
Leveraging Federated Satellite Systems for Unmanned Medical Evacuation on the Battlefield

 , , , , and
, , , , and
Abstract
1. Introduction
2. The MEDEVAC Mission
2.1. Phases of the MEDEVAC Mission
2.2. Elements of the MEDEVAC Mission
3. Simulation of MEDEVAC Mission
3.1. The Simulation Model
3.2. The Performance Metrics
3.2.1. The Mission Duration Metric
3.2.2. The Data Latency Metric
4. Simulation Results
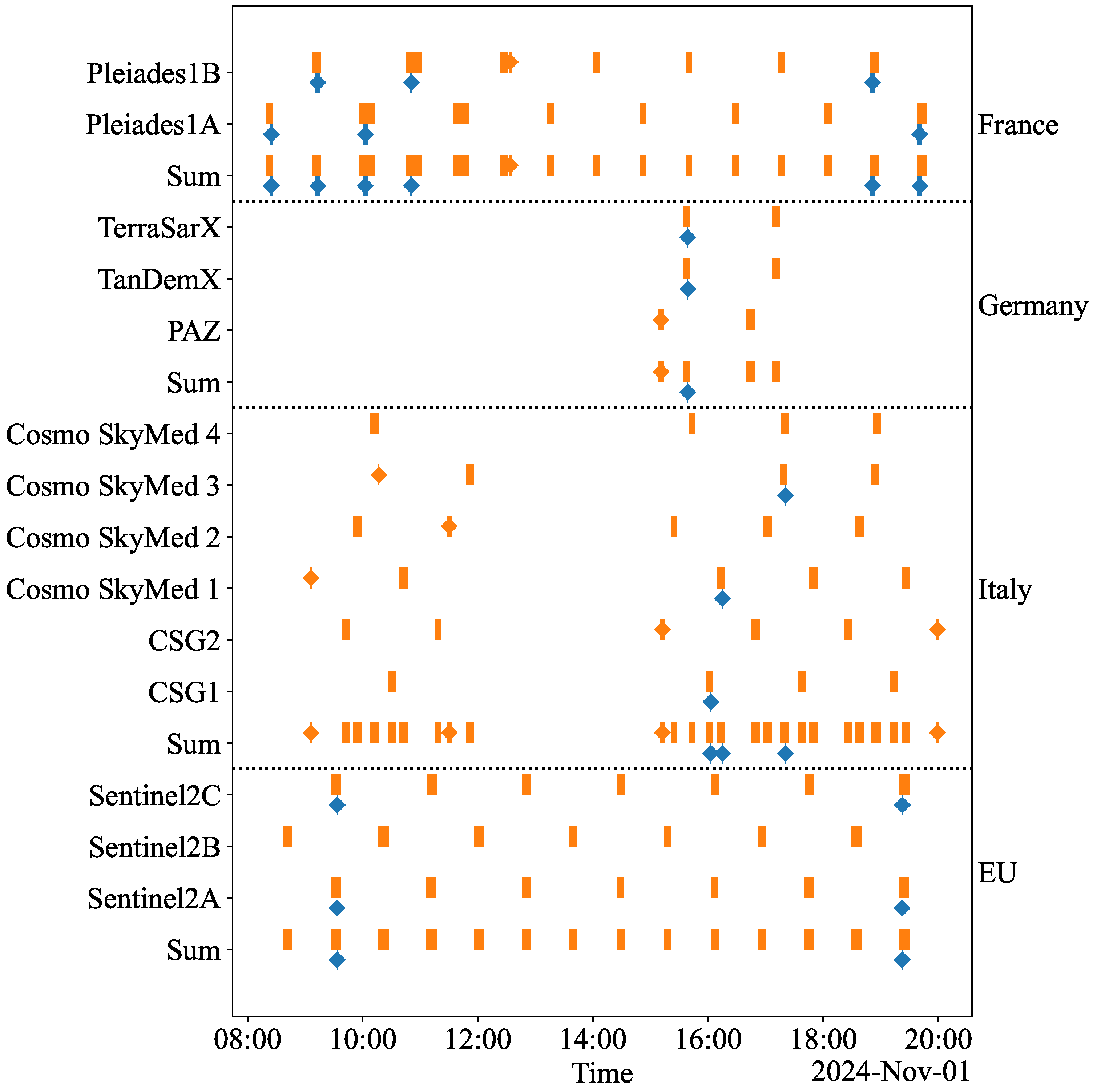
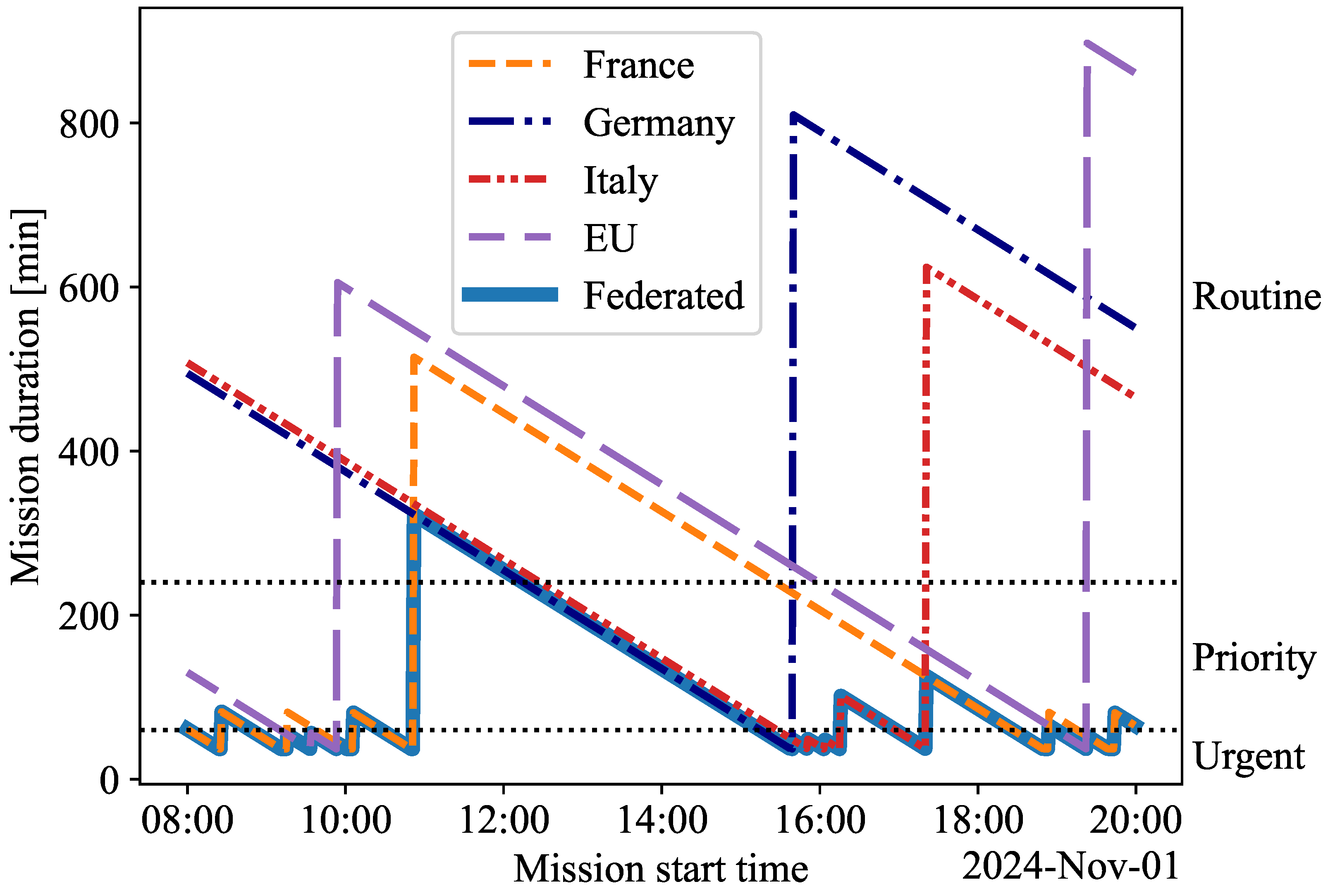
4.1. Duration of MEDEVAC Mission
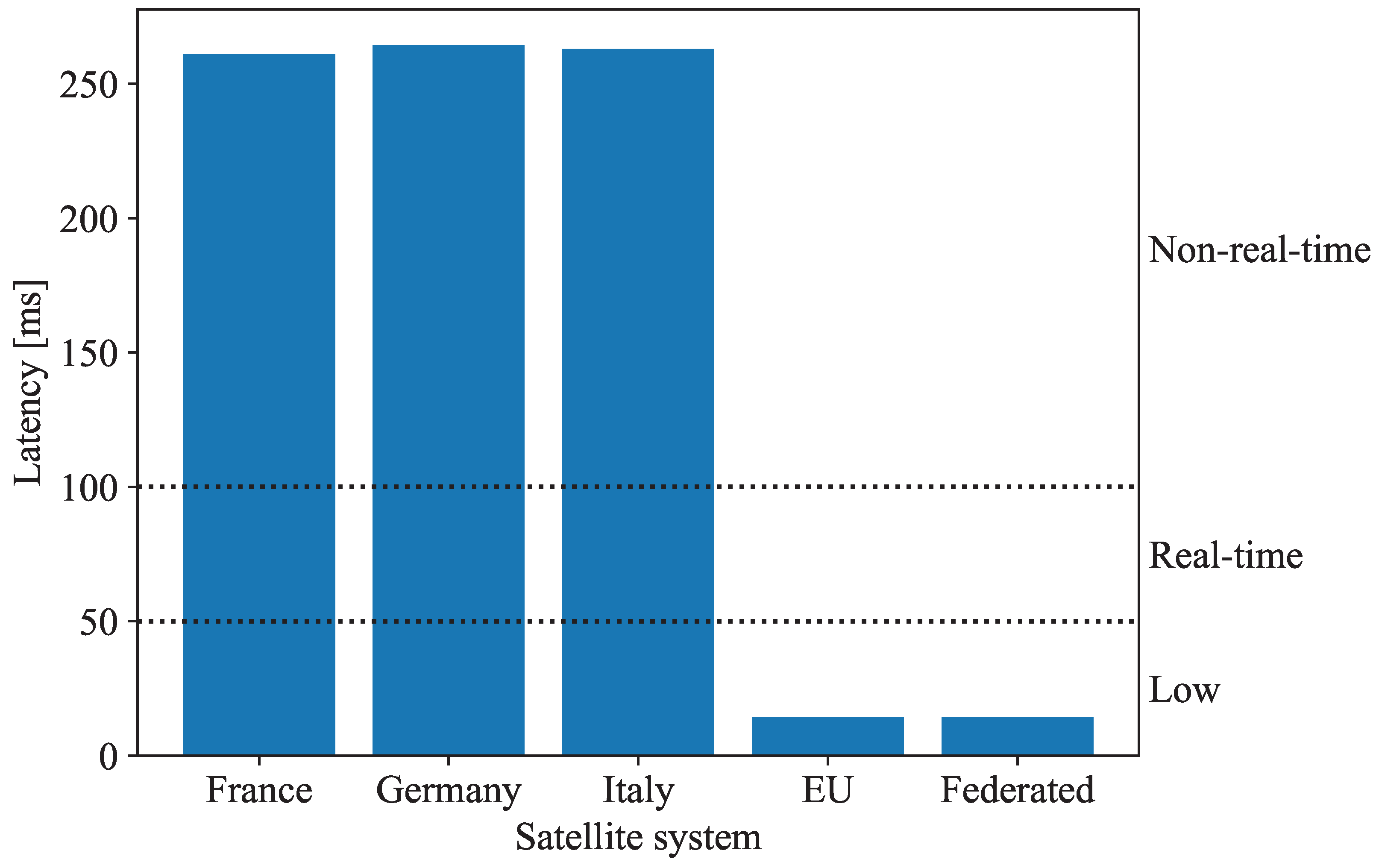
4.2. Latency of Data Transmission
5. Discussion
5.1. Interpretation of Simulation Results
5.2. Implications of the Simulation Results
5.3. Limitations
5.4. Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cunningham, C.W.; Keen, D.E.; Schauer, S.G.; Kharod, C.U.; De Lorenzo, R.A. Military Casualty Evacuation: MEDEVAC. In Aeromedical Evacuation: Management of Acute and Stabilized Patients; Hurd, W.W., Beninati, W., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 21–40. [Google Scholar] [CrossRef]
- Weissmann, M. Urban Warfare: Challenges of Military Operations on Tomorrow’s Battlefield. In Advanced Land Warfare: Tactics and Operations; Oxford University Press: Oxford, UK, 2023. [Google Scholar] [CrossRef]
- Naylor, J.F.; April, M.D.; Thronson, E.E.; Hill, G.J.; Schauer, S.G. U.S. Military Medical Evacuation and Prehospital Care of Pediatric Trauma Casualties in Iraq and Afghanistan. Prehospital Emerg. Care 2020, 24, 265–272. [Google Scholar] [CrossRef]
- Jenkins, P.R.; Lunday, B.J.; Robbins, M.J. Aerial MEDEVAC Operations: Decision Making Under Uncertainty to Save Lives. Phalanx 2020, 53, 63–66. [Google Scholar]
- Andås, H.E. Emerging Technology Trends for Defence and Security; Technical Report FFI-RAPPORT 20/01050; Norwegian Defence Research Establishment (FFI): Kjeller, Norway, 2020. [Google Scholar]
- Elmokadem, T.; Savkin, A.V. Towards Fully Autonomous UAVs: A Survey. Sensors 2021, 21, 6223. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, F.; Zielinski, Z.; Wrona, K.; Suri, N.; Fuchs, C.; Pradhan, M.; Furtak, J.; Vasilache, D.; Pellegrini, V.; Dyk, M.; et al. Application of IoT in military operations in a smart city. In Proceedings of the 2018 International Conference on Military Communications and Information Systems (ICMCIS), Warsaw, Poland, 22–23 May 2018; pp. 1–8. [Google Scholar] [CrossRef]
- Fisher, N. USAMRDC: Medical Operations in the Multidomain Battlefield. Available online: https://mrdc.health.mil/index.cfm/media/articles/2017/medical_operations_in_multidomain_battlefield (accessed on 1 November 2024).
- Li, Z.; Min, G.; Ren, P.; Luo, C.; Zhao, L.; Luo, C. Ubiquitous and Robust UxV Networks: Overviews, Solutions, Challenges, and Opportunities. IEEE Netw. 2024, 38, 26–34. [Google Scholar] [CrossRef]
- Ialongo, I.; Bun, R.; Hakkarainen, J.; Virta, H.; Oda, T. Satellites capture socioeconomic disruptions during the 2022 full-scale war in Ukraine. Sci. Rep. 2023, 13, 14954. [Google Scholar] [CrossRef]
- Bhat, S.; Meenakshi, M. Vision based robotic system for military applications—Design and real time validation. In Proceedings of the 2014 Fifth International Conference on Signal and Image Processing, Bangalore, India, 8–10 January 2014; pp. 20–25. [Google Scholar] [CrossRef]
- Munir, A.; Aved, A.; Blasch, E. Situational Awareness: Techniques, Challenges, and Prospects. AI 2022, 3, 55–77. [Google Scholar] [CrossRef]
- Wang, Q.; Li, W.; Yu, Z.; Abbasi, Q.; Imran, M.; Ansari, S.; Sambo, Y.; Wu, L.; Li, Q.; Zhu, T. An Overview of Emergency Communication Networks. Remote Sens. 2023, 15, 1595. [Google Scholar] [CrossRef]
- Eshmawi, A.A.; Umer, M.; Ashraf, I.; Park, Y. Enhanced Machine Learning Ensemble Approach for Securing Small Unmanned Aerial Vehicles From GPS Spoofing Attacks. IEEE Access 2024, 12, 27344–27355. [Google Scholar] [CrossRef]
- Zabala-López, A.; Linares-Vásquez, M.; Haiduc, S.; Donoso, Y. A survey of data-centric technologies supporting decision-making before deploying military assets. Def. Technol. 2024, 42, 226–246. [Google Scholar] [CrossRef]
- Colwell, J.E.; Esposito, L.W.; Bundy, D. Fragmentation rates of small satellites in the outer solar system. J. Geophys. Res. Planets 2000, 105, 17589–17599. [Google Scholar] [CrossRef]
- Matthiesen, B.; Razmi, N.; Leyva-Mayorga, I.; Dekorsy, A.; Popovski, P. Federated Learning in Satellite Constellations. IEEE Netw. 2024, 38, 232–239. [Google Scholar] [CrossRef]
- Pastore, T.; Galdorisi, G.; Jones, A. Command and Control (C2) to enable multi-domain teaming of unmanned vehicles (UxVs). In Proceedings of the OCEANS 2017—Anchorage, Anchorage, AK, USA, 18–21 September 2017; pp. 1–7. [Google Scholar]
- Golkar, A.; Lluch i Cruz, I. The Federated Satellite Systems paradigm: Concept and business case evaluation. Acta Astronaut. 2015, 111, 230–248. [Google Scholar] [CrossRef]
- NATO. Topic: NATO’s Approach to Space. Available online: https://www.nato.int/cps/en/natohq/topics_175419.htm (accessed on 1 December 2024).
- Alves, H.; Mikhaylov, K.; Höyhtyä, M. Integration of MTC and Satellites for IoT Toward 6G Era; John Wiley & Sons: Hoboken, NJ, USA, 2024. [Google Scholar]
- Wang, J.; Jiang, C.; Kuang, L. High-Mobility Satellite-UAV Communications: Challenges, Solutions, and Future Research Trends. IEEE Commun. Mag. 2022, 60, 38–43. [Google Scholar] [CrossRef]
- Andersson, C.A.; Halme, K.; Laine, M.; Hulkko, V.; Virtanen, K. Effectiveness of an Expendable Unmanned Ground Vehicle Stalling a Mechanized Infantry Company’s Primary Combat Units—A Virtual Simulation Experiment. J. Field Robot. 2024, 1–18. [Google Scholar] [CrossRef]
- Bohemia Interactive. Home Page. Available online: https://www.bohemia.net/ (accessed on 5 December 2024).
- Mansikka, H.; Virtanen, K.; Harris, D.; Salomäki, J. Live–virtual–constructive simulation for testing and evaluation of air combat tactics, techniques, and procedures, Part 1: Assessment framework. J. Def. Model. Simul. Appl. Methodol. Technol. 2021, 18, 285–293. [Google Scholar] [CrossRef]
- Mansikka, H.; Virtanen, K.; Harris, D.; Salomäki, J. Live–virtual–constructive simulation for testing and evaluation of air combat tactics, techniques, and procedures, Part 2: Demonstration of the framework. J. Def. Model. Simul. Appl. Methodol. Technol. 2021, 18, 295–308. [Google Scholar] [CrossRef]
- Jiang, W.; Zhan, Y.; Xiao, X.; Sha, G. Network Simulators for Satellite-Terrestrial Integrated Networks: A Survey. IEEE Access 2023, 11, 98269–98292. [Google Scholar] [CrossRef]
- Ansys Government Initiatives. Ansys STK. Available online: https://www.ansys.com/products/missions/ansys-stk (accessed on 1 November 2024).
- ESA. Kiruna Station. Available online: https://www.esa.int/Enabling_Support/Operations/ESA_Ground_Stations/Kiruna_station (accessed on 5 December 2024).
- CNES. Toulouse Station. Available online: https://regina.cnes.fr/fr/stations/TLSG (accessed on 5 December 2024).
- DLR. Weilheim and Neustrelitz Stations. Available online: https://gsn.dlr.de/ (accessed on 5 December 2024).
- CONAE. Cordoba Station. Available online: https://landsat.usgs.gov/COA (accessed on 5 December 2024).
- Avilus. Grille—The German Rescue Drone. Available online: https://avilus.com/solution (accessed on 10 December 2024).
- Gosselin-Malo, E. Unmanned Systems Seen as Future of Battlefield Casualty Evacuation. Available online: https://www.c4isrnet.com/battlefield-tech/2024/02/15/unmanned-systems-seen-as-future-of-battlefield-casualty-evacuation/ (accessed on 5 December 2024).
- Langfield, M. Unmanned K-MAX Performs First Casevac. Available online: https://www.airmedandrescue.com/latest/news/unmanned-k-max-performs-first-casevac (accessed on 5 December 2024).
- Poli, D.; Remondino, F.; Angiuli, E.; Agugiaro, G. Evaluation of Pleiades—1A triplet on Trento testingfield. Int. Arch. Photogramm. Remote Sens. Spat. Inf. Sci. 2013, XL-1-W1, 287–292. [Google Scholar] [CrossRef]
- Thales Group. Syracuse III Ground Segment: Helping French Forces Achieve a Big Ambition|Thales Group. Available online: https://www.thalesgroup.com/en/worldwide/defence-and-security/references/syracuse-iii-ground-segment-helping-french-forces-achieve (accessed on 12 November 2024).
- Krieger, G.; Moreira, A.; Fiedler, H.; Hajnsek, I.; Werner, M.; Younis, M.; Zink, M. TanDEM-X: A Satellite Formation for High-Resolution SAR Interferometry. IEEE Trans. Geosci. Remote Sens. 2007, 45, 3317–3341. [Google Scholar] [CrossRef]
- Werninghaus, R.; Buckreuss, S. The TerraSAR-X Mission and System Design. IEEE Trans. Geosci. Remote Sens. 2010, 48, 606–614. [Google Scholar] [CrossRef]
- DLR. SATCOMBw. Available online: https://www.dlr.de/en/rb/research-operation/missions/communications/satcombw (accessed on 12 November 2024).
- Covello, F.; Battazza, F.; Coletta, A.; Lopinto, E.; Fiorentino, C.; Pietranera, L.; Valentini, G.; Zoffoli, S. COSMO-SkyMed an existing opportunity for observing the Earth. J. Geodyn. 2010, 49, 171–180. [Google Scholar] [CrossRef]
- Sacco, P.; Parca, G.; Codispoti, G.; Bertocchi, L.; Russo, E.; Tuozzi, A.; Matarazzi, C.; Coletta, A. The Italian assets for the CLOSEYE EU project: Cosmo-Skymed and Athena-Fidus satellite systems. In Proceedings of the 2016 IEEE International Geoscience and Remote Sensing Symposium (IGARSS), Beijing, China, 10–15 July 2016; pp. 2054–2057. [Google Scholar] [CrossRef]
- Phiri, D.; Simwanda, M.; Salekin, S.; Nyirenda, V.R.; Murayama, Y.; Ranagalage, M. Sentinel-2 Data for Land Cover/Use Mapping: A Review. Remote Sens. 2020, 12, 2291. [Google Scholar] [CrossRef]
- Capez, G.M.; Cáceres, M.A.; Armellin, R.; Bridges, C.P.; Frey, S.; Garello, R.; Bargellini, P. Characterization of Mega-Constellation Links for LEO Missions with Applications to EO and ISS Use Cases. IEEE Access 2023, 11, 25616–25628. [Google Scholar] [CrossRef]
- Chorvalli, V.; Cazaubiel, V.; Bursch, S.; Welsch, M.; Sontag, H.; Martimort, P.; Bello, U.D.; Sy, O.; Laberinti, P.; Spoto, F. Design and development of the Sentinel-2 Multi Spectral Instrument and satellite system. In SPIE Remote Sensing, Proceedings of the Sensors, Systems, and Next-Generation Satellites XIV, Toulouse, France, 20–23 September 2010; Meynart, R., Neeck, S.P., Shimoda, H., Eds.; Society of Photo-Optical Instrumentation Engineers (SPIE): Toulouse, France, 2010; Volume 7826, pp. 134–137. [Google Scholar] [CrossRef]
- Neumeier, S.; Wintersberger, P.; Frison, A.K.; Becher, A.; Facchi, C.; Riener, A. Teleoperation: The Holy Grail to Solve Problems of Automated Driving? Sure, but Latency Matters. In Proceedings of the AutomotiveUI ’19: 11th International Conference on Automotive User Interfaces and Interactive Vehicular Applications, Utrecht, The Netherlands, 21–25 September 2019; pp. 186–197. [Google Scholar] [CrossRef]
- Nakamura, E. Signal Time-Delay Tolerance in Teleoperated Vehicles. In Proceedings of the 2021 IEEE 10th Global Conference on Consumer Electronics (GCCE), Kyoto, Japan, 12–15 October 2021; pp. 770–773. [Google Scholar] [CrossRef]
- Morton, A.; Mghazli, Y.E.; Dolly, M.; Tarapore, P.; Ash, G.; Dvorak, C. Y.1541-QOSM: Model for Networks Using Y.1541 Quality-of-Service Classes; Request for Comments RFC 5976; Internet Engineering Task Force: Wilmington, DE, USA, 2010. [Google Scholar] [CrossRef]
- Nankaku, A.; Tokunaga, M.; Yonezawa, H.; Kanno, T.; Kawashima, K.; Hakamada, K.; Hirano, S.; Oki, E.; Mori, M.; Kinugasa, Y. Maximum acceptable communication delay for the realization of telesurgery. PLoS ONE 2022, 17, e0274328. [Google Scholar] [CrossRef]
- Marescaux, J.; Leroy, J.; Gagner, M.; Rubino, F.; Mutter, D.; Vix, M.; Butner, S.E.; Smith, M.K. Transatlantic robot-assisted telesurgery. Nature 2001, 413, 379–380. [Google Scholar] [CrossRef]
- Ruiz-de Azua, J.A.; Garzaniti, N.; Golkar, A.; Calveras, A.; Camps, A. Towards Federated Satellite Systems and Internet of Satellites: The Federation Deployment Control Protocol. Remote Sens. 2021, 13, 982. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Federated Satellite System | Standalone Satellite System |
|---|---|---|
| Architecture | A network of interconnected satellites linked through ISLs. | Independent satellites with no interlinking. |
| Data sharing | Authenticated users gain access to data from all satellites within the federation. | Authenticated users access data from a single satellite system. |
| Coverage | Provides a wider coverage area by leveraging multiple satellite constellations. | Limited to the coverage area of a standalone satellite system. |
| Revisit times | Reduced revisit times due to multiple satellites. | Longer revisit times dependent on the availability of individual satellites. |
| Communication speed | Faster, as data can be directly relayed to the target location through ISLs. | Slower, relying on a direct ground station link. |
| Payload resource | Payload is shared across the satellite network. | Restricted to the independent capability of each satellite. |
| Operational flexibility | High flexibility, allowing for data rerouting and imaging tasks across the entire satellite network. | Limited flexibility, with satellites operating independently. |
| Resilience to coverage gaps | Highly resilient, with additional constellations compensating for coverage gaps. | Vulnerable to gaps due to a limited number of satellites. |
| System complexity | Higher complexity due to inter-satellite coordination among multiple organizations. | Simpler, with less need for cross-organizational management. |
| Satellite System | Imaging Satellites | Communication Satellites | |
|---|---|---|---|
| Satellites | Ground Stations | ||
| France | Pleiades1A Pleiades1B | Toulouse, France Kiruna, Sweden | Syracuse3A Syracuse3B |
| Germany | TanDemX TerraSarX PAZ | Weilheim, Germany Neustrelitz, Germany | ComSatBw1 ComSatBw2 |
| Italy | CosmoSkymed1 CosmoSkymed2 CosmoSkymed3 CosmoSkymed4 CosmoSkymed4 CSG2 | Cordoba, Argentina Kiruna, Sweden | Athena-Fidus |
| EU | Sentinel2A Sentinel2B Sentinel2C | Kiruna, Sweden | OneWeb constellation |
| Federated | France Germany Italy EU | Uses the closest ground station available | Uses the fastest communication satellite available |
| Classification | Duration of Mission (h) | Description |
|---|---|---|
| Urgent | 0–1 | Casualties needing urgent evacuation within one hour must be quickly treated to prevent serious complications or permanent damage. |
| Priority | 1–4 | Casualties needing evacuation within four hours require prompt action to prevent worsening conditions or increased suffering. |
| Routine | 4–24 | Casualties needing evacuation within 24 h have stable conditions and are unlikely to worsen. |
| Classification | Latency (ms) | Description |
|---|---|---|
| Low | 0–50 | Low latency enables telesurgery and all activities included in the ‘Real-time’ and ‘Non-real-time’ classes. |
| Real-time | 50–100 | Real-time latency enables the steering of the UXV and all activities included in the ‘Non-real-time’ class. |
| Non-real-time | >100 | Non-real-time latency enables the evacuation of a casualty such that the route of the UXV is determined prior to the dispatch of the UXV. |
| Satellite System | Capability for Urgent Missions (%) | Capability for Priority Missions (%) | Capability for Routine Missions (%) |
|---|---|---|---|
| France | 22.1 | 39.7 | 38.2 |
| Germany | 3.5 | 25.0 | 71.5 |
| Italy | 9.9 | 30.8 | 59.3 |
| EU | 9.2 | 34.9 | 56.0 |
| Federated | 39.0 | 49.4 | 11.5 |
| Satellite System | The Most Suitable MEDEVAC Mission Type | Capability for Low Latency |
|---|---|---|
| France | Priority | No |
| Germany | Routine | No |
| Italy | Routine | No |
| EU | Routine | Yes |
| Federated | Priority | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halme, K.; Kirjamäki, O.; Pietarinen, S.; Majanen, M.; Virtanen, K.; Höyhtyä, M. Leveraging Federated Satellite Systems for Unmanned Medical Evacuation on the Battlefield. Sensors 2025, 25, 1655. https://doi.org/10.3390/s25061655
Halme K, Kirjamäki O, Pietarinen S, Majanen M, Virtanen K, Höyhtyä M. Leveraging Federated Satellite Systems for Unmanned Medical Evacuation on the Battlefield. Sensors. 2025; 25(6):1655. https://doi.org/10.3390/s25061655
Chicago/Turabian StyleHalme, Kasper, Oskari Kirjamäki, Samuli Pietarinen, Mikko Majanen, Kai Virtanen, and Marko Höyhtyä. 2025. "Leveraging Federated Satellite Systems for Unmanned Medical Evacuation on the Battlefield" Sensors 25, no. 6: 1655. https://doi.org/10.3390/s25061655
APA StyleHalme, K., Kirjamäki, O., Pietarinen, S., Majanen, M., Virtanen, K., & Höyhtyä, M. (2025). Leveraging Federated Satellite Systems for Unmanned Medical Evacuation on the Battlefield. Sensors, 25(6), 1655. https://doi.org/10.3390/s25061655