
Does Overhead Squat Performance Affect the Swing Kinematics and Lumbar Spine Loads during the Golf Downswing?



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Protocol
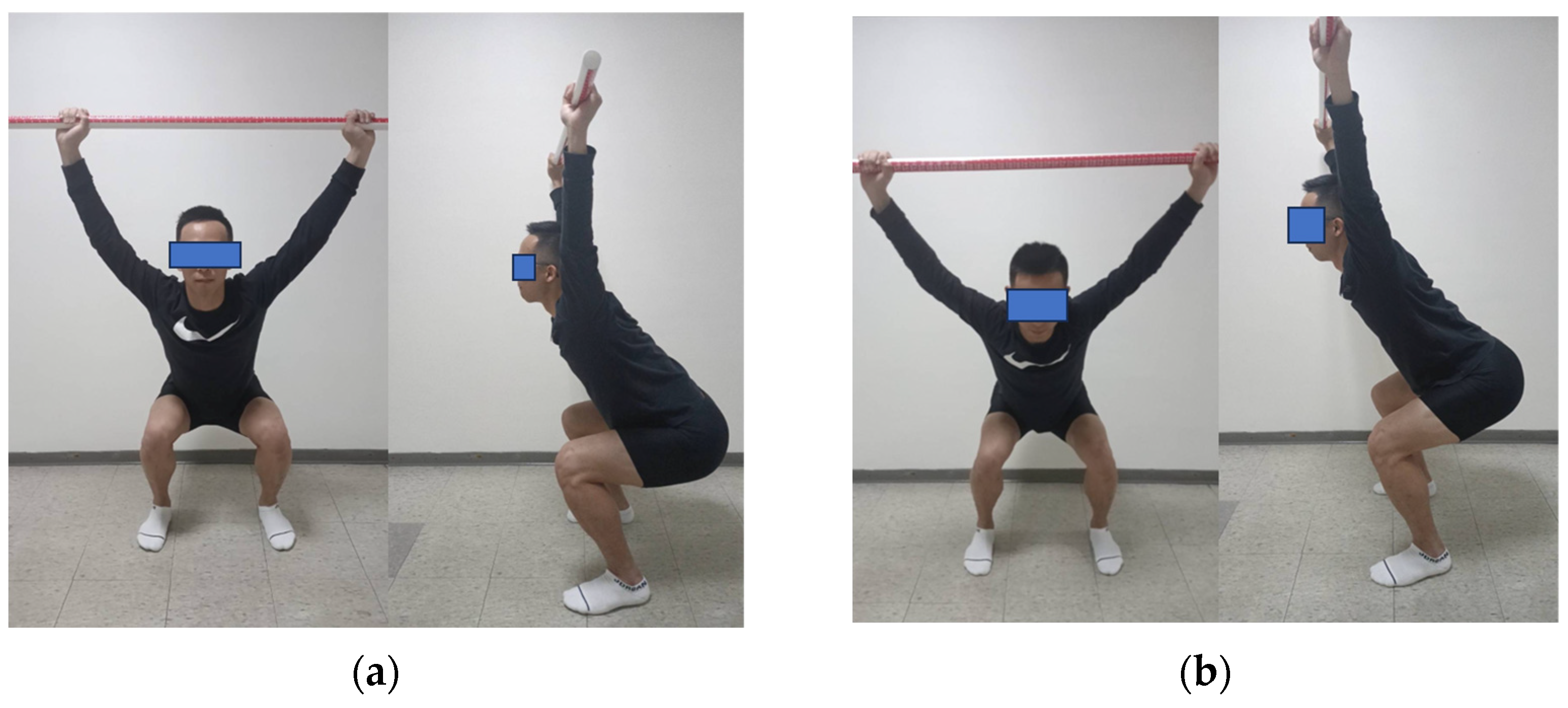
2.3. Overhead Squat Test
2.4. Kinematic and Kinetic Data Collection
2.5. Computer Simulation
2.6. Statistical Analyses
3. Results
3.1. Lumbar Joint Kinematics during the Downswing
3.2. Lumbar Joint Loads during the Downswing
4. Discussion
4.1. Influence of the OHS on Golf Performance
4.2. The Influence of the OHS on Lumbar Spine Kinematics in the Sagittal Plane
4.3. Impact of the OHS on Lumbar Spine Kinematics in the Frontal Plane
4.4. Impact of the OHS on Lumbar Spine Loads
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lindsay, D.M.; Vandervoort, A.A. Golf-related low back pain: A review of causative factors and prevention strategies. Asian J. Sports Med. 2014, 5, e24289. [Google Scholar] [CrossRef]
- Versteegh, T.H.; Vandervoort, A.A.; Lindsay, D.M.; Lynn, S.K. Fitness, performance and injury prevention strategies for the senior golfer. Int. J. Sports Sci. Coach. 2008, 3 (Suppl. S1), 199–214. [Google Scholar] [CrossRef]
- Cann, A.P.; Vandervoort, A.A.; Lindsay, D.M. Optimizing the benefits versus risks of golf participation by older people. J. Geriatr. Phys. Ther. 2005, 28, 85–92. [Google Scholar] [CrossRef]
- Thériault, G.; Lachance, P. Golfing injuries. An overview. Sports Med. 1993, 16, 64–71. [Google Scholar]
- McCarroll, J.R.; Gioe, T.J. Professional golfers and the price they pay. Physician Sports Med. 1982, 10, 64–70. [Google Scholar] [CrossRef]
- Gosheger, G.; Liem, D.; Ludwig, K.; Greshake, O.; Winkelmann, W. Injuries and overuse syndromes in golf. Am. J. Sports Med. 2003, 31, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.H.; Grimshaw, P.N. The biomechanics of the modern golf swing: Implications for lower back injuries. Sports Med. 2016, 46, 339–351. [Google Scholar] [CrossRef]
- McHardy, A.J.; Pollard, H.P.; Luo, K. Golf-related lower back injuries: An epidemiological survey. J. Chiropr. Med. 2007, 6, 20–26. [Google Scholar] [CrossRef]
- Hosea, T.M.; Gatt, C.J., Jr. Back pain in golf. Clin. Sports Med. 1996, 15, 37–53. [Google Scholar] [CrossRef] [PubMed]
- Cook, G.; Burton, L.; Hoogenboom, B. Pre-participation screening: The use of fundamental movements as an assessment of function–part 1. N. Am. J. Sports Phys. Ther. 2006, 1, 62. [Google Scholar] [PubMed]
- Kritz, M.; Cronin, J.; Hume, P. The bodyweight squat: A movement screen for the squat pattern. Strength Cond. J. 2009, 31, 76–85. [Google Scholar] [CrossRef]
- Gulgin, H.R.; Schulte, B.C.; Crawley, A.A. Correlation of Titleist Performance Institute (TPI) level 1 movement screens and golf swing faults. J. Strength Cond. Res. 2014, 28, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Speariett, S.; Armstrong, R. The relationship between the Golf-Specific Movement Screen and golf performance. J. Sport Rehabil. 2019, 29, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.; Sugaya, H.; Banks, S.; Cook, F. A new ‘twist’ on golf kinematics and low back injuries: The crunch factor. In Proceedings of the 21st Annual Meeting of the American Society of Biomechanics, Clemson, SC, USA, 27 September 1997; pp. 24–27. [Google Scholar]
- Lindsay, D.M.; Horton, J.F.; Paley, R.D. Trunk motion of male professional golfers using two different golf clubs. J. Appl. Biomech. 2002, 18, 366–373. [Google Scholar] [CrossRef]
- Grimshaw, P.N.; Burden, A.M. Case report: Reduction of low back pain in a professional golfer. Med. Sci. Sports Exerc. 2000, 32, 1667–1673. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.J.; Peng, Y.C.; Yang, C.J.; Hsu, C.Y.; Hamill, J.; Tang, W.T. Lower Limb Biomechanics during the Golf Downswing in Individuals with and without a History of Knee Joint Injury. Bioengineering 2023, 10, 626. [Google Scholar] [CrossRef] [PubMed]
- Eric, S.; Jennifer, S. Sports Injury: Prevention & Rehabilitation; McGraw-Hill: New York, NY, USA, 2001. [Google Scholar]
- Dolan, P.; Adams, M.A. Influence of lumbar and hip mobility on the bending stresses acting on the lumbar spine. Clin. Biomech. 1993, 8, 185–192. [Google Scholar] [CrossRef]
- Horton, J.F. Abdominal Muscle Characteristics of Elite Male Golfers with and without Chronic Low Back Pain. 2000. Available online: https://cir.nii.ac.jp/crid/1130000798217084800 (accessed on 31 December 2023).
- Hosea, T. Biomechanical analysis of the golfer’s back. In Science and Golf; Routledge: London, UK, 1990; pp. 43–48. [Google Scholar]
- Lim, Y.T.; Chow, J.W.; Chae, W.S. Lumbar spinal loads and muscle activity during a golf swing. Sports Biomech. 2012, 11, 197–211. [Google Scholar] [CrossRef]
- Crosby, B.R.; Stanek, J.M.; Dodd, D.J.; Begalle, R.L. Analysis of Preferred Footwear on Weight Bearing Scores Using the Functional Movement Screen. Int. J. Athl. Ther. Train. 2018, 23, 101–107. [Google Scholar] [CrossRef]
- Delp, S.L.; Anderson, F.C.; Arnold, A.S.; Loan, P.; Habib, A.; John, C.T.; Guendelman, E.; Thelen, D.G. OpenSim: Open-source software to create and analyze dynamic simulations of movement. IEEE Trans. Biomed. Eng. 2007, 54, 1940–1950. [Google Scholar] [CrossRef]
- Raabe, M.E.; Chaudhari, A.M. An investigation of jogging biomechanics using the full-body lumbar spine model: Model development and validation. J. Biomech. 2016, 49, 1238–1243. [Google Scholar] [CrossRef] [PubMed]
- Steele, K.M.; DeMers, M.S.; Schwartz, M.H.; Delp, S.L. Compressive tibiofemoral force during crouch gait. Gait Posture 2012, 35, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Seth, A.; Hicks, J.L.; Uchida, T.K.; Habib, A.; Dembia, C.L.; Dunne, J.J.; Ong, C.F.; DeMers, M.S.; Rajagopal, A.; Millard, M.; et al. OpenSim: Simulating musculoskeletal dynamics and neuromuscular control to study human and animal movement. PLoS Comput. Biol. 2018, 14, e1006223. [Google Scholar] [CrossRef] [PubMed]
- Sell, T.C.; Tsai, Y.S.; Smoliga, J.M.; Myers, J.B.; Lephart, S.M. Strength, flexibility, and balance characteristics of highly proficient golfers. J. Strength Cond. Res. 2007, 21, 1166–1171. [Google Scholar]
- Sato, K.; Kenny, I.C. Current golf performance literature and application to training. J. Trainol. 2013, 2, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Haher, T.R.; O’Brien, M.; Kauffman, C.; Liao, K.C. Biomechanics of the spine in sports. Clin. Sports Med. 1993, 12, 449–464. [Google Scholar] [CrossRef] [PubMed]
- Burnett, A.; O’Sullivan, P.; Ankarberg, L.; Gooding, M.; Nelis, R.; Offermann, F.; Persson, J. Lower lumbar spine axial rotation is reduced in end-range sagittal postures when compared to a neutral spine posture. Man. Ther. 2008, 13, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Vad, V.B.; Bhat, A.L.; Basrai, D.; Gebeh, A.; Aspergren, D.D.; Andrews, J.R. Low back pain in professional golfers: The role of associated hip and low back range-of-motion deficits. Am. J. Sports Med. 2004, 32, 494–497. [Google Scholar] [CrossRef]
- Nikolai, B. Clinical Anatomy of the Lumbar Spine and Sacrum; Elsevier Health Sciences: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Joyce, C.; Burnett, A.; Cochrane, J.; Ball, K. Three-dimensional trunk kinematics in golf: Between-club differences and relationships to clubhead speed. Sports Biomech. 2013, 12, 108–120. [Google Scholar] [CrossRef]
- Putnam, C.A. Sequential motions of body segments in striking and throwing skills: Descriptions and explanations. J. Biomech. 1993, 26, 125–135. [Google Scholar] [CrossRef]
- Crews, D.; Lutz, R. Comparison of kinematic sequence parameters between amateur and professional golfers. Sci. Golf 2007, 5, 30–36. [Google Scholar]
- Lindsay, D.M.; Horton, J.F. Comparison of spine motion in elite golfers with and without low back pain. In Science and Golf IV; Routledge: Oxfordshire, UK, 2012; pp. 77–87. [Google Scholar]
- Kim, S.B.; You, J.S.H.; Kwon, O.Y.; Yi, C.H. Lumbopelvic kinematic characteristics of golfers with limited hip rotation. Am. J. Sports Med. 2015, 43, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.H.; Grimshaw, P.N. The crunch factor’s role in golf-related low back pain. Spine J. 2014, 14, 799–807. [Google Scholar] [CrossRef]
- Bae, T.S.; Cho, W.; Kim, K.H.; Chae, S.W. Biomechanical effect of altered lumbar lordosis on intervertebral lumbar joints during the golf swing: A simulation study. J. Biomech. Eng. 2014, 136, 111005. [Google Scholar] [CrossRef] [PubMed]
- Hutton, W.C.; Stott, J.R.R.; Cyron, B.M. Is spondylolysis a fatigue fracture? Spine 1977, 2, 202–209. [Google Scholar] [CrossRef]
- Cyron, B.M.; Hutton, W.C. The fatigue strength of the lumbar neural arch in spondylolysis. J. Bone Jt. Surg. Br. Vol. 1978, 60, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Sugaya, H. Low back injury in elite and professional golfers: An epidemiologic and radiographic study. In Science and GolfIII, Proceedings of the 3rd World Scientific Congress of Golf; Human Kinetics: Champaign, IL, USA, 1998; pp. 83–91. [Google Scholar]
- Moore, K.L.; Dalley, A.F.; Agur, A.M. Clinically Oriented Anatomy; Wolters kluwer india Pvt Ltd.: Chandigarh, India, 2018. [Google Scholar]
- Monteiro, E.R.; Škarabot, J.; Vigotsky, A.D.; Brown, A.F.; Gomes, T.M.; da Silva Novaes, J. Acute effects of different self-massage volumes on the fms™ overhead deep squat performance. Int. J. Sports Phys. Ther. 2017, 12, 94. [Google Scholar]
- Egret, C.I.; Vincent, O.; Weber, J.; Dujardin, F.H.; Chollet, D. Analysis of 3D kinematics concerning three different clubs in golf swing. Int. J. Sports Med. 2003, 24, 465–470. [Google Scholar]
- Edwards, N.; Dickin, C.; Wang, H. Low back pain and golf: A review of biomechanical risk factors. Sports Med. Health Sci. 2020, 2, 10–18. [Google Scholar] [CrossRef]
- Christopher, J. An examination of the correlation amongst trunk flexibility, x-factor and clubhead speed in skilled golfers. J. Sports Sci. 2017, 35, 2035–2041. [Google Scholar]
- Tsai, Y.S.; Sell, T.C.; Smoliga, J.M.; Myers, J.B.; Learman, K.E.; Lephart, S.M. A comparison of physical characteristics and swing mechanics between golfers with and without a history of low back pain. J. Orthop. Sports Phys. Ther. 2010, 40, 430–438. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Tests | 3 Points | 2 Points | 1 Point | 0 Points |
|---|---|---|---|---|
| Overhead Squat | Upper torso is parallel with tibia or toward vertical. | Meet criteria of 3 points with 2 × 6 board under heels. | Tibia and upper torso are not parallel. | If pain is associated with any portion of this test. |
| Femur is below horizontal. Knees are aligned over feet. Dowel is aligned over feet. | Knees are not aligned over feet. | Femur is not below horizontal. Knees are not aligned over feet. Lumbar flexion is noted. |
| Mean (SD) | df | t | p | ||
|---|---|---|---|---|---|
| LS-G (N = 11) | HS-G (N = 10) | ||||
| Downswing time (s) | 0.29 (0.06) | 0.30 (0.03) | 19 | −0.78 | 0.452 |
| Height (m) | 1.68 (0.10) | 1.61 (0.05) | 19 | 2.00 | 0.061 |
| Weight (kg) | 75.00 (14.37) | 68.06 (13.67) | 19 | 1.13 | 0.268 |
| Best scores | 68.45 (3.14) | 69.90 (4.07) | 19 | −0.92 | 0.367 |
| Ball speed (mph) | 142.44 (16.95) | 126.29 (11.52) | 19 | 2.53 | 0.022 * |
| Mean (SD) | df | t | p | ||
|---|---|---|---|---|---|
| LS-G (N = 11) | HS-G (N = 10) | ||||
| Lumbar flexion angle at impact (°) | −21.37 (6.39) | −26.20 (5.90) | 19 | 1.792 | 0.089 |
| Lumbar angular extension displacement (°) | 17.72 (5.94) | 24.36 (7.11) | 19 | −2.33 | 0.031 * |
| Lumbar peak extension angular velocity (°/s) | 119.52 (59.23) | 40.51 (26.79) | 19 | 3.87 | 0.000 *** |
| Lumbar peak flexion angular velocity (°/s) | −269.34 (181.03) | −288.95 (162.68) | 19 | 0.26 | 0.798 |
| Mean (SD) | df | t | p | ||
|---|---|---|---|---|---|
| LS-G (N = 11) | HS-G (N = 10) | ||||
| Lumbar right-side bending angle at impact (°) 1 | 21.07 (0.48) | 20.93 (0.70) | 19 | 0.55 | 0.591 |
| Lumbar angular bending displacement (°) 1 | 34.89 (5.95) | 31.21 (7.28) | 19 | −1.27 | 0.218 |
| Lumbar peak right-side bending angular velocity (°/s) 1 | 329.35 (43.79) | 287.42 (62.27) | 19 | 1.80 | 0.088 |
| Mean (SD) | df | t | p | ||
|---|---|---|---|---|---|
| LS-G (N = 11) | HS-G (N = 10) | ||||
| L1-L2 | 712.67 (74.46) | 737.97 (133.89) | 19 | −0.54 | 0.594 |
| L2-L3 | 487.45 (70.43) | 530.31 (104.34) | 19 | −1.11 | 0.280 |
| L3-L4 | 327.81 (75.54) | 337.94 (56.10) | 19 | −0.35 | 0.733 |
| L4-L5 | 387.19 (89.16) | 299.54 (37.30) | 19 | 2.88 | 0.010 ** |
| L5-S1 | 525.19 (86.69) | 407.90 (59.06) | 19 | 3.59 | 0.002 ** |
| Mean (SD) | df | t | p | ||
|---|---|---|---|---|---|
| LS-G (N = 11) | HS-G (N = 10) | ||||
| L1-L2 | 3018.92 (233.43) | 3059.77 (356.55) | 19 | −0.31 | 0.757 |
| L2-L3 | 3412.79 (289.78) | 3515.89 (424.28) | 19 | −0.66 | 0.520 |
| L3-L4 | 3668.80 (326.21) | 3797.82 (443.92) | 19 | −0.76 | 0.454 |
| L4-L5 | 3770.94 (338.66) | 3921.69 (450.25) | 19 | −0.87 | 0.394 |
| L5-S1 | 3759.18 (328.70) | 3918.67 (447.88) | 19 | −0.94 | 0.361 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.-H.; Pandy, M.; Huang, T.-Y.; Tang, W.-T. Does Overhead Squat Performance Affect the Swing Kinematics and Lumbar Spine Loads during the Golf Downswing? Sensors 2024, 24, 1252. https://doi.org/10.3390/s24041252
Chen Z-H, Pandy M, Huang T-Y, Tang W-T. Does Overhead Squat Performance Affect the Swing Kinematics and Lumbar Spine Loads during the Golf Downswing? Sensors. 2024; 24(4):1252. https://doi.org/10.3390/s24041252
Chicago/Turabian StyleChen, Zi-Han, Marcus Pandy, Tsung-Yu Huang, and Wen-Tzu Tang. 2024. "Does Overhead Squat Performance Affect the Swing Kinematics and Lumbar Spine Loads during the Golf Downswing?" Sensors 24, no. 4: 1252. https://doi.org/10.3390/s24041252
APA StyleChen, Z.-H., Pandy, M., Huang, T.-Y., & Tang, W.-T. (2024). Does Overhead Squat Performance Affect the Swing Kinematics and Lumbar Spine Loads during the Golf Downswing? Sensors, 24(4), 1252. https://doi.org/10.3390/s24041252