
Field Testing Multi-Parametric Wearable Technologies for Wildfire Firefighting Applications

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
- ‘Stop 1’: 3 min of baseline data collection to establish physiological norms while the participants were at rest.
- ‘Run 1’: 2 min of running to elevate physiological stress
- ‘Stop 2’: 2 min of static rest to observe recovery patterns.
- ‘Run 2’: 1 additional min of running simulating an approach towards a fire.
- ‘Fire’ (Figure 2): 5 min of fire suppression, during which the team was divided into three functional roles: handling the hose for direct fire suppression (‘L1’ for Team 1, ‘L2’and ‘L3’ for Team 2), providing hose support (‘S1’ for Team 1 and ‘S2’ for Team 2), and using rakes to manage surrounding debris (‘R1’,’R2’,’R3’,’R4’, in Team 1, ‘R5’ and ‘R6’ for Team 2).
- ‘Stop 3’: 1 min of data collection during the post-suppression recovery phase to assess physiological return to baseline.
2.1. Data Processing
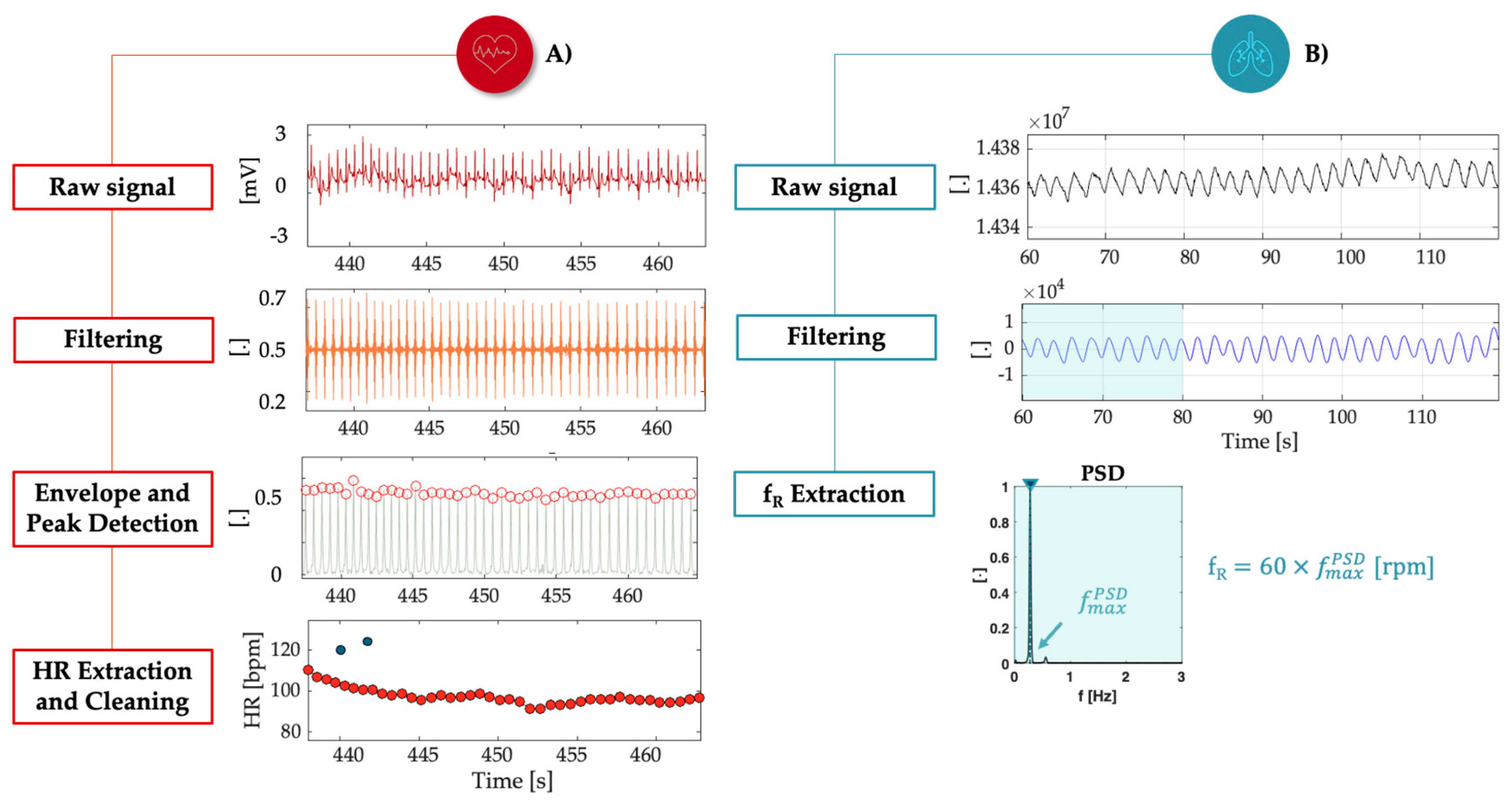
2.1.1. Physiological Signals Processing
2.1.2. Physical Data Processing
3. Results
3.1. Physiological Data
3.1.1. Heart Rate Range and Maximum Measures
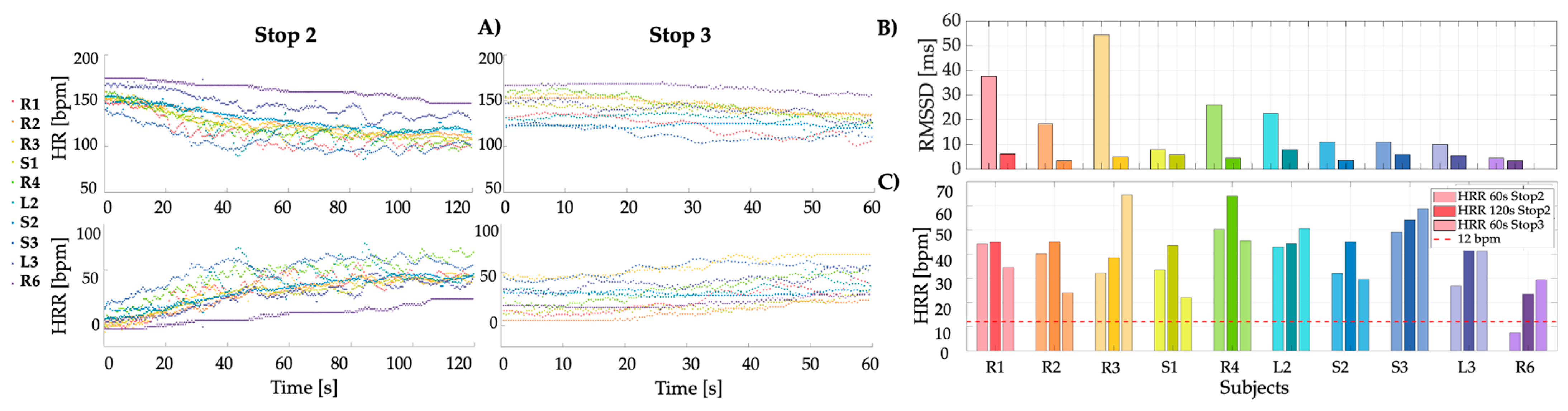
3.1.2. Heart Rate Recovery and Heart Rate Variability
3.1.3. Respiratory Data
- Bradypnea, characterized by a slow breathing rate, is typically less than 12 rpm and may indicate a state of relaxation or, in some cases, respiratory suppression.
- Eupnea, or normal, un-labored breathing, from 12 to 20 rpm, reflects a stable and comfortable state of respiration.
- Tachypnea, which is an elevated respiratory rate exceeding 20 rpm, often occurs in response to stress or increased physiological demand, serving as a mechanism to enhance oxygen intake and carbon dioxide expulsion.
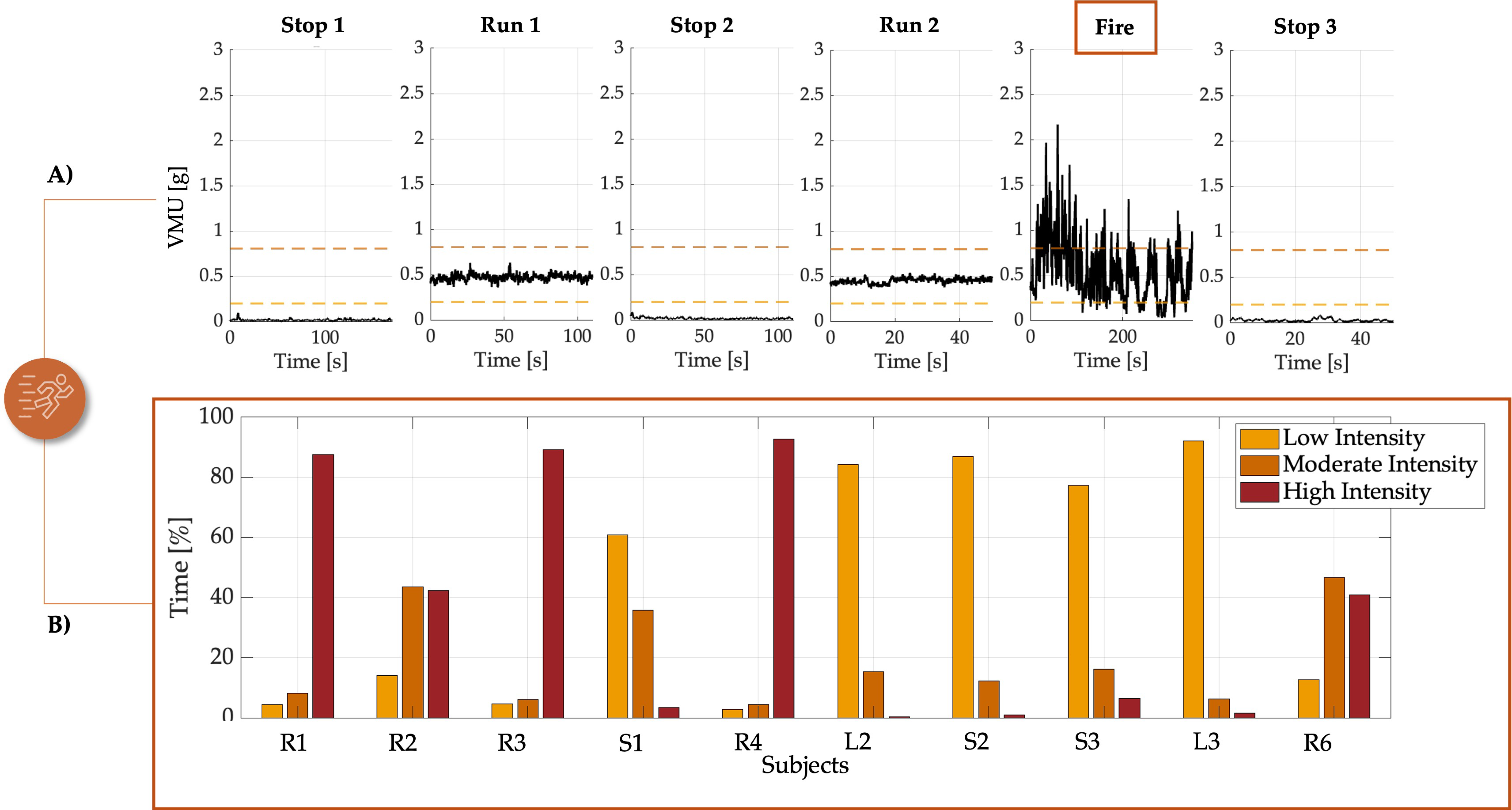
3.2. Physical Data
- (i)
- Low Intensity (<0.2 g): activities registering under 0.2 g are considered low intensity, indicating minimal exertion like slow walking. This level is typically associated with tasks requiring little physical effort.
- (ii)
- Moderate Intensity (0.2 g to 0.8 g): values within this range denote moderate activity levels, characteristic of standard intense walk\run activities. This intensity reflects the typical demands of firefighting operations that do not require maximal effort.
- (iii)
- High Intensity (>0.8 g): readings above 0.8 g are categorized as high intensity, indicative of vigorous and sustained physical efforts. Such levels are usually required in emergency situations where rapid and intense actions are necessary.
4. Discussions and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Avci, M.G.; Avci, M.; Battarra, M.; Erdoğan, G. The wildfire suppression problem with multiple types of resources. Eur. J. Oper. Res. 2024, 316, 488–502. [Google Scholar] [CrossRef]
- Incendi Forestali: Da Gennaio a Luglio 2024 in Linea Con la Media dal 2006. Episodi Più Gravi in Sicilia e Sardegna, a Vieste Salva la Copertura Forestale—Italiano. Available online: https://www.isprambiente.gov.it/it/news/incendi-forestali-da-gennaio-a-luglio-2024-in-linea-con-la-media-dal-2006-episodi-piu-gravi-in-sicilia-e-sardegna-a-vieste-salva-la-copertura-forestale# (accessed on 11 October 2024).
- Stephens, S.L.; Adams, M.A.; Handmer, J.; Kearns, F.R.; Leicester, B.; Leonard, J.; Moritz, M.A. Urban-wildland fires: How California and other regions of the US can learn from Australia. Environ. Res. Lett. 2009, 4, 014010. [Google Scholar] [CrossRef]
- Ferguson, S.A.; Smith, B.P.; Browne, M.; Rockloff, M.J. Fatigue in Emergency Services Operations: Assessment of the Optimal Objective and Subjective Measures Using a Simulated Wildfire Deployment. Int. J. Environ. Res. Public Health 2016, 13, 171. [Google Scholar] [CrossRef] [PubMed]
- Katan, J.; Perez, L. ABWiSE v1.0: Toward an Agent-Based Approach to Simulating Wildfire Spread. Nat. Hazards Earth Syst. Sci. 2021, 21, 3141–3160. [Google Scholar] [CrossRef]
- Ghosh, R.; Adhikary, J.; Chemlal, R. Fire Spread Modeling Using Probabilistic Cellular Automata. Commun. Comput. Inf. Sci. 2024, 2021, 45–55. [Google Scholar] [CrossRef]
- Schumaker, N.H.; Watkins, S.M.; Heinrichs, J.A. HexFire: A Flexible and Accessible Wildfire Simulator. Land 2022, 11, 1288. [Google Scholar] [CrossRef]
- Arca, B.; Pedes, F.; Salis, M.; Pellizzaro, G.; Duce, P.; Ventura, A.; Canu, A.; Jahdi, R.; Giudice, L.D.; Scarpa, C.; et al. Evaluating Wildfire Simulators Based on the 2021 Large Fires Occurring in Sardinia. Environ. Sci. Proc 2022, 17, 74. [Google Scholar] [CrossRef]
- Parker, R.; Vitalis, A.; Walker, R.; Riley, D.; Pearce, H.G. Measuring wildland fire fighter performance with wearable technology. Appl. Ergon. 2017, 59, 34–44. [Google Scholar] [CrossRef]
- Rodrigues, S.; Dias, D.; Paiva, J.; Cunha, J.P.S. Psychophysiological Stress Assessment among On-Duty Firefighters. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBS), Honolulu, HI, USA, 18–21 July 2018. [Google Scholar] [CrossRef]
- NFPA Reveals Rise in Fatal Firefighter Injuries in the US During 2022. Available online: https://internationalfireandsafetyjournal.com/nfpa-reveals-rise-in-fatal-firefighter-injuries-in-the-us-during-2022/ (accessed on 16 October 2024).
- Rodríguez-Marroyo, J.A.; López-Satue, J.; Pernía, R.; Carballo, B.; García-López, J.; Foster, C.; Villa, J.G. Physiological work demands of Spanish wildland firefighters during wildfire suppression. Int. Arch. Occup. Environ. Health 2012, 85, 221–228. [Google Scholar] [CrossRef]
- Tochihara, Y.; Lee, J.Y.; Son, S.Y. A review of test methods for evaluating mobility of firefighters wearing personal protective equipment. Ind. Health 2022, 60, 106–120. [Google Scholar] [CrossRef]
- Rodríguez-Marroyo, J.A.; Villa, J.G.; López-Satue, J.; Pernía, R.; Carballo, B.; García-López, J.; Foster, C. Physical and thermal strain of firefighters according to the firefighting tactics used to suppress wildfires. Ergonomics 2011, 54, 1101–1108. [Google Scholar] [CrossRef]
- Taborri, J.; Pasinetti, S.; Cardinali, L.; Perroni, F.; Rossi, S. Preventing and monitoring work-related diseases in firefighters: A literature review on sensor-based systems and future perspectives in robotic devices. Int. J. Environ. Res. Public Health 2021, 18, 9723. [Google Scholar] [CrossRef] [PubMed]
- Bustos, D.; Cardoso, R.; Carvalho, D.D.; Guedes, J.; Vaz, M.; Torres Costa, J.; Santos Baptista, J.; Fernandes, R.J. Exploring the Applicability of Physiological Monitoring to Manage Physical Fatigue in Firefighters. Sensors 2023, 23, 5127. [Google Scholar] [CrossRef]
- Angerer, P.; Kadlez-Gebhardt, S.; Delius, M.; Raluca, P.; Nowak, D. Comparison of Cardiocirculatory and Thermal Strain of Male Firefighters During Fire Suppression to Exercise Stress Test and Aerobic Exercise Testing. Am. J. Cardiol. 2008, 102, 1551–1556. [Google Scholar] [CrossRef]
- Smith, D.L.; Haller, J.M.; Benedict, R.; Moore-Merrell, L. Cardiac Strain Associated with High-rise Firefighting. J. Occup. Environ. Hyg. 2015, 12, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Ebersole, K.T.; Cornell, D.J.; Flees, R.J.; Shemelya, C.M.; Noel, S.E. Contribution of the autonomic nervous system to recovery in firefighters. J. Athl. Train. 2020, 55, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.; Roberts, J.; Simms, K.; Cheng, D.; Hartman, J.; Bartlett, C. Measurement of Functional Capacity Requirements to Aid in Development of an Occupation-Specific Rehabilitation Training Program to Help Firefighters with Cardiac Disease Safely Return to Work. Am. J. Cardiol. 2009, 103, 762–765. [Google Scholar] [CrossRef]
- Del Sal, M.; Barbieri, E.; Garbati, P.; Sisti, D.; Rocchi, M.B.; Stocchi, V. Physiologic Responses of Firefighter Recruits During A Supervised Live-Fire Work Performance Test. J. Strength Cond. Res. 2009, 23, 2396–2404. [Google Scholar] [CrossRef]
- Okutucu, S.; Karakulak, U.N.; Aytemir, K.; Oto, A. Heart rate recovery: A practical clinical indicator of abnormal cardiac autonomic function. Expert Rev. Cardiovasc. Ther. 2011, 9, 1417–1430. [Google Scholar] [CrossRef]
- Pluntke, U.; Gerke, S.; Sridhar, A.; Weiss, J.; Michel, B. Evaluation and Classification of Physical and Psychological Stress in Firefighters using Heart Rate Variability. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 2207–2212. [Google Scholar] [CrossRef]
- Meina, M.; Ratajczak, E.; Sadowska, M.; Rykaczewski, K.; Dreszer, J.; Bałaj, B.; Biedugnis, S.; Węgrzyński, W.; Krasuski, A. Heart rate variability and accelerometry as classification tools for monitoring perceived stress levels—A pilot study on firefighters. Sensors 2020, 20, 2834. [Google Scholar] [CrossRef]
- Vyas, K.; Mcgregor, C. The use of heart rate for the assessment of firefighter resilience: A literature review. In Proceedings of the 2018 IEEE Life Sciences Conference, LSC 2018, Montreal, QC, Canada, 28–30 October 2018; pp. 259–262. [Google Scholar] [CrossRef]
- Jeklin, A.T.; Perrotta, A.S.; Davies, H.W.; Bredin, S.S.D.; Paul, D.A.; Warburton, D.E.R. The association between heart rate variability, reaction time, and indicators of workplace fatigue in wildland firefighters. Int. Arch. Occup. Environ. Health 2021, 94, 823–831. [Google Scholar] [CrossRef]
- Nicolò, A.; Massaroni, C.; Schena, E.; Sacchetti, M. The Importance of Respiratory Rate Monitoring: From Healthcare to Sport and Exercise. Sensors 2020, 20, 6396. [Google Scholar] [CrossRef]
- Horn, G.P.; Gutzmer, S.; Fahs, C.A.; Petruzzello, S.J.; Goldstein, E.; Fahey, G.C.; Fernhall, B.; Smith, D.L. Physiological Recovery from Firefighting Activities in Rehabilitation and Beyond. Prehospital Emerg. Care 2011, 15, 214–225. [Google Scholar] [CrossRef] [PubMed]
- Schermer, T.; Malbon, W.; Newbury, W.; Holton, C.; Smith, M.; Morgan, M.; Crockett, A. Spirometry and impulse oscillometry (IOS) for detection of respiratory abnormalities in metropolitan firefighters. Respirology 2010, 15, 975–985. [Google Scholar] [CrossRef] [PubMed]
- Raiano, L.; Di Tocco, J.; Massaroni, C.; Di Pino, G.; Schena, E.; Formica, D. Respiratory rate estimation during walking/running activities using principal components estimated from signals recorded by a smart garment embedding piezoresistive sensors. In Proceedings of the 2021 IEEE International Workshop on Metrology for Industry 4.0 and IoT, MetroInd 4.0 and IoT 2021, Rome, Italy, 7–9 June 2021; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2021; pp. 544–549. [Google Scholar] [CrossRef]
- Kral, T.R.A.; Weng, H.Y.; Mitra, V.; Imhoff-Smith, T.P.; Azemi, E.; Goldman, R.I.; Rosenkranz, M.A.; Wu, S.; Chen, A.; Davidson, R.J. Slower respiration rate is associated with higher self-reported well-being after wellness training. Sci. Rep. 2023, 13, 15953. [Google Scholar] [CrossRef] [PubMed]
- Salim, F.; Belbasis, A.; Prohasky, D.; Houshyar, S.; Fuss, F.K. Design and evaluation of smart wearable undergarment for monitoring physiological extremes in firefighting. In ISWC ’14 Adjunct, Proceedings of the 2014 ACM International Symposium on Wearable Computers: Adjunct Program, Seattle, DC, USA, 13–17 September 2014; Association for Computing Machinery: New York, NY, USA, 2014; pp. 249–254. [Google Scholar] [CrossRef]
- Tartare, G.; Zeng, X.; Koehl, L. Development of a wearable system for monitoring the firefighter’s physiological state. In Proceedings of the 2018 IEEE Industrial Cyber-Physical Systems, ICPS 2018, St. Petersburg, Russia, 15–18 May 2018; pp. 561–566. [Google Scholar] [CrossRef]
- Carballo-Leyenda, B.; Villa, J.G.; López-Satué, J.; Rodríguez-Marroyo, J.A. Wildland firefighters’ thermal exposure in relation to suppression tasks. Int. J. Wildland Fire 2021, 30, 475–483. [Google Scholar] [CrossRef]
- Massaroni, C.; Sacchetti, M.; Romano, C.; Schena, E.; Innocenti, L.; Nicolo, A. The effects of different algorithms on the performance of a strain-based wearable device estimating respiratory rate during cycling exercise. In Proceedings of the 2023 IEEE International Workshop on Metrology for Industry 4.0 and IoT, MetroInd4.0 and IoT 2023, Brescia, Italy, 6–8 June 2023; pp. 142–147. [Google Scholar] [CrossRef]
- Marcel-Millet, P.; Ravier, G.; Grospretre, S.; Gimenez, P.; Freidig, S.; Groslambert, A. Physiological responses and parasympathetic reactivation in rescue interventions: The effect of the breathing apparatus. Scand. J. Med. Sci. Sports 2018, 28, 2710–2722. [Google Scholar] [CrossRef]
- Ensari, I.; Motl, R.W.; Klaren, R.E.; Fernhall, B.; Smith, D.L.; Horn, G.P. Firefighter exercise protocols conducted in an environmental chamber: Developing a laboratory-based simulated firefighting protocol. Ergonomics 2017, 60, 657–668. [Google Scholar] [CrossRef]
- Magenes, G.; Curone, D.; Secco, E.L.; Bonfiglio, A. Biosensing and environmental sensing for emergency and protection e-Textiles. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Boston, MA, USA, 30 August–3 September 2011; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2011; pp. 8365–8366. [Google Scholar] [CrossRef]
- Ubiquitous Computing and Ambient Intelligence; Bravo, J., López-de-Ipiña, D., Moya, F., Eds.; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Massaroni, C.; Silvestri, S.; Schena, E. Comparison between heart rate estimated by single-lead ECG and optical-based wearable systems during outdoor running. In Proceedings of the 2024 IEEE International Workshop on Metrology for Industry 4.0 and IoT, MetroInd4.0 and IoT 2024, Firenze, Italy, 29–31 May 2024; pp. 407–411. [Google Scholar] [CrossRef]
- Massaroni, C.; Di Tocco, J.; Bravi, M.; Carnevale, A.; Presti, D.L.; Sabbadini, R.; Miccinilli, S.; Sterzi, A.; Formica, S.; Schena, E. Respiratory Monitoring during Physical Activities with a Multi-Sensor Smart Garment and Related Algorithms. IEEE Sens. J. 2020, 20, 2173–2180. [Google Scholar] [CrossRef]
- Pinnelli, M.; Presti, D.L.; Silvestri, S.; Setola, R.; Schena, E.; Massaroni, C. Towards the Instrumentation of Facemasks Used as Personal Protective Equipment for Unobtrusive Breathing Monitoring of Workers. Sensors 2024, 24, 5815. [Google Scholar] [CrossRef]
- Pinnelli, M.; Romano, C.; Pulcinelli, M.; Schena, E.; Silvestri, S.; Fortino, G.; Massaroni, C.; Setola, R.; Presti, D.L. A Wearable Platform as a First Step towards Enabling Collective Intelligence in Alzheimer’s Disease Management: Feasibility Assessment on Healthy Volunteers. In Proceedings of the 2024 IEEE International Workshop on Metrology for Industry 4.0 and IoT, MetroInd4.0 and IoT 2024, Firenze, Italy, 29–31 May 2024; pp. 395–400. [Google Scholar] [CrossRef]
- Nunan, D.; Sandercock, G.R.H.; Brodie, D.A. A Quantitative Systematic Review of Normal Values for Short-Term Heart Rate Variability in Healthy Adults. Pacing Clin. Electrophysiol. 2010, 33, 1407–1417. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Extra Beats Removed (Percentage of Removal) | |||||
|---|---|---|---|---|---|---|
| Stop 1 | Run 1 | Stop 2 | Run 2 | Fire | Stop 3 | |
| R1 | 52 (22%) | 5 (2%) | 0 (0%) | 3 (2%) | 0 (0%) | 0 (0%) |
| R2 | 8 (3%) | 7 (3%) | 0 (0%) | 0 (0%) | 11 (1%) | 0 (0%) |
| R3 | 90 (37%) | 173 (60%) | 3 (1%) | 74 (60%) | 247 (28%) | 0 (0%) |
| S1 | 0 (0%) | 86 (30%) | 0 (0%) | 61 (44%) | 22 (3%) | 0 (0%) |
| R4 | 35 (13%) | 12 (4%) | 3 (1%) | 22 (15%) | 29 (3%) | 3 (2%) |
| L2 | 10 (3%) | 110 (35%) | 13 (5%) | 23 (16%) | 27 (3%) | 0 (0%) |
| S2 | 88 (28%) | 109 (41%) | 36 (13%) | 48 (37%) | 100 (12%) | 0 (0%) |
| S3 | 0 (0%) | 39 (14%) | 0 (0%) | 33 (23%) | 76 (10%) | 3 (0%) |
| L3 | 0 (0%) | 30 (10%) | 7 (2%) | 18 (12%) | 10 (1%) | 0 (0%) |
| R1 | 0 (0%) | 0 (0%) | 0 (0%) | 1 (1%) | 34 (0%) | 0 (0%) |
| Stop 1 | Run 1 | Stop 2 | Run 2 | Fire | Stop 3 | |
|---|---|---|---|---|---|---|
| R1 | 10.1 ± 1.7 | 22.1 ± 6.0 | 12.9 ± 2.0 | 13.7 ± 8.9 | 24.3 ± 8.1 | 11.8 ± 0.8 |
| R2 | 12.5 ± 3.5 | 22.2 ± 6.6 | 19.3 ± 5.9 | 25.8 ± 11.4 | 20.6 ± 9.4 | 18.4 ± 5.9 |
| R3 | 11.2 ± 2.2 | 15.3 ± 2.7 | 13.4 ± 1.5 | 11.8 ± 6.4 | 20.4 ± 4.2 | 15.1 ± 2.4 |
| S1 | 15.7 ± 7.6 | 22.3 ± 1.8 | 15.8 ± 6.1 | 24.0 ± 1.4 | 15.5 ± 6.9 | 10.7 ± 2.3 |
| R4 | 14.6 ± 2.3 | 15.9 ± 1.6 | 17.0 ± 3.4 | 18.6 ± 7.2 | 33.5 ± 9.1 | 19.5 ± 0.9 |
| L2 | 15.4 ± 5.1 | 26.6 ± 7.4 | 22.2 ± 2.2 | 17.5 ± 6.1 | 15.1 ± 7.6 | 16.4 ± 7.9 |
| S2 | 21.7 ± 9.6 | 22.5 ± 11.8 | 26.7 ± 9.0 | 48.9 ± 25.5 | 23.5 ± 14.0 | 26.6 ± 9.2 |
| S3 | 17.3 ± 6.8 | 20.3 ± 10.6 | 26.1 ± 6.0 | 18.9 ± 11.6 | 16.4 ± 11.0 | 21.1 ± 6.8 |
| L3 | 11.5 ± 3.6 | 16.3 ± 4.9 | 21.0 ± 9.2 | 24.1 ± 18.0 | 16.2 ± 9.3 | 11.4 ± 1.9 |
| R6 | 17.9 ± 4.1 | 22.6 ± 3.8 | 20.7 ± 2.2 | 31.7 ± 2.8 | 26.8 ± 11.4 | 18.3 ± 6.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinnelli, M.; Marsella, S.; Tossut, F.; Schena, E.; Setola, R.; Massaroni, C. Field Testing Multi-Parametric Wearable Technologies for Wildfire Firefighting Applications. Sensors 2025, 25, 3066. https://doi.org/10.3390/s25103066
Pinnelli M, Marsella S, Tossut F, Schena E, Setola R, Massaroni C. Field Testing Multi-Parametric Wearable Technologies for Wildfire Firefighting Applications. Sensors. 2025; 25(10):3066. https://doi.org/10.3390/s25103066
Chicago/Turabian StylePinnelli, Mariangela, Stefano Marsella, Fabio Tossut, Emiliano Schena, Roberto Setola, and Carlo Massaroni. 2025. "Field Testing Multi-Parametric Wearable Technologies for Wildfire Firefighting Applications" Sensors 25, no. 10: 3066. https://doi.org/10.3390/s25103066
APA StylePinnelli, M., Marsella, S., Tossut, F., Schena, E., Setola, R., & Massaroni, C. (2025). Field Testing Multi-Parametric Wearable Technologies for Wildfire Firefighting Applications. Sensors, 25(10), 3066. https://doi.org/10.3390/s25103066