
Advancing Precision: A Comprehensive Review of MRI Segmentation Datasets from BraTS Challenges (2012–2025)



Abstract
1. Introduction
2. MRI Technology: A Critical Tool for Brain Tumor Segmentation
Evolution of MRI Extraction Technologies from 2012 to Present
3. Overview of BraTS Challenges
4. Evolution of BraTS Datasets (2012–2025)
4.1. Dataset Review: BraTS Challenge 2012
- Number of tasks: 1: Multimodal Brain Tumor Image Segmentation—segmentation of gliomas in pre-operative scans.
- Initial number of classes: two class labels:
- Label 1—ED: edema;
- Label 2—TC: tumor core.
- Final number of classes: four class labels:
- Label 1—NCR: necrotic tumor;
- Label 2—ED: peritumoral edema;
- Label 3—NET: non-enhancing tumor;
- Label 4—ET: enhancing tumor;
- Label 0: everything else.
- MRI modalities: All four modalities were available: T1-weighted, native image (T1); T1-weighted, contrast-enhanced (Gadolinium) image (T1c); T2-weighted image (T2); and T2-weighted FLAIR image (FLAIR). In subsequent BraTS challenges, these four modalities were consistently employed unless noted otherwise in the challenge description.
- Whole tumor region (WT): Includes all four tumor structures, corresponding to labels 1 + 2 + 3 + 4.
- Tumor core region (TC): Contains all tumor structures except for “edema”, corresponding to labels 1 + 3 + 4.
- Active tumor region (AT): Includes only the “enhancing core” structures that are unique to high-grade cases, corresponding to labels 1 + 4.
- Pre-Processing Data Protocol: To ensure uniformity across the dataset, the volumetric images of each subject were rigidly aligned to their respective T1c MRI scans. Subsequently, these images were resampled to a standard resolution of 1mm³ using linear interpolation and reoriented to a consistent axial plane. The alignment was facilitated by a rigid registration model that utilized mutual information as the similarity measure, specifically using the “VersorRigid3DTransform” with the “MattesMutualInformation” metric and implemented across three multi-resolution levels within The Insight Toolkit (ITK) software. No attempt was made to align the individual patients within a common reference space. Additionally, all images underwent skull stripping to ensure the anonymization of patient data [13].
- Annotation Method: The simulated images were provided with predefined “ground truth” data for the location of various tumor structures, whereas the clinical images were labeled manually. They established four categories of tumor sub-regions: “edema”, “non-enhancing (solid) core”, “necrotic (or fluid-filled) core”, and “enhancing core”. The annotation protocol for identifying these visual structures in both low- and high-grade cases was as follows:
- The “edema” was primarily segmented from T2-weighted images. FLAIR sequences were used to verify the extent of the edema and to differentiate it from ventricles and other fluid-filled structures. Initial segmentation in T2 and FLAIR included the core structures, which were then reclassified in subsequent steps.
- The gross tumor core, encompassing both enhancing and non-enhancing structures, was initially segmented by assessing hyper-intensities on T1c images (for high-grade tumors) along with inhomogeneous components of the hyper-intense lesion evident in T1 and the hypo-intense areas seen in T1.
- The “enhancing core” of the tumor was subsequently segmented by thresholding T1c intensities within the resulting gross tumor core. This segmentation included the Gadolinium-enhancing tumor rim while excluding the necrotic center and blood vessels. The intensity threshold for segmentation was determined visually for each case.
- The “necrotic (or fluid-filled) core” was identified as irregular, low-intensity necrotic areas within the enhancing rim on T1c images. This label was also applied to the occasional hemorrhages observed in the BRATS dataset.
- The “non-enhancing (solid) core” was characterized as the part of the gross tumor core remaining after the exclusion of the “enhancing core” and the “necrotic (or fluid-filled) core”.
- Multi-Center Imaging Data Acquisition Details: The data were collected from four distinct institutions: Bern University, Debrecen University, Heidelberg University, and Massachusetts General Hospital. These images were gathered over several years, utilizing MRI scanners from various manufacturers, featuring varying magnetic field strengths (1.5 T and 3 T) and different implementations of imaging protocols (such as 2D or 3D) [12,13].
4.2. Dataset Review: BraTS Challenge 2013
- Number of tasks: 1: Multimodal Brain Tumor Image Segmentation—segmentation of gliomas in pre-operative scans.
- Number of classes: four class labels:
- Label 1—NCR: necrotic tumor;
- Label 2—ED: peritumoral edema;
- Label 3—NET: non-enhancing tumor;
- Label 4—ET: enhancing tumor;
- Label 0: everything else.
- Challenge Data: BraTs 2013 had the same objective as BraTS 2012. The training data for BraTS 2013 was identical to the real training data of the 2012 Challenge but with the updated labels (4-class labels). No synthetic cases were evaluated in 2013, and therefore, no synthetic training data were provided. In addition, 10 new data were added to the test set. To summarize, the training data consisted of 30 multi-contrast MRI scans of 10 low- and 20 high-grade glioma patients, while the test images consisted of 25 MRI scans of 11 high- and 4 low-grade real cases from BraTS 2012, as well as 10 new high-grade real cases. Note that the pre-processing Data Protocol, the Annotation Method, and the contributing institutions (Multi-Center Imaging Data Acquisition Details) are the same as in BraTS 2012 [13].
4.3. Dataset Review: BraTS Challenge 2014–2016
- Number of tasks: 2:
- Multimodal Brain Tumor Image Segmentation—segmentation of gliomas in pre-operative scans;
- Disease progression assessment.
- Number of classes: four class labels:
- Label 1—NCR: necrotic tumor;
- Label 2—ED: peritumoral edema;
- Label 3—NET: non-enhancing tumor;
- Label 4—ET: enhancing tumor;
- Label 0: everything else.
- Challenge Data: BraTS has predominantly been engaged in the segmentation of brain tumor sub-regions. Yet, beyond its initial editions in 2012–2013, the challenge’s potential for clinical impact became evident. Subsequently, BraTS introduced secondary tasks, leveraging the outcomes of brain tumor segmentation algorithms to enhance further analyses. Particularly, to highlight the clinical relevance of these segmentation tasks, the BraTS challenges from 2014 to 2016 incorporated longitudinal scans into the datasets. These additions aimed to assess the efficacy and potential of automated tumor volumetry in monitoring disease progression [2].
- Annotation Method: The annotation was accomplished by fusing results of high-ranked segmentation algorithms in BraTS 2012 and BraTS 2013 challenges. These annotations were then approved by visual inspection of experienced raters [16].
4.4. Dataset Review: BraTS Challenge 2017
- Number of tasks: 2:
- Multimodal Brain Tumor Image Segmentation—segmentation of gliomas in pre-operative scans;
- Prediction of patient overall survival (OS) from pre-operative scans.
- Number of classes: three class labels:
- Label 1—NCR/NET: necrotic and non-enhancing tumor;
- Label 2—ED: the peritumoral edema;
- Label 4—ET: the GD-enhancing tumor;
- Label 0: everything else.
- Challenge Data: Task 1 involved developing methodologies for segmenting gliomas on pre-operative scans, utilizing clinically-acquired training data. The analyzed sub-regions included: (1) the enhancing tumor (ET), (2) the tumor core (TC), and (3) the whole tumor (WT). Specifically, WT is defined as the combination of labels 1, 2, and 4; TC comprises labels 1 and 4; and ET corresponds solely to label 4. Figure 5 illustrates how the previous four-class labeling (top panel) was refined in 2017 by omitting the non-enhancing tumor label (NET) and merging it with the necrotic core (NCR). This shift simplified annotations and ensured greater consistency in segmentation tasks across diverse data sources.
- Pre-Processing Data Protocol: A consistent pre-processing protocol has been applied to all BraTS mpMRI scans. This protocol involves converting DICOM files to the NIfTI format, co-registering images to a standard anatomical template (SRI24), resampling them to a uniform isotropic resolution (1 ), and performing skull-stripping. Detailed information on the entire pre-processing pipeline is available through the Cancer Imaging Phenomics Toolkit (CaPTk) and the Federated Tumor Segmentation (FeTS) tool. Converting to NIfTI format removes accompanying metadata from the original DICOM images, effectively stripping out all Protected Health Information (PHI) from the DICOM headers. Additionally, skull-stripping helps prevent any potential facial reconstruction or patient identification. Note that in subsequent challenges, this standardized pre-processing protocol has been consistently employed unless otherwise specified in the challenge description.
- Annotation Method: All ground truth labels from BraTS 2016 were meticulously revised by expert board-certified neuroradiologists. Each imaging dataset underwent manual segmentation by one to four raters, adhering to a consistent annotation protocol. These annotations, which include the GD-enhancing tumor (ET—label 4), the peritumoral edema (ED—label 2), and the necrotic and non-enhancing tumor (NCR/NET—label 1), received approval from experienced neuroradiologists. For further details on the pre-processing and annotation protocols, refer to the following papers: [2,13,18].
- Multi-Center Imaging Data Acquisition Details: The multimodal MRI data were acquired with different clinical protocols and various scanners from multiple (n = 19) institutions. The data contributors are located in the following countries: United States, Switzerland, Hungary, and Germany.
4.5. Dataset Review: BraTS Challenge 2018
- Number of tasks: 2:
- Multimodal Brain Tumor Image Segmentation—segmentation of gliomas in pre-operative scans;
- Prediction of patient overall survival (OS) from pre-operative scans.
- Number of classes: three class labels:
- Label 1—NCR/NET: necrotic and non-enhancing tumor;
- Label 2—ED: the peritumoral edema;
- Label 4—ET: the GD-enhancing tumor;
- Label 0: everything else.
- Challenge Data: The tasks for BraTS 2018 remained unchanged from BraTS 2017: participants were required to develop methods for generating segmentation labels for various glioma sub-regions and to extract imaging/radiomic features to predict patient overall survival (OS) using machine learning techniques. The dataset for BraTS 2018 utilized the same training set as in 2017, but featured different validation and test sets. All ground truth labels were carefully revised by expert board-certified neuroradiologists, and the validation set’s ground truth was not disclosed to participants [16,19].
- It is important to note that only patients who underwent Gross Total Resection (GTR) were considered for the OS prediction analyses [19].
- Annotation Method: All the imaging datasets underwent manual segmentation by one to four raters, following a consistent annotation protocol. All annotations received approval from experienced neuroradiologists. For additional information on the pre-processing and annotation protocols, refer to these papers: [2,13,18].
- Multi-Center Imaging Data Acquisition Details: All BraTS multimodal scans were acquired with different clinical protocols and various scanners from multiple (n = 19) institutions. The institutions contributing to the data are located in the following countries: United States, Switzerland, Hungary, Germany, and India.
4.6. Dataset Review: BraTS Challenge 2019
- Number of tasks: 3:
- Multimodal Brain Tumor Image Segmentation—segmentation of gliomas in pre-operative scans;
- Prediction of patient overall survival (OS) from pre-operative scans;
- Quantification of Uncertainty in Segmentation.
- Number of classes: three class labels:
- Label 1—NCR/NET: necrotic and non-enhancing tumor;
- Label 2—ED: the peritumoral edema;
- Label 4—ET: the GD-enhancing tumor;
- label 0: everything else.
- Challenge Data: In addition to Tasks 1 and 2 from BraTS 2018 and 2017, BraTS 2019 introduced a new challenge focused on evaluating uncertainty measures in glioma segmentation. This task aimed to encourage methods that yield high confidence when predictions are accurate and low confidence when they are not. Participants were required to submit three separate uncertainty maps—one for each voxel label corresponding to: (1) enhancing tumor (ET), (2) tumor core (TC), and (3) whole tumor (WT). These maps were to be evaluated in conjunction with the established BraTS Dice metric.
- The BraTS 2019 challenge provided participants with multi-institutional, routinely acquired pre-operative multimodal MRI scans of high-grade glioblastoma (GBM/HGG) and lower-grade glioma (LGG), all of which had a pathologically confirmed diagnosis and available OS data. The datasets for this year’s challenge were enhanced since BraTS 2018, incorporating more routinely acquired 3T multimodal MRI scans, each annotated with ground truth labels by expert board-certified neuroradiologists. In this challenge, as well as in all subsequent ones, the ground truth labels for the validation data were not provided to the participants. Consistent with prior iterations, only patients who had undergone a gross total resection (GTR) were eligible for the OS prediction assessment [20].
- Annotation Method: All the imaging datasets underwent manual segmentation by one to four raters, following a consistent annotation protocol. All annotations received approval from experienced neuroradiologists. For additional information on the pre-processing and annotation protocol, refer to these papers: [2,13,18].
- Multi-Center Imaging Data Acquisition Details: All BraTS multimodal MRI data were acquired using different clinical protocols and various scanners from multiple (n = 19) institutions. The institutions contributing to the data are located in the following countries: United States, Switzerland, Hungary, Germany, and India.
4.7. Dataset Review: BraTS Challenge 2020
- Number of tasks: 3:
- Multimodal Brain Tumor Image Segmentation—segmentation of gliomas in pre-operative scans;
- Prediction of patient overall survival (OS) from pre-operative scans;
- Quantification of Uncertainty in Segmentation.
- Number of classes: three class labels:
- Label 1—NCR/NET: necrotic and non-enhancing tumor;
- Label 2—ED: peritumoral edema;
- Label 4—ET: GD-enhancing tumor;
- Label 0: everything else.
- Challenge Data: For this year’s BraTS challenge, the dataset was enhanced with an increased number of routinely acquired 3T multimodal MRI scans, all annotated with ground truth labels by expert board-certified neuroradiologists. The format of the overall survival (OS) data remained consistent with previous years. Moreover, to aid in broader research efforts, they have provided a naming convention and direct filename mapping between the data from BraT 2020 to 2017 and the TCGA-GBM and TCGA-LGG collections hosted by The Cancer Imaging Archive (TCIA), thereby supporting studies that extend beyond the immediate scope of the BraTS tasks [21].
- Annotation Method: All datasets underwent manual segmentation by one to four raters, adhering to a consistent annotation protocol. All annotations received approval from experienced neuroradiologists. For additional information on the pre-processing and annotation protocols, refer to these papers: [2,13,18].
- Multi-Center Imaging Data Acquisition Details: All BraTS multimodal MRI data were acquired with different clinical protocols and various scanners from multiple (n = 19) institutions. The institutions contributing to the data are located in the following countries: United States, Switzerland, Hungary, Germany, and India.
4.8. Dataset Review: BraTS Challenge 2021
- Number of tasks: 2:
- Multimodal Brain Tumor Image Segmentation—segmentation of gliomas in pre-operative scans;
- Radiogenomic Classification—evaluation of classification methods to predict the MGMT promoter methylation status at pre-operative baseline scans.
- Number of classes: three class labels:
- Label 1—NCR: necrotic tumor;
- Label 2—ED: peritumoral edema;
- Label 4—ET: GD-enhancing tumor;
- Label 0: everything else.
- Challenge Data: The BraTS Challenge 2021 was hosted by the Radiological Society of North America (RSNA), the American Society of Neuroradiology (ASNR), and the Medical Image Computing and Computer-Assisted Interventions (MICCAI) Society. The RSNA-ASNR-MICCAI BraTS 2021 challenge utilized multi-institutional multi-parametric magnetic resonance imaging (mpMRI) scans, continuing to focus on Task 1: assessing advanced methods for segmenting brain glioblastoma sub-regions in mpMRI scans.
- The 2021 revision of the World Health Organization (WHO) classification of CNS tumors underscored the importance of integrated diagnostics, transitioning from solely morphologic–histopathologic classifications to incorporating molecular–cytogenetic features. One such feature, the methylation status of the O6-methylguanine-DNA methyltransferase (MGMT) promoter in newly diagnosed GBM, was recognized as a significant prognostic factor and predictor of chemotherapy response. Consequently, determining the MGMT promoter methylation status in newly diagnosed GBM became crucial for guiding treatment decisions. In response, BraTS 2021 introduced Task 2, which evaluated classification methods for predicting the MGMT promoter methylation status from pre-operative baseline scans, specifically distinguishing between methylated (MGMT+) and unmethylated (MGMT-) tumors.
- The RSNA-ASNR-MICCAI BraTS 2021 Challenge released the largest and most diverse retrospective cohort of glioma patients to date. The impact of this challenge is underscored by the dramatic increase in the number of participating teams, which rose from 78 in 2020 to over 2300 in 2021. The datasets for this year’s challenge were notably expanded since BraTS 2020 with a significant increase in routine clinically-acquired mpMRI scans, raising the total number of cases from 660 to 2040 and thereby broadening the demographic diversity of the patient population represented. Ground truth annotations of the tumor sub-regions were all verified by expert neuroradiologists for Task 1, while the MGMT methylation status was determined based on laboratory assessments of the surgical brain tumor specimens [3,22].
- Pre-Processing Data Protocol: For Task 1, which involves the segmentation of tumor sub-regions, the standardized pre-processing protocol established by BraTS has been applied to all mpMRI scans. For Task 2, focusing on radiogenomic classification, all imaging volumes were initially processed as in Task 1 to produce skull-stripped volumes. These were then reconverted from NIfTI back to the DICOM format. Once the mpMRI sequences were reverted to DICOM, further de-identification was implemented through a two-step process. For more details on the pre-processing protocols employed for both tasks, refer to this paper [3].
- Annotation Protocol: In earlier BraTS challenges, specifically for Task 1, the annotation process typically began with manual delineation of the abnormal signal on T2-weighted images to define the WT, followed by the TC, and ultimately addressing the enhancing and non-enhancing/necrotic core, often employing semi-automatic tools. For BraTS 2021, to streamline the annotation process, initial automated segmentations were produced by combining methods from previously top-performing algorithms at BraTS. These included DeepMedic, DeepScan, and nnU-Net, all of which were trained on the BraTS 2020 dataset. The STAPLE label fusion technique was utilized to merge the segmentations from these individual methods, helping to address systematic errors from each. This entire segmentation process, including the automated fusion technique, has been made accessible on the Federated Tumor Segmentation (FeTS) platform.
- Volunteer expert neuroradiology annotators were provided with all four mpMRI modalities alongside the automated fused segmentation volumes to begin manual adjustments. ITK-SNAP software was employed for these refinements. After the initial automated segmentations were refined, they were reviewed by two senior attending board-certified neuroradiologists, each with over 15 years of experience. Based on their evaluation, these segmentations were either approved or sent back to the annotators for further adjustments. This iterative process continued until the refined tumor sub-region segmentations were deemed satisfactory for public release and use in the challenge. The tumor sub-regions were delineated according to established radiological observations (VASARI features) and consist of the Gd-enhancing tumor (ET—label 4), the peritumoral edematous or invaded tissue (ED—label 2), and the necrotic tumor core (NCR—label 1) [3]. The significant annotation contributions to the dataset were made possible by over forty volunteer neuroradiology experts from around the world [22].
- The determination of the MGMT promoter methylation status in the BraTS 2021 dataset at each hosting institution was performed using various methods, including pyrosequencing and next-generation quantitative bisulfite sequencing of promoter CpG sites. Adequate tumor tissue collected at the time of surgery was required for these assessments.
- Multi-Center Imaging Data Acquisition Details: The dataset describes a collection of brain tumor mpMRI scans acquired from multiple different institutions under standard clinical conditions, but with different equipment and imaging protocols, resulting in a vastly heterogeneous image quality reflecting diverse clinical practice across different institutions [3]. The multimodal scans were collected from fourteen distinct institutions that are located in the following countries: United States, Germany, Switzerland, Canada, Hungary, and India.
4.9. Dataset Review: BraTS Challenge 2022
4.10. Dataset Review: BraTS Challenge 2023
- Number of tasks: 8:
- Segmentation—adult glioma: RSNA-ASNR-MICCAI BraTS Continuous Evaluation Challenge;
- Segmentation—BraTS-Africa: BraTS Challenge on Sub-Sahara-Africa Adult Glioma;
- Segmentation—meningioma: ASNR-MICCAI BraTS Intracranial Meningioma Challenge;
- Segmentation—brain metastases: ASNR-MICCAI BraTS Brain Metastasis Challenge;
- Segmentation—pediatric tumors: ASNR-MICCAI BraTS Pediatrics Tumor Challenge;
- Synthesis (Global)—missing MRI: ASNR-MICCAI BraTS MRI Synthesis Challenge (BraSyn);
- Synthesis (Local)—inpainting: ASNR-MICCAI BraTS Local Synthesis of Tissue via Inpainting;
- Evaluating Augmentations for BraTS: BraTS Challenge on Relevant Augmentation Techniques.
- Number of classes for tasks 1–8: three class labels:
- Label 1—NCR: necrotic tumor core;
- Label 2—ED: peritumoral edematous/invaded tissue;
- Label 3—ET: GD-enhancing tumor;
- Label 0: everything else.
- Number of classes for tasks 2–4: three class labels:
- Label 1—NETC: non-ehancing tumor core;
- Label 2—SNFH: surrounding non-enhancing FLAIR hyperintensity;
- Label 3—ET: enhancing tumor;
- Label 0: everything else.
- Number of classes for tasks 5: three class labels:
- Label 1—NC: non-enhancing component (a combination of nonenhancing tumor, cystic component, and necrosis);
- Label 2—ED: peritumoral edematous area;
- Label 3—ET: enhancing tumor;
- Label 0: everything else.
- MRI modalities: All four modalities were available: T1-weighted, native image (T1); T1-weighted, contrast-enhanced (Gadolinium) image (T1c); T2-weighted image (T2), and T2-weighted FLAIR image (FLAIR).
- Primarily due to computational constraints, the synthesis (local)–inpainting task exclusively utilized T1 scans.
- Challenge Data:
- Segmentation—adult glioma: RSNA-ASNR-MICCAI BraTS Continuous Evaluation Challenge: The BraTS Continuous Challenge is a continuation of the 2021 challenge. The training and validation datasets, identical to those used for the RSNA-ASNR-MICCAI BraTS 2021 Challenge, encompass a total of 5880 MRI scans from 1470 patients with brain diffuse gliomas. While the training and validation data remained consistent with those used in BraTS 2021, the testing dataset for this year’s challenge was significantly expanded to include a larger number of routine clinically-acquired mpMRI scans [10].
- Segmentation—BraTS-Africa: BraTS Challenge on Sub-Sahara-Africa Adult Glioma: The BraTS-Africa Challenge focuses on addressing the disparity in glioma treatment outcomes between high-income regions and Sub-Saharan Africa (SSA), where survival rates have not improved significantly due to factors such as the use of lower-quality MRI technology (see Figure 6), late-stage disease presentation, and unique glioma characteristics. Brain MRI scans from SSA typically exhibit reduced contrast and resolution, as demonstrated in Figure 6, which underscores the need for advanced pre-processing to enhance image quality prior to ML-based segmentation. This challenge is part of a broader effort to adapt and evaluate computer-aided diagnostic (CAD) tools for glioma detection in resource-limited settings, aiming to bridge the gap between research and clinical practice.The MICCAI-CAMERA-Lacuna Fund BraTS-Africa 2023 Challenge has assembled the largest publicly available retrospective cohort of pre-operative glioma MRI scans from adult Africans, including both low-grade glioma (LGG) and glioblastoma/high-grade glioma (GBM/HGG). The BraTS-Africa challenge involves developing machine learning algorithms to automatically segment intracranial gliomas into three distinct classes using a new 3-label system. The sub-regions for evaluation are enhancing tumor (ET), non-enhancing tumor core (NETC), and surrounding non-enhancing FLAIR hyperintensity (SNFH), which are crucial for enhancing diagnostic accuracy and treatment planning in these underserved populations [10,25].
- Segmentation—meningioma: ASNR-MICCAI BraTS Intracranial Meningioma Challenge: Meningioma is the most prevalent intracranial brain tumor in adults, often causing significant health issues. While about 80% of these tumors are benign WHO grade 1 meningiomas, effectively managed through observation or therapy, the more aggressive grades 2 and 3 meningiomas pose greater risks, frequently recurring despite comprehensive treatment. Currently, there is no effective noninvasive technique for determining the grade of meningioma, its aggressiveness, or for predicting outcomes.Automated brain MRI tumor segmentation has evolved into a clinically useful tool that provides precise measurements of tumor volume, aiding in surgical and radiotherapy planning and monitoring treatment responses. Yet, most segmentation research has primarily focused on gliomas. Meningiomas present unique challenges for segmentation due to their extra-axial location and the likelihood of involving the skull base. Moreover, since meningiomas are often identified through imaging alone, accurate MRI analysis becomes crucial for effective treatment planning.The aim of the BraTS 2023 Meningioma Challenge was to develop an automated multi-compartment brain MRI segmentation algorithm specifically for meningiomas. This tool was intended not only to assist in accurate surgical and radiotherapy planning but also to pave the way for future research into meningioma classification, aggressiveness evaluation, and recurrence prediction based solely on MRI scans. For this challenge, all meningioma MRI scans were taken pre-operatively and pre-treatment. The objective was to automate the segmentation of these tumors using a three-label system: enhancing tumor (ET), non-enhancing tumor core (NETC), and surrounding non-enhancing FLAIR hyperintensity (SNFH) [10].
- Segmentation—brain metastases: ASNR-MICCAI BraTS Brain Metastasis Challenge: Brain metastases are the most prevalent type of CNS malignancy in adults and pose significant challenges in clinical assessments. This complexity is mainly due to the common occurrence of multiple, often small, metastases within a single patient. Additionally, the extensive time required to meticulously analyze multiple lesions across consecutive scans complicates detailed evaluations. Consequently, the development of automated segmentation tools for brain metastases is vital for enhancing patient care. Precisely detecting small metastatic lesions, especially those under 5 mm, is crucial for improving patient prognosis, as overlooking even a single lesion could result in treatment delays and repeated medical procedures. Moreover, the total volume of brain metastases is a critical indicator of patient outcomes, yet it remains unmeasured in routine clinical settings due to the lack of effective volumetric segmentation tools.The solution lies in crafting innovative segmentation algorithms capable of identifying and accurately quantifying the volume of all lesions. While some algorithms perform well with larger metastases, they often fail to detect or accurately segment smaller metastases. The inclusion criteria for the BraTS 2023 Brain Metastases challenge were MRI scans that showed untreated brain metastases with all four MRI modalities. Exclusion criteria included scans with prior treatment effects, missing required MRI sequences, or poor-quality images due to motion or other significant artifacts. Cases with post-treatment changes were deferred to BraTS-METS 2024.The dataset encompasses a collection of treatment-naive brain metastases mpMRI scans from various institutions, captured under standard clinical protocols. A total of 1303 studies were annotated, with 402 studies comprising 3076 lesions made publicly available for the competition. Additionally, 31 studies with 139 lesions were set aside for validation, and 59 studies with 218 lesions were designated for testing. Notably, the Stanford University dataset, despite being publicly accessible, was excluded from the primary dataset due to the absence of T2 sequences but was available for optional additional training [10,26].
- Segmentation—pediatric tumors: ASNR-MICCAI BraTS Pediatrics Tumor Challenge: The ASNR-MICCAI BraTS Pediatrics Tumor 2023 Challenge marked the inaugural focus on pediatric brain tumors within the BraTS series, targeting a significant area of concern as pediatric central nervous system tumors are the leading cause of cancer-related mortality in children. The five-year survival rate for high-grade gliomas in children is less than 20%. Furthermore, due to their rarity, the diagnosis is often delayed and treatment relies on historical methods, with clinical trials requiring collaboration across multiple institutions.The 2023 Pediatrics Tumor Challenge leveraged a comprehensive international dataset gathered from consortia dedicated to pediatric neuro-oncology. Notably, it provided the largest annotated public retrospective cohort of high-grade pediatric glioma cases.The dataset for BraTS-PEDs 2023 included a multi-institutional cohort of standard clinical MRI scans, with inherent variations in imaging protocols and equipment across different institutions contributing to the diversity in image quality. The inclusion criteria for the challenge were pediatric patients with histologically confirmed high-grade gliomas, ensuring the availability of all four mpMRI sequences on treatment-naive scans. Exclusion criteria included images of poor quality or containing artifacts that hinder reliable tumor segmentation and infants younger than one month.Data for a total of 228 pediatric patients with high-grade gliomas was sourced from CBTN, Boston Children’s Hospital, and Yale University. This cohort was divided into subsets for training (99 cases), validation (45 cases), and testing (84 cases) [27].
- Synthesis (Global)—missing MRI: ASNR-MICCAI BraTS MRI Synthesis Challenge (BraSyn). Most segmentation algorithms depend on the availability of four standard MRI modalities: T1-weighted images with and without contrast, T2-weighted images, and FLAIR images. However, in clinical settings, certain sequences might be missing due to factors like time constraints or patient movement, which can introduce artifacts. Therefore, developing methods to effectively substitute missing modalities and maintain segmentation accuracy is crucial for these algorithms to be widely used in clinical routines. To address this, BraTS 2023 launched the Brain MR Image Synthesis (BraSyn) Challenge, aimed at evaluating methods that can realistically synthesize absent MRI modalities given multiple available images.The BraSyn-2023 dataset is based on the RSNA-ASNR-MICCAI BraTS 2021 dataset, comprising 1251 training cases, 219 validation cases, and 570 testing cases. The challenge required participants to handle scenarios where one of the four modalities was randomly absent (‘dropout’) in the test set provided for each subject, leaving only three modalities available. Participants’ algorithms were expected to generate plausible images for the missing modality. Figure 7 illustrates the BraSyn-2023 design, where one of the four modalities is randomly dropped during the validation and test phases, requiring participants to synthesize the missing modality and still achieve accurate segmentation. The synthesized images were evaluated on three criteria: their overall quality, the accuracy of segmentation within the generated images, and the effectiveness of a subsequent tumor segmentation algorithm when applied to the completed image set [28].
- Synthesis (Local)—inpainting: ASNR-MICCAI BraTS Local Synthesis of Tissue via Inpainting: In the BraTS 2023 inpainting challenge, participants were required to develop algorithmic solutions for synthesizing 3D healthy brain tissue in regions affected by glioma. This challenge arose from the need for improved tools to assist clinicians in decision-making and care provision, as most existing brain MR image analysis algorithms are optimized for healthy brains and may underperform on pathological images. These algorithms include, but are not limited to, brain anatomy parcellation, tissue segmentation, and brain extraction.The inpainting challenge addressed this issue by assigning the task of filling in pathological brain areas with synthesized healthy tissue, utilizing provided images and inpainting masks (See Figure 8). Since no actual healthy tissue data existed for tumor regions, surrogate inpainting masks created from the healthy portions of the brain were crafted using a specific protocol and provided to participants to train these algorithms. During training, participants were provided with T1 images featuring voided regions along with a corresponding void mask, the original T1 scans, and two additional masks: one for the tumor and one for the healthy area. This challenge exclusively utilized T1 scans for two main reasons: to reduce the computational demands on participants and to develop algorithms that could be generalized to other brain pathologies, as T1 scans are commonly included in MRI protocols for various conditions [29].In addition to enabling the application of standard brain image segmentation algorithms to tumor-affected brains, local inpainting also allows for the synthetic removal of tumor areas from images. This could deepen the understanding of the interplay between different brain regions and abnormal brain tissue, and is crucial for tasks such as brain tumor modeling. Moreover, inpainting helps manage local artifacts like B-field inhomogeneities, which sometimes impair the quality of brain tumor images.
- Evaluating Augmentations for BraTS: BraTS Challenge on Relevant Augmentation Techniques: The concept of data-centric machine learning focuses on enhancing model performance through the use of high-quality, meaningful training data. While data augmentation is recognized for boosting the robustness of machine learning models, the specific types of augmentations that benefit biomedical imaging remain uncertain. Participants were asked to develop methods to augment training data, aiming to enhance the robustness of a baseline model on newly introduced data.Software as a Medical Device (SaMD), as defined by the International Medical Device Regulators Forum (IMDRF), refers to software designed for medical use that operates independently of any hardware device. The challenge directly addressed concerns about algorithmic bias—where model predictions could be unfairly skewed against certain groups—and sought to improve algorithm robustness. Participants were tasked with creating computational methods that augmented a dataset of medical images, such that retraining a baseline AI/ML model on this augmented dataset led to improved accuracy and robustness on independent test data not previously exposed to the model. This approach would ensure that the AI/ML models used in SaMD are both effective and reliable, particularly in imaging-focused applications.The challenge used the RSNA-ASNR-MICCAI BraTS 2021 dataset to allow participants to develop and test their augmentation techniques. The goal was to improve a segmentation model with enhanced training data [10].
- Pre-Processing Data Protocol: The standardized pre-processing protocol established by BraTS has been applied to all mpMRI scans.
- Annotation Method:
- Segmentation—Adult Glioma Dataset: The BraTS Adult Glioma training and validation data were identical to the RSNA-ASNR-MICCAI BraTS 2021 dataset, and thus used the same annotation protocol. The only change, implemented starting in 2023, was a new naming convention where the ET label value was updated from ‘4’ to ‘3’. The annotations include the GD-enhancing tumor (ET—label 3), the peritumoral edematous/invaded tissue (ED—label 2), and the necrotic tumor core (NCR—label 1) [10].
- Segmentation—BraTS-Africa Dataset: All imaging data were reviewed and manually annotated by board-certified radiologists specializing in neuro-oncology, following the BraTS pre-processing and annotation protocols. Figure 9 demonstrates the new segmentation labeling introduced in 2023, which is also employed in the BraTS-Meningioma and BraTS-Metastasis 2023 challenge. This labeling system delineates three tumor sub-regions:
- (a)
- Enhancing tumor (ET): represents all tumor portions with a noticeable increase in T1 signal on post-contrast images compared to pre-contrast images, excluding adjacent blood vessels, intrinsic T1 hyperintensity, or abnormal signal in non-tumor tissues.
- (b)
- Non-enhancing tumor core (NETC): includes all non-enhancing tumor core areas, such as necrosis, cystic changes, calcification, and other non-enhancing components. Intrinsic T1 hyperintensity (e.g., intratumoral hemorrhage or fat) is also included.
- (c)
- Surrounding non-enhancing FLAIR hyperintensity (SNFH): covers the full extent of FLAIR signal abnormalities surrounding the tumor that are unrelated to the tumor core. For meningiomas, this corresponds to “vasogenic edema”, excluding non-tumor-related FLAIR abnormalities like prior infarcts or microvascular ischemic changes [10].
- Segmentation—meningioma: ASNR-MICCAI BraTS Intracranial Meningioma Challenge: Prior to manual segmentation, an automated pre-segmentation model using a deep convolutional neural network (nnU-Net) was used to produce initial multi-region segmentations. This model was initially trained on a dataset of 73 manually labeled studies from a single institution, all involving meningiomas that had undergone surgical resection. While effective, this initial training set introduced a bias that could reduce model performance for non-surgical cases. To mitigate this, the model was iteratively retrained during the challenge preparation phase using additional manually corrected cases from various sites, including non-surgical meningiomas. This iterative process aimed to enhance the model’s generalizability across diverse MRI appearances and reduce pre-segmentation bias.Manual corrections of the pre-segmented labels were performed by a diverse group of annotators, ranging from medical students to experienced neuroradiologists with over 10 years of expertise. Corrections were carried out using ITK-SNAP, an open-source tool for segmenting 3D and 4D biomedical images. Annotators were provided with detailed instructions, written descriptions of tumor sub-compartment compositions, and examples of common pre-segmentation errors to ensure consistency and reduce variability in corrections. After annotators completed their corrections, each case was reviewed by a trained neuroradiologist. Cases identified as incomplete or inaccurate were returned for additional refinement by a different annotator.For BraTS 2023 Meningioma, the task was to automatically segment intracranial meningiomas using a three-label system: enhancing tumor (ET), non-enhancing tumor core (NETC), and surrounding non-enhancing FLAIR hyperintensity (SNFH). For additional details on the pre-segmentation and annotation procedures, refer to the task manuscript: [30].
- Segmentation—brain metastases: ASNR-MICCAI BraTS Brain Metastasis Challenge: To ensure consistency in tumor labeling, a comprehensive annotation pipeline was established. This pipeline, designed to generate accurate ground truth (GT) labels, comprises five main stages: pre-segmentation, annotation refinement, technical quality control (QC), initial approval, and final approval. The pre-segmentation phase involved generating segmentation using three nnU-Net models trained on different datasets:
- (1)
- A model trained on the UCSF-BMSR MRI dataset to produce ET labels, fused with NETC and SNFH predictions from a model trained on the BraTS 2021 glioma dataset.
- (2)
- A model trained on the AURORA multicenter dataset to generate SNFH and tumor core (ET + NETC) labels.
- (3)
- A model trained on the Heidelberg dataset to segment SNFH and tumor core labels.
The label fusion methods varied by label type: SNFH (label 2) was fused using the STAPLE algorithm to address systematic errors; ET (label 3) was combined using minority voting to improve the detection of small metastases; NETC (label 1) was derived solely from the UCSF-BMSR-trained model, overlapping ET and SNFH labels. Annotators were provided with pre-segmentations, fused segmentations, and subtraction images to refine annotations. Over 150 annotators, including students and neuroradiology experts, participated under coordinator supervision, receiving training through group reviews and lectures. Incomplete cases were returned for re-annotation. Additionally, quality control (QC) ensured proper alignment with the SRI24 atlas and validated the presence of all required segmentation masks. Each refined case underwent secondary review by another neuroradiologist, with discrepancies resolved directly by the reviewers. A final dataset review by an experienced neuroradiologist ensured uniformity and consistency. For more details, refer to the task manuscript [26]. - Segmentation—pediatric tumors: ASNR-MICCAI BraTS Pediatrics Tumor Challenge: Following pre-processing, the images were segmented into tumor subregions using two pediatric-specific automated deep-learning models. These models produced preliminary segmentations of four tumor subregions, as recommended by the Response Assessment in Pediatric Neuro-Oncology (RAPNO) working group for assessing treatment response in high-grade gliomas and DIPGs. The subregions included the following:
- -
- Enhancing tumor (ET): Bright areas on T1 post-contrast images compared to T1 pre-contrast, with mild enhancement verified by comparing normal brain signal intensity.
- -
- Cystic component (CC): Very bright on T2 and dark on T1CE, resembling cerebrospinal fluid (CSF) and located within the tumor, either centrally or peripherally.
- -
- Non-enhancing tumor (NET): Any abnormal signal within the tumor not classified as enhancing or cystic.
- -
- Peritumoral edema (ED): Bright, finger-like areas on FLAIR scans, preserving underlying brain structure and surrounding the tumor.
The automated segmentations served as the basis for manual refinement by volunteer neuroradiology experts using ITK-SNAP software. Annotators were provided with all four mpMRI sequences and the fused segmentation volume to guide their corrections. Refined segmentations were then reviewed by three board-certified neuroradiologists. Cases were either approved or returned for additional adjustments in an iterative process until the segmentations were deemed acceptable.For consistency with other BraTS 2023 challenges and to facilitate integration with adult glioma datasets, participants were provided with three final segmentation labels, enhancing tumor (ET), peritumoral edematous area (ED), and non-enhancing component (NC), which is a combination of non-enhancing tumor, cystic component, and necrosis [27]. Figure 10 illustrates this consolidation process: the left image shows the initial four-class subregions (ET, NET, CC, ED), while the right image depicts how these were merged into the final three-class labeling scheme used for model training. - Synthesis (Global)—missing MRI: ASNR-MICCAI BraTS MRI Synthesis Challenge (BraSyn): The BraSyn-2023 dataset is based on the RSNA-ASNR-MICCAI BraTS 2021 dataset and, therefore, shares the same annotation protocol [28].
- Synthesis (Local)—inpainting: ASNR-MICCAI BraTS Local Synthesis of Tissue via Inpainting: For the BraTS 2023 challenge, T1 sequence images were used to generate two types of masks for participants. The first mask type delineates tumor-affected areas, while the second identifies likely healthy brain regions. Healthy brain masks were created by sampling existing tumor shapes and placing them in regions distant from tumors, enabling realistic training and evaluation of inpainting methods.The procedure for generating inpainting masks involves several steps. A pool of 1429 tumor masks was extracted from 1251 brains in the BraTS 2023 Adult Glioma dataset, selecting disconnected tumor compartments with at least 800 voxels. Masks were chosen based on tumor size, with small masks assigned to large tumors and vice versa, ensuring variability. Masks underwent transformations, including mirroring and random rotations, and were placed at semi-random positions distant from the tumor. Validity checks ensured masks met specific criteria, such as maintaining a minimum distance of five voxels from the tumor and limited overlap with the background. Once valid, both healthy and tumor masks were provided to participants. Participants were encouraged to enhance the process and create additional masks for training. To ensure healthy masks were accurate, medical experts manually reviewed and selected the best candidates from algorithm-generated options. Larger masks were preferred where possible to counteract a statistical bias toward smaller ones. For more details, refer to the task manuscript [29].
- Evaluating Augmentations for BraTS: BraTS Challenge on Relevant Augmentation Techniques: The dataset is based on the RSNA-ASNR-MICCAI BraTS 2021 dataset and, therefore, shares the same annotation protocol.
- Multi-Center Imaging Data Acquisition Details:
- For each task, a detailed list of contributors and their affiliations is available in the respective manuscripts or in the complete contributor list here: [10].
- Segmentation—adult glioma: RSNA-ASNR-MICCAI BraTS Continuous Evaluation Challenge: Same as BraTS 2021.
- Segmentation—BraTS-Africa: BraTS Challenge on Sub-Sahara-Africa Adult Glioma: Contributions to the BraTS-Africa data came from a total of four medical professionals across several prestigious institutions in Nigeria.
- Segmentation—meningioma: ASNR-MICCAI BraTS Intracranial Meningioma Challenge: The dataset for the ASNR-MICCAI BraTS Intracranial Meningioma Challenge comprises contributions from six institutions, all located in the United States (USA).
- Segmentation—brain metastases: ASNR-MICCAI BraTS Brain Metastasis Challenge: The BraTS-METS dataset included mpMRI scans from diverse institutions, representing the variability in imaging protocols and equipment reflective of global clinical practices. Eleven source institutions contributed to the Brain Metastases Dataset, with nine located in the United States, one in Germany, and one in Egypt.
- Segmentation—pediatric tumors: ASNR-MICCAI BraTS Pediatrics Tumor Challenge: Eight source institutions contributed to the dataset, all located in the United States (USA).
- Synthesis (Global)—missing MRI: ASNR-MICCAI BraTS MRI Synthesis Challenge (BraSyn): The BraSyn-2023 dataset is based on the RSNA-ASNR-MICCAI BraTS 2021 dataset. Therefore, data contributors are the same as BraTS 2021.
- Synthesis (Local)—inpainting: ASNR-MICCAI BraTS Local Synthesis of Tissue via Inpainting: BraTS Local Inpainting Challenge exclusively employs T1 scans from the multi-modal BraTS 2023 glioma segmentation challenge; therefore, the data contributors are the same as those for BraTS 2021.
- Evaluating Augmentations for BraTS: BraTS Challenge on Relevant Augmentation Techniques: The dataset is based on the RSNA-ASNR-MICCAI BraTS 2021 dataset. Therefore, data contributors are the same as BraTS 2021.
4.11. Dataset Review: BraTS Challenge 2024
- Number of tasks: 10:
- Segmentation—adult glioma post-treatment: BraTS Adult Glioma Post Treatment Challenge;
- Segmentation—BraTS-Africa: BraTS Challenge on Sub-Sahara-Africa Adult Glioma;
- Segmentation—meningioma radiotherapy: BraTS Meningioma Radiotherapy Challenge;
- Segmentation—brain metastases: ASNR-MICCAI BraTS Brain Metastasis Challenge;
- Segmentation—pediatric tumors: ASNR-MICCAI BraTS Pediatrics Tumor Challenge;
- Segmentation—generalizability: ASNR-MICCAI BraTS Generalizability Across Brain Tumors;
- Synthesis (Global)—missing MRI: ASNR-MICCAI BraTS MRI Synthesis Challenge (BraSyn);
- Synthesis (Local)—inpainting: ASNR-MICCAI BraTS Local Synthesis of Tissue via Inpainting;
- Evaluating Augmentations for BraTS: BraTS Challenge on Relevant Augmentation Techniques;
- Pathology.
- Number of classes for tasks 1: four class labels:
- Label 1—NETC: non-enhancing tumor core;
- Label 2—SNFH: surrounding non-enhancing FLAIR hyperintensity;
- Label 3—ET: enhancing tumor;
- Label 4—RC: resection cavity;
- Label 0: everything else.
- Number of classes for task 3: one class label:
- Label 1—GTV: gross tumor volume.
- Number of classes for tasks 9: three class labels:
- Label 1—NCR: necrotic tumor core;
- Label 2—ED: peritumoral edematous/invaded tissue;
- Label 3—ET: GD-enhancing tumor;
- Label 0: everything else.
- Number of classes for tasks 2–4: three class labels:
- Label 1—NETC: non-enhancing tumor core;
- Label 2—SNFH: surrounding non-enhancing FLAIR hyperintensity;
- Label 3—ET: enhancing tumor;
- Label 0: everything else.
- Number of classes for tasks 5: four class labels:
- Label 1—ET: enhancing tumor;
- Label 2—NET: non-enhancing tumor;
- Label 3—CC: cystic component;
- Label 4—ED: peritumoral edema;
- Label 0: everything else.
- Number of classes for tasks 10: nine class labels:
- Label 1—CT: presence of cellular tumor;
- Label 2—PN: pseudopalisading necrosis;
- Label 3—MP: areas abundant in microvascular proliferation;
- Label 4—NC: geographic necrosis;
- Label 5—IC: infiltration into the cortex;
- Label 6—WM: penetration into white matter;
- Label 7—LI: leptomeningeal infiltration;
- Label 8—DM: regions dense with macrophages;
- Label 9—PL: presence of lymphocytes;
- Label 0: everything else.
- MRI modalities: All four modalities were available: T1-weighted, native image (T1); T1-weighted, contrast-enhanced (Gadolinium) image (T1c); T2-weighted image (T2); and T2-weighted FLAIR image (FLAIR).
- Primarily due to computational constraints, the synthesis (local)—inpainting task exclusively utilized T1 scans. In addition, the 2024 Meningioma Radiotherapy Challenge dataset utilized only T1-weighted scans in native acquisition space. This approach is designed to mimic the data typically available for most radiotherapy planning scenarios.
- Challenge Data:
- Segmentation—adult glioma post-treatment: BraTS Adult Glioma Post Treatment Challenge: Gliomas are the most common malignant primary brain tumors in adults, with diffuse gliomas being particularly prevalent. Treatment typically involves a combination of surgery, radiation, and systemic therapies tailored to the tumor’s characteristics and the patient’s condition. MRI remains the gold standard for monitoring diffuse gliomas post-treatment, offering critical insights into tumor size, location, and morphological changes, which are essential for guiding treatment adjustments and predicting clinical outcomes.The 2024 BraTS challenge introduced a focus on post-treatment gliomas for the first time. Task 1 aimed to develop an automated brain tumor segmentation algorithm for high- and low-grade diffuse gliomas in post-treatment MRI, including a new subregion: the resection cavity (RC). Data and algorithms generated from this challenge have the potential to aid in objectively assessing residual tumor volume, improving treatment planning and outcome prediction [11].
- Segmentation—BraTS-Africa: BraTS Challenge on Sub-Sahara-Africa Adult Glioma: The BraTS-Africa Challenge, first launched in 2023, introduced labeled datasets specifically for adult populations in Sub-Saharan Africa. Building on its success, the second BraTS-Africa Challenge (BraTS-Africa 2024) was organized. The MICCAI-CAMERA-Lacuna Fund BraTS-Africa 2024 Challenge offered the largest publicly available annotated retrospective dataset of pre-operative glioma cases in adult Africans, including both low-grade glioma (LGG) and glioblastoma/high-grade glioma (GBM/HGG). Participants were tasked with developing segmentation methods using the clinically acquired BraTS-Africa training data, supplemented with training and validation datasets from the BraTS 2023 Adult Glioma Challenge [11].
- Segmentation—meningioma radiotherapy: BraTS Meningioma Radiotherapy Challenge: Meningioma is the most common primary intracranial tumor, with about 80% being benign and effectively managed with positive outcomes. However, higher-grade meningiomas (WHO grades 2 and 3) pose greater health risks and have higher recurrence rates. They are primarily treated with radiation therapy, which may be used as the main treatment, as a postoperative adjunct, or for recurring cases. Accurate segmentation of the gross tumor volume (GTV) is critical for radiotherapy planning but remains complex and time-intensive, with no reliable automated solutions currently available.The BraTS 2024 Meningioma Radiotherapy Segmentation Challenge aimed to bridge existing gaps by developing algorithms capable of automatically segmenting gross tumor volumes (GTVs) in cranial and facial meningiomas from radiotherapy planning MRI scans.The BraTS-MEN-RT challenge exclusively includes radiotherapy planning brain MRI scans, either preoperative or postoperative, with tumors that are radiographically or pathologically consistent with meningioma. These scans consist of a single series (T1-weighted imaging) in native acquisition space, reflecting typical radiotherapy planning scenarios. This approach replaces the multi-sequence, co-registered MRI scans used in each of the BraTS 2023 automated segmentation challenges [11].
- Segmentation—brain metastases: ASNR-MICCAI BraTS Brain Metastasis Challenge: The challenge focused on developing versatile autosegmentation algorithms capable of precisely delineating brain metastases of varying sizes. These algorithms aim to streamline monitoring and management in both pre- and post-treatment settings, offering the potential to significantly enhance patient care and treatment planning [11].
- Segmentation—pediatric tumors: ASNR-MICCAI BraTS Pediatrics Tumor Challenge: Building on the first BraTS-PEDs Challenge in 2023, the 2024 BraTS-PEDs Challenge expanded to include a larger and more diverse dataset from additional institutions, enhancing its scope and clinical relevance.The 2024 challenge provided the largest publicly available annotated cohort of high-grade pediatric gliomas, including astrocytoma and diffuse midline glioma (DMG)/diffuse intrinsic pontine glioma (DIPG).This year, the challenge introduced significant updates to the processing pipeline and tumor subregion evaluation. The evaluated regions now include: (i) enhancing tumor (ET); (ii) non-enhancing tumor (NET); (iii) cystic component (CC); (iv) edema (ED); (v) tumor core (TC), which combines ET, NET, and CC; and (vi) the whole tumor (WT) [31].
- Segmentation—generalizability: ASNR-MICCAI BraTS Generalizability Across Brain Tumors: While segmentation is a widely studied medical image processing task, the BraTS Generalizability Across Tumors (BraTS-GoAT) Challenge emphasizes algorithmic generalizability across various tumor types and patient populations. The goal was to develop a segmentation algorithm that can adapt to different brain tumor types with limited training data.Candidate algorithms should demonstrate the ability to generalize across: lesion types (variability in lesion count, size, and brain location), institutions (differences in MRI scanners and acquisition protocols), and demographics (patient age, sex, and other factors). Although the segmentation mask labels remained consistent (“1” for NCR (necrosis), “2” for ED (edema/invaded tissue), “3” for ET (enhancing tumor), and “0” for everything else), the prevalence of each label varied within and across tumor types, reflecting the diverse imaging characteristics of the lesions.The challenge used preoperative MRI data from BraTS 2023 tasks (1 through 5), focusing on assessing the ability of algorithms to generalize beyond individual datasets and across multiple clinical applications [11].
- Synthesis (Global)—missing MRI: ASNR-MICCAI BraTS MRI Synthesis Challenge (BraSyn): Continuing from the success of the BraSyn 2023 Challenge, the 2024 iteration maintained the goal of evaluating image synthesis methods that create realistic image contrasts from available MRI modalities to aid automated brain tumor segmentation. The BraSyn-2024 dataset, identical in task to BraSyn-2023 [11].
- Synthesis (Local)—inpainting: ASNR-MICCAI BraTS Local Synthesis of Tissue via Inpainting: The ASNR-MICCAI BraTS Local Synthesis of Tissue via Inpainting Challenge continued for BraTS 2024 with the same design, task, evaluation metrics, and ranking scheme as the previous year. This iteration introduced an additional test set of 277 patients from the BraTS Meningioma Challenge, enabling an assessment of how well algorithms generalize to other pathologies and imaging data acquired from different MRI scanners [29].
- Evaluating Augmentations for BraTS: BraTS Challenge on Relevant Augmentation Techniques: BraTS 2024 Challenge on Relevant Augmentation Techniques shared the same objectives and dataset as the BraTS 2023 Challenge on Relevant Augmentation Techniques.
- Pathology: glioblastoma has a poor prognosis, with median survival ranging from 12 to 18 months with treatment and only 4 months without. Its infiltrative nature and heterogeneous molecular and micro-environmental profiles make treatment challenging. Accurate diagnosis and assessment of tumor heterogeneity are critical for selecting effective therapies and potentially improving patient outcomes. The BraTS-Path Challenge leverages whole slide histopathology images (WSI) to enhance the understanding of glioblastoma by detecting various morpho-pathological features in digitized tissue sections. It draws on the gold-standard histopathology-based approach, which traditionally focuses on identifying features such as cellular tumor regions, necrosis, microvascular proliferation, cortical infiltration, and immune cell presence. By providing a robust dataset, the challenge aims to develop deep-learning models capable of automatically classifying these distinct tumor sub-regions with varied histological profiles. These models are designed to mimic and extend the gold-standard process, supporting more consistent diagnosis and grading, thus enhancing both research and clinical applications [32].The dataset included a retrospective, multi-institutional cohort of de novo diffuse gliomas. Expert neuropathologists annotated and segmented histological regions into patches for classification based on specific characteristics. The dataset consists of 195,000 training data points from 130 digitized tissue sections, 25,000 validation data points from 18 digitized tissue sections, and 60,000 testing data points from 40 digitized tissue sections. Nine histologic areas of interest are considered as classes [11].
- Pre-Processing Data Protocol: The standardized pre-processing protocol established by BraTS has been applied to all datasets except the following, which exhibit some slight differences:
- Task 3 Segmentation—meningioma radiotherapy: All images underwent standardized preprocessing, including conversion from DICOM and DICOM-RT to NIfTI format using dcmrtstruct2nii, followed by automated defacing with the AFNI toolbox. Cases where the AFNI defacing algorithm removed the meningioma entirely from the field of view (e.g., anterior intraorbital meningiomas) were excluded from the dataset [33].
- Task 5 Segmentation—pediatric tumors: ASNR-MICCAI BraTS Pediatrics Tumor Challenge: All mpMRI scans were processed through a three-step pipeline. First, pre-processing was carried out using the “BraTS Pipeline”, a standardized approach that is publicly available through the Cancer Imaging Phenomics Toolkit (CaPTk) and Federated Tumor Segmentation (FeTS) tool. Next, a pediatric-specific automated defacing method was applied to ensure patient anonymity. Finally, tumor subregion segmentation was completed using a pediatric autosegmentation method.It is important to note that the BraTS-PEDs 2024 dataset does not include skull stripping.
- Task 10—pathology: The preprocessing pipeline for H&E-stained FFPE tissue sections of glioblastoma multiform (GBM) was specifically designed to facilitate detailed histological analysis.(1) Patch Extraction and Standardization: Tissue sections annotated by expert neuropathologists are segmented into standardized 512 × 512-pixel patches. This size minimizes boundary noise and ensures comprehensive coverage of annotated regions.(2) Quality Control: Only high-quality sections are included, excluding those with artifacts such as tissue folding, pen markings, or glass slippage.(3) Patch Classification: Each patch is categorized based on its histologic features, which are used throughout training, validation, and testing to evaluate the challenges and accuracy of feature detection.This structured pipeline ensures high-quality data for histological studies, with each patch treated as an independent unit for comprehensive analysis [32].
- Annotation Method:
- Segmentation—adult glioma post-treatment: BraTS Adult Glioma Post Treatment Challenge: The BraTS 2024 Post-Treatment Adult Glioma Challenge builds upon the framework established in the BraTS 2021–2023 challenges by introducing modifications tailored specifically to the post-treatment context. All imaging datasets were manually annotated by one to four raters using a standardized, clinically approved protocol developed by expert neuroradiologists and radiation oncologists. Annotators followed detailed guidelines, including examples of challenging cases, to ensure consistency. For a full description of the protocol, refer to the challenge manuscript: [34].Preprocessed MRI volumes were segmented using five nnU-Net-based pre-segmentation methods. These outputs were fused using the STAPLE algorithm to generate consensus segmentations. Additionally, digital subtraction images (T1-Gd minus T1) were provided to radiologists to improve annotation accuracy.As shown in Figure 11, the annotations included the following tumor subregions: the enhancing tissue (ET—label 3); the surrounding non-enhancing FLAIR hyperintensity (SNFH—label 2); the non-enhancing tumor core (NETC—label 1), and the newly introduced resection cavity (RC—label 4). This expanded labeling scheme highlights the complexities of post-treatment imaging—such as surgical cavities and residual tumors—thereby enabling researchers to investigate regrowth patterns, therapy response, and other clinically relevant factors in greater detail. Annotations were iteratively refined and reviewed by board-certified neuroradiologists. This process continued until segmentations met the required quality standard for public release. Test data annotations underwent review by two sets of annotators and approvers to ensure inter-rater reliability [11,34].
- Segmentation—BraTS-Africa: BraTS Challenge on Sub-Sahara-Africa Adult Glioma: Same annotation protocol as BraTS-Africa Challenge 2023.
- Segmentation—meningioma radiotherapy: BraTS Meningioma Radiotherapy Challenge: For the BraTS-MEN-RT 2024 challenge, a single “target volume” label was employed, representing both the gross tumor volume (GTV) and any at-risk postoperative site. Consequently, the definition of GTV varies depending on the radiotherapy planning context:
- Preoperative setting: The target volume includes the portion of the tumor visible on T1c brain MRI.
- Postoperative setting: The target volume includes the resection bed and any residual enhancing tumor (ET) visible on T1c brain MRI.
Figure 12 provides an example of postoperative meningioma data with this target volume label, illustrating how the resection bed and any residual enhancing tumor are encompassed within the single “target volume” annotation.For cases without gross tumor volume (GTV) labels provided by the treating institution (about 10% of the dataset), an automated pre-segmentation algorithm using nnU-Net was applied. All cases, whether pre-segmented or labeled by the institution, underwent manual review and correction by a senior radiation oncology resident. Subsequently, a fellowship-trained neuroradiologist (“approver”) performed a final review to ensure data quality. Manual reviews and corrections were conducted using ITKSnap [33]. - Segmentation—brain metastases: ASNR-MICCAI BraTS Brain Metastasis Challenge: The dataset includes retrospective treatment-naive brain metastasis MRI scans, adhering to the BraTS 2023 annotation protocol.The post-treatment brain metastasis MRI scans, sourced from an external dataset, are expected to follow a five-label system that includes the necrotic core of tumor (NCR), FLAIR hyperintensity (SNFH), enhancing tumor (ET), hemorrhage (HM), and resection cavity (RC). While the detailed annotation protocol for the post-treatment cases has not yet been released, additional information will be provided in the forthcoming challenge manuscript, with updates available on the official challenge website (Synapse.org) [11].
- Segmentation—pediatric tumors: ASNR-MICCAI BraTS Pediatrics Tumor Challenge: Following pre-processing and defacing, a pediatric automated segmentation method was employed to preliminarily segment tumors into four main subregions: enhancing tumor (ET; label 1), non-enhancing tumor (NET; label 2), cystic component (CC; label 3), and peritumoral edema (ED; label 4).The automated segmentation outputs were manually revised by volunteer neuroradiology experts with varying levels of experience, following established annotation guidelines. Refinements were conducted using ITK-SNAP software. Afterward, the refined segmentations were reviewed by three board-certified neuroradiologists. Cases deemed incomplete or inaccurate were returned to the annotators for further adjustments. This iterative review process continued until the segmentations were approved by the neuroradiologists [31]. Note that for the BraTS-PEDs 2024 challenge, the tumor sub-regions considered for evaluation returned to the original four, as initially planned for the BraTS-PEDs 2023 challenge but not implemented that year (see left image in Figure 10).
- Segmentation—generalizability: ASNR-MICCAI BraTS Generalizability Across Brain Tumors: In BraTS-GoAT, preoperative MRI data from the BraTS 2023 challenge is utilized, specifically from tasks 1, 2, 3, 4, and 5. The sub-regions considered for evaluation are the enhancing tumor (ET), the tumor core (TC), and the whole tumor (WT). The provided segmentation labels have values of: “1” for NCR (necrosis), “2” for ED (edema/invaded tissue), “3” for ET (enhancing tumor), and “0” for everything else [11]. Details regarding the annotation protocol have not yet been disclosed.
- Synthesis (Global)—missing MRI: ASNR-MICCAI BraTS MRI Synthesis Challenge (BraSyn): Same as BraSyn 2023 Challenge.
- Synthesis (Local)—inpainting: ASNR-MICCAI BraTS Local Synthesis of Tissue via Inpainting: Same as BraTS Local Inpainting 2023 Challenge.
- Evaluating Augmentations for BraTS: BraTS Challenge on Relevant Augmentation Techniques: Same as BraTS Challenge on Relevant Augmentation 2023.
- Pathology: The annotation process adhered to a clinically approved protocol, defined by expert neuropathologists, which provided detailed instructions on segmenting each histologic feature. For further details, refer to the challenge manuscript: [32]. Each case was assigned to an annotator–approver pair. To assess inter-rater variability, three cases were annotated by all annotators. Annotators varied in experience and rank, while approvers were highly experienced, board-certified neuropathologists with over 10 years of expertise.Once annotations were completed, they were reviewed by the approvers, who evaluated their quality alongside the corresponding tissue sections. If the initial annotations on a tissue section produced fewer than approximately 1500 patches, that section was returned to the annotators for further refinement. This iterative process continued until the approvers approved the annotations. The segmented regions were then divided into patches and classified based on specific histologic features. This established a classification task focused on accurately identifying patches with distinct morphological characteristics [32].Histologic areas of interest for classification included the following:(1) Presence of cellular tumor (CT);(2) Pseudopalisading necrosis (PN);(3) Areas abundant in microvascular proliferation (MP);(4) Geographic necrosis (NC);(5) Infiltration into the cortex (IC);(6) Penetration into white matter (WM);(7) Leptomeningeal infiltration (LI);(8) Regions dense with macrophages (DMs);(9) Presence of lymphocytes (PLs).An example of these annotated histological sub-regions is illustrated in Figure 13, which displays a whole slide histopathology image (WSI) from the BraTS-Path 2024 Challenge. The figure delineates various glioblastoma (GBM) sub-regions with distinct colors, capturing critical pathological features. These comprehensive annotations are essential for training machine learning models, facilitating more precise and automated histopathological analysis of brain tumors and improving diagnostic accuracy in neuro-oncology.
- Multi-Center Imaging Data Acquisition Details: For each task, a detailed list of contributors and their affiliations is available in the respective manuscripts or in the complete contributor list here: [11].
- Segmentation—adult glioma post-treatment: BraTS Adult Glioma Post Treatment Challenge: BraTS mpMRI scans come from multiple contributing institutions using various scanners and clinical protocols. Data from seven institutions contributed to the dataset, with locations across the United States and one in Germany.
- Segmentation—BraTS-Africa: BraTS Challenge on Sub-Sahara-Africa Adult Glioma: The BraTS-Africa 2024 dataset saw an expansion in the number of contributors compared to the 2023 edition, reflecting a substantial enlargement of the dataset. This increase includes new collaborations from additional healthcare institutions across several African countries, including Tanzania and Ghana.
- Segmentation—meningioma radiotherapy: BraTS Meningioma Radiotherapy Challenge: 750 radiotherapy planning T1c brain MRI scans were contributed from seven academic medical centers across the United States and the United Kingdom.
- Segmentation—brain metastases: ASNR-MICCAI BraTS Brain Metastasis Challenge: Contributions to the dataset came from ten institutions located across the United States, Germany, and Egypt.
- Segmentation—pediatric tumors: ASNR-MICCAI BraTS Pediatrics Tumor Challenge: The image acquisition protocols and MRI equipment vary between institutions, leading to differences in image quality within the provided cohort. The dataset from the CBTN-CONNECT-DIPGr-ASNR-MICCAI BraTS-PEDs initiative includes contributions from a total of eight institutions, all located in the United States.
- Segmentation—generalizability: ASNR-MICCAI BraTS Generalizability Across Brain Tumors: The data contributors include those involved in challenges 1, 2, 3, 4, and 5 from the 2023 edition. This collaborative effort provides a comprehensive and diverse dataset, supporting the development of models with improved generalizability across various brain tumor types.
- Synthesis (Global)—missing MRI: ASNR-MICCAI BraTS MRI Synthesis Challenge (BraSyn): Same as BraTS 2021.
- Synthesis (Local)—inpainting: ASNR-MICCAI BraTS Local Synthesis of Tissue via Inpainting: Same as BraTS 2021.
- Evaluating Augmentations for BraTS: BraTS Challenge on Relevant Augmentation Techniques: Same as BraTS 2021.
- Pathology: Contributions to the dataset came from ten institutions across the United States and one in Italy.
Table 3 provides a concise summary of each challenge’s main characteristics—such as the tasks, MRI modalities employed, number of classes, contributing institutions, and whether it includes data from low- and middle-income countries (LMICs).
4.12. BraTS Challenge 2025 Overview
- Pre- and Post-Treatment Adult Glioma;
- Preoperative Meningioma Tumor Segmentation;
- Pre-Radiotherapy Intracranial Meningioma;
- Pre- and Post-Treatment Brain Metastases;
- Brain Glioma in the Underserved Sub-Saharan African Patient Population;
- Pre-Treatment Pediatric Tumor Patients in Partnership with Multiple Related Societies;
- Generalizability of Segmentation Methods Across Tumors;
- MRI Global Synthesis;
- MRI Local Inpainting;
- Assessing the Heterogeneous Histologic Landscape of Glioma;
- Predicting the Tumor Response During Therapy.
5. BraTS Challenge Results over the Years: SOTA Development
- 2012: The BraTS challenge started with models achieving Dice scores between 0.14 and 0.70 for whole tumors (WT) and 0.09–0.37 for tumor core (TC). The models were mainly based on Random Forests, logistic regression, and Markov Random Fields. The best-performing model was a Random Forest-based approach, achieving a Dice score of 0.70 and 0.25 for the whole tumor and tumor core, respectively.
- 2013: Dice scores improved, ranging from 0.71 to 0.87 for whole tumors (WT), from 0.46 to 0.78 for tumor core (TC), and from 0.52 to 0.74 for enhancing tumor (ET). This year saw a continuation of the success of RF-based methods that utilized advanced texture features and multimodal MRI data.
- 2014: Introduced deep convolutional networks alongside traditional RF methods, marking the beginning of deep learning’s influence in medical image segmentation. U-Net, a CNN architecture, began to emerge as a central model, with top models reaching Dice scores up to 0.87 for whole tumors.
- 2015: CNNs dominated, driven by their high segmentation accuracy. The InputCascadeCNN, a sophisticated 2D CNN architecture, performed well on the BraTS 2013 dataset with Dice scores of 0.88, 0.79, and 0.73 for whole tumor (WT), tumor core (TC), and enhancing tumor (ET), respectively. Architectural enhancements included residual connections and densely connected layers.
- 2016: DeepMedic, an 11-layer 3D CNN with dual pathways and residual connections, led the challenge, achieving Dice scores of 0.89, 0.76, and 0.72 for whole tumor (WT), tumor core (TC), and enhancing tumor (ET), respectively. This solidified the position of 3D CNNs in volumetric segmentation tasks.
- 2017: Over 50 papers were submitted, predominantly leveraging U-Net and DeepMedic architectures. Ensemble methods, like EMMA (Ensemble of Multiple Models and Architectures), became prominent. EMMA, comprising two different DeepMedics, two fully convolutional networks, and a U-Net, won with Dice scores of 0.90, 0.82, and 0.75 for whole tumor (WT), tumor core (TC), and enhancing tumor (ET), respectively, on blinded validation.
- 2018: The challenge witnessed a dominant use of CNNs, particularly U-net architectures and their ensembles, which formed the basis of the top submissions. A notable trend was the integration of advanced CNN architectures like ResNet and DenseNet. The top-ranked model employed an asymmetric encoder–decoder architecture with a larger encoder to extract more features, complemented by a variational auto-encoder branch for input reconstruction. This innovative approach, alongside an ensemble of 10 individually trained models, led to impressive Dice scores of 0.91 for whole tumor (WT), 0.86 for tumor core (TC), and 0.82 for enhancing tumor (ET). The methods employed underscored a shift towards more sophisticated, ensemble-based strategies [16].
- 2019: The Two-Stage Cascaded U-Net introduced a coarse-to-fine segmentation approach, achieving Dice scores of 0.88796 for whole tumors (WT), 0.83697 for tumor core (TC), and 0.83267 for enhancing tumor (ET). This model effectively balanced precision across tumor subregions [36].
- 2020: The nnU-Net framework dominated, employing BraTS-specific optimizations such as batch Dice loss, aggressive data augmentation, and post-processing tailored to handle small enhancing tumor (ET) regions. Dice scores on the test dataset were 0.8895 for whole tumors (WT), 0.8506 for tumor core (TC), and 0.8203 for enhancing tumors (ET). The ensemble approach balanced performance across tumor subregions [37].
- 2021: The winning model extended nnU-Net, incorporating a larger network architecture, group normalization, and axial attention in the decoder. It achieved an impressive Dice scores of 0.9275 for whole tumor (WT), 0.8781 for tumor core (TC), and 0.8451 for enhancing tumors (ET) [38]. The significant improvement in Dice scores from 2020 to 2021 can likely be attributed to the considerable expansion of the dataset that year, which provided a richer variety of training examples. In 2021, pioneering research introduced few-shot and zero-shot learning approaches to the BraTS dataset. For example, Zhang et al. proposed a self-supervised tumor segmentation method based on layer decomposition that achieved a Dice score of around 71.6% on BraTS2018 for whole tumor segmentation in a zero-shot setting—that is, without any task-specific fine-tuning. With limited annotated data (e.g., 10%, 20%, or 40% of the training set), the method consistently outperformed other self-supervised approaches, demonstrating robust performance in low-data regimes. When fully supervised fine-tuning is applied using 100% of the labeled data, the Dice score improves to about 86.1%. These comparisons underscored the potential of zero-shot and few-shot strategies to significantly reduce reliance on extensive manual annotations while maintaining strong segmentation performance [39].
- 2022: The winning ensemble combined DeepSeg, an improved nnU-Net, and DeepSCAN architectures, utilizing the STAPLE method for final predictions. Dice scores on the BraTS 2021 test dataset reached 0.9294 for whole tumors (WT), 0.8788 for tumor core (TC), and 0.8803 for enhancing tumors (ET). The model excelled on the Sub-Saharan Africa dataset, achieving Dice scores of 0.9737 for whole tumors, showcasing its adaptability to underrepresented populations. However, performance on the pediatric dataset highlighted the need for further specialization in this domain [40].
- 2023: In 2023, the BraTS challenge saw significant advancements in various tasks: For task 1: Adult Glioma Segmentation, an ensemble comprising nnU-Net, Swin UNETR, and the BraTS 2021 winning model excelled, utilizing advanced synthetic data augmentation techniques such as GANs and registration. This approach not only harnessed the strengths of CNNs and transformers but also achieved impressive Dice score results of 0.9005 for whole tumor (WT), 0.8673 for tumor core (TC), 0.8509 for enhancing tumor (ET), with an average of 0.8729 [41].
- Notably a team topped several categories, securing first place in Meningioma, BraTS-Africa, and Brain Metastases, and achieving second in Adult Glioma and Pediatric Tumors. Their achievements in Meningioma included the highest DSC for ET at 0.899, TC at 0.904, and WT at 0.871, demonstrating the efficacy of their model across diverse tumor types and complexities. The success of their model was the use of the AutoSeg3D framework, a flexible, Pytorch-based platform optimized to scale across GPUs. It incorporated advanced training techniques, including five-fold training with models such as SegResNet, DiNTS, and SwinUNETR, with SegResNet being particularly pivotal, chosen for its accuracy and suitability for complex tasks [42].
- The winner of the Pediatric Tumor Challenge employed a model ensemble technique. They addressed the task using an ensemble of nnU-Net and Swin UNETR, with a strategic focus on maximizing the effectiveness of segmentation across multiple tumor sub-regions. This method involved tailored ensemble strategies for different tumor regions, enhancing both the accuracy and robustness of the segmentation results [43].
- The BraSyn Challenge for Synthesizing Missing MRI Sequences was addressed by two groups. The winning group explored multiple advanced loss functions to improve the quality and realism of synthesized MRI images. Their innovative approach, which combined multiple loss functions such as L1 norm, masked L1 loss, adversarial loss, and others, significantly enhanced the synthesis quality. This was evidenced by median Dice scores of 0.72 for ET, 0.78 for TC, and 0.44 for WT, with an overall mean SSIM of 0.817 for the test set [44].
- The winning team of the Inpainting Challenge addressed the task using a 3D U-Net model optimized with MAE and SSIM loss functions, which yielded robust performance metrics: a median similarity index measure (SSIM) of 0.91, a median root mean square error (RMSE) of 0.07, and a median peak signal-to-noise ratio (PSNR) of 23.59. This task demonstrated the specialized yet critical role of inpainting in biomedical image analysis, highlighting the potential for significant advancements in diagnostic imaging techniques [29].
- 2024: In Task 1: Post-Treatment Glioma Segmentation, the same team that topped the rankings in Task 1 2023 continued their success by utilizing a sophisticated strategy with neural networks, specifically nnU-Net, MedNeXt, and Swin-UNETR. These networks were enhanced with synthetic data augmentation using GliGANs to boost tumor variability and balance class differences between healthy and diseased tissue. This strategy led to a broad improvement in the model’s generalization capabilities. The ensemble of models, including those trained on both real and synthetic data, produced balanced DSC validation results of 0.7557 for enhancing tumor (ET), 0.7868 for non-enhancing tumor core (NETC), 0.7053 for resection cavity (RC), 0.8704 for surrounding non-enhancing FLAIR hyperintensity (SNFH), 0.7500 for tumor core (TC), and 0.8734 for whole tumor (WT) [45].
- The winning model for the BraTS Africa 2024 challenge used an ensemble approach combining nnU-Net and MedNeXt, adapted for the Sub-Saharan context with limited data quality and quantity. This involved a stratified fine-tuning strategy using both BraTS2023 Adult Glioma and BraTS-Africa datasets, focusing on radiomic analysis to refine the training process. The ensemble method and adaptive post-processing led to impressive validation test Dice scores of 0.870 for enhancing tumor (ET), 0.865 for tumor core (TC), and 0.926 for whole tumor (WT) [46].
- The winning team of Task 7: Synthesis (Global)—missing MRI, used a novel two-stage model that significantly improved the synthesis of brain MRI images compared to 2023 results. Initially, the model synthesized MRI images from 2D slices using a new intensity encoding method, followed by a ‘Refiner’ stage using 3D volumetric data to enhance image quality. This approach not only mimicked original MRI sequences closely but also enhanced detail and accuracy in tumor depiction, achieving on a test set an SSIM of 0.8183, and Dice scores of 0.8399 for whole tumor (WT), 0.7133 for enhancing tumor (ET), and 0.7572 for tumor core (TC) [47].
6. Datasets Growing Complexity over the Years
7. Dataset Usage and Impact on Research: Potential Clinical Practice
8. Challenges and Future Perspectives
9. Conclusions
- BraTS Dataset Growth: Over a decade of challenges has seen a remarkable increase in dataset size, complexity, and diversity, fostering continual improvements in segmentation accuracy and clinical relevance. This growth is crucial for data-intensive deep learning methods.
- Standardized Pre-Processing Protocol: Introducing a uniform pre-processing pipeline enabled global data collection from institutions worldwide, ensuring diverse yet high-quality datasets. However, these standardized steps may also limit performance in real-world scenarios where protocols deviate from BraTS guidelines. Future research can leverage these pipelines to build larger, more consistent repositories while also exploring methods to maintain robustness under varying acquisition conditions.
- Standardized Annotation Protocol: Refined annotation methods and multi-rater consensus have enhanced the granularity and reliability of tumor segmentation. These consistent labels across different institutions reduce inter-observer variability and ensure more robust model training and evaluation.
- Inclusion and Representativeness: Recent expansions incorporate underrepresented populations (e.g., Sub-Saharan Africa, pediatric cases), new tumor types (meningiomas, metastases), and post-treatment datasets, supporting algorithmic generalization and advancing global health equity.
- Clinical Translation: Beyond boosting segmentation performance, these standardized datasets aim to streamline clinical workflows by saving clinician’s time and improving diagnostic and therapeutic planning. The datasets reinforce personalized treatment strategies, real-time monitoring, and post-treatment evaluation, aligning with the principles of precision medicine.
- Challenges and Limitations: Despite the substantial progress, obstacles like missing data, heterogeneous imaging protocols, and ensuring cross-institutional generalizability persist. Some BraTS subsets also remain relatively small and would benefit from further expansion.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- SEER. Brain and Other Nervous System Cancer—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/brain.html (accessed on 1 December 2024).
- Bakas, S.; Reyes, M.; Jakab, A.; Bauer, S.; Rempfler, M.; Crimi, A.; Shinohara, R.T.; Berger, C.; Ha, S.M.; Rozycki, M.; et al. Identifying the Best Machine Learning Algorithms for Brain Tumor Segmentation, Progression Assessment, and Overall Survival Prediction in the BRATS Challenge. arXiv 2019, arXiv:1811.02629v3. [Google Scholar]
- Baid, U.; Ghodasara, S.; Mohan, S.; Bilello, M.; Calabrese, E.; Colak, E.; Farahani, K.; Kalpathy-Cramer, J.; Kitamura, F.C.; Pati, S.; et al. The RSNA-ASNR-MICCAI BraTS 2021 Benchmark on Brain Tumor Segmentation and Radiogenomic Classification. arXiv 2021, arXiv:2107.02314v2. [Google Scholar]
- Hussain, S.; Anwar, S.M.; Majid, M. MRI-based brain tumor segmentation using FPGA-accelerated neural network. BMC Bioinform. 2021, 22, 421. [Google Scholar] [CrossRef]
- Liu, J.; Li, M.; Wang, J.; Wu, F.; Liu, T.; Pan, Y. A survey of MRI-based brain tumor segmentation methods. Tsinghua Sci. Technol. 2014, 19, 578–595. [Google Scholar] [CrossRef]
- Karim, S.; Tong, G.; Yu, Y.; Laghari, A.A.; Khan, A.A.; Ibrar, M.; Mehmood, F. Developments in Brain Tumor Segmentation Using MRI: Deep Learning Insights and Future Perspectives. IEEE Access 2024, 12, 26875–26895. [Google Scholar] [CrossRef]
- Ghosh, A.; Chakraborty, S. Efficient Brain Tumor Segmentation with Mamba. In Proceedings of the 2024 7th International Conference of Computer and Informatics Engineering (IC2IE), Bali, Indonesia, 12–13 September 2024; IEEE: Piscataway, NJ, USA, 2024. [Google Scholar] [CrossRef]
- Kose, K. Physical and technical aspects of human magnetic resonance imaging: Present status and 50 years historical review. Adv. Phys. X 2021, 6, 1885310. [Google Scholar] [CrossRef]
- Kabasawa, H. MR Imaging in the 21st Century: Technical Innovation over the First Two Decades. Magn. Reson. Med. Sci. 2021, 21, 71–82. [Google Scholar] [CrossRef]
- BraTS 2023 Challenges. Available online: https://www.synapse.org/Synapse:syn51156910/wiki/ (accessed on 15 September 2024).
- BraTS 2024 Challenges. Available online: https://www.synapse.org/Synapse:syn53708249/wiki/626323 (accessed on 15 September 2024).
- BraTS 2012 Challenge on Multimodal Brain Tumor Segmentation. Available online: http://www2.imm.dtu.dk/projects/BRATS2012/index.html (accessed on 15 September 2024).
- Menze, B.H.; Jakab, A.; Bauer, S.; Kalpathy-Cramer, J.; Farahani, K.; Kirby, J.; Burren, Y.; Porz, N.; Slotboom, J.; Wiest, R.; et al. The Multimodal Brain Tumor Image Segmentation Benchmark (BRATS). IEEE Trans. Med. Imaging 2015, 34, 1993–2024. [Google Scholar] [CrossRef]
- Narmatha, C.; Eljack, S.M.; Tuka, A.A.R.M.; Manimurugan, S.; Mustafa, M. A hybrid fuzzy brain-storm optimization algorithm for the classification of brain tumor MRI images. J. Ambient. Intell. Humaniz. Comput. 2020. [CrossRef]
- Fernandez, X.T.; Warfield, S.K. Automatic Brain Tumor Segmentation based on a Coupled Global-Local Intensity Bayesian Model. In Proceedings of the MICCAI BraTS 2012, Nice, France, 1 October 2012; Available online: https://www2.imm.dtu.dk/projects/BRATS2012/proceedingsBRATS2012.pdf (accessed on 15 September 2024).
- Ghaffari, M.; Sowmya, A.; Oliver, R. Automated Brain Tumor Segmentation Using Multimodal Brain Scans: A Survey Based on Models Submitted to the BraTS 2012–2018 Challenges. IEEE Rev. Biomed. Eng. 2020, 13, 156–168. [Google Scholar] [CrossRef]
- BraTS 2017 Challenge on Multimodal Brain Tumor Segmentation. Available online: https://www.med.upenn.edu/sbia/brats2017/registration.html (accessed on 15 September 2024).
- Bakas, S.; Akbari, H.; Sotiras, A.; Bilello, M.; Rozycki, M.; Kirby, J.S.; Freymann, J.B.; Farahani, K.; Davatzikos, C. Advancing The Cancer Genome Atlas glioma MRI collections with expert segmentation labels and radiomic features. Sci. Data 2017, 4, 170117. [Google Scholar] [CrossRef] [PubMed]
- BraTS 2018 Challenge on Multimodal Brain Tumor Segmentation. Available online: https://www.med.upenn.edu/sbia/brats2018/registration.html (accessed on 15 September 2024).
- BraTS 2019 Challenge on Multimodal Brain Tumor Segmentation. Available online: https://www.med.upenn.edu/cbica/brats2019/registration.html (accessed on September 2024).
- BraTS 2020 Challenge on Multimodal Brain Tumor Segmentation. Available online: https://www.med.upenn.edu/cbica/brats2020/ (accessed on 15 September 2024).
- RSNA-ASNR-MICCAI BraTS Challenge 2021. Available online: https://www.synapse.org/Synapse:syn25829067/wiki/610863 (accessed on 15 September 2024).
- Bakas, S.; Farahani, K.; Linguraru, M.G.; Anazodo, U.; Carr, C.; Flanders, A.; Prevedello, L.M.; Kitamura, F.C.; Kalpathy-Cramer, J.; Mongan, J.; et al. The Brain Tumor Segmentation Challenge (2022 Continuous Updates & Generalizability Assessment): Structured Description of the Challenge Design. 2022. Available online: https://zenodo.org/records/6362180 (accessed on 15 September 2024).
- Synapse. Brain Tumor Segmentation Challenge (BraTS) Continuous Evaluation. Available online: https://www.synapse.org/Synapse:syn27046444/wiki/616571 (accessed on 15 September 2024).
- Adewole, M.; Rudie, J.D.; Gbadamosi, A.; Toyobo, O.; Raymond, C.; Zhang, D.; Omidiji, O.; Akinola, R.; Suwaid, M.A.; Emegoakor, A.; et al. The Brain Tumor Segmentation (BraTS) Challenge 2023: Glioma Segmentation in Sub-Saharan Africa Patient Population (BraTS-Africa). arXiv 2023, arXiv:2305.19369v1. [Google Scholar]
- Moawad, A.W.; Janas, A.; Baid, U.; Ramakrishnan, D.; Saluja, R.; Ashraf, N.; Jekel, L.; Amiruddin, R.; Adewole, M.; Albrecht, J.; et al. The Brain Tumor Segmentation (BraTS-METS) Challenge 2023: Brain Metastasis Segmentation on Pre-treatment MRI. arXiv 2024, arXiv:2306.00838v2. [Google Scholar]
- Kazerooni, A.F.; Khalili, N.; Liu, X.; Haldar, D.; Jiang, Z.; Anwar, S.M.; Albrecht, J.; Adewole, M.; Anazodo, U.; Anderson, H.; et al. The Brain Tumor Segmentation (BraTS) Challenge 2023: Focus on Pediatrics (CBTN-CONNECT-DIPGR-ASNR-MICCAI BraTS-PEDs). arXiv 2024, arXiv:2305.17033v7. [Google Scholar]
- Pati, S.; Baid, U.; Edwards, B.; Sheller, M.J.; Foley, P.; Anthony Reina, G.; Thakur, S.; Sako, C.; Bilello, M.; Davatzikos, C.; et al. The federated tumor segmentation (FeTS) tool: An open-source solution to further solid tumor research. Phys. Med. Biol. 2022, 67, 20. [Google Scholar] [CrossRef]
- Kofler, F.; Meissen, F.; Steinbauer, F.; Graf, R.; Ehrlich, S.K.; Reinke, A.; Oswald, E.; Waldmannstetter, D.; Hoelzl, F.; Horvath, I.; et al. The Brain Tumor Segmentation (BraTS) Challenge: Local Synthesis of Healthy Brain Tissue via Inpainting. arXiv 2024, arXiv:2305.08992v3. [Google Scholar]
- LaBella, D.; Adewole, M.; Alonso-Basanta, M.; Altes, T.; Anwar, S.M.; Baid, U.; Bergquist, T.; Bhalerao, R.; Chen, S.; Chung, V.; et al. ASNR-MICCAI Brain Tumor Segmentation (BraTS) Challenge 2023: Intracranial Meningioma. arXiv 2023, arXiv:2305.07642v1. [Google Scholar]
- Kazerooni, A.F.; Khalili, N.; Liu, X.; Gandhi, D.; Jiang, Z.; Anwar, S.M.; Albrecht, J.; Adewole, M.; Anazodo, U.; Anderson, H.; et al. The Brain Tumor Segmentation in Pediatrics (BraTS-PEDs) Challenge: Focus on Pediatrics (CBTN-CONNECT-DIPGR-ASNR-MICCAI BraTS-PEDs). arXiv 2024, arXiv:2404.15009v4. [Google Scholar]
- Bakas, S.; Thakur, S.P.; Faghani, S.; Moassefi, M.; Baid, U.; Chung, V.; Pati, S.; Innani, S.; Baheti, B.; Albrecht, J.; et al. BraTS-Path Challenge: Assessing Heterogeneous Histopathologic Brain Tumor Sub-regions. arXiv 2024, arXiv:2405.10871v1. [Google Scholar]
- LaBella, D.; Schumacher, K.; Mix, M.; Leu, K.; McBurney-Lin, S.; Nedelec, P.; Villanueva-Meyer, J.; Shapey, J.; Vercauteren, T.; Chia, K.; et al. Brain Tumor Segmentation (BraTS) Challenge 2024: Meningioma Radiotherapy Planning Automated Segmentation. arXiv 2024, arXiv:2405.18383v2. [Google Scholar]
- de Verdier, M.C.; Saluja, R.; Gagnon, L.; LaBella, D.; Baid, U.; Tahon, N.H.; Foltyn-Dumitru, M.; Zhang, J.; Alafif, M.; Baig, S.; et al. The 2024 Brain Tumor Segmentation (BraTS) Challenge: Glioma Segmentation on Post-treatment MRI. arXiv 2024, arXiv:2405.18368v1. [Google Scholar]
- Synapse.BraTS-Lighthouse 2025 Challenge. Available online: https://www.synapse.org/Synapse:syn64153130/wiki/ (accessed on 1 March 2025).
- Jiang, Z.; Ding, C.; Liu, M.; Tao, D. Two-Stage Cascaded U-Net: 1st Place Solution to BraTS Challenge 2019 Segmentation Task. In Brainlesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries: 5th International Workshop, BrainLes 2019, Held in Conjunction with MICCAI 2019, Shenzhen, China, 17 October 2019; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Isensee, F.; Jäger, P.F.; Full, P.M.; Vollmuth, P.; Maier-Hein, K.H. nnU-Net for Brain Tumor Segmentation. arXiv 2020, arXiv:2011.00848v1. [Google Scholar]
- Luu, H.M.; Park, S.H. Extending nn-UNet for brain tumor segmentation. arXiv 2021, arXiv:2112.04653. [Google Scholar]
- Zhang, X.; Xie, W.; Huang, C.; Wang, Y.; Zhang, Y.; Chen, X.; Tian, Q. Self-supervised Tumor Segmentation through Layer Decomposition. arXiv 2021, arXiv:2109.03230v3. [Google Scholar]
- Zeineldin, R.A.; Karar, M.E.; Burgert, O.; Mathis-Ullrich, F. Multimodal CNN Networks for Brain Tumor Segmentation in MRI: A BraTS 2022 Challenge Solution. arXiv 2022, arXiv:2212.09310. [Google Scholar]
- Ferreira, A.; Solak, N.; Li, J.; Dammann, P.; Kleesiek, J.; Alves, V.; Egger, J. How we won BraTS 2023 Adult Glioma challenge? Just faking it! Enhanced Synthetic Data Augmentation and Model Ensemble for brain tumour segmentation. arXiv 2024, arXiv:2402.17317v2. [Google Scholar]
- LaBella, D.; Baid, U.; Khanna, O.; McBurney-Lin, S.; McLean, R.; Nedelec, P.; Rashid, A.; Tahon, N.H.; Altes, T.; Bhalerao, R.; et al. Analysis of the BraTS 2023 Intracranial Meningioma Segmentation Challenge. arXiv 2024, arXiv:2405.09787v1. [Google Scholar] [CrossRef]
- Capellán-Martín, D.; Jiang, Z.; Parida, A.; Liu, X.; Lam, V.; Nisar, H.; Tapp, A.; Elsharkawi, S.; Ledesma-Carbayo, M.J.; Anwar, S.M.; et al. Model Ensemble for Brain Tumor Segmentation in Magnetic Resonance Imaging. arXiv 2024, arXiv:2409.08232v1. [Google Scholar]
- Baltruschat, I.M.; Janbakhshi, P.; Lenga, M. BraSyn 2023 challenge: Missing MRI synthesis and the effect of different learning objectives. arXiv 2024, arXiv:2403.07800v2. [Google Scholar]
- Ferreira, A.; Jesus, T.; Puladi, B.; Kleesiek, J.; Alves, V.; Egger, J. Improved Multi-Task Brain Tumour Segmentation with Synthetic Data Augmentation. arXiv 2024, arXiv:2411.04632v1. [Google Scholar]
- Parida, A.; Capellán-Martín, D.; Jiang, Z.; Tapp, A.; Liu, X.; Anwar, S.M.; Ledesma-Carbayo, M.J.; Linguraru, M.G. Adult Glioma Segmentation in Sub-Saharan Africa using Transfer Learning on Stratified Finetuning Data. arXiv 2024, arXiv:2412.04111v1. [Google Scholar]
- Cho, J.; Park, S.; Park, J. Two-Stage Approach for Brain MR Image Synthesis: 2D Image Synthesis and 3D Refinement. arXiv 2024, arXiv:2410.10269v2. [Google Scholar]
- Cox, J.; Liu, P.; Stolte, S.E.; Yang, Y.; Liu, K.; See, K.B.; Ju, H.; Fang, R. BrainSegFounder: Towards Foundation Models for Neuroimage Segmentation. arXiv 2024, arXiv:2406.10395v3. [Google Scholar] [CrossRef] [PubMed]

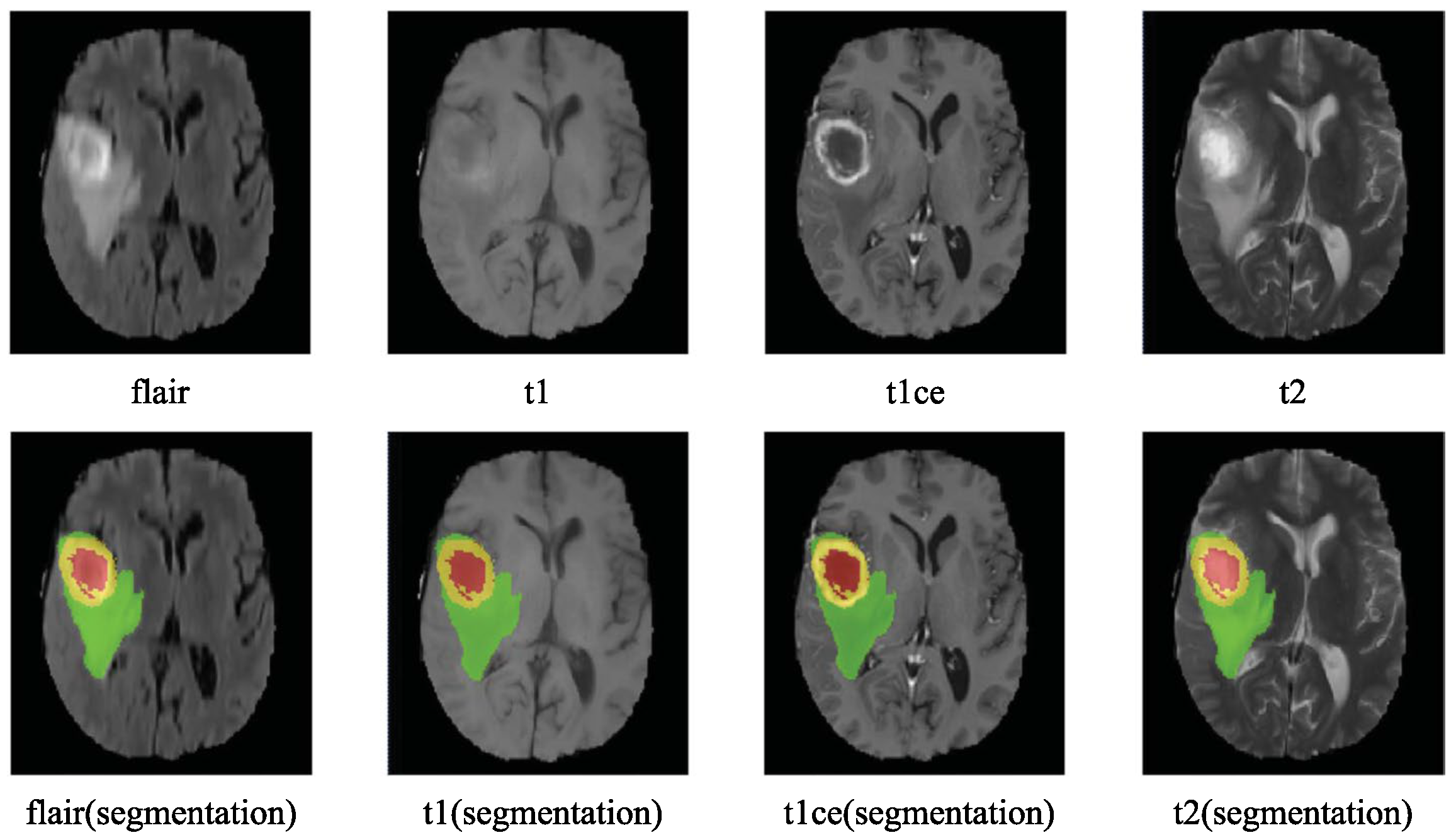
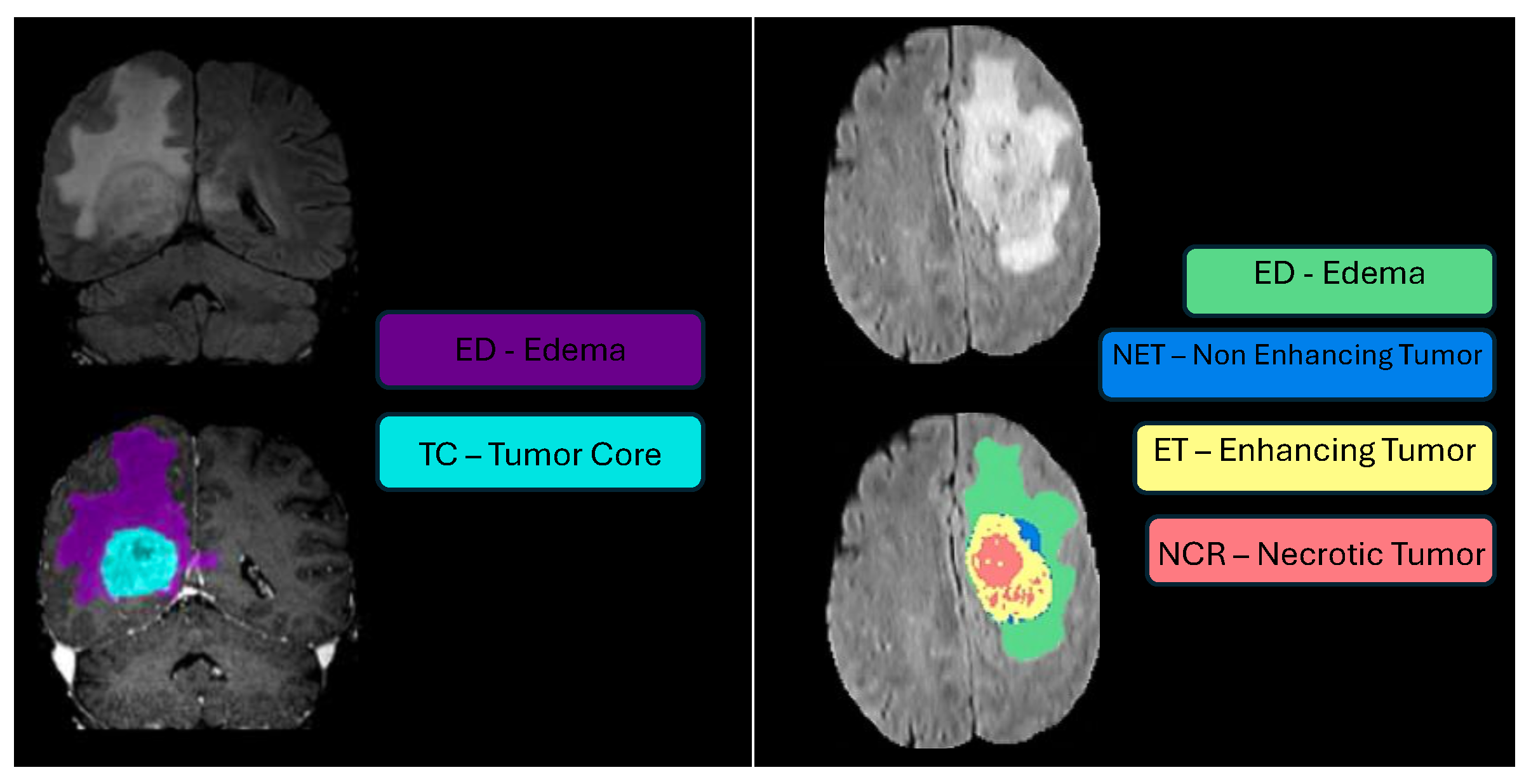


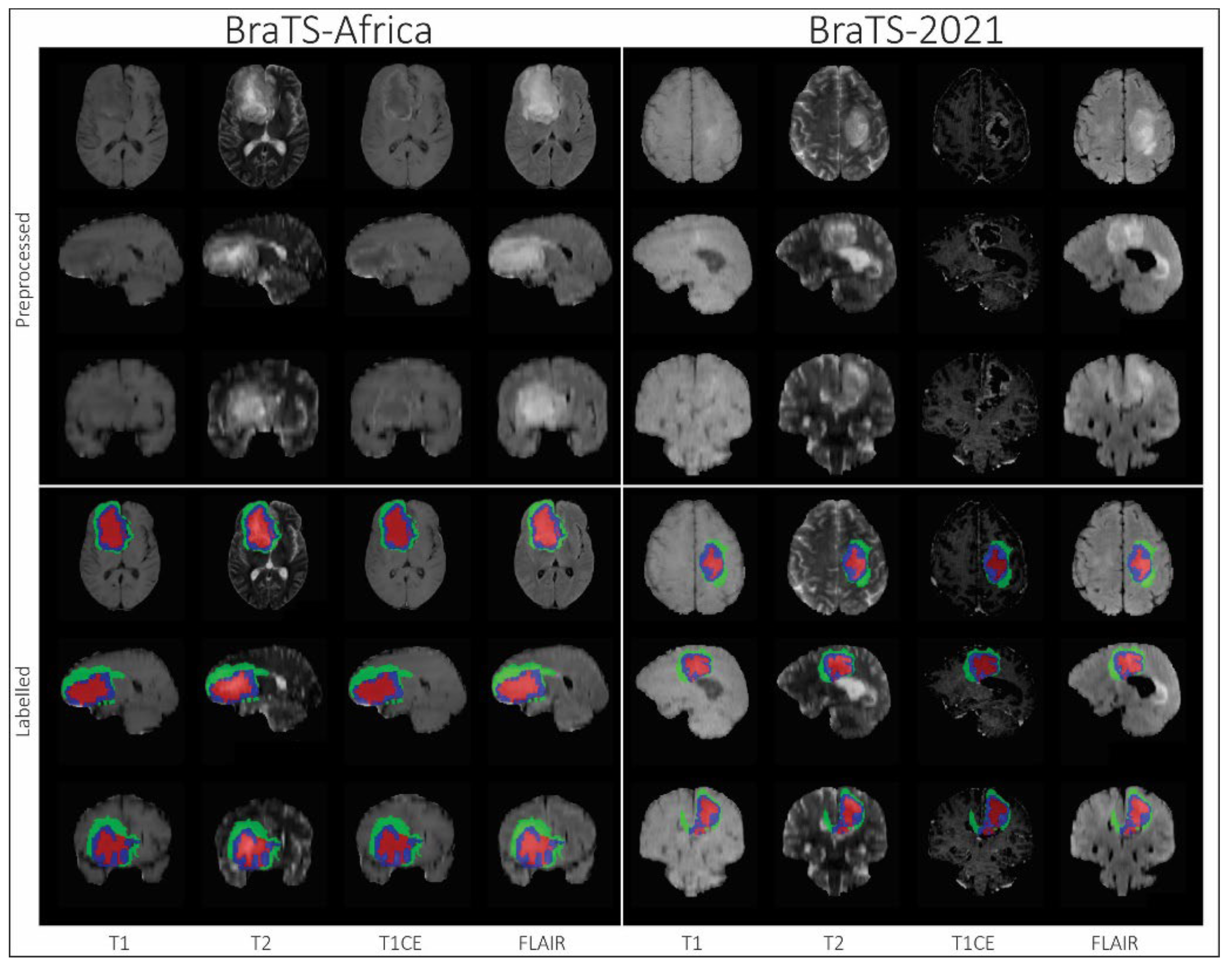

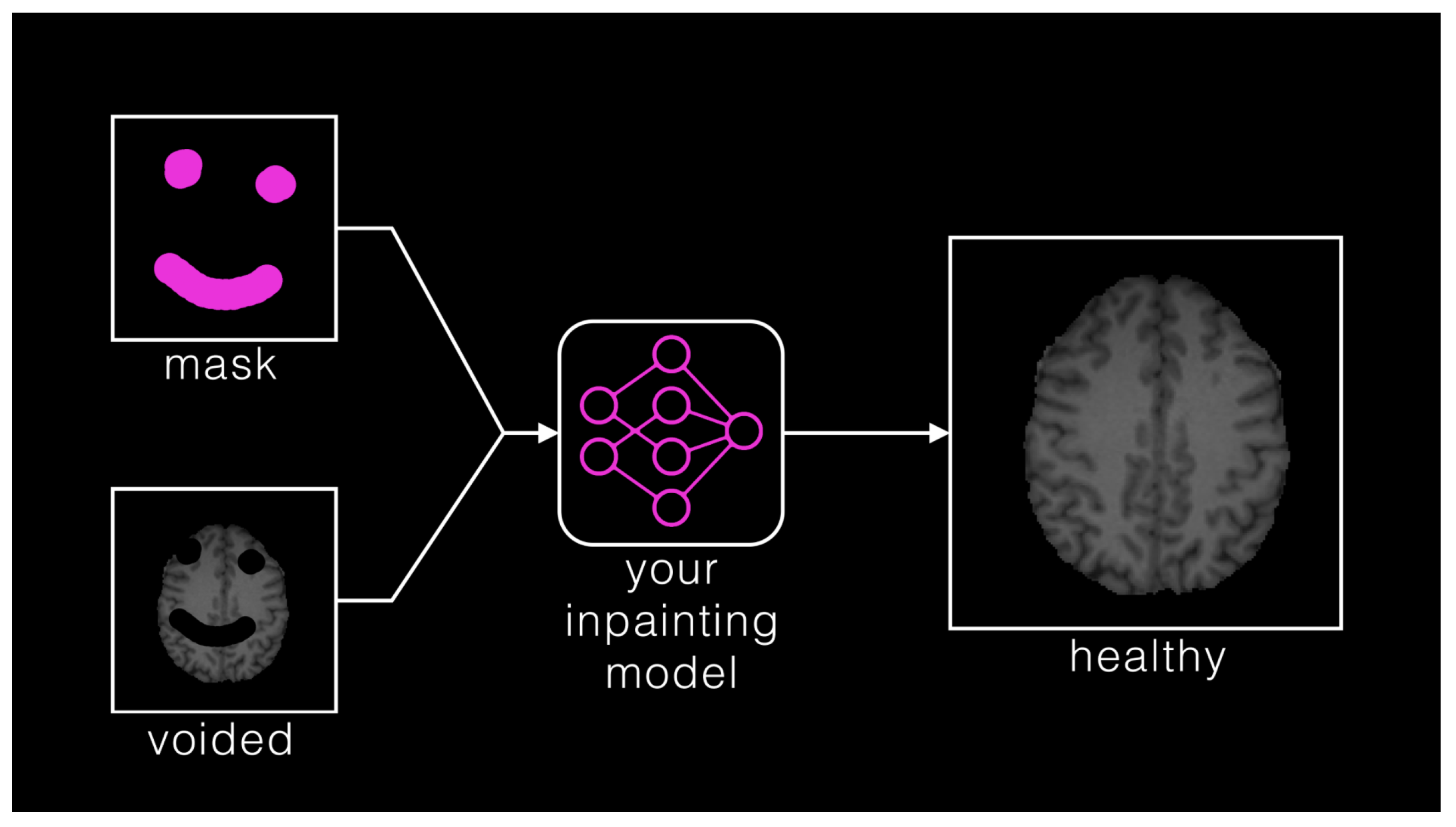



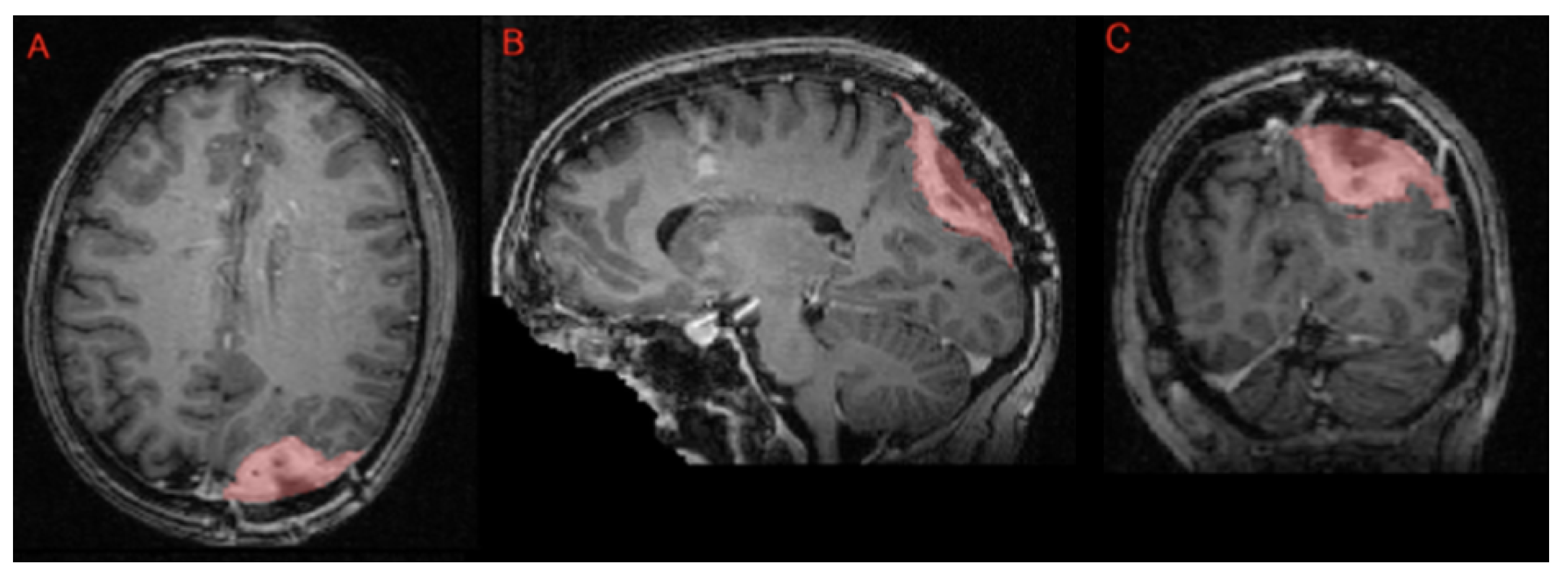

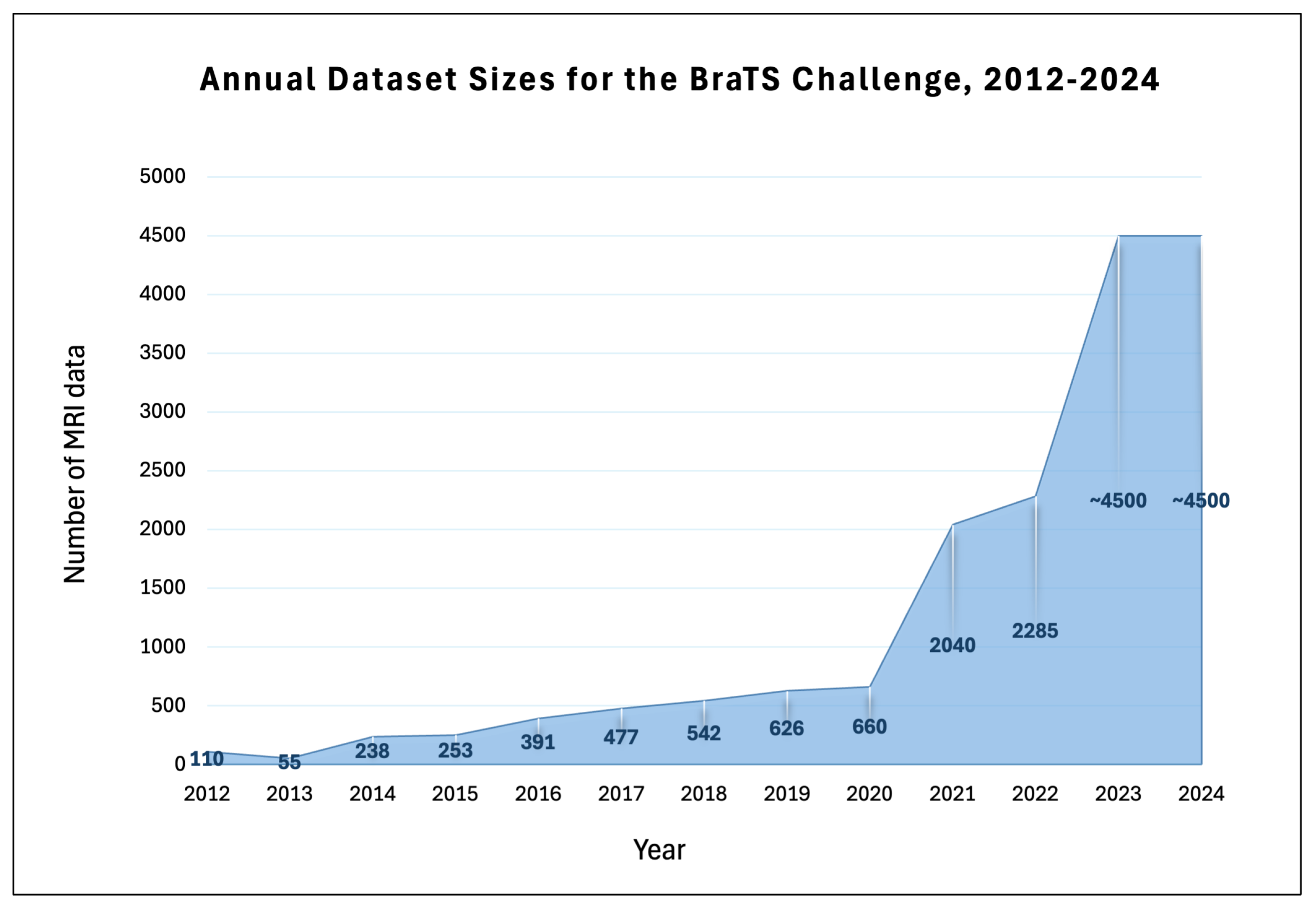


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Total | Training | Validation | Testing | Tasks | Timepoint |
|---|---|---|---|---|---|---|
| Data | Data | Data | Data | |||
| 2012 | 45 real | 30 | NA | 15 | Brain Tumor Segmentation | Pre-operative |
| 65 synthetic | 50 | NA | 15 | |||
| 2013 | 55 | 30 | NA | 25 | Brain Tumor Segmentation | Pre-operative |
| 2014 | 238 | 200 | NA | 38 | Brain Tumor Segmentation | Longitudinal |
| Disease Progression | ||||||
| 2015 | 253 | 200 | NA | 53 | Brain Tumor Segmentation | Longitudinal |
| Disease Progression | ||||||
| 2016 | 391 | 200 | NA | 191 | Brain Tumor Segmentation | Longitudinal |
| Disease Progression | ||||||
| 2017 | 477 | 285 | 46 | 146 | Brain Tumor Segmentation | Pre-operative |
| Overall Survival Prediction | ||||||
| 2018 | 542 | 285 | 66 | 191 | Brain Tumor Segmentation | Pre-operative |
| Overall Survival Prediction | ||||||
| 2019 | 626 | 335 | 125 | 166 | Brain Tumor Segmentation | Pre-operarive |
| Overall Survival Prediction | ||||||
| Quantification of Uncertanty | ||||||
| 2020 | 660 | 369 | 125 | 166 | Brain Tumor Segmentation | Pre-operative |
| Overall Survival Prediction | ||||||
| Quantification of Uncertanty | ||||||
| 2021 | 2040 | 1251 | 219 | 570 | Brain Tumor Segmentation | Pre-operative |
| MGMT classification | ||||||
| 2022 | 2285 | 1251 | 219 | 815 | Brain Tumor Segmentation | Pre-operative |
| 2023 | 2040 | 1251 | 219 | 570 | Segmentation: Adult Glioma | Pre-operative |
| 105 | 60 | 15 | 30 | Segmentation: BraTS-Africa | Pre-operative | |
| 1424 | 1000 | 141 | 283 | Segmentation: Meningioma | Pre-operative | |
| 966 | 402 | 31 | 59 | Segmentation: Brain Metastases | Pre-operative | |
| 228 | 99 | 45 | 84 | Segmentation: Pediatric Tumors | Pre-operative | |
| 2040 | 1251 | 219 | 570 | Synthesis (Global): Inpainting | Pre-operative | |
| 2038 | 1251 | 219 | 568 | Synthesis (Local): Inpainting | Pre-operative | |
| 2040 | 1251 | 219 | 570 | Evaluating Augmentations for BraTS | Pre-operative | |
| 2024 | 2200 | 1540 | 220 | 440 | Segmentation: Adult Glioma Post Treatment | Post-operative |
| / | 60 | 35 | / | Segmentation: BraTS-Africa | Pre-operative | |
| 750 | 500 | 70 | 180 | Segmentation: Meningioma Radiotherapy | Pre & Post-operative | |
| / | 652 | 88 | / | Segmentation: Brain Metastases | Pre & Post-operative | |
| 464 | 261 | 91 | 112 | Segmentation: Pediatric Tumors | Pre-operative | |
| / | 2489 | 451 | / | Segmentation: Generalizability | Pre-operative | |
| 2099 | 1251 | 219 | 629 | Synthesis (Global): Missing MRI | Pre-operative | |
| 2315 | 1251 | 219 | 845 | Synthesis (Local): Inpainting | Pre-operative | |
| 2040 | 1251 | 219 | 570 | Evaluating Augmentations for BraTS | Pre-operative | |
| 280,000 | 195,000 | 25,000 | 60,000 | Pathology | Pre-operative |
| Year | Total Data | Training Data | Validation Data | Test Data |
|---|---|---|---|---|
| BraTS 2014 | 238 | 200 data points: from BraTS 2012–2013 and TCIA, including longitudinal data | NA | 38 unseen data points from BraTS 2012–2013 test set and TCIA |
| BraTS 2015 | 253 | 200 data points: identical to the BraTS 2014 training set | NA | 53 unseen data points from BraTS 2012–2013 test set and TCIA |
| BraTS 2016 | 391 | 200 data points: identical to the BraTS 2014 training set | NA | 191 unseen data points from BraTS 2012–2013 test set and TCIA |
| Year | Tasks | MRI | Classes | Contributing | LMICs |
|---|---|---|---|---|---|
| Modalities | per Task | Institutions | |||
| 2012 | Brain Tumor Segmentation | T1, T1c, T2, FLAIR | initial: 2 | 4 | False |
| final: 4 | |||||
| 2013 | Brain Tumor Segmentation | T1, T1c, T2, FLAIR | 4 | 4 | False |
| 2014 | Brain Tumor Segmentation | T1, T1c, T2, FLAIR | 4 | 5 | False |
| Disease Progression | / | ||||
| 2015 | Brain Tumor Segmentation | T1, T1c, T2, FLAIR | 4 | 5 | False |
| Disease Progression | / | ||||
| 2016 | Brain Tumor Segmentation | T1, T1c, T2, FLAIR | 4 | 5 | False |
| Disease Progression | / | ||||
| 2017 | Brain Tumor Segmentation | T1, T1c, T2, FLAIR | 3 | 19 | False |
| Overall Survival Prediction | / | ||||
| 2018 | Brain Tumor Segmentation | T1, T1c, T2, FLAIR | 3 | 19 | False |
| Overall Survival Prediction | / | ||||
| 2019 | Brain Tumor Segmentation | T1, T1c, T2, FLAIR | 3 | 19 | False |
| Overall Survival Prediction | / | ||||
| Quantification of Uncertanty | / | ||||
| 2020 | Brain Tumor Segmentation | T1, T1c, T2, FLAIR | 3 | 19 | False |
| Overall Survival Prediction | / | ||||
| Quantification of Uncertanty | / | ||||
| 2021 | Brain Tumor Segmentation | T1, T1c, T2, FLAIR | 3 | 14 | False |
| MGMT classification | / | ||||
| 2022 | Brain Tumor Segmentation | T1, T1c, T2, FLAIR | 3 | 14 | False |
| 2023 | Segmentation: Adult Glioma | T1, T1c, T2, FLAIR | 3 | 14 | False |
| Segmentation: BraTS-Africa | T1, T1c, T2, FLAIR | 3 | 4 | True | |
| Segmentation: Meningioma | T1, T1c, T2, FLAIR | 3 | 6 | False | |
| Segmentation: Brain Metastases | T1, T1c, T2, FLAIR | 3 | 11 | False | |
| Segmentation: Pediatric Tumors | T1, T1c, T2, FLAIR | 3 | 8 | False | |
| Synthesis (Global): Inpainting | T1, T1c, T2, FLAIR | / | 14 | False | |
| Synthesis (Local): Inpainting | T1 | / | 14 | False | |
| Evaluating Augmentations for BraTS | T1, T1c, T2, FLAIR | 3 | 14 | False | |
| 2024 | Segmentation: Adult Glioma Post Treatment | T1, T1c, T2, FLAIR | 4 | 7 | False |
| Segmentation: BraTS-Africa | T1, T1c, T2, FLAIR | 3 | 10 | True | |
| Segmentation: Meningioma Radiotherapy | T1c | 1 | 7 | False | |
| Segmentation: Brain Metastases | T1, T1c, T2, FLAIR | 3 | 10 | False | |
| Segmentation: Pediatric Tumors | T1, T1c, T2, FLAIR | 4 | 8 | False | |
| Segmentation: Generalizability | T1, T1c, T2, FLAIR | 3 | / | False | |
| Synthesis (Global): Missing MRI | T1, T1c, T2, FLAIR | / | 14 | False | |
| Synthesis (Local): Inpainting | T1 | / | 14 | False | |
| Evaluating Augmentations for BraTS | T1, T1c, T2, FLAIR | 3 | 14 | False | |
| Pathology | / | 9 | 11 | False |
| Year | Top-Performing Approaches |
|---|---|
| 2012 | Predominance of Random Forests, logistic regression, and Markov Random Fields. |
| 2013 | Continuation of predominance of Random Forests-based methods. |
| 2014 | Deep convolutional network introduction alongside traditional RF methods. Emergence of U-Net, a CNN architecture. |
| 2015 | Domination of CNNs. |
| 2012 | Predominance of Random Forests, logistic regression, and Markov Random Fields. |
| 2016 | 3D CNNs, DeepMedic, led the challenge. |
| 2017 | Predominance of U-Net and DeepMedic architectures. Ensemble methods became prominent. |
| 2018 | Dominant use of CNNs, particularly U-net architectures and their ensembles, which formed the basis of the top submissions. |
| 2019 | The Two-Stage Cascaded U-Net introduced a coarse-to-fine segmentation approach, winning the challenge. |
| 2020 | The nnU-Net framework dominated. |
| 2021 | The winning model extended nnU-Net, incorporating a larger network architecture, group normalization, and axial attention in the decoder. |
| 2022 | The winning ensemble combined DeepSeg, an improved nnU-Net, and DeepSCAN architectures, utilizing the STAPLE method for final predictions. |
| 2023 | Predominance of ensemble approaches combining CNNs (e.g., nnU-Net, SegResNet) with transformer architectures (e.g., Swin-UNETR). Widespread adoption of advanced data augmentation (GANs, registration, multi-fold training) and specialized tasks—like inpainting and MRI synthesis—employing innovative loss functions (e.g., adversarial, masked L1) to enhance realism and segmentation performance. |
| 2024 | Continued evolution through ensemble strategies and innovative synthetic augmentation. Ensembles that combine CNN-based models (e.g., nnU-Net, MedNeXt) with transformer architectures (e.g., Swin-UNETR) and enhanced by synthetic data augmentation using GliGANs emerged as top-performing submissions. For MRI synthesis, a novel two-stage model—first synthesizing MRI slices with an innovative intensity encoding and then refining with 3D volumetric data—achieved strong results. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonato, B.; Nanni, L.; Bertoldo, A. Advancing Precision: A Comprehensive Review of MRI Segmentation Datasets from BraTS Challenges (2012–2025). Sensors 2025, 25, 1838. https://doi.org/10.3390/s25061838
Bonato B, Nanni L, Bertoldo A. Advancing Precision: A Comprehensive Review of MRI Segmentation Datasets from BraTS Challenges (2012–2025). Sensors. 2025; 25(6):1838. https://doi.org/10.3390/s25061838
Chicago/Turabian StyleBonato, Beatrice, Loris Nanni, and Alessandra Bertoldo. 2025. "Advancing Precision: A Comprehensive Review of MRI Segmentation Datasets from BraTS Challenges (2012–2025)" Sensors 25, no. 6: 1838. https://doi.org/10.3390/s25061838
APA StyleBonato, B., Nanni, L., & Bertoldo, A. (2025). Advancing Precision: A Comprehensive Review of MRI Segmentation Datasets from BraTS Challenges (2012–2025). Sensors, 25(6), 1838. https://doi.org/10.3390/s25061838