiatry 2020, 77, 936–943. [Google Scholar]
- Arnold, S.; Reed, P. Reading Assessments for Students with ASD: A Survey of Summative Reading Assessments Used in Special Educational Schools in the UK. Br. J. Spec. Educ. 2016, 43, 122–141. [Google Scholar]
- Cole, P.M.; Michel, M.K.; Teti, L.O. The Development of Emotion Regulation and Dysregulation: A Clinical Perspective. Monogr. Soc. Res. Child Dev. 1994, 59, 73–100. [Google Scholar]
- Case-Smith, J.; Weaver, L.L.; Fristad, M.A. A Systematic Review of Sensory Processing Interventions for Children with Autism Spectrum Disorders. Autism 2014, 19, 133–148. [Google Scholar]
- Robertson, C.E.; Baron-Cohen, S. Sensory Perception in Autism. Nat. Rev. Neurosci. 2017, 18, 671–684. [Google Scholar] [CrossRef]
- Matson, J.L.; Kozlowski, A.M. The Increasing Prevalence of Autism Spectrum Disorders. Res. Autism Spectr. Disord. 2010, 5, 418–425. [Google Scholar]
- Jang, J.; Dixon, D.R.; Tarbox, J.; Granpeesheh, D. Symptom Severity and Challenging Behavior in Children with ASD. Res. Autism Spectr. Disord. 2010, 5, 1028–1032. [Google Scholar] [CrossRef]
- Huebner, R. Autism: A Sensorimotor Approach to Management; Aspen Publisher: New York, NY, USA, 2001. [Google Scholar]
- Koegel, R.L.; Koegel, L.K.; Surratt, A. Language Intervention and Disruptive Behavior in Preschool Children with Autism. J. Autism Dev. Disord. 1992, 22, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Ben-Sasson, A.; Hen, L.; Fluss, R.; Cermak, S.A.; Engel-Yeger, B.; Gal, E. A Meta-Analysis of Sensory Modulation Symptoms in Individuals with Autism Spectrum Disorders. J. Autism Dev. Disord. 2008, 39, 1–11. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, A.; McCreadie, M.; Mills, R.; Deveau, R.; Anker, R.; Hayden, J. The Role of Physiological Arousal in the Management of Challenging Behaviours in Individuals with Autistic Spectrum Disorders. Res. Dev. Disabil. 2014, 36, 311–322. [Google Scholar] [CrossRef]
- Loveland, K.A. Social-Emotional Impairment and Self-Regulation in Autism Spectrum Disorders. In Emotional Development: Recent Research Advances; eBooks; Oxford University Press: Oxford, UK, 2004; pp. 365–382. [Google Scholar]
- Groden, J.; Cautela, J.; Prince, S.; Berryman, J. The Impact of Stress and Anxiety on Individuals with Autism and Developmental Disabilities. In Behavioral Issues in Autism; eBooks; Springer: Berlin/Heidelberg, Germany, 1994; pp. 177–194. [Google Scholar]
- Whitman, T.L. The Development of Autism A Self-Regulatory Perspective; Jessica Kingsley Publishers: New York, NY, USA, 2004. [Google Scholar]
- Kanne, S.M.; Mazurek, M.O. Aggression in Children and Adolescents with ASD: Prevalence and Risk Factors. J. Autism Dev. Disord. 2010, 41, 926–937. [Google Scholar] [CrossRef]
- Siegel, M.; Gabriels, R.L. Psychiatric Hospital Treatment of Children with Autism and Serious Behavioral Disturbance. Child Adolesc. Psychiatr. Clin. North Am. 2013, 23, 125–142. [Google Scholar] [CrossRef]
- Weiss, J.A.; Cappadocia, M.C.; MacMullin, J.A.; Viecili, M.; Lunsky, Y. The Impact of Child Problem Behaviors of Children with ASD on Parent Mental Health: The Mediating Role of Acceptance and Empowerment. Autism 2012, 16, 261–274. [Google Scholar] [CrossRef]
- Gregori, E.; Wendt, O.; Gerow, S.; Peltier, C.; Genc-Tosun, D.; Lory, C.; Gold, Z.S. Functional Communication Training for Adults with Autism Spectrum Disorder: A Systematic Review and Quality Appraisal. J. Behav. Educ. 2019, 29, 42–63. [Google Scholar] [CrossRef]
- Bourgeois, M.; Sénéchal, C.; Larivée, S.; Lepore, F. Effets des programmes d’interventions cognitivo-comportementaux et d’entraînements cognitifs sur les fonctions exécutives (FE) chez les personnes atteintes du trouble du spectre autistique (TSA): Revue systématique. Ann. Médico-Psychol. Rev. Psychiatr. 2019, 177, 749–757. [Google Scholar] [CrossRef]
- Roane, H.S.; Fisher, W.W.; Carr, J.E. Applied Behavior Analysis as Treatment for Autism Spectrum Disorder. J. Pediatr. 2016, 175, 27–32. [Google Scholar] [CrossRef]
- O’Nions, E.; Happé, F.; Evers, K.; Boonen, H.; Noens, I. How Do Parents Manage Irritability, Challenging Behaviour, Non-Compliance and Anxiety in Children with Autism Spectrum Disorders? A Meta-Synthesis. J. Autism Dev. Disord. 2017, 48, 1272–1286. [Google Scholar]
- Goodwin, M.S.; Özdenizci, O.; Cumpanasoiu, C.; Tian, P.; Guo, Y.; Stedman, A.; Peura, C.; Mazefsky, C.; Siegel, M.; Erdoğmuş, D.; et al. Predicting Imminent Aggression Onset in Minimally-Verbal Youth with Autism Spectrum Disorder Using Preceding Physiological Signals. In Proceedings of the 12th EAI International Conference on Pervasive Computing Technologies for Healthcare, New York, NY, USA, 21–24 May 2018; Volume 201, pp. 201–207. [Google Scholar]
- Wink, L.K.; Pedapati, E.V.; Horn, P.S.; McDougle, C.J.; Erickson, C.A. Multiple Antipsychotic Medication Use in Autism Spectrum Disorder. J. Child Adolesc. Psychopharmacol. 2015, 27, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Shafiq, S.; Pringsheim, T. Using Antipsychotics for Behavioral Problems in Children. Expert Opin. Pharmacother. 2018, 19, 1475–1488. [Google Scholar]
- Horner, R.H.; Carr, E.G.; Strain, P.S.; Todd, A.W.; Reed, H.K. Problem Behavior Interventions for Young Children with Autism: A Research Synthesis. J. Autism Dev. Disord. 2002, 32, 423–446. [Google Scholar]
- Nuske, H.J.; Finkel, E.; Hedley, D.; Parma, V.; Tomczuk, L.; Pellecchia, M.; Herrington, J.; Marcus, S.C.; Mandell, D.S.; Dissanayake, C. Heart Rate Increase Predicts Challenging Behavior Episodes in Preschoolers with Autism. Stress 2019, 22, 303–311. [Google Scholar]
- Xiao, H.; Liu, T.; Sun, Y.; Li, Y.; Zhao, S.; Avolio, A. Remote photoplethysmography for heart rate measurement: A review. Biomed. Signal Process. Control 2024, 88 Pt B, 105608. [Google Scholar] [CrossRef]
- Ferguson, B.J.; Hamlin, T.; Lantz, J.F.; Villavicencio, T.; Coles, J.; Beversdorf, D.Q. Examining the Association Between Electrodermal Activity and Problem Behavior in Severe Autism Spectrum Disorder: A Feasibility Study. Front. Psychiatry 2019, 10, 654. [Google Scholar] [CrossRef]
- Goumopoulos, C.; Menti, E. Stress Detection in Seniors Using Biosensors and Psychometric Tests. Procedia Comput. Sci. 2019, 152, 18–27. [Google Scholar]
- Bakker, J.; Pechenizkiy, M.; Sidorova, N. What’s Your Current Stress Level? Detection of Stress Patterns from GSR Sensor Data. In Proceedings of the 2011 IEEE 11th International Conference on Data Mining Workshops, Vancouver, BC, Canada, 11 December 2011; IEEE: Piscataway, NJ, USA, 2011; pp. 573–580. [Google Scholar]
- Tansey, E.A.; Johnson, C.D. Recent Advances in Thermoregulation. AJP Advances In Physiology. Education 2015, 39, 139–148. [Google Scholar]
- M ohamed, Y.; Ballardini, G.; Parreira, M.T.; Lemaignan, S.; Leite, I. Automatic Frustration Detection Using Thermal Imaging. In Proceedings of the 17th ACM/IEEE International Conference on Human-Robot Interaction (HRI), Sapporo, Japan, 7–10 March 2022; pp. 451–459. [Google Scholar] [CrossRef]
- Yu, B.; Funk, M.; Hu, J.; Wang, Q.; Feijs, L. Biofeedback for Everyday Stress Management: A Systematic Review. Front. ICT 2018, 5, 23. [Google Scholar] [CrossRef]
- Huysmans, D.; Smets, E.; De Raedt, W.; Van Hoof, C.; Bogaerts, K.; Van Diest, I.; Helic, D. Unsupervised Learning for Mental Stress Detection. In Proceedings of the 15th International Joint Conference on Biomedical Engineering Systems and Technologies, Funchal, Portugal, 19–21 January 2018; Volume 2635. [Google Scholar]
- Hosseini, S.A.; Khalilzadeh, M.A. Emotional Stress Recognition System Using EEG and Psychophysiological Signals: Using New Labelling Process of EEG Signals in Emotional Stress State. In Proceedings of the International Conference on Biomedical Engineering and Computer Science, Wuhan, China, 23–25 April 2010; Volume 16. [Google Scholar]
- Dimberg, U. Facial Reactions to Facial Expressions. Psychophysiology 1982, 19, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, D.A.; Hoskyn, M.; Birmingham, E. Facial Expression Production in Autism: A Meta-Analysis. Autism Res. 2018, 11, 1586–1601. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.R.; Roberts, J.E.; Baranek, G.T.; Mandulak, K.C.; Dalton, J.C. Behavioral and Physiological Responses to Child-Directed Speech of Children with Autism Spectrum Disorders or Typical Development. J. Autism Dev. Disord. 2011, 42, 1616–1629. [Google Scholar]
- Van Hecke, A.V.; Lebow, J.; Bal, E.; Lamb, D.; Harden, E.; Kramer, A.; Denver, J.; Bazhenova, O.; Porges, S.W. Electroencephalogram and Heart Rate Regulation to Familiar and Unfamiliar People in Children With Autism Spectrum Disorders. Child Dev. 2009, 80, 1118–1133. [Google Scholar] [CrossRef]
- Neuhaus, E.; Bernier, R.; Beauchaine, T.P. Brief Report: Social Skills, Internalizing and Externalizing Symptoms, and Respiratory Sinus Arrhythmia in Autism. J. Autism Dev. Disord. 2013, 44, 730–737. [Google Scholar]
- Edmiston, E.K.; Jones, R.M.; Corbett, B.A. Physiological Response to Social Evaluative Threat in Adolescents with Autism Spectrum Disorder. J. Autism Dev. Disord. 2016, 46, 2992–3005. [Google Scholar] [CrossRef]
- Lory, C.; Kadlaskar, G.; Keehn, R.M.; Francis, A.L.; Keehn, B. Brief Report: Reduced Heart Rate Variability in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2020, 50, 4183–4190. [Google Scholar]
- Ming, X.; Julu, P.O.O.; Brimacombe, M.; Connor, S.; Daniels, M.L. Reduced Cardiac Parasympathetic Activity in Children with Autism. Brain Dev. 2005, 27, 509–516. [Google Scholar] [CrossRef]
- Kushki, A.; Brian, J.; Dupuis, A.; Anagnostou, E. Functional Autonomic Nervous System Profile in Children with Autism Spectrum Disorder. Mol. Autism 2014, 5, 39. [Google Scholar]
- Bujnakova, I.; Ondrejka, I.; Mestanik, M.; Visnovcova, Z.; Mestanikova, A.; Hrtanek, I.; Fleskova, D.; Calkovska, A.; Tonhajzerova, I. Autism Spectrum Disorder Is Associated with Autonomic Underarousal. Physiol. Res. 2016, 65, S673–S682. [Google Scholar] [CrossRef]
- Chiu, T.A.; Anagnostou, E.; Brian, J.; Chau, T.; Kushki, A. Specificity of Autonomic Arousal to Anxiety in Children with Autism Spectrum Disorder. Autism Res. 2015, 9, 491–501. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, M.S.; Mazefsky, C.A.; Ioannidis, S.; Erdogmus, D.; Siegel, M. Predicting Aggression to Others in Youth with Autism Using a Wearable Biosensor. Autism Res. 2019, 12, 1286–1296. [Google Scholar] [CrossRef] [PubMed]
- Taj-Eldin, M.; Ryan, C.; O’Flynn, B.; Galvin, P. A Review of Wearable Solutions for Physiological and Emotional Monitoring for Use by People with Autism Spectrum Disorder and Their Caregivers. Sensors 2018, 18, 4271. [Google Scholar] [CrossRef]
- Black, M.H.; Milbourn, B.; Chen, N.T.M.; McGarry, S.; Wali, F.; Ho, A.S.V.; Lee, M.; Bölte, S.; Falkmer, T.; Girdler, S. The Use of Wearable Technology to Measure and Support Abilities, Disabilities and Functional Skills in Autistic Youth: A Scoping Review. Scand. J. Child Adolesc. Psychiatry Psychol. 2020, 8, 48–69. [Google Scholar] [CrossRef]
- Cabibihan, J.-J.; Javed, H.; Aldosari, M.; Frazier, T.; Elbashir, H. Sensing Technologies for Autism Spectrum Disorder Screening and Intervention. Sensors 2016, 17, 46. [Google Scholar] [CrossRef]
- Kasari, C.; Brady, N.; Lord, C.; Tager-Flusberg, H. Assessing the Minimally Verbal School-Aged Child With Autism Spectrum Disorder. Autism Res. 2013, 6, 479–493. [Google Scholar] [CrossRef]
- Li, J.; Wang, P.; Barakova, E.; Hu, J. Embodied Technologies for Stress Management in Children: A Systematic Review. In Proceedings of the 2023 32nd IEEE International Conference on Robot and Human Interactive Communication (RO-MAN), Busan, Republic of Korea, 28–31 August 2023; IEEE: Piscataway, NJ, USA, 2023; pp. 1420–1427. [Google Scholar]
- Cano, S.; Cubillos, C.; Alfaro, R.; Romo, A.; García, M.; Moreira, F. Wearable Solutions Using Physiological Signals for Stress Monitoring on Individuals with Autism Spectrum Disorder (ASD): A Systematic Literature Review. Sensors 2024, 24, 8137. [Google Scholar] [CrossRef]
- Mistry, K.; Dafoulas, G. IoT Wearables in Child Health: A Comprehensive Scoping Review and Exploration of Ubiquitous Computing. Internet Things 2025, 31, 101556. [Google Scholar] [CrossRef]
- Cantin-Garside, K.D.; Nussbaum, M.A.; White, S.W.; Kim, S.; Kim, C.D.; Fortes, D.M.G.; Valdez, R.S. Understanding the Experiences of Self-Injurious Behavior in Autism Spectrum Disorder: Implications for Monitoring Technology Design. J. Am. Med. Inform. Assoc. 2020, 28, 303–310. [Google Scholar] [CrossRef]
- Witteman, H.O.; Vaisson, G.; Provencher, T.; Dansokho, S.C.; Colquhoun, H.; Dugas, M.; Fagerlin, A.; Giguere, A.M.; Haslett, L.; Hoffman, A.; et al. An 11-Item Measure of User- and Human-Centered Design for Personal Health Tools (UCD-11): Development and Validation. J. Med. Internet Res. 2021, 23, e15032. [Google Scholar] [CrossRef]
- Luijcks, R.; Hermens, H.J.; Bodar, L.; Vossen, C.J.; Van Os, J.; Lousberg, R. Experimentally Induced Stress Validated by EMG Activity. PLoS ONE 2014, 9, e95215. [Google Scholar] [CrossRef] [PubMed]
- Jena, S. Examination Stress and Its Effect on EEG. Int. J. Med. Sci. Public Health 2015, 4, 1493. [Google Scholar]
- Koo, S.H.; Gaul, K.; Rivera, S.; Pan, T.; Fong, D. Wearable Technology Design for Autism Spectrum Disorders. Arch. Des. Res. 2018, 31, 37–55. [Google Scholar]
- Nawrocki, R.A. Super- and Ultrathin Organic Field-Effect Transistors: From Flexibility to Super- and Ultraflexibility. Adv. Funct. Mater. 2019, 29, 1906908. [Google Scholar]
- Ferrari, L.M.; Sudha, S.; Tarantino, S.; Esposti, R.; Bolzoni, F.; Cavallari, P.; Cipriani, C.; Mattoli, V.; Greco, F. Ultraconformable Temporary Tattoo Electrodes for Electrophysiology. Adv. Sci. 2018, 5, 1700771. [Google Scholar]
- Galliani, M.; Ferrari, L.M.; Ismailova, E. Conformable Wearable Electrodes: From Fabrication to Electrophysiological Assessment. J. Vis. Exp. 2022, 185, e63204. [Google Scholar] [CrossRef]
- Zwilling, M.; Romano, A.; Hoffman, H.; Lotan, M.; Tesler, R. Development and Validation of a System for the Prediction of Challenging Behaviors of People with Autism Spectrum Disorder Based on a Smart Wearable Shirt: A Mixed-Methods Design. Front. Behav. Neurosci. 2022, 16, 948184. [Google Scholar]
- Pergantis, P.; Drigas, A. Assistive Technology for Autism Spectrum Disorder Children That Experiences Stress and Anxiety. Braz. J. Sci. 2023, 2, 77–93. [Google Scholar] [CrossRef]
- Beniwal, A.; Khandelwal, G.; Mukherjee, R.; Mulvihill, D.M.; Li, C. Eco-Friendly Textile-Based Wearable Humidity Sensor with Multinode Wireless Connectivity for Healthcare Applications. ACS Appl. Bio Mater. 2024, 7, 4772–4784. [Google Scholar]
- Vidhya, C.M.; Maithani, Y.; Singh, J.P. Recent Advances and Challenges in Textile Electrodes for Wearable Biopotential Signal Monitoring: A Comprehensive Review. Biosensors 2023, 13, 679. [Google Scholar] [CrossRef]
- Takamatsu, S.; Lonjaret, T.; Crisp, D.; Badier, J.-M.; Malliaras, G.G.; Ismailova, E. Direct Patterning of Organic Conductors on Knitted Textiles for Long-Term Electrocardiography. Sci. Rep. 2015, 5, 15003. [Google Scholar]
- Mshali, H.; Lemlouma, T.; Moloney, M.; Magoni, D. A Survey on Health Monitoring Systems for Health Smart Homes. Int. J. Ind. Ergon. 2018, 66, 26–56. [Google Scholar]
- Jeong, J.-W.; Lee, W.; Kim, Y.-J. A Real-Time Wearable Physiological Monitoring System for Home-Based Healthcare Applications. Sensors 2021, 22, 104. [Google Scholar] [CrossRef]
- Puli, A.; Kushki, A. Toward Automatic Anxiety Detection in Autism: A Real-Time Algorithm for Detecting Physiological Arousal in the Presence of Motion. IEEE Trans. Biomed. Eng. 2019, 67, 646–657. [Google Scholar] [PubMed]
- Chaptoukaev, H.; Strizhkova, V.; Panariello, M.; D’alpaos, B.; Reka, A.; Manera, V.; Thümmler, S.; Ismailova, E.; Evans, N.; Bremond, F.F.; et al. StressID: A Multimodal Dataset for Stress Identification. In Proceedings of the Advances In Neural Information Processing Systems 36 (NeurIPS 2023) Datasets And Benchmarks Track, New Orleans, LA, USA, 10–16 December 2023. [Google Scholar]
| Section | Theme | Question | Question Style |
|---|---|---|---|
| 1. General Information | Relationship with child | N/A | Multiple choice |
| Child Characteristics | Age Sex Severity of disorder Level of verbal communication Frequency of challenging behavior | Open-ended Binary Multiple choice Binary Multiple choice | |
| 2. Sensitivity | Assessment of acceptance of various contacts based on each location | Light, brief touch Light, sustained touch Pressure touch Light, sustained contact with object Moving contact Contact with a liquid substance | Likert scales * |
| Previous experience and acceptation | Bracelet, watch Connected watch ECG, EEG Temporary tattoo Wires | Binary and Likert scales * | |
| 3. Emotions | Capacity of recognition | Happiness Pain Intensity of pain Sickness Stress/anxiety Cause of anxiety | Likert scales * |
| Characteristics Challenging behavior Communication of emotions | Hypo/hypersensitivity Capacity to anticipate Used a technologic/non technologic method and utility | Binary and Likert scales * | |
| 4. Device presentation | Picture and information about the device |  | N/A |
| Potential utility and tolerability according to the respondent | Utility in general Acceptation and tolerability Utility at home/hospital/caring unit Utility all day | Likert scales * | |
| 5. Technical parameters | Advice for conception | Location Wires Sensors Colors T-shirt integration Suggestions | Multiple choice Likert scales * Likert scales * Multiple choice Likert scales * Open comment |
| Study Population | N = 40 | % of Total | |
|---|---|---|---|
| Gender | Male | 29 | 72.5% |
| Female | 11 | 27.5% | |
| ASD Severity | Mild | 2 | 5% |
| Moderate | 9 | 22.5% | |
| Severe | 26 | 65% | |
| N/A * | 3 | 7.5% | |
| Verbal Communication Skills ** | Nonverbal | 20 | 50% |
| Minimal verbal | 20 | 50% | |
| Challenging Behaviors *** | Never or rarely | 7 | 17.5% |
| 1 time or more each day | 15 | 37.5% | |
| 15 times or more each day | 11 | 27.5% | |
| 30 times or more each day | 7 | 17.5% |
| Item | Always | Often | Sometimes | Rarely | Not at all | N/A * |
|---|---|---|---|---|---|---|
| Can you clearly determine when the child is happy? | 45% | 40% | 12.5% | 0% | 2.5% | 0% |
| Can you recognize when the child is in pain? | 10% | 30% | 47.5% | 10% | 2.5% | 0% |
| Can you assess the intensity of the pain the child is experiencing? | 5% | 7.5% | 25% | 25% | 37.5% | 0% |
| Can you recognize when the child is ill? | 17.5% | 30% | 47.5% | 5% | 0% | 0% |
| Can you recognize when the child is anxious/nervous? | 25% | 40% | 27.5% | 2.5% | 5% | 0% |
| Can you identify what causes the child’s anxiety? | 0% | 27.5% | 32.5% | 17.5% | 20% | 2.5% |
| Can you anticipate the emergence of inappropriate behaviors in the child, such as aggression? | 7.5% | 35% | 35% | 5% | 15% | 2.5% |
| Do you know if the child has hyposensitivity? | 17.5% | 17.5% | 25% | 5% | 30% | 5% |
| Do you know if the child has hypersensitivity? | 10% | 25% | 12.5% | 15% | 32.5% | 5% |
| For children who have used non-technological means to communicate their emotions, was it helpful for them? | 9.09% | 45.45% | 18.18% | 18.18% | 9.09% | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weber, A.-S.; Barbini, C.; Vidal, O.; Ferrari, L.M.; Thellier, D.; Derreumaux, A.; Ismailova, E.; Askenazy, F.; Thümmler, S. Challenging Behaviors in Children with Nonverbal Autism: A Questionnaire to Guide the Design of a Wearable Device for Biomarker Recording. Sensors 2025, 25, 2009. https://doi.org/10.3390/s25072009
Weber A-S, Barbini C, Vidal O, Ferrari LM, Thellier D, Derreumaux A, Ismailova E, Askenazy F, Thümmler S. Challenging Behaviors in Children with Nonverbal Autism: A Questionnaire to Guide the Design of a Wearable Device for Biomarker Recording. Sensors. 2025; 25(7):2009. https://doi.org/10.3390/s25072009
Chicago/Turabian StyleWeber, Anne-Sophie, Camilla Barbini, Olivia Vidal, Laura M. Ferrari, Dimitri Thellier, Alexandre Derreumaux, Esma Ismailova, Florence Askenazy, and Susanne Thümmler. 2025. "Challenging Behaviors in Children with Nonverbal Autism: A Questionnaire to Guide the Design of a Wearable Device for Biomarker Recording" Sensors 25, no. 7: 2009. https://doi.org/10.3390/s25072009
APA StyleWeber, A.-S., Barbini, C., Vidal, O., Ferrari, L. M., Thellier, D., Derreumaux, A., Ismailova, E., Askenazy, F., & Thümmler, S. (2025). Challenging Behaviors in Children with Nonverbal Autism: A Questionnaire to Guide the Design of a Wearable Device for Biomarker Recording. Sensors, 25(7), 2009. https://doi.org/10.3390/s25072009