

Variability between Different Hand-Held Dynamometers for Measuring Muscle Strength
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Equipment
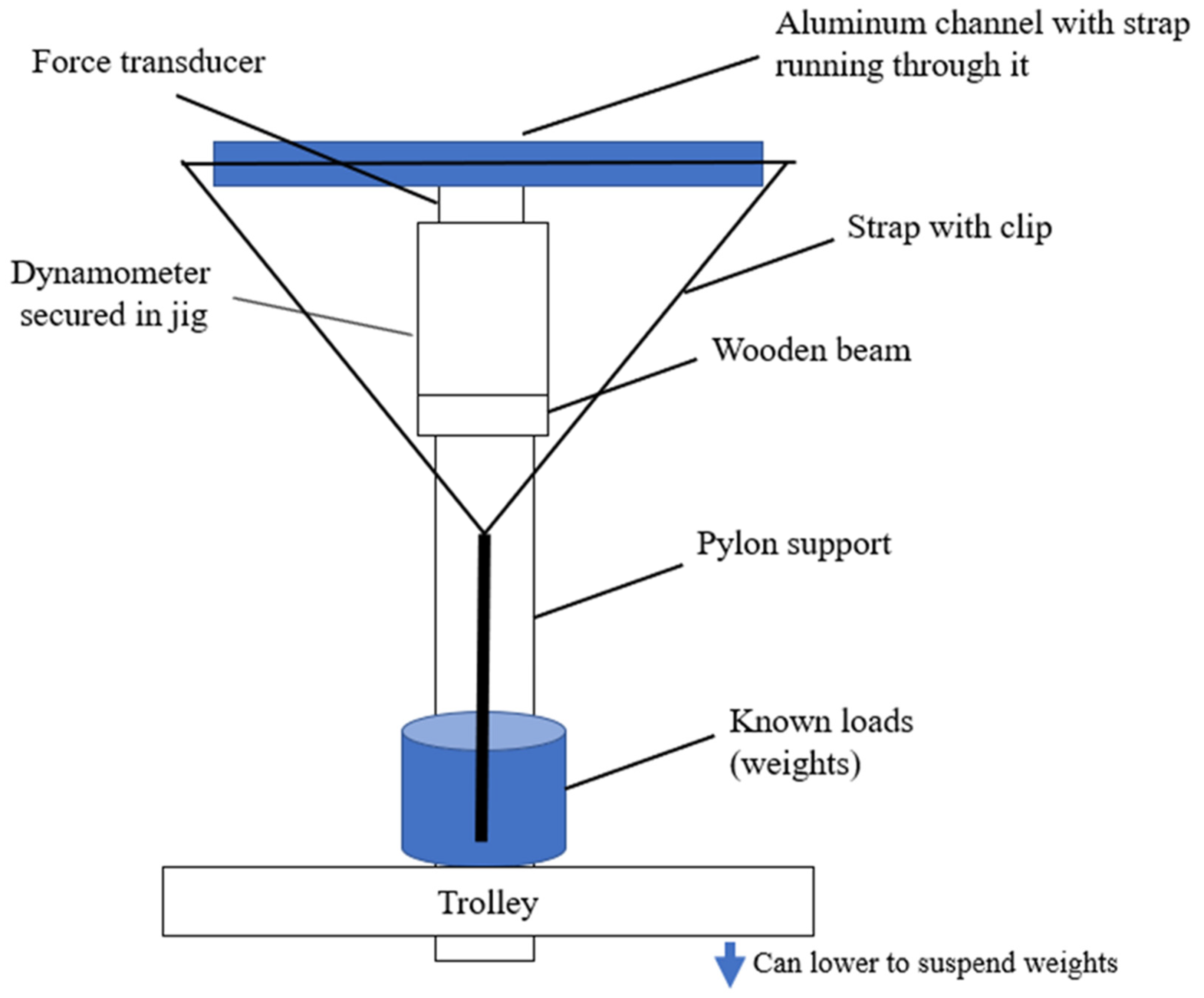
2.3. Calibration
2.4. Data Collection
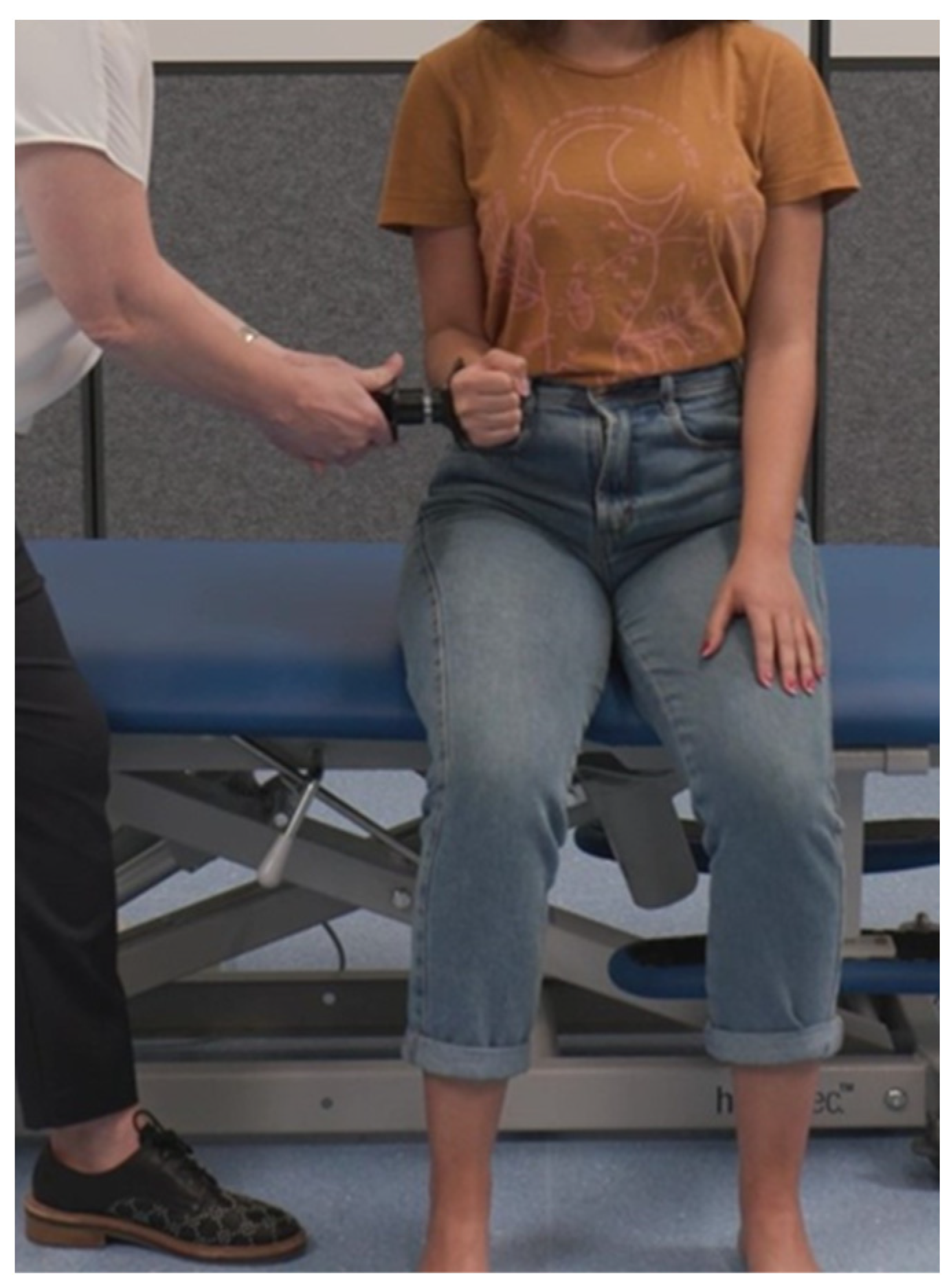
2.5. Isometric Muscle Strength Assessment Protocol
2.6. Data Analysis
3. Results
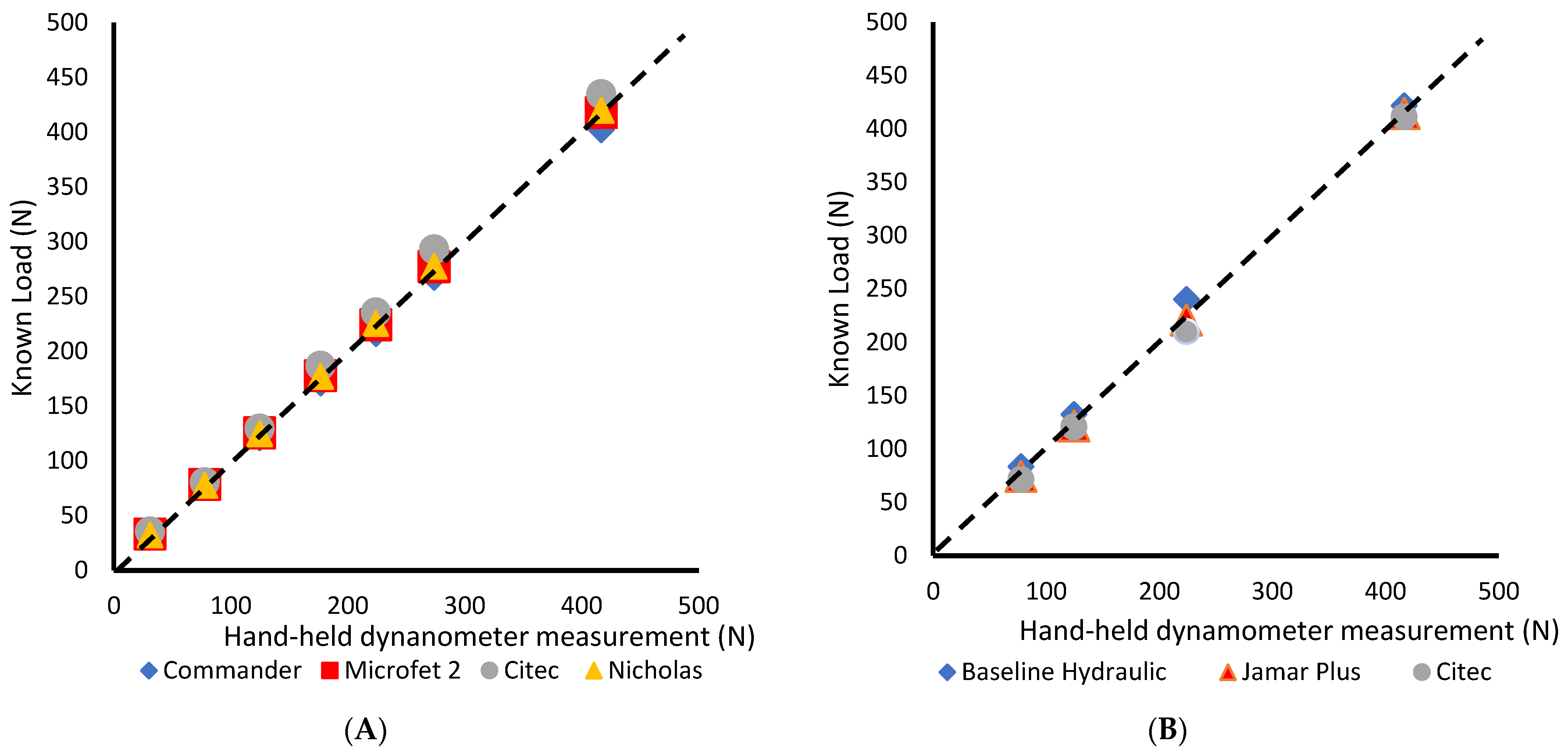
3.1. Calibration
3.2. Variability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stark, T.; Walker, B.; Phillips, J.K.; Fejer, R.; Beck, R. Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: A systematic review. PMR 2011, 3, 472–479. [Google Scholar] [CrossRef]
- Cuthbert, S.C.; Goodheart, G.J. On the reliability and validity of manual muscle testing: A literature review. Chiropr. Osteopat. 2007, 15, 4. [Google Scholar] [CrossRef]
- O’Neill, S.; Jaszczak, S.L.T.; Steffensen, A.K.S.; Debrabant, B. Using 4+ to grade near-normal muscle strength does not improve agreement. Chiropr. Man. Ther. 2017, 25, 28. [Google Scholar] [CrossRef]
- Morin, M.; Duchesne, E.; Bernier, J.; Blanchette, P.; Langlois, D.; Hébert, L.J. What is Known About Muscle Strength Reference Values for Adults Measured by Hand-Held Dynamometry: A Scoping Review. Arch. Rehabil. Res. Clin. Transl. 2021, 4, 100172. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Hand-held dynamometry: A practicable alternative for obtaining objective measures of muscle strength. Isokinet. Exerc. Sci. 2012, 20, 301–315. [Google Scholar]
- Mijnarends, D.M.; Meijers, J.M.; Halfens, R.J.; ter Borg, S.; Luiking, Y.C.; Verlaan, S.; Schoberer, D.; Jentoft, A.J.C.; van Loon, L.J.; Schols, J.M. Validity and reliability of tools to measure muscle mass, strength, and physical performance in community-dwelling older people: A systematic review. J. Am. Med. Dir. Assoc. 2013, 14, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Schrama, P.P.; Stenneberg, M.S.; Lucas, C.; Van Trijffel, E. Intraexaminer reliability of hand-held dynamometry in the upper extremity: A systematic review. Arch. Rehabil. Res. Clin. Transl. 2014, 95, 2444–2469. [Google Scholar] [CrossRef] [PubMed]
- Kolber, M.J.; Cleland, J.A. Strength testing using hand-held dynamometry. Phys. Ther. Rev. 2005, 10, 99–112. [Google Scholar] [CrossRef]
- Mori, L.; Prada, V.; Signori, A.; Pareyson, D.; Piscosquito, G.; Padua, L.; Pazzaglia, C.; Fabrizi, G.M.; Smania, N.; Picelli, A. Outcome measures in the clinical evaluation of ambulatory Charcot-Marie-Tooth 1A subjects. Eur. J. Phys. Rehabil. Med. 2019, 55, 47–55. [Google Scholar] [CrossRef]
- Burns, J.; Redmond, A.; Ouvrier, R.; Crosbie, J. Quantification of muscle strength and imbalance in neurogenic pes cavus, compared to health controls, using hand-held dynamometry. Foot Ankle Int. 2005, 26, 540–544. [Google Scholar] [CrossRef]
- Elsheikh, B.; King, W.; Peng, J.; Swoboda, K.J.; Reyna, S.P.; LaSalle, B.; Prior, T.W.; Arnold, W.D.; Kissel, J.T.; Kolb, S.J. Outcome measures in a cohort of ambulatory adults with spinal muscular atrophy. Muscle Nerve 2020, 61, 187–191. [Google Scholar] [CrossRef]
- Shefner, J.M. Strength testing in motor neuron diseases. Neurotherapeutics 2017, 14, 154–160. [Google Scholar] [CrossRef]
- Arnold, J.B.; Halstead, J.; Grainger, A.J.; Keenan, A.M.; Hill, C.L.; Redmond, A.C. Foot and leg muscle weakness in people with midfoot osteoarthritis. Arthritis Care Res. 2021, 73, 772–780. [Google Scholar] [CrossRef]
- Koblbauer, I.F.H.; Lambrecht, Y.; van der Hulst, M.L.M.; Neeter, C.; Engelbert, R.H.H.; Poolman, R.W.; Scholtes, V.A. Reliability of maximal isometric knee strength testing with modified hand-held dynamometry in patients awaiting total knee arthroplasty: Useful in research and individual patient settings? A reliability study. BMC Musculoskelet. Disord. 2011, 12, 249. [Google Scholar] [CrossRef]
- Baschung Pfister, P.; de Bruin, E.D.; Sterkele, I.; Maurer, B.; de Bie, R.A.; Knols, R.H. Manual muscle testing and hand-held dynamometry in people with inflammatory myopathy: An intra-and interrater reliability and validity study. PLoS ONE 2018, 13, e0194531. [Google Scholar] [CrossRef]
- Merlini, L.; Cecconi, I.; Parmeggiani, A.; Cordelli, D.M.; Dormi, A. Quadriceps muscle strength in Duchenne muscular dystrophy and effect of corticosteroid treatment. Acta Myol. 2020, 39, 200. [Google Scholar]
- do Amaral Benfica, P.; Aguiar, L.T.; de Brito, S.A.F.; Bernardino, L.H.N.; Teixeira-Salmela, L.F.; de Morais Faria, C.D.C. Reference values for muscle strength: A systematic review with a descriptive meta-analysis. Braz. J. Phys. Ther. 2018, 22, 355–369. [Google Scholar] [CrossRef]
- Douma, R.K.; Soer, R.; Krijnen, W.P.; Reneman, M.; Van Der Schans, C.P. Reference values for isometric muscle force among workers for the Netherlands: A comparison of reference values. BMC Sports Sci. Med. Rehabil. 2014, 6, 10. [Google Scholar] [CrossRef]
- Alvarenga, G.; Kiyomoto, H.D.; Martinez, E.C.; Polesello, G.; Alves, V.L.d.S. Normative isometric hip muscle force values assessed by a manual dynamometer. Acta Ortop. Bras. 2019, 27, 124–128. [Google Scholar] [CrossRef]
- Van Harlinger, W.; Blalock, L.; Merritt, J.L. Upper limb strength: Study providing normative data for a clinical handheld dynamometer. PMR 2015, 7, 135–140. [Google Scholar] [CrossRef]
- Ramskov, D.; Pedersen, M.; Kastrup, K.; Lønbro, S.; Jacobsen, J.; Thorborg, K.; Nielsen, R.; Rasmussen, S. Normative values of eccentric hip abduction strength in novice runners: An equation adjusting for age and gender. Int. J. Sports Phys. Ther. 2014, 9, 68. [Google Scholar]
- Bohannon, R.W. Reference values for extremity muscle strength obtained by hand-held dynamometry from adults aged 20 to 79 years. Arch. Phys. Med. Rehabil. 1997, 78, 26–32. [Google Scholar] [CrossRef]
- McKay, M.J.; Baldwin, J.N.; Ferreira, P.; Simic, M.; Vanicek, N.; Burns, J. Normative reference values for strength and flexibility of 1000 children and adults. Neurology 2017, 88, 36–43. [Google Scholar] [CrossRef]
- Beenakker, E.; Van der Hoeven, J.; Fock, J.; Maurits, N. Reference values of maximum isometric muscle force obtained in 270 children aged 4–16 years by hand-held dynamometry. Neuromuscul. Disord. 2001, 11, 441–446. [Google Scholar] [CrossRef]
- Amaral, J.F.; Mancini, M.; Novo Júnior, J.M. Comparison of three hand dynamometers in relation to the accuracy and precision of the measurements. Braz. J. Phys. Ther. 2012, 16, 216–224. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Vizenor, L.; Melander, D. Comparison of baseline instruments to the Jamar dynamometer and the B&L engineering pinch gauge. Occup. Ther. J. Res. 2000, 20, 147–162. [Google Scholar]
- Fenter, C.; Bellew, J.W.; Pitts, T.; Kay, R. A comparison of 3 hand-held dynamometers used to measure hip abduction strength. J. Strength. Cond. Res. 2003, 17, 531–535. [Google Scholar] [CrossRef]
- Kimura, I.F.; Jefferson, L.M.; Gulick, D.T.; Coll, R.D. Intra-and intertester reliability of Chatillon and Microfet hand-held dynamometers in measuring force production. J. Sport. Rehabil. 1996, 5, 197–205. [Google Scholar] [CrossRef][Green Version]
- McKay, M.J.; Baldwin, J.N.; Ferreira, P.; Simic, M.; Vanicek, N.; Hiller, C.E.; Nightingale, E.J.; Moloney, N.A.; Quinlan, K.G.; Pourkazemi, F.; et al. 1000 Norms Project: Protocol of a cross-sectional study cataloging human variation. Physiotherapy 2016, 102, 50–56. [Google Scholar] [CrossRef]
- Bohannon, R.W. Parallel comparison of grip strength measures obtained with a MicroFET 4 and a Jamar dynamometer. Percept. Mot. Skills. 2005, 100, 795–798. [Google Scholar] [CrossRef]
- Bohannon, R.W. Comparability of force measurements obtained with different strain gauge hand-held dynamometers. J. Orthop. Sports Phys. Ther. 1993, 18, 564–567. [Google Scholar] [CrossRef][Green Version]
- Mentiplay, B.F.; Perraton, L.G.; Bower, K.J.; Adair, B.; Pua, Y.-H.; Williams, G.P.; McGaw, R.; Clark, R.A. Assessment of lower limb muscle strength and power using hand-held and fixed dynamometry: A reliability and validity study. PLoS ONE 2015, 10, e0140822. [Google Scholar] [CrossRef]
- Phillips, B.A.; Lo, S.K.; Mastaglia, F.L. Muscle force measured using “break” testing with a hand-held myometer in normal subjects aged 20 to 69 years. Arch. Phys. Med. Rehabil. 2000, 81, 653–661. [Google Scholar] [CrossRef]
- Mathiowetz, V. Comparison of Rolyan and Jamar dynamometers for measuring grip strength. Occup. Ther. Int. 2002, 9, 201–209. [Google Scholar] [CrossRef]
- Shechtman, O.; Davenport, R.; Malcolm, M.; Nabavi, D. Reliability and validity of the BTE-Primus grip tool. J. Hand Ther. 2003, 16, 36–42. [Google Scholar] [CrossRef]
- Savas, S.; Kilavuz, A.; Kayhan Koçak, F.Ö.; Cavdar, S. Comparison of Grip Strength Measurements by Widely Used Three Dynamometers in Outpatients Aged 60 Years and Over. J. Clin. Med. 2023, 12, 4260. [Google Scholar] [CrossRef]
- McDowell, T.W.; Wimer, B.M.; Welcome, D.E.; Warren, C.; Dong, R.G. Effects of handle size and shape on measured grip strength. Int. J. Ind. Ergon. 2012, 42, 199–205. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dynamometer | Manufacturer | Unit Range | Muscle Groups |
|---|---|---|---|
| Citec Hand-held Dynamometer CT 3001 (Citec) | CIT Technics, Groningen, The Netherlands | 0–500 Newtons | Hand grip muscles Shoulder external rotators Hip internal rotators Ankle dorsiflexors |
| Lafayette Model 01163, Nicholas Manual Muscle Tester (Nicholas) | Lafayette Instrument, Lafayette, IN, USA | 0–1335 Newtons | Shoulder external rotators Hip internal rotators Ankle dorsiflexors |
| Hoggan MicroFET2 (MicroFET2) | Hoggan Scientific, LLC, Salt Lake City, UT, USA | 0–660 Newtons | Shoulder external rotators Hip internal rotators Ankle dorsiflexors |
| Commander PowerTrack II Muscle Tester (Commander) | JTECH Medical Industries, Inc. Midvale, UT, USA | 0–550 Newtons | Shoulder external rotators Hip internal rotators Ankle dorsiflexors |
| Baseline Hydraulic Hand Dynamometer, Model 10602 (Baseline Hydraulic) | Fabrications Enterprises, White Plains, NY, USA | 0–890 Newtons | Hand grip muscles |
| Jamar Plus Digital Hand Dynamometer (Jamar Plus) | Performance Health Supply, Cedarburg, WI, USA | 0–890 Newtons | Hand grip muscles |
| Muscle Group and Device | Mean (SD) | Range | Mean (SD) and Percentage Difference (%) | ||||
|---|---|---|---|---|---|---|---|
| Citec | Nicholas | Commander | MicroFET2 | ||||
| Shoulder External Rotation (N) | |||||||
| Citec | 98.1 (30.1) | 59.7–169.0 | 2.6 (10.6) 2.7% | 4.9 (11.2) 5.1% | 2.8 (8.1) 2.9% | ||
| Nicholas | 95.5 (26.2) | 63.1–169.7 | 2.6 (10.6) 2.7% | 2.3 (7.8) 2.4% | 0.2 (8.0) 0.2% | ||
| Commander | 93.2 (26.9) | 55.0–165.0 | 4.9 (11.2) 5.1% | 2.3 (7.8) 2.4% | 2.1 (7.8) 2.2% | ||
| MicroFET2 | 95.3 (27.7) | 60.2–160.0 | 2.8 (8.1) 2.9% | 0.2 (8.0) 0.2% | 2.1 (7.8) 2.2% | ||
| Hip Internal Rotation (N) | |||||||
| Citec | 168.9 (50.4) | 90.0–276.0 | 0.9 (18.5) 0.6% | 9.7 (18.7) 5.9% a | 2.2 (24.1) 1.3% | ||
| Nicholas | 167.8 (42.6) | 96.8–242.6 | 0.9 (18.5) 0.6% | 8.7 (15.0) 5.3% a | 1.3 (21.2) 0.6% | ||
| Commander | 159.2 (40.6) | 94.1–242.0 | 9.7 (18.7) 5.9% a | 8.7 (15.0) 5.3% a | 7.5 (21.8) 4.5% | ||
| MicroFET2 | 166.7 (47.8) | 97.8–264.5 | 2.2 (24.1) 1.3% | 1.3 (21.2) 0.6% | 7.5 (21.8) 4.5% | ||
| Ankle Dorsiflexion (N) | |||||||
| Citec | 254.6 (53.5) | 111.0–359.7 | 8.0 (32.8) 3.1% | 3.4 (33.7) 1.3% | 6.3 (25.1) 2.4% | ||
| Nicholas | 262.6 (52.3) | 122.3–350.1 | 8.0 (32.8) 3.1% | 11.3 (29.3) 4.4% | 1.7 (28.4) 0.6% | ||
| Commander | 251.3 (44.5) | 165.7–338.3 | 3.4 (33.7) 1.3% | 11.3 (29.3) 4.4% | 9.6 (25.2) 3.7% | ||
| MicroFET2 | 260.9 (52.2) | 127.7–338.5 | 6.3 (25.1) 2.4% | 1.7 (28.4) 0.6% | 9.6 (25.2) 3.7% | ||
| Hand Grip (N) | Citec | Jamar Plus | Baseline Hydraulic | ||||
| Citec | 284.0 (83.9) | 149.3–457.3 | 45.2 (50.5) 14.7% b | 49.5 (56.7) 16.0% b | |||
| Jamar Plus | 329.2 (95.0) | 209.9–494.6 | 45.2 (50.5) 14.7% b | 4.3 (37.4) 1.3% | |||
| Baseline Hydraulic | 333.5 (103.6) | 176.5–575.7 | 49.5 (56.7) 16.0% b | 4.3 (37.4) 1.3% | |||
| Citec (subgroup, n = 8) | 242.0 (29.3) | 202.7–296.0 | 11.7 (27.2) 4.7% | 6.5 (29.4) 2.7% | |||
| Jamar Plus (subgroup, n = 8) | 253.7 (37.8) | 209.9–310.9 | 11.7 (27.2) 4.7% | 5.2 (30.5) 2.1% | |||
| Baseline Hydraulic (subgroup, n = 8) | 248.5 (28.2) | 215.8–307.3 | 6.5 (29.4) 2.7% | 5.2 (30.5) 2.1% | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, W.; Cornett, K.M.D.; Donlevy, G.A.; Burns, J.; McKay, M.J. Variability between Different Hand-Held Dynamometers for Measuring Muscle Strength. Sensors 2024, 24, 1861. https://doi.org/10.3390/s24061861
Du W, Cornett KMD, Donlevy GA, Burns J, McKay MJ. Variability between Different Hand-Held Dynamometers for Measuring Muscle Strength. Sensors. 2024; 24(6):1861. https://doi.org/10.3390/s24061861
Chicago/Turabian StyleDu, William, Kayla M. D. Cornett, Gabrielle A. Donlevy, Joshua Burns, and Marnee J. McKay. 2024. "Variability between Different Hand-Held Dynamometers for Measuring Muscle Strength" Sensors 24, no. 6: 1861. https://doi.org/10.3390/s24061861
APA StyleDu, W., Cornett, K. M. D., Donlevy, G. A., Burns, J., & McKay, M. J. (2024). Variability between Different Hand-Held Dynamometers for Measuring Muscle Strength. Sensors, 24(6), 1861. https://doi.org/10.3390/s24061861