1. Introduction
Low back pain (LBP) is the main cause of absenteeism and disability in industrialized societies. Prolonged duration of LBP can significantly affect quality of life due to biomechanical alterations, such as movement alteration, muscular compensation, pustular change, joint degeneration or core dysfunction, reducing the ability to perform daily activities [
1]. LBP is an extremely common symptom worldwide and occurs in all age groups, from children to the elderly population [
2]. Approximately 10–20% of patients develop chronic LBP, defined as pain and disability persisting for more than 12 weeks [
3]. Therefore, there is a clear necessity of reducing the disability caused by this problem; hence, efficient methodologies are needed to improve the function of people suffering these problems.
Traditional physiotherapy treatments have proven to be effective in enhancing function and reducing disability in patients with chronic LBP. Therefore, graded activity or exercise programs that focus on improving function and preventing disability are recommended as primary treatment strategies [
4]. Consequently, there is a heightened focus on physical treatments that allow self-management, with less emphasis on pharmacological and surgical interventions [
4].
Analyzing how a patient responds to a therapeutic approach by administering pre-treatment and post-treatment tests can help determine whether this should be modified, substituted or discontinued [
5,
6]. In this regard, some researchers propose the use of tools and indicators to assess the minimal detectable change (MDC) in order to evaluate and ensure actual response to treatments in clinical practice [
5,
6]. The use of these kinds of tools could reduce or facilitate the monitoring of the effect of treatments without the need to constantly test patients with questionnaire-based measures [
7].
The MDC is the minimum quantity of change that can be detected in order to be considered “real” instead of that resulting from potential measurement error [
5]. This index represents the variability of the measures of each variable. If a change of one variable is detected and it is lower than its MDC value, it would not be considered statistically significant, since it is lower than the variability of the test [
8]. The MDC is important for clinical decision-making because it can provide a threshold value for therapists, clinical therapists, and clinical researchers to determine whether the results represent a real change or reflect intrinsic variability of measurement [
9].
The integration of MDC into therapeutic strategies such as DOT or traditional physiotherapy treatment facilitates the evaluation of patient progress. Consequently, physicians are able to monitor patient improvement to ensure that the administered treatments or therapies are yielding satisfactory outcomes [
6]. Currently, assessing improvements is normally conducted through qualitative techniques after treatment, either by observation of body movements or through interviews with the patient, as is used for assessing the state of patients before treatment [
10]. As exemplified by Marín et al. [
10,
11], the integration of inertial measurement units (IMUs) for movement analysis via full-body motion capture (MoCap) into rehabilitation assessment based on medical examination is feasible. This is mainly because IMU-based technologies are amongst the most prevalent methodologies employed for MoCap.
MoCap provides information about spatio-temporal and kinematic variables [
10,
11,
12]. These variables are particularly useful for monitoring the progress of patients with musculoskeletal disorders and can offer many opportunities in the field of rehabilitation to aid decision-making using measurements before and after treatment, intervention, or therapy [
5,
10,
11,
13,
14]. IMUs are electronic devices that capture motion through signal processing of output data from various embedded sensors (accelerometers, gyroscopes, and magnetometers) [
15,
16,
17]. In addition, IMUs have become particularly important because they do not require external cameras and can be embedded in wearable technology [
6,
18].
Despite the ostensibly broad applicability of clinical movement analysis [
19,
20], its comprehensive integration into routine clinical practice encounters certain hurdles, most notably the complexity of data analysis stemming from measurement processes. This necessitates the development of strategies for the automatic and consistent processing of the spatiotemporal and kinematic variables information that is generated [
10,
12]. A particular requirement is the standardization of methods to facilitate a comparative analysis of variables generated from two distinct measurement sessions, for instance, those conducted pre-and post-treatment, or at different junctures during the rehabilitation process [
11]. Furthermore, the incorporation of MoCap-based tests needs to address the inherent heterogeneity among patients in routine clinical rehabilitation practice. This entails surmounting the challenge of carrying out individual patient assessments, tracking intra-patient session data over time, individually managing recovery trajectories, and comparing the efficacy of treatments across diverse patient profiles [
11].
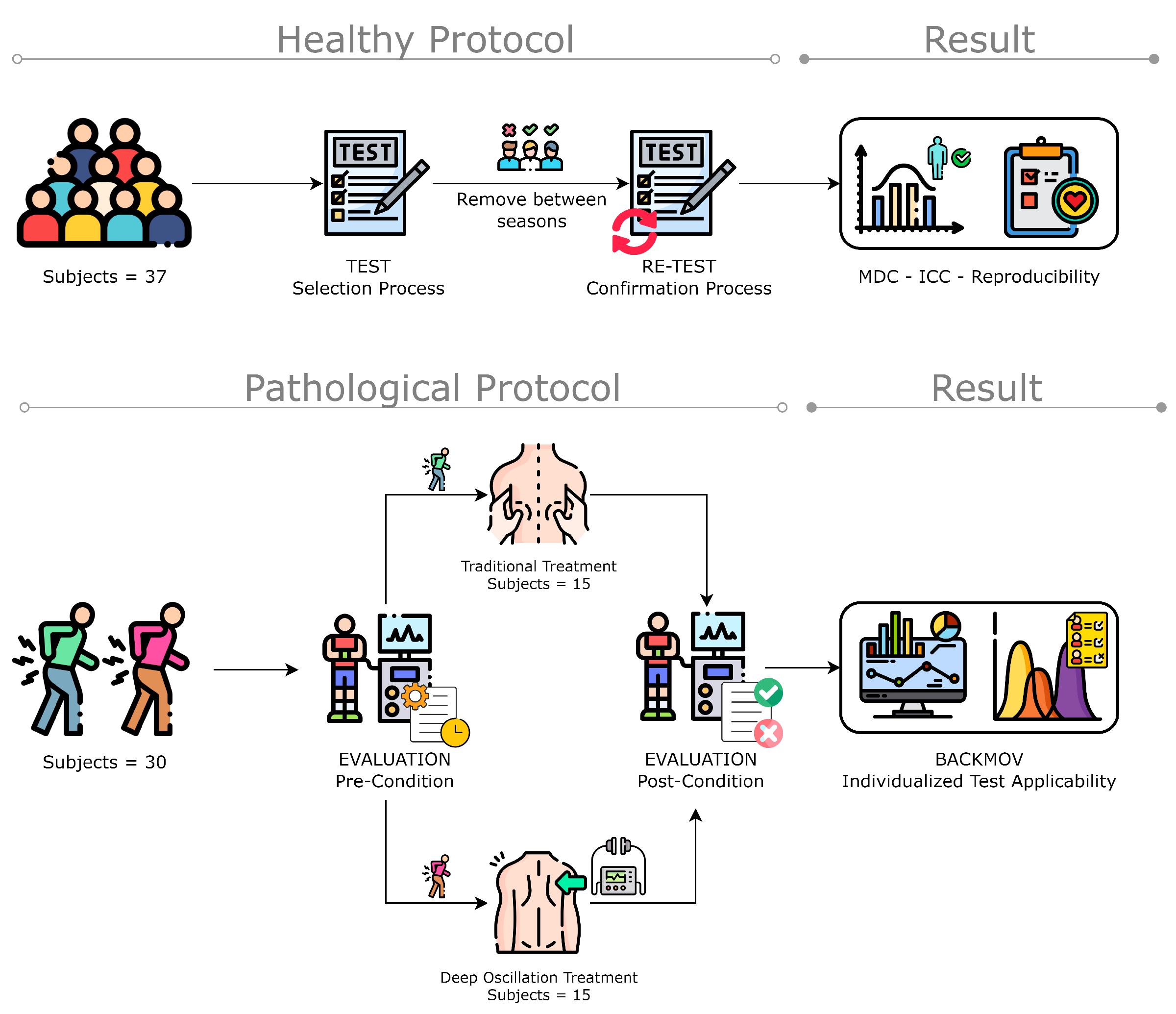
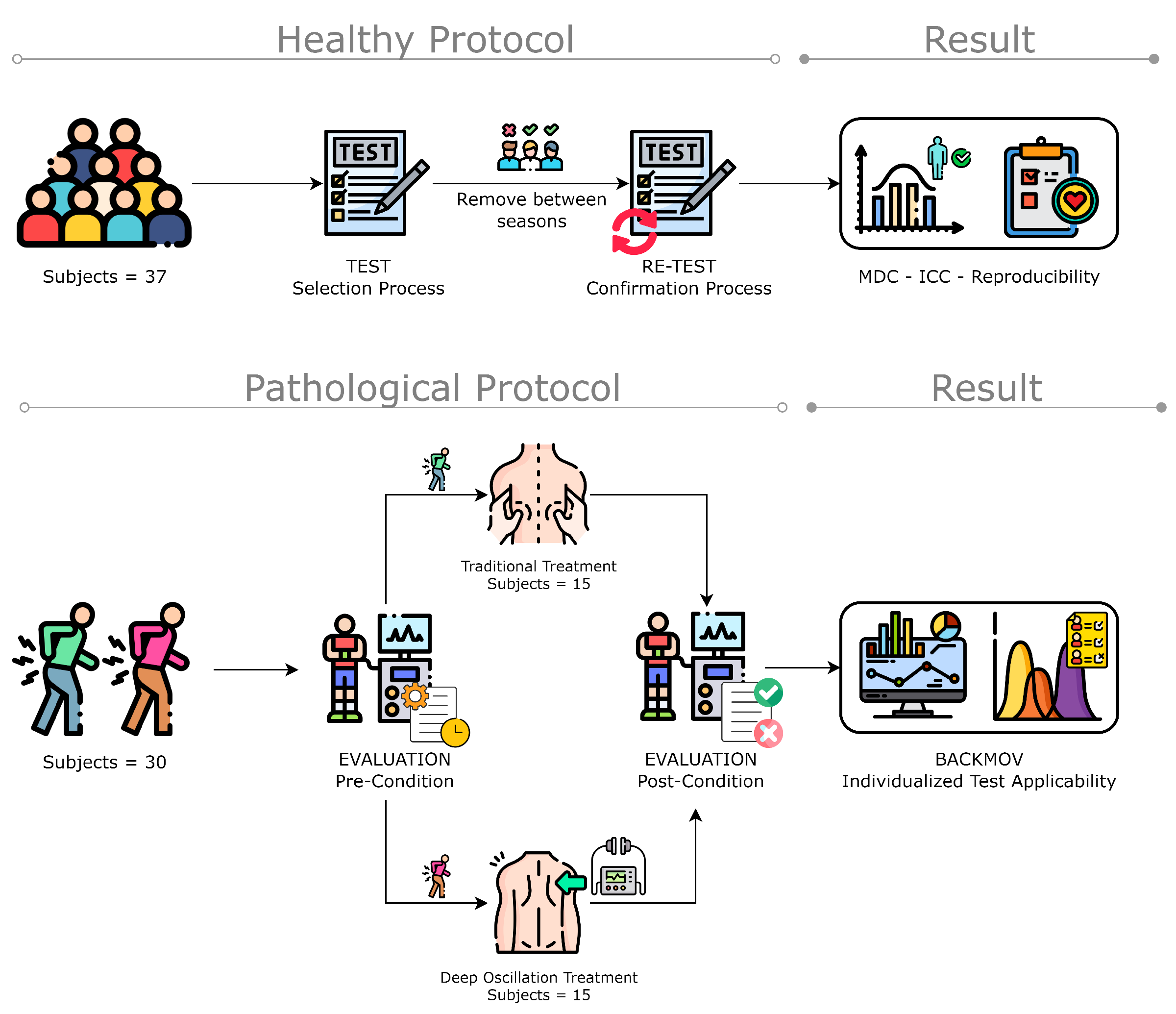
This study introduces the BackMov test, leveraging inertial MoCap sensor technology for comprehensive lumbar movement analysis. Crafted to objectively track patient progress during rehabilitation, the BackMov test involves two pivotal measurement sessions: pre- and post-treatment. The primary goal is to precisely quantify advancements or setbacks in patients with low back pain (LBP) post-rehabilitation, establishing a correlation between positive changes in kinematic variables of lumbar movements and recovery after therapy. To validate the test’s reliability, a test-retest involving three lumbar movements was conducted on 37 healthy volunteers, utilizing the minimal detectable change (MDC) as a statistical benchmark.
To illustrate its clinical relevance, the BackMov test was administered to 30 LBP-diagnosed patients, capturing the same three-segment movement before and after therapy. The resulting data were then compared to evaluations by a specialist physician. Considered as a novel tool, the BackMov test aims to provide a quantifiable assessment of movement recovery in LBP patients post-therapy. By doing so, it can support specialists in determining the efficacy of treatments in restoring mobility, thereby reducing the disability caused by LBP. The BackMov test enhances decision-making and introduces a systematic approach to the management and treatment of LBP, offering tailored patient monitoring to ensure more effective rehabilitation strategies.
2. Materials and Methods
2.1. Participants and Protocol
In this study, 37 healthy volunteers, both male and female, were recruited to determine the reproducibility of the test using the minimum detectable change (MDC) criterion. A call for volunteers between 18 and 65 years of age was made through social media. The inclusion criteria for participation in this study included having a diagnosis of low back pain (LBP) made by a doctor or specialist and the experiencing of a reduction in mobility or increased difficulty in movement. The exclusion criteria included individuals presenting any disease or disability that may have hindered their movement, as well as those who were high-level athletes. Additionally, individuals engaging in dangerous activities during the study period were excluded, as well as individuals undergoing any specific drug treatment to alleviate pain. To be eligible for participation, volunteers must not have received physiotherapeutic treatment during the previous 6 months. All participants were required to sign an informed consent form and to attend treatment sessions in person. The final consent was signed on 12 March 2023. Following recruitment, patients underwent the MoCap movement test to evaluate flexion–extension, lateralization, and rotation movements. Among these patients, fifteen (7 men and 8 women) received traditional treatment, including massage, exercise, heat therapy, and cold therapy. The remaining fifteen (7 men and 8 women) were treated with the deep oscillation method to analyze their response to an additional treatment different from the conventional one. Moreover, it was important to know how the clinician evaluated the patient. First, a clinical review was performed, including collecting information about the type of work the patient performed, if the patient practiced any sport, if the patient had experienced any impactful events in the last few weeks or months, and if any type of chronic disease was present. Secondly, the clinician observed the entire posterior trunk, detecting anomalies in the whole spine, accompanied by a palpatory examination of the lumbar spine. Third, the treatments were applied. For the conventional treatment, the clinician applied a combination of different treatments that have yielded positive results. First, a heat treatment was applied for 10 min [
21], then a magneto machine was applied for another 20 min [
22]. Finally, a massage series was performed [
23], which was coupled with three William’s exercises (the first three exercise describe in William’s program) [
24] consisting of two series of 10 repetitions of each exercise for five minutes. These treatments were used in order to consider their effects in combination, producing a multi-factorial therapy program that could guarantee yielding results in both the short and long run of the experiment [
25].
A deep oscillation treatment was also performed as a novel treatment based on research findings on electrostatic fields used in chronic pain treatment [
26]. The clinicians asked the patient to lie down on the table and to remove their T-shirt in order to provide a visible lumbar zone for performance of the treatment. Then, heat was applied to the lumbar region for 10 min. Next, talcum powder was applied and deep oscillation treatment was immediately performed for 15 min. Finally, the patient was massaged on the treated area for 5 min. These massages were also coupled with the William’s exercises as described for the previous treatment. Patients had to perform three sessions per week, i.e., in total, to complete 12 treatment sessions.
To evaluate the patient’s physical improvements, the clinicians used the Short Form-36 Physical Functioning scale specific to low back pain pathologies [
27].
Patient-related information, such as age, BMI, diagnosis, pain level were not included in this document because these variables were not considered when conducting this study. However, information regarding the patients and the procedures performed on each patient is summarized in
Table 1. Further details on the status of the patients prior to the treatments can be found in the
Supplementary Materials where details of BMI, pain level, age, and a brief description of the situation of the patients is provided. A flowchart of the methodology for ROM classification is presented in
Figure 1.
2.2. Ethical Statement
The study was conducted in accordance with the Declaration of Helsinki and the protocol was approved by the Ethics Committee for Research on Human Beings of the Pontificia Universidad Católica del Ecuador (PUCE), Ecuador (N° EO-146-2022). Written informed consent was obtained from each participant.
2.3. Technology and Instrumentation
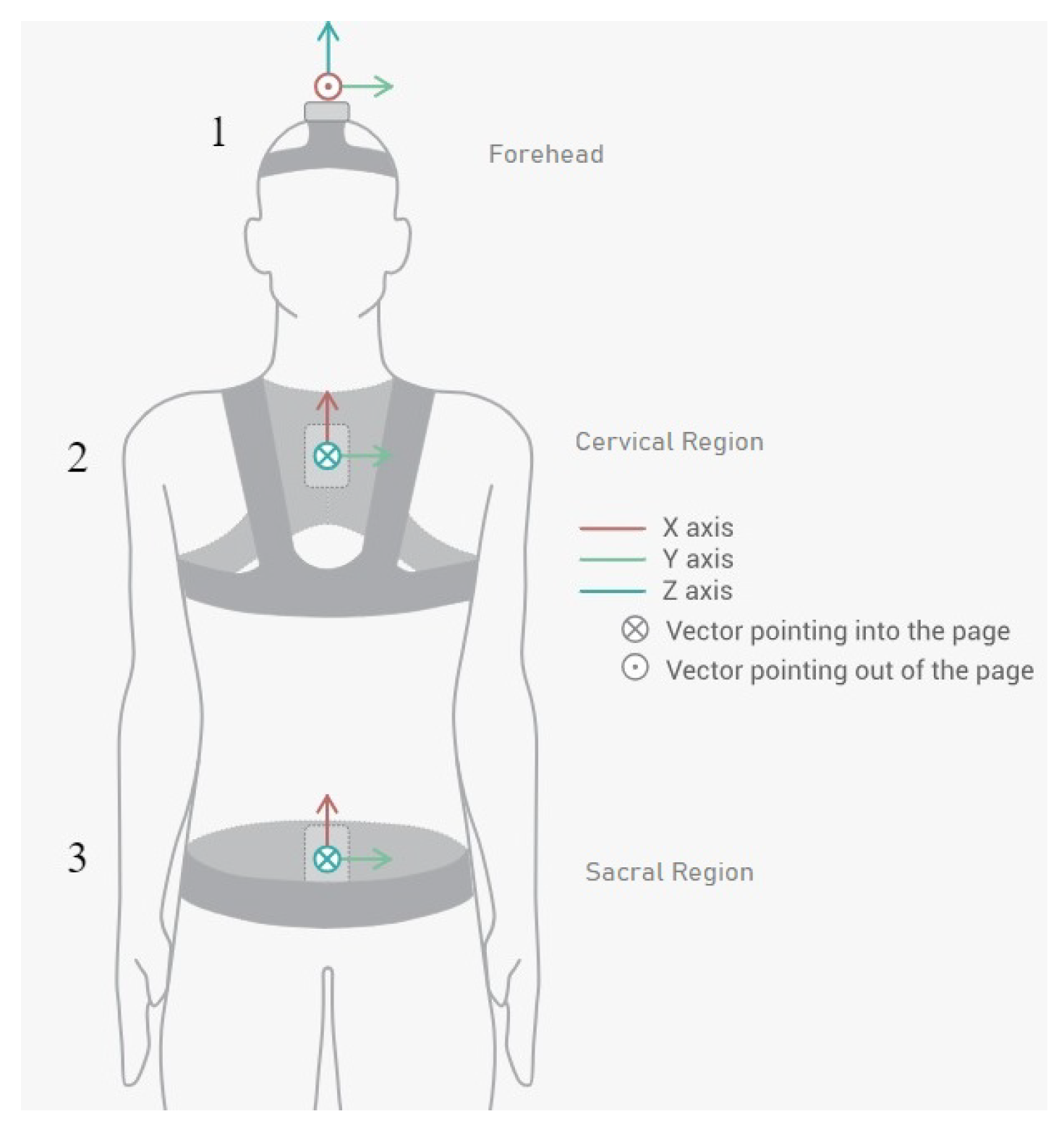
We employed the Move Human (MH) Sensors MoCap system which was developed by IDERGO (Investigación y Desarrollo en Ergonomía Research Group, V19-07.011, University of Zaragoza, Zaragoza, Spain) using NGIMU (x-io technologies, Bristol, UK). This system relies on inertial measurement units (IMUs) securely positioned on three key areas of the body: sensor 1 is collocated in the superior head region (forehead), sensor 2 is collocated in the cervical region (specifically at C7), and sensor 3 is collocated in the sacral region (at the iliac crest level) (see
Figure 2) for comprehensive analysis. This system provides accurate information on the rotations and displacements of each body segment at a frequency of 60 Hz.
The MH-Sensors system enables the visualization and real-time monitoring of movement on a digital representation of a human body, or avatar, which is adjusted to the subject’s body dimensions. In addition, the inertial sensor system houses three types of sensors: accelerometers, gyroscopes, and magnetometers. These signals are combined, enabling the clinician to obtain three rotation angles in the axes of space (as well as the angular velocities and accelerations).
2.4. Varirable
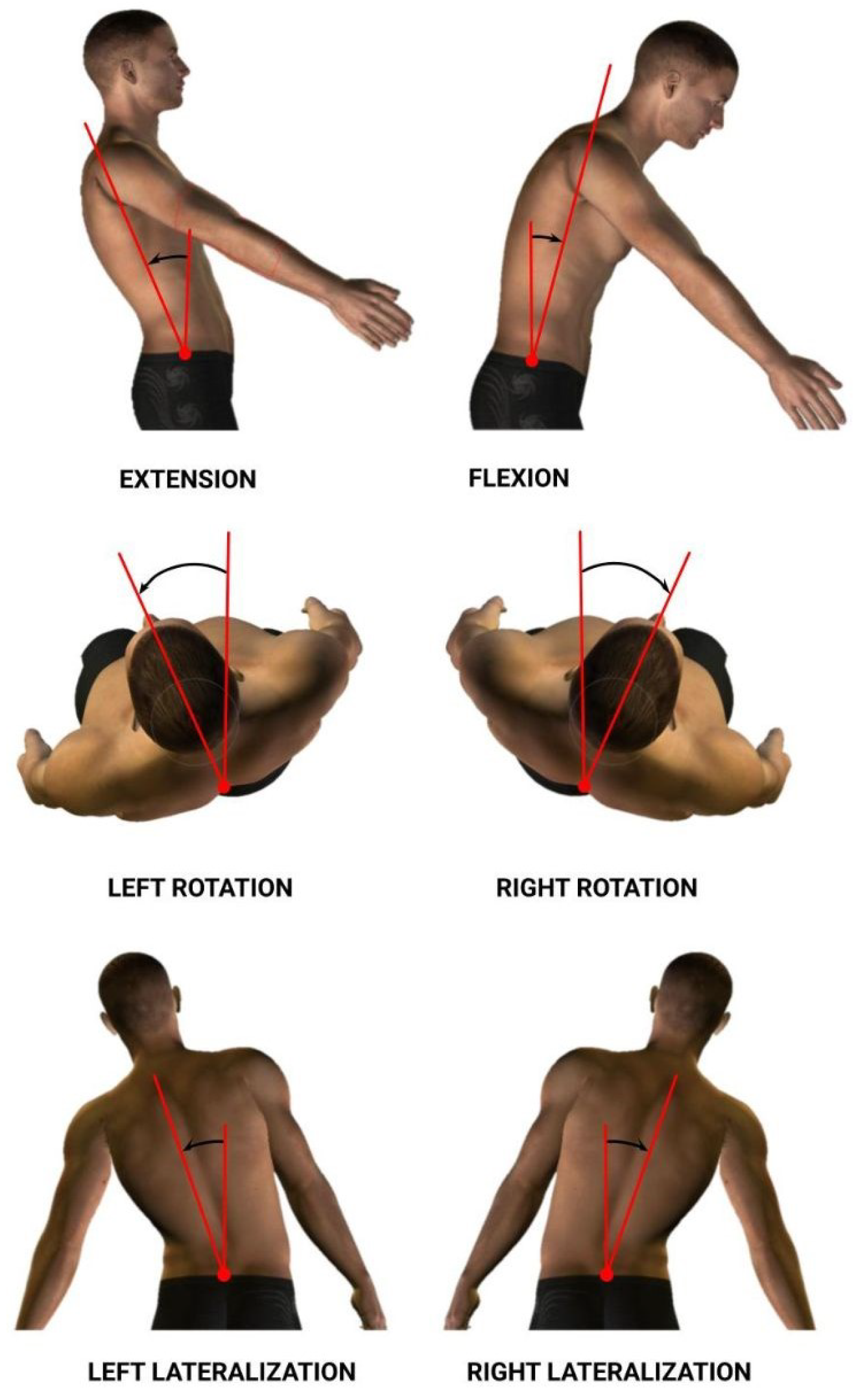
The dorsal–lumbar movements analyzed to obtain data were flexion–extension (Flex), right–left rotation (Rot), and right–left lateralization (Lat) (See
Figure 3). As a result, we acquired information relating to spatiotemporal and kinematic variables. Each variable was calculated for each dorsal–lumbar movement (Flex, Rot, and Lat). Information for the variables considered in the study is summarized in
Table 2.
2.5. Magnitude-Based Decision (MBD) to Monitor Individuals with LBP
To measure the effects of the treatment on patients, it is necessary to use the statistical approach, magnitude-based decision MBD, in order to compare the effect size with a predetermined threshold. When discussing individual monitoring, it is important to consider that each patient performed six complete cycles during each session (one session prior to the treatments and one session after the treatments; these two sessions were conducted for both types of treatment, traditional treatment and deep oscillation treatment), attempting to reach their maximum range in each exercise in order to obtain the necessary information to evaluate the respective variables needed for assessment. Thus, for individual monitoring of each variable, it was possible to compare two sets of measurements: one from the pre-treatment session (
n1 samples,
X1 mean, and
SD1 standard deviation) and another from the post-treatment session session (
n2,
X2 mean, and
SD2 standard deviation). For this purpose, we used the same discerning method as described in Marin et al. [
11], the magnitude-based decision method. This method provides the probability that a change (which is defined by the confidence interval of the difference, CIdiff) exceeds a specific threshold (
,
) [
19], in this case, the MDC [
29] (
1).
MDC values at 95% confidence were calculated using the following expression:
In this equation, SD stands for the weighted mean of the standard deviation between test and retest, ICC is the intraclass correlation coefficient, and SEM is the measurement standard error.
In this way, a change is only considered substantial if it overcomes the test’s inherent faults, so that it can be stated that the change observed is real and is not the product of a measurement error. This can be especially helpful to physicians when used in conjunction with clinical data.
By calculating the CIdiff, we can create a graph for each variable that depicts the threshold (
,
) and the t-distribution of the change between the pre- and post-series, like the one presented in
Figure 4. Analysis of where changes occur with respect to the threshold is made clearer using this depiction. To conduct this analysis statistically, we determined specific domains of probability denoted negative change (N), trivial change (T), and positive change (P). These domains are defined by the proportion of the t area that falls inside; as such, we have a “negative” region (
), a “trivial” region (
,
), and a “positive” region (
).
In this case, a change is regarded as null or insignificant if it does not surpass the threshold in any direction where the percentages of P and N are both less than 5% (N < 5% and P < 5%). A change is classified as uncertain if both P and N surpass 5% (P > 5% and N > 5%), because it occurs concurrently in both directions. With a predetermined likelihood of change, any further measure of CIdiff can be classified as either positive (increment) or negative (decrement). The probability of change is P when there is an increase in the change, and N when there is a decrease in the change. According to the classification of the likelihood of change, 5 to 25% is considered “unlikely”, 25 to 75% is “possible”, 75 to 95% is “likely”, 95 to 99% is “very likely”, and greater than 99% is considered “extremely likely”.
Apart from the application of the MDC, another important point to observe in the individual analysis is that most changes in the variables are neither necessarily beneficial nor harmful. Increasing or decreasing the magnitude of a particular variable may be beneficial to one patient but harmful to another because LBP affects patients differently. Therefore, the results must be interpreted individually for each patient.
4. Discussion
To assess the reproducibility in our test-retest results, we evaluated the ICC values, which exceeded 0.7. These results are satisfactory in comparison to those reported in a similar study [
30], where use was made of an optical motion capture system to analyze the same movements but in a seated position; in this study only moderate ICC values (0.6–0.7) for most of their variables were obtained. In another study by Megan O’Grady et al. [
31], use was similarly made of an IMU system to analyze lumbar movement (flexion–extension, lateral flexion left to right, and rotation). When calculating the reproducibility, these authors obtained values (0.95 < ICC < 1.00) for the kinematics they were evaluating. The values obtained in our study with respect to the same variables were very similar to those reported in Megan O’Grady’s study [
31] (ICC > 0.85). Both of these findings indicate the reliability of IMU systems and their potential to assess the kinematics of lumbar movement. Most of the kinetics variables also exhibited high reproducibility (ICC > 0.85), with the exception of the accelerations for the lateralization and rotation movement. When compared to other studies that also dealt with MDC, we note that our results for the ROM were comparable with those obtained in similar studies [
32,
33]. However, we were unable to find details of previous MDC studies focusing on the velocities of these movements, so we are not able to fully support our findings with respect to these variables.
The utility of the test is determined by the MDC value of the variables, with
Table 3,
Table 4 and
Table 5 (marked with a *) indicating the variables with the lowest MDC ranges and the greatest ICC in our study. Furthermore, based on the statistical application of the MDC technique in a sample of 30 patients, these are the variables most relevant for measuring change at the individual level and, hence, the efficacy of an intervention/treatment. The findings were compared to those of various studies of individuals with LBP, where the most reliable variables are those in which the biggest change was identified in relation to improvement [
34,
35,
36,
37,
38,
39]. As a result, the BackMov test could give clinicians reliable and easy to understand information about the change in a particular characteristic seen in a patient, enabling them to clearly see the improvement or impairment of a patient. The clinician, who can now be aware of these specific characteristics in the patient’s circumstances may find it easier to decide whether or not to continue with a treatment or whether to change it in favor of a treatment to target the specific change that they may have noticed.
For example, we draw attention to the graphs depicted in
Figure 5,
Figure 6,
Figure 7,
Figure 8,
Figure 9 and
Figure 10 with regard to the findings of this study. These graphs were created to graphically and intuitively display the changes observed in the set of variables, making it easier for the physician to recognize the factors that need further consideration and analysis. This information can be useful, as a significant number of guidelines primarily focus on assessing the disability that the LBP may be causing the patient [
40]. In relation to this, we saw that the improvement in ROM and velocities could be directly related to the abilities of individuals to perform physical activities. This is supported by the observation that for patients that exhibited a significant change in these variables when responding to the questionnaire conducted by the physicians (see
Supplementary Materials S5), their answers showed that most of them were better when performing activities that involved a high degree of movement from their point of view, such as going up the stairs or walking. Furthermore, as the velocities of the patients also seemed to have improved, this could be related to the therapies helping patients to overcome their fear of movement so that they were less hesitant to move, therefore decreasing the overall time it took them to perform an activity [
41,
42]. Overcoming the fear of movement would correlate with the improvement in these variables with overall improvement in performing daily activities. Furthermore, as movement increases this also helps to reduce muscle tension and stiffness that may have been caused as a result of the individuals trying to move as little as possible to avoid pain [
43,
44,
45]. The results of our MDC comparisons are in line with evaluation of progress in the patients conducted by the specialist physicians using the low-back-specific form of the SF-36 Physical Functioning scale. The results were that both groups showed real changes in the variables that can be associated with disability and thus may influence recovery of LBP patients. In this way, the graphs are intended to make it easier to identify a change in a variable related to disability, thus facilitating monitoring of treatment without the need to keep completing questionnaires to assess progress. Furthermore, if the clinician needs to pursue a more extensive and rigorous analysis, the tables (
Table 6,
Table 7,
Table 8,
Table 9,
Table 10 and
Table 11) contain more detailed information on the variables and the changes in the patients kinematics.
Personalized medicine has become an important goal for health professionals [
46]. The response to therapy for conditions like LBP problems can be objectively described through individual patient assessment, so these kinds of tools that reduce the time to assess progression can be good for the future of therapy. Although there seems to be benefit in using the BackMov test for the purposes described, there are certain issues that need to be addressed as they may cause the results to not be reliable if they are not taken into account. A clear issue is the fact that IMUs suffer from integration drift, which involves small errors appearing during the measurement of acceleration and angular velocity that can be progressively combined into larger errors in velocity and angle, which are compounded into still greater errors in position [
47]. Another issue that may arise from this test that must be taken into consideration is the effect of noise associated with other variables, including pathology, treatment used between pre- and post-testing, illness progression, and even private personal events [
48,
49,
50,
51,
52]. Despite the promising results and the potential utility of the BackMov test in assessing lumbar movement recovery in LBP patients post-therapy, it is crucial to acknowledge certain limitations that may impact the interpretation of our findings. One notable limitation is the exclusion criteria employed in participant selection. Excluding individuals with pre-existing diseases or disabilities that might hinder their movement was essential for maintaining homogeneity in the study cohort. However, it is important to recognize that the applicability of the BackMov test to a broader patient population, including those with comorbidities or disabilities, remains to be explored. Another limitation stems from the exclusion of high-level athletes from the study cohort. While this decision aimed to control for the potential influence of exceptional physical fitness on lumbar movement, it has inadvertently limited the generalizability of our findings to this specific subgroup. The BackMov test’s effectiveness in assessing movement recovery in athletes with LBP warrants further investigation to ascertain its relevance and applicability across diverse patient profiles.
Additionally, the exclusion of individuals engaged in dangerous activities during the study period raises questions about the test’s external validity in real-world scenarios where patients may need to resume such activities post-therapy. The BackMov test’s capacity to capture improvements in lumbar movement relevant to occupational or recreational activities involving increased risk remains an avenue for future research. Moreover, the exclusion of individuals undergoing drug-specific treatments to alleviate pain introduces another layer of complexity. Many LBP patients often rely on pharmacological interventions for pain management. The impact of these treatments on lumbar movement and the BackMov test’s sensitivity to changes in patients undergoing drug-specific interventions were not explored in this study. Future investigations should consider incorporating these variables to enhance the test’s applicability in a broader clinical context.
As an important note, while the BackMov test appears to possess great potential to detect when a patient experiences a relevant change in a particular variable (high likelihood of change), the physician should still not only rely on these results for determining whether or not this change is important for treatment. This is significant because, despite the fact that this kind of metric is meant to offer unbiased data in support of a diagnosis, the MDC itself is not a definitive diagnosis and should not be used as the only tool to determine a clinical decision as it is based on merely an association of certain variables with the disability produced by the LBP [
53,
54,
55]. Some of these associations are still in need of further evaluation to be considered directly proportional to the effects of LBP. Furthermore, these values do not account for the psychological aspect that must be addressed when dealing with these kinds of problems [
56,
57]. Regarding the study’s implications for research and clinical practice, we believe that the use of the BackMov test as a ’logical’ guideline can be the foundation for future patient studies for the evaluation of treatments. However, it is necessary to further develop the rules that allow for more effective qualification of the change detected in the variables. This would further support use of the method in the evaluation of treatments or the monitoring of a patient’s overall recovery based on the premise of disability recovery from improved kinematics of lumbar movements.
5. Future Work
To enhance the understanding and potential of this methodology, a more comprehensive and rigorous approach is proposed. In the newly suggested methodology, a control group should be included to observe the progress of LBP patients in the absence of any treatment. Additionally, other therapeutic treatments for the pathology should be incorporated. In future studies, greater attention must be given to the psychological and psychosocial aspects of the disease. Furthermore, the utilization of alternative statistical tools, such as the minimal important difference (MID), should be considered to complement the minimum detectable change (MDC). Determining MID thresholds, alongside MDC, would offer a more valuable means to assess therapies, provide evidence for diagnoses, and facilitate the monitoring of patient recoveries. Lastly, unless more evidence emerges regarding the relationship between disability and kinematic variables or the association of fear of movement with kinematics, a dedicated study focusing on establishing these connections should be planned to support the use of this methodology.

 ,
, 











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}