
Obesity-Specific Considerations for Assessing Gait with Inertial Measurement Unit-Based vs. Optokinetic Motion Capture


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
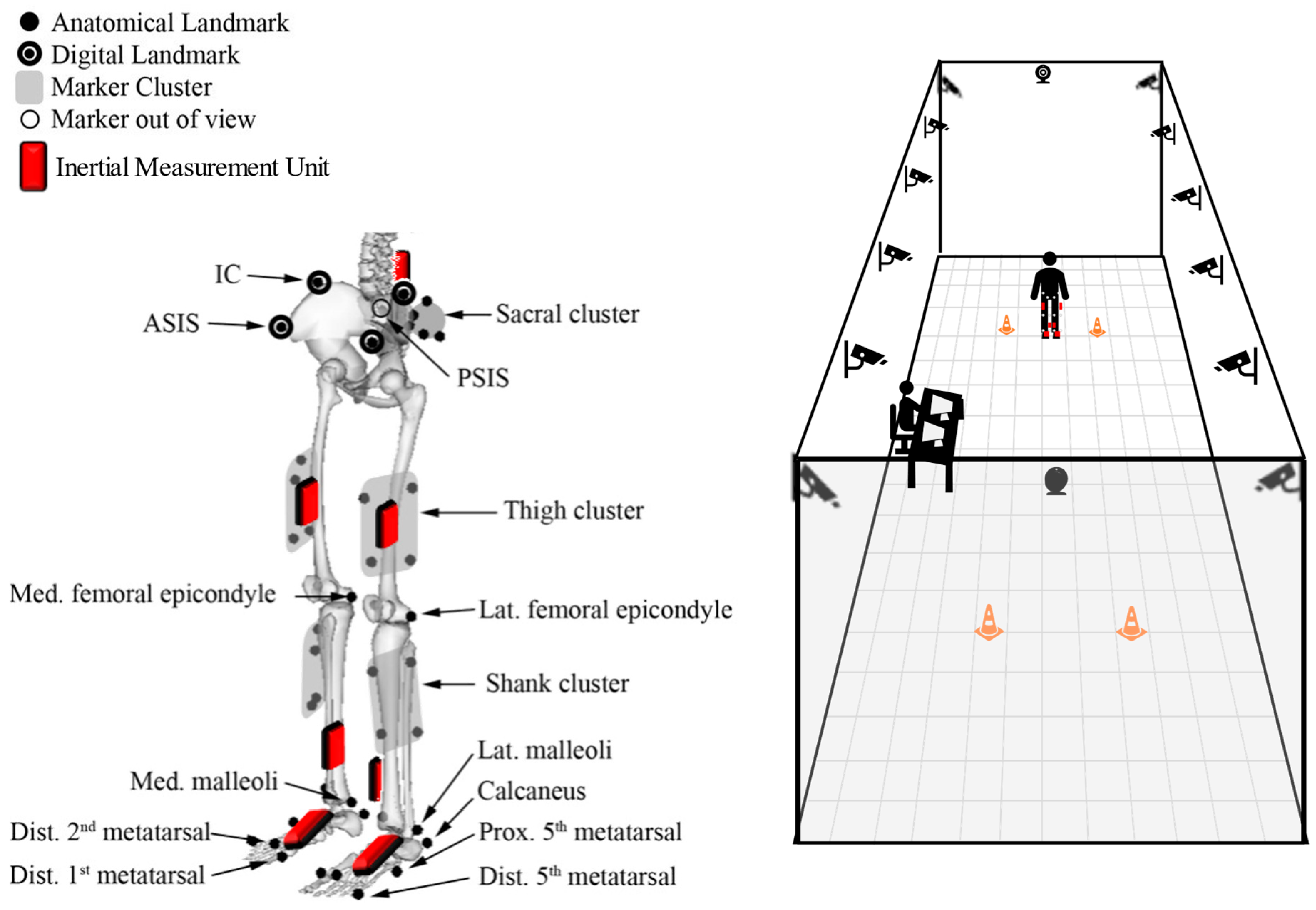
2.2. Procedures
2.3. Data Analysis
2.4. Statistical Analysis
2.4.1. Participant Summary
2.4.2. System Summary
2.4.3. System Differences
2.4.4. Clinical Applications
3. Results
3.1. Participant Summary
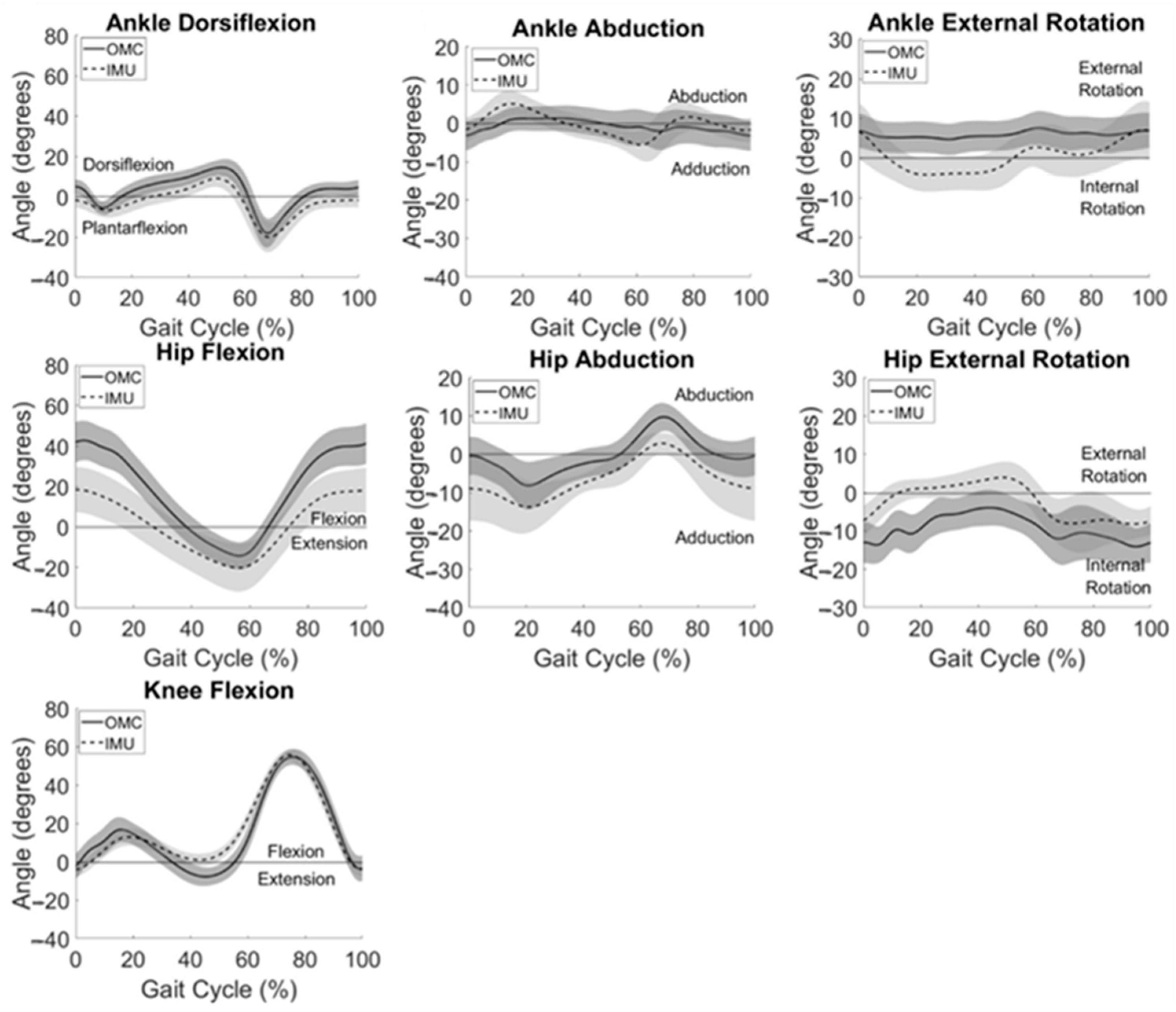
3.2. System Summary
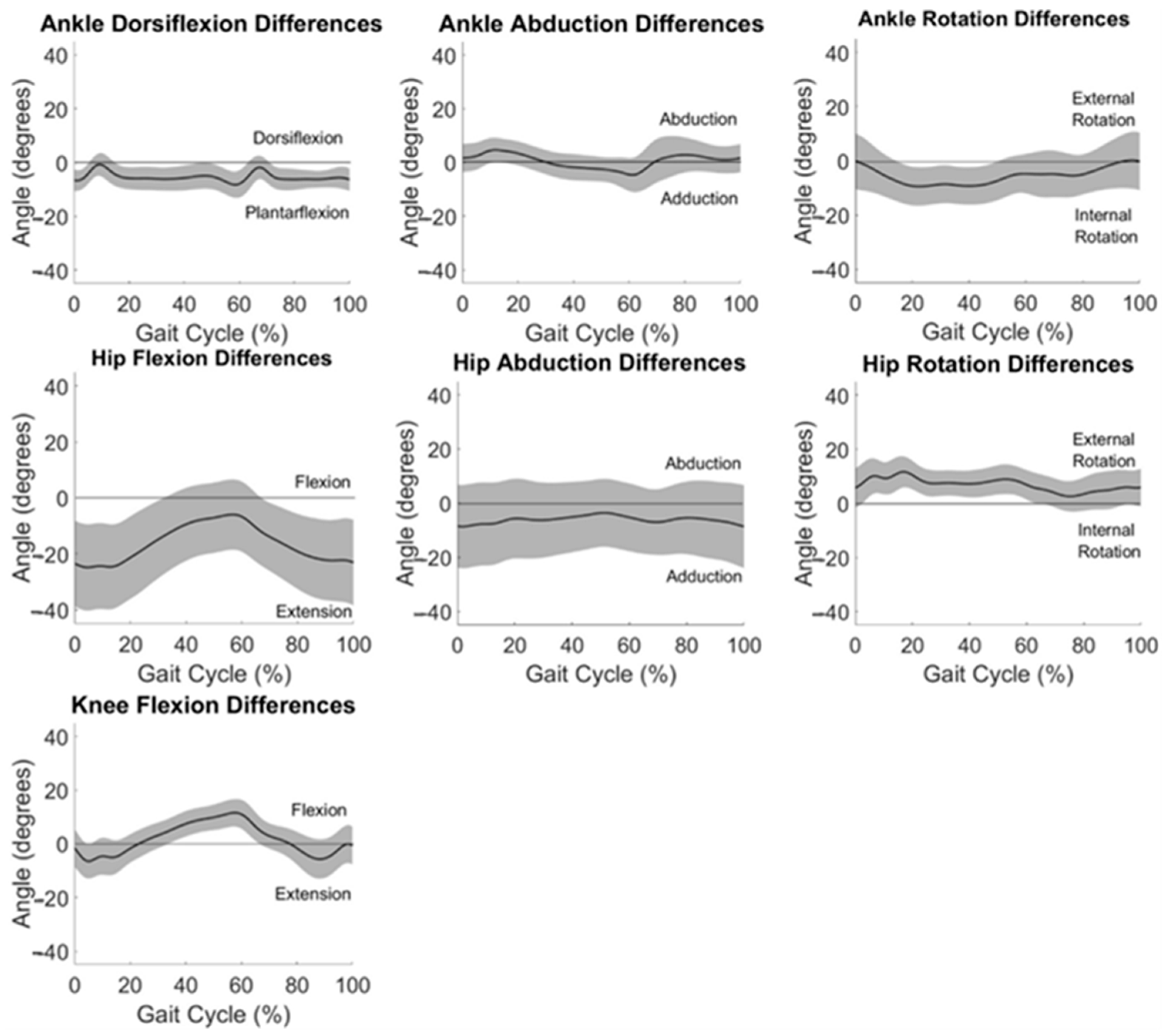
3.3. System Differences
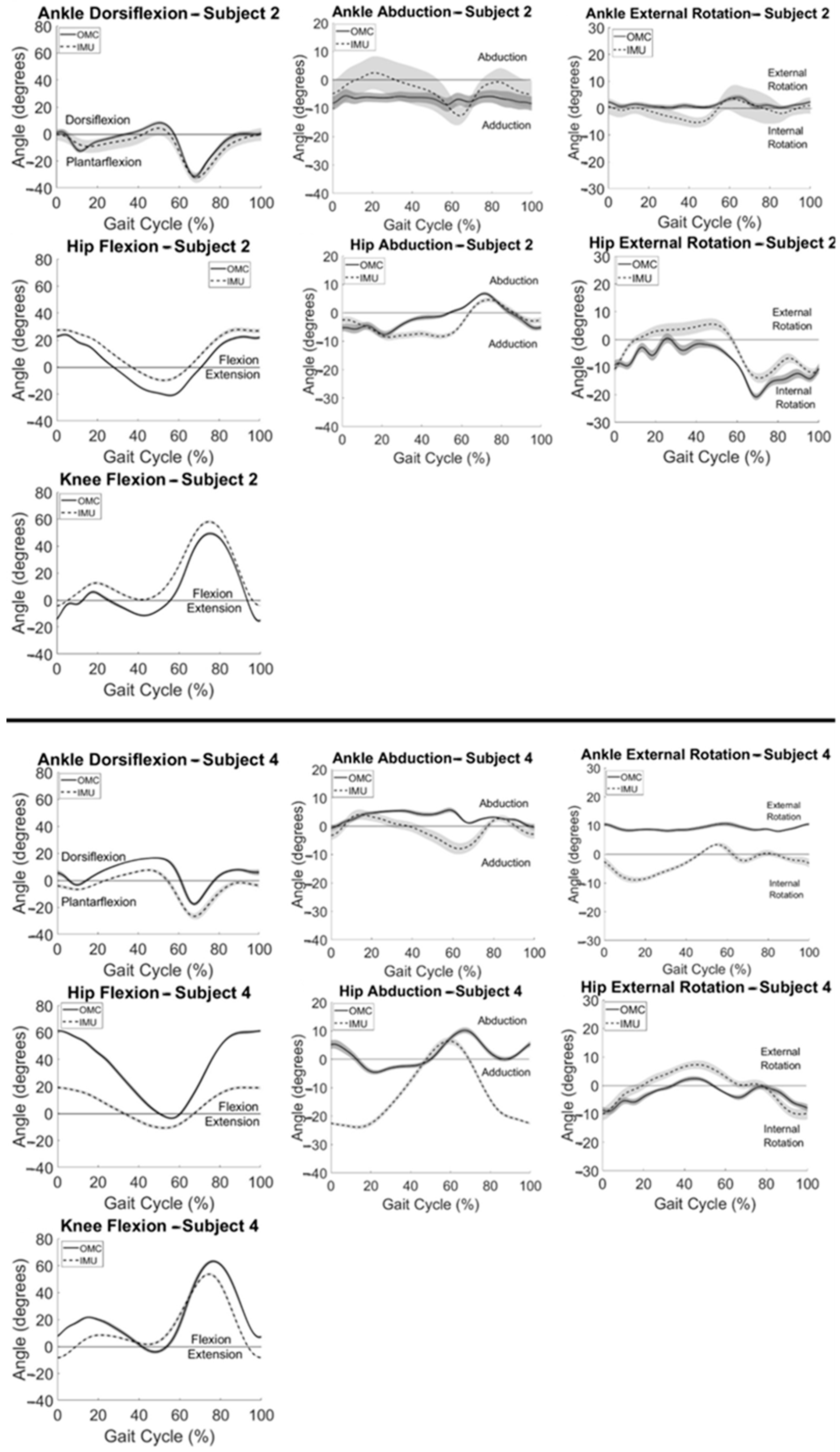
3.4. Clinical Application
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of obesity among adults and youth: United States, 2017–2018. NCHS Data Brief 2020. Available online: https://www.cdc.gov/nchs/data/databriefs/db360-h.pdf (accessed on 30 November 2023).
- Blaszczyk, J.; Plewa, M.; Cieslinska-Swider, J.; Bacik, B.; Zahorska-Markiewicz, B.; Markiewicz, A. Impact of excess body weight on walking at the preferred speed. Acta Neurobiol. Exp. 2011, 71, 528–540. [Google Scholar] [CrossRef] [PubMed]
- Lockhart, T.E.; Frames, C.W.; Soangra, R.; Lieberman, A. Effects of Obesity and Fall Risk on Gait and Posture of Community-Dwelling Older Adults. Int. J. Progn. Health Manag. 2019, 10, 019. [Google Scholar] [CrossRef] [PubMed]
- Naugle, K.M.; Higgins, T.J.; Manini, T.M. Obesity and use of compensatory strategies to perform common daily activities in pre-clinically disabled older adults. Arch. Gerontol. Geriatr. 2012, 54, e134–e138. [Google Scholar] [CrossRef] [PubMed]
- Houston, D.K.; Ding, J.; Nicklas, B.J.; Harris, T.B.; Lee, J.S.; Nevitt, M.C.; Rubin, S.M.; Tylavsky, F.A.; Kritchevsky, S.B. Overweight and obesity over the adult life course and incident mobility limitation in older adults: The health, aging and body composition study. Am. J. Epidemiol. 2009, 169, 927–936. [Google Scholar] [CrossRef]
- Bell, J.A.; Sabia, S.; Singh-Manoux, A.; Hamer, M.; Kivimaki, M. Healthy obesity and risk of accelerated functional decline and disability. Int. J. Obes. 2017, 41, 866–872. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, Y.-Z.; Xiao, F.; Gu, D.-Y. Kinematic characteristics of gait in middle-aged adults during level walking. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 6915–6918. [Google Scholar] [CrossRef]
- Kuo, A.D.; Donelan, J.M. Dynamic principles of gait and their clinical implications. Phys. Ther. 2010, 90, 157–174. [Google Scholar] [CrossRef] [PubMed]
- Saint-Maurice, P.F.; Troiano, R.P.; Bassett, D.R.; Graubard, B.I.; Carlson, S.A.; Shiroma, E.J.; Fulton, J.E.; Matthews, C.E. Association of Daily Step Count and Step Intensity With Mortality Among US Adults. J. Am. Med. Assoc. 2020, 323, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, E.J.; Richardson, J.; McCallum, C.A.; Wilhelm, M. The Predictive Validity of Physical Performance Measures in Determining Markers of Preclinical Disability in Community-Dwelling Middle-Aged and Older Adults: A Systematic Review. Phys. Ther. 2018, 98, 1010–1021. [Google Scholar] [CrossRef]
- Tao, W.; Liu, T.; Zheng, R.; Feng, H. Gait Analysis Using Wearable Sensors. Sensors 2012, 12, 2255–2283. Available online: https://www.mdpi.com/1424-8220/12/2/2255 (accessed on 30 November 2023). [CrossRef]
- Chen, S.; Lach, J.; Lo, B.; Yang, G.-Z. Toward Pervasive Gait Analysis With Wearable Sensors: A Systematic Review. IEEE J. Biomed. Health Inform. 2016, 20, 1521–1537. [Google Scholar] [CrossRef]
- de Bruin, E.D.; Hartmann, A.; Uebelhart, D.; Murer, K.; Zijlstra, W. Wearable systems for monitoring mobility-related activities in older people: A systematic review. Clin. Rehabil. 2008, 22, 878–895. [Google Scholar] [CrossRef] [PubMed]
- Rekant, J.; Rothenberger, S.; Chambers, A. Inertial measurement unit-based motion capture to replace camera-based systems for assessing gait in healthy young adults: Proceed with caution. Meas. Sens. 2022, 23, 100396. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.-S.; Jang, S.-H.; Cho, J.-S.; Kim, M.-J.; Lee, H.D.; Lee, S.Y.; Moon, S.-B. Evaluation of Validity and Reliability of Inertial Measurement Unit-Based Gait Analysis Systems. Ann. Rehabil. Med. 2018, 42, 872–883. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Yoon, S. Validity Evaluation of an Inertial Measurement Unit (IMU) in Gait Analysis Using Statistical Parametric Mapping (SPM). Sensors 2021, 21, 3667. [Google Scholar] [CrossRef] [PubMed]
- Lerner, Z.F.; Board, W.J.; Browning, R.C. Effects of an obesity-specific marker set on estimated muscle and joint forces in walking. Med. Sci. Sports Exerc. 2014, 46, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Mei, Q.; Kim, H.K.; Xiang, L.; Shim, V.; Wang, A.; Baker, J.S.; Gu, Y.; Fernandez, J. Toward improved understanding of foot shape, foot posture, and foot biomechanics during running: A narrative review. Front. Physiol. 2022, 13, 1062598. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion--part I: Ankle, hip, and spine. International Society of Biomechanics. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Grood, E.S.; Suntay, W.J. A joint coordinate system for the clinical description of three-dimensional motions: Application to the knee. J. Biomech. Eng. 1983, 105, 136–144. [Google Scholar] [CrossRef]
- Fettrow, T.; DiBianca, S.; dos Santos, F.V.; Reimann, H.; Jeka, J. Flexible Recruitment of Balance Mechanisms to Environmental Constraints during Walking. Front. Virtual Real. 2020, 1, 5. [Google Scholar] [CrossRef]
- Ferrari, A.; Cutti, A.G.; Cappello, A. A new formulation of the coefficient of multiple correlation to assess the similarity of waveforms measured synchronously by different motion analysis protocols. Gait Posture 2010, 31, 540–542. [Google Scholar] [CrossRef]
- Pagnon, D.; Domalain, M.; Reveret, L. Pose2Sim: An End-to-End Workflow for 3D Markerless Sports Kinematics-Part 2: Accuracy. Sensors 2022, 22, 2712. [Google Scholar] [CrossRef]
- Kaufman, K.R.; Hughes, C.; Morrey, B.F.; Morrey, M.; An, K.-N. Gait characteristics of patients with knee osteoarthritis. J. Biomech. 2001, 34, 907–915. [Google Scholar] [CrossRef]
- Ginis, P.; Pirani, R.; Basaia, S.; Ferrari, A.; Chiari, L.; Heremans, E.; Canning, C.G.; Nieuwboer, A. Focusing on heel strike improves toe clearance in people with Parkinson’s disease: An observational pilot study. Physiotherapy 2017, 103, 485–490. [Google Scholar] [CrossRef]
- Shan, G.; Zhang, H.; Jiang, T. Correlation Coefficients for a Study with Repeated Measures. Comput. Math. Methods Med. 2020, 2020, 7398324. [Google Scholar] [CrossRef]
- Hamlett, A.; Ryan, L.; Wolfinger, R. On the use of PROC MIXED to estimate correlation in the presence of repeated measures. In Proceedings of the Statistics and Data Analysis Section; SAS Users Group International: Cary, NC, USA, 2004; pp. 1–7. [Google Scholar]
- Altman, D.G.; Bland, J.M. Measurement in Medicine: The Analysis of Method Comparison Studies. J. R. Stat. Society. Ser. D (Stat.) 1983, 32, 307–317. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The reliability of three-dimensional kinematic gait measurements: A systematic review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Berner, K.; Cockcroft, J.; Morris, L.D.; Louw, Q. Concurrent validity and within-session reliability of gait kinematics measured using an inertial motion capture system with repeated calibration. J. Bodyw. Mov. Ther. 2020, 24, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Rekant, J.; Chambers, A. Validation of Inertial Measurement Unit-Based Motion Capture with a Single Calibration File for Assessing Gait in Healthy Young Adults. SSRN 2022, 22, 20. [Google Scholar] [CrossRef]
- Lenz, A.L.; Strobel, M.A.; Anderson, A.M.; Fial, A.V.; MacWilliams, B.A.; Krzak, J.J.; Kruger, K.M. Assignment of local coordinate systems and methods to calculate tibiotalar and subtalar kinematics: A systematic review. J. Biomech. 2021, 120, 110344. [Google Scholar] [CrossRef]
- Montefiori, E.; Fiifi Hayford, C.; Mazzà, C. Variations of lower-limb joint kinematics associated with the use of different ankle joint models. J. Biomech. 2022, 136, 111072. [Google Scholar] [CrossRef] [PubMed]
- Della Croce, U.; Leardini, A.; Chiari, L.; Cappozzo, A. Human movement analysis using stereophotogrammetry. Part 4: Assessment of anatomical landmark misplacement and its effects on joint kinematics. Gait Posture 2005, 21, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Garcia, S.A.; Vakula, M.N.; Holmes, S.C.; Pamukoff, D.N. The influence of body mass index and sex on frontal and sagittal plane knee mechanics during walking in young adults. Gait Posture 2021, 83, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Segal, N.A.; Yack, H.J.; Khole, P. Weight, Rather Than Obesity, Distribution, Explains Peak External Knee Adduction Moment During Level Gait. Am. J. Phys. Med. Rehabil. 2009, 88, 180–188. [Google Scholar] [CrossRef]
- Harrington, M.; Zavatsky, A.; Lawson, S.; Yuan, Z.; Theologis, T. Prediction of the hip joint centre in adults, children, and patients with cerebral palsy based on magnetic resonance imaging. J. Biomech. 2007, 40, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Kainz, H.; Carty, C.P.; Modenese, L.; Boyd, R.N.; Lloyd, D.G. Estimation of the hip joint centre in human motion analysis: A systematic review. Clin. Biomech. 2015, 30, 319–329. [Google Scholar] [CrossRef]
- Macleod, C.A.; Conway, B.A.; Allan, D.B.; Galen, S.S. Development and validation of a low-cost, portable and wireless gait assessment tool. Med. Eng. Phys. 2014, 36, 541–546. [Google Scholar] [CrossRef][Green Version]
- Müller, B.; Ilg, W.; Giese, M.A.; Ludolph, N. Validation of enhanced kinect sensor based motion capturing for gait assessment. PLoS ONE 2017, 12, e0175813. [Google Scholar] [CrossRef]
- Wang, S.; Zeng, X.; Huangfu, L.; Xie, Z.; Ma, L.; Huang, W.; Zhang, Y. Validation of a portable marker-based motion analysis system. J. Orthop. Surg. Res. 2021, 16, 425. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ankle Dorsiflexion | Ankle Abduction | Ankle Rotation | Hip Flexion | Hip Abduction | Hip Rotation | Knee Flexion | |
|---|---|---|---|---|---|---|---|
| Subject 1 | 0.59 | nan # | nan # | 0.95 | nan # | nan # | 0.99 |
| Subject 2 a | 0.91 | nan # | nan # | 0.92 | 0.75 | 0.79 | 0.94 |
| Subject 3 | 0.65 | nan # | 0.30 | 0.80 | 0.88 | 0.34 | 0.98 |
| Subject 4 b | 0.71 | nan # | nan # | 0.33 | nan # | 0.75 | 0.89 |
| Subject 5 | 0.98 | nan # | nan # | 0.77 | 0.56 | 0.78 | 0.96 |
| Subject 6 | 0.95 | nan # | nan # | 0.76 | 0.90 | nan # | 0.92 |
| Subject 7 | 0.97 | 0.37 | nan # | nan # | nan # | 0.50 | 0.97 |
| Subject 8 | 0.93 | nan # | nan # | 0.64 | nan # | 0.87 | 0.93 |
| Subject 9 | 0.67 | nan # | nan # | 0.94 | 0.56 | nan # | 0.97 |
| Subject 10 | 0.80 | 0.39 | nan # | 0.50 | 0.94 | 0.31 | 0.99 |
| Timepoint | |||
|---|---|---|---|
| Heel Strike | Maximum/Minimum | ||
| Motion | Ankle Dorsiflexion | 0.38 | 0.83 |
| Hip Flexion | −0.05 | 0.15 | |
| Knee Flexion | 0.18 | 0.00 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rekant, J.; Rothenberger, S.; Chambers, A. Obesity-Specific Considerations for Assessing Gait with Inertial Measurement Unit-Based vs. Optokinetic Motion Capture. Sensors 2024, 24, 1232. https://doi.org/10.3390/s24041232
Rekant J, Rothenberger S, Chambers A. Obesity-Specific Considerations for Assessing Gait with Inertial Measurement Unit-Based vs. Optokinetic Motion Capture. Sensors. 2024; 24(4):1232. https://doi.org/10.3390/s24041232
Chicago/Turabian StyleRekant, Julie, Scott Rothenberger, and April Chambers. 2024. "Obesity-Specific Considerations for Assessing Gait with Inertial Measurement Unit-Based vs. Optokinetic Motion Capture" Sensors 24, no. 4: 1232. https://doi.org/10.3390/s24041232
APA StyleRekant, J., Rothenberger, S., & Chambers, A. (2024). Obesity-Specific Considerations for Assessing Gait with Inertial Measurement Unit-Based vs. Optokinetic Motion Capture. Sensors, 24(4), 1232. https://doi.org/10.3390/s24041232