
Validation of the Activ8 Activity Monitor for Monitoring Postures, Motions, Transfers, and Steps of Hospitalized Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Optimization Process
2.2. Study Population
2.3. Measurement Protocol
2.4. Activity Monitor
2.5. Video Recording
2.6. Data Analysis
3. Results
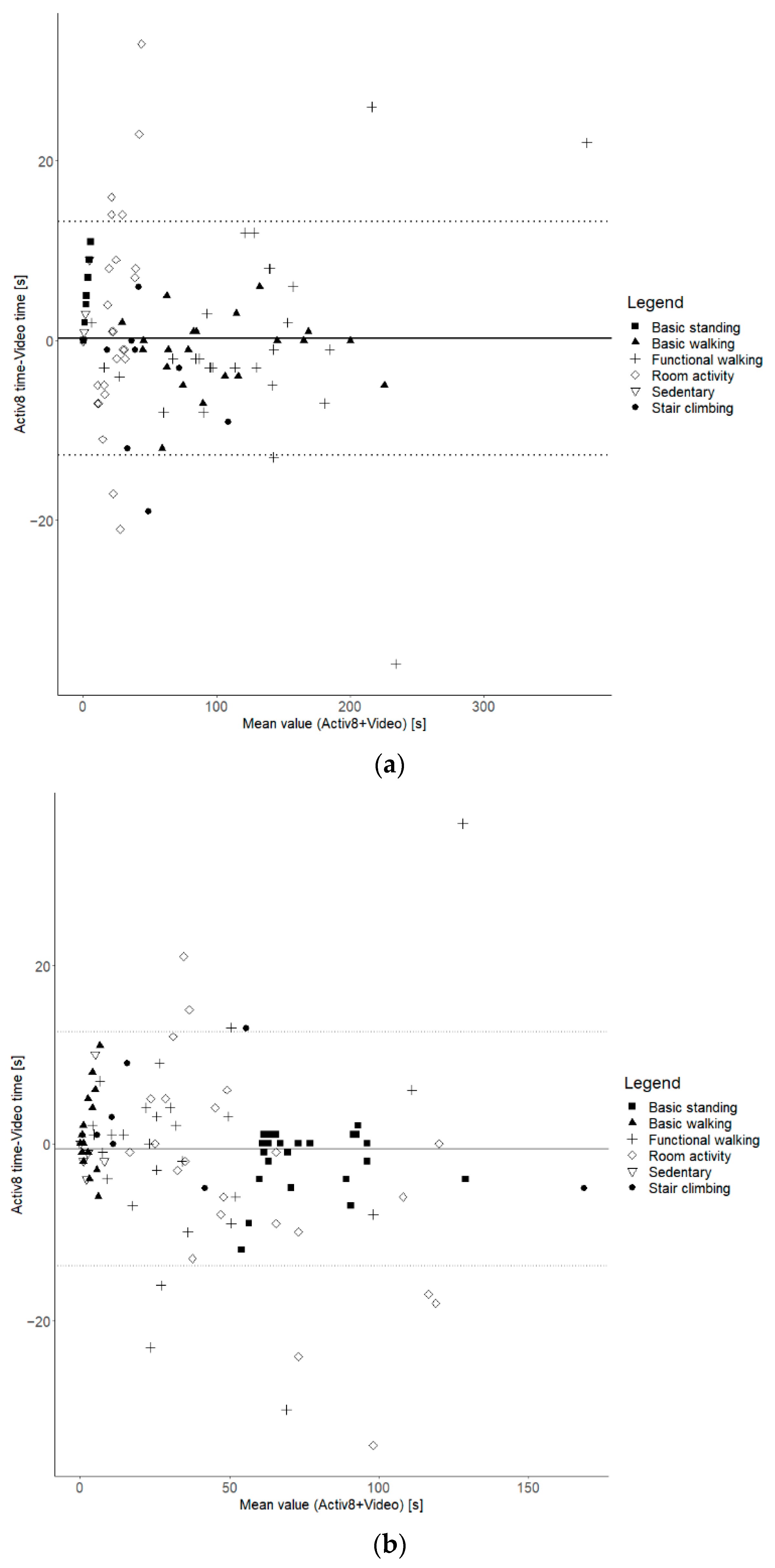
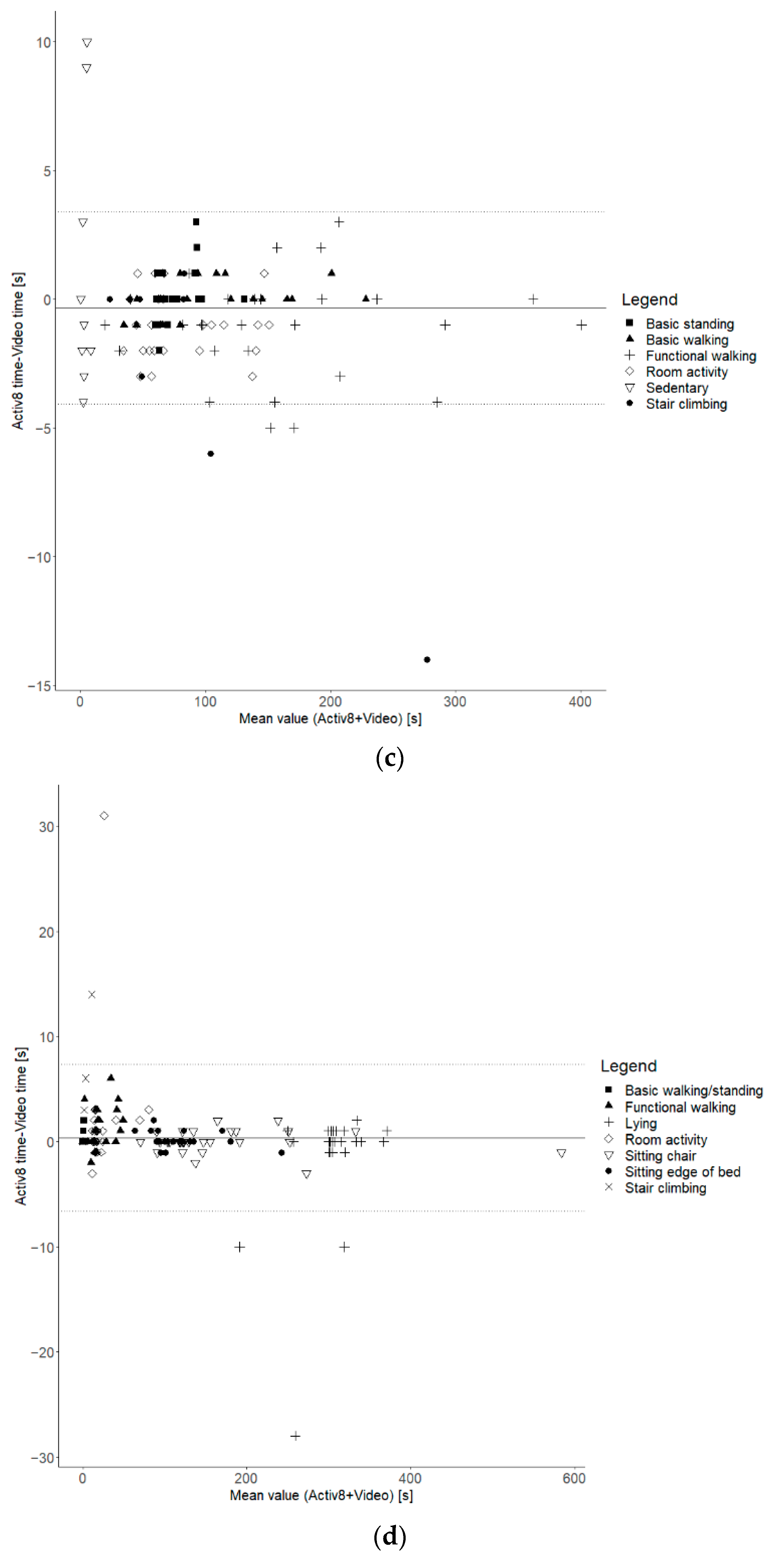
3.1. Time Spent Walking, Standing, Upright, and Sedentary
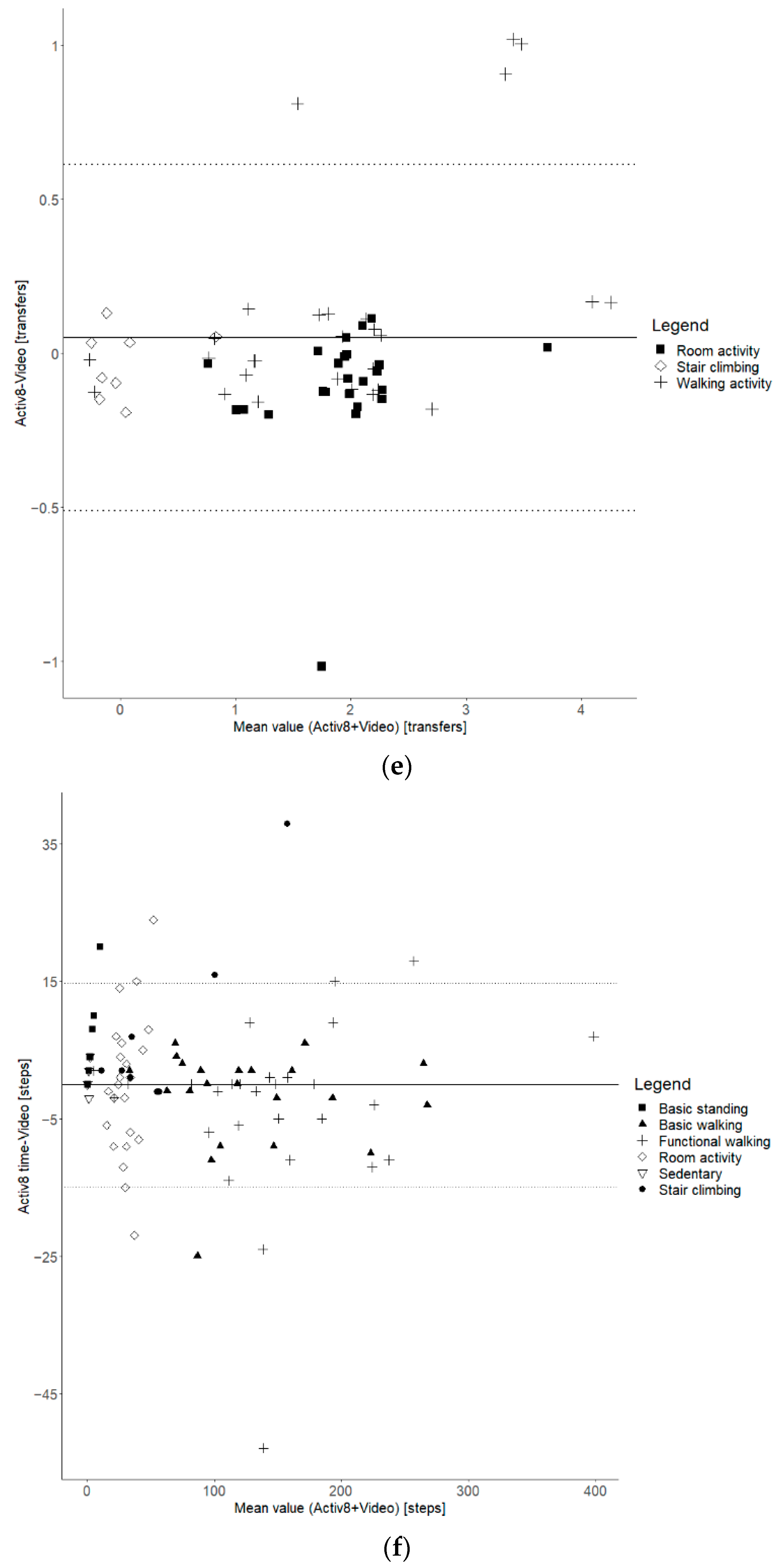
3.2. Transfer and Step Count
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kirk, A.G.; Behm, K.J.; Kimmel, L.A.; Ekegren, C.L. Levels of Physical Activity and Sedentary Behavior During and After Hospitalization: A Systematic Review. Arch. Phys. Med. Rehabil. 2021, 102, 1368–1378. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.J.; Redden, D.T.; Flood, K.L.; Allman, R.M. The underrecognized epidemic of low mobility during hospitalization of older adults. J. Am. Geriatr. Soc. 2009, 57, 1660–1665. [Google Scholar] [CrossRef] [PubMed]
- Tasheva, P.; Kraege, V.; Vollenweider, P.; Roulet, G.; Méan, M.; Marques-Vidal, P. Accelerometry assessed physical activity of older adults hospitalized with acute medical illness—An observational study. BMC Geriatr. 2020, 20, 382. [Google Scholar] [CrossRef] [PubMed]
- Covinsky, K.E.; Palmer, R.M.; Fortinsky, R.H.; Counsell, S.R.; Stewart, A.L.; Kresevic, D.; Burant, C.J.; Landefeld, C.S. Loss of independence in activities of daily living in older adults hospitalized with medical illnesses: Increased vulnerability with age. J. Am. Geriatr. Soc. 2003, 51, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Hartley, P.; Romero-Ortuno, R.; Wellwood, I.; Deaton, C. Changes in muscle strength and physical function in older patients during and after hospitalisation: A prospective repeated-measures cohort study. Age Ageing 2020, 50, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef]
- Cortes, O.L.; Delgado, S.; Esparza, M. Systematic review and meta-analysis of experimental studies: In-hospital mobilization for patients admitted for medical treatment. J. Adv. Nurs. 2019, 75, 1823–1837. [Google Scholar] [CrossRef]
- Kalisch, B.J.; Lee, S.; Dabney, B.W. Outcomes of inpatient mobilization: A literature review. J. Clin. Nurs. 2014, 23, 1486–1501. [Google Scholar] [CrossRef]
- de Foubert, M.; Cummins, H.; McCullagh, R.; Brueton, V.; Naughton, C. Systematic review of interventions targeting fundamental care to reduce hospital-associated decline in older patients. J. Adv. Nurs. 2021, 77, 4661–4678. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe; The European Observatory on Health Systems and Policies; Rafferty, A.M.; Busse, R.; Zander-Jentsch, B.; Sermeus, W.; Bruyneel, L. Strengthening Health Systems through Nursing: Evidence from 14 European Countries; World Health Organization. Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- Geelen, S.J.G.; van Dijk-Huisman, H.C.; de Bie, R.A.; Veenhof, C.; Engelbert, R.; van der Schaaf, M.; Lenssen, A.F. Barriers and enablers to physical activity in patients during hospital stay: A scoping review. Syst. Rev. 2021, 10, 293. [Google Scholar] [CrossRef]
- Koenders, N.; van Oorsouw, R.; Seeger, J.P.H.; Nijhuis-van der Sanden, M.W.G.; van de Glind, I.; Hoogeboom, T.J. “I’m not going to walk, just for the sake of walking…”: A qualitative, phenomenological study on physical activity during hospital stay. Disabil. Rehabil. 2018, 42, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Hoyer, E.H.; Brotman, D.J.; Chan, K.S.; Needham, D.M. Barriers to early mobility of hospitalized general medicine patients: Survey development and results. Am. J. Phys. Med. Rehabil. 2015, 94, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Brickwood, K.-J.; Watson, G.; O’Brien, J.; Williams, A.D. Consumer-based wearable activity trackers increase physical activity participation: Systematic review and meta-analysis. JMIR mHealth uHealth 2019, 7, e11819. [Google Scholar] [CrossRef] [PubMed]
- Laranjo, L.; Ding, D.; Heleno, B.; Kocaballi, B.; Quiroz, J.C.; Tong, H.L.; Chahwan, B.; Neves, A.L.; Gabarron, E.; Dao, K.P. Do smartphone applications and activity trackers increase physical activity in adults? Systematic review, meta-analysis and metaregression. Br. J. Sports Med. 2021, 55, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Lyons, E.J.; Lewis, Z.H.; Mayrsohn, B.G.; Rowland, J.L. Behavior change techniques implemented in electronic lifestyle activity monitors: A systematic content analysis. J. Med. Internet Res. 2014, 16, e192. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; McNarry, M.A.; Mackintosh, K.A. Feasibility and effectiveness of using wearable activity trackers in youth: A systematic review. JMIR mHealth uHealth 2016, 4, e6540. [Google Scholar] [CrossRef] [PubMed]
- Vaes, A.W.; Cheung, A.; Atakhorrami, M.; Groenen, M.T.J.; Amft, O.; Franssen, F.M.E.; Wouters, E.F.M.; Spruit, M.A. Effect of ‘activity monitor-based’counseling on physical activity and health-related outcomes in patients with chronic diseases: A systematic review and meta-analysis. Ann. Med. 2013, 45, 397–412. [Google Scholar] [CrossRef] [PubMed]
- Garzon-Serrano, J.; Ryan, C.; Waak, K.; Hirschberg, R.; Tully, S.; Bittner, E.A.; Chipman, D.W.; Schmidt, U.; Kasotakis, G.; Benjamin, J.; et al. Early mobilization in critically ill patients: Patients’ mobilization level depends on health care provider’s profession. Pm R. 2011, 3, 307–313. [Google Scholar] [CrossRef]
- Graham, J.E.; Fisher, S.R.; Bergés, I.-M.; Kuo, Y.-F.; Ostir, G.V. Walking speed threshold for classifying walking independence in hospitalized older adults. Phys. Ther. 2010, 90, 1591–1597. [Google Scholar] [CrossRef]
- Villumsen, M.; Jorgensen, M.G.; Andreasen, J.; Rathleff, M.S.; Mølgaard, C.M. Very Low Levels of Physical Activity in Older Patients During Hospitalization at an Acute Geriatric Ward: A Prospective Cohort Study. J. Aging Phys. Act. 2015, 23, 542–549. [Google Scholar] [CrossRef]
- McCullagh, R.; Brady, N.M.; Dillon, C.; Horgan, N.F. A review of the accuracy and utility of motion sensors to measure physical activity of frail, older hospitalized patients. J. Aging Phys. Act. 2016, 24, 465–475. [Google Scholar] [CrossRef]
- Pedersen, B.S.; Kristensen, M.T.; Josefsen, C.O.; Lykkegaard, K.L.; Jønsson, L.R.; Pedersen, M.M. Validation of Two Activity Monitors in Slow and Fast Walking Hospitalized Patients. Rehabil. Res. Pr. 2022, 2022, 9230081. [Google Scholar] [CrossRef] [PubMed]
- Valkenet, K.; Bor, P.; van Delft, L.; Veenhof, C. Measuring physical activity levels in hospitalized patients: A comparison between behavioural mapping and data from an accelerometer. Clin. Rehabil. 2019, 33, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- van Dijk-Huisman, H.C.; Bijnens, W.; Senden, R.; Essers, J.M.N.; Meijer, K.; Aarts, J.; Lenssen, A.F. Optimization and validation of a classification algorithm for assessment of physical activity in hospitalized patients. Sensors 2021, 21, 1652. [Google Scholar] [CrossRef] [PubMed]
- Claridge, E.A.; van den Berg-Emons, R.J.G.; Horemans, H.L.D.; van der Slot, W.; van der Stam, N.; Tang, A.; Timmons, B.W.; Gorter, J.W.; Bussmann, J.B.J. Detection of body postures and movements in ambulatory adults with cerebral palsy: A novel and valid measure of physical behaviour. J. Neuroeng. Rehabil. 2019, 16, 125. [Google Scholar] [CrossRef] [PubMed]
- Fanchamps, M.H.J.; Horemans, H.L.D.; Ribbers, G.M.; Stam, H.J.; Bussmann, J.B.J. The accuracy of the detection of body postures and movements using a physical activity monitor in people after a stroke. Sensors 2018, 18, 2167. [Google Scholar] [CrossRef] [PubMed]
- van Rooij, W.M.J.; van den Berg-Emons, H.J.G.; Horemans, H.L.D.; Fanchamps, M.H.J.; de Laat, F.A.; Bussmann, J.B.J. Validation of a Clinically Feasible Activity Monitor Which Measures Body Postures and Movements in Adults With Lower-Limb Amputation Who Wear a Prosthesis. J. Meas. Phys. Behav. 2020, 3, 135–146. [Google Scholar] [CrossRef]
- Keadle, S.K.; Lyden, K.A.; Strath, S.J.; Staudenmayer, J.W.; Freedson, P.S. A Framework to Evaluate Devices That Assess Physical Behavior. Exerc. Sport Sci. Rev. 2019, 47, 206–214. [Google Scholar] [CrossRef]
- Lindemann, U.; Zijlstra, W.; Aminian, K.; Chastin, S.F.; de Bruin, E.D.; Helbostad, J.L.; Bussmann, J.B. Recommendations for standardizing validation procedures assessing physical activity of older persons by monitoring body postures and movements. Sensors 2014, 14, 1267–1277. [Google Scholar] [CrossRef]
- Taraldsen, K.; Askim, T.; Sletvold, O.; Einarsen, E.K.; Grüner Bjåstad, K.; Indredavik, B.; Helbostad, J.L. Evaluation of a Body-Worn Sensor System to Measure Physical Activity in Older People With Impaired Function. Phys. Ther. 2011, 91, 277–285. [Google Scholar] [CrossRef]
- Baldwin, C.E.; Johnston, K.N.; Rowlands, A.V.; Williams, M.T. Physical activity of ICU survivors during acute admission: Agreement of the activPAL with observation. Physiother. Can. 2018, 70, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Kirk, A.G.; Kimmel, L.A.; Behm, K.J.; Peiris, C.L.; Ekegren, C.L. Validity of the ActivPAL and ActiGraph for measuring sitting time and steps in hospitalised orthopaedic patients with altered weight bearing. Disabil. Rehabil. 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Valkenet, K.; Veenhof, C. Validity of three accelerometers to investigate lying, sitting, standing and walking. PLoS ONE 2019, 14, e0217545. [Google Scholar] [CrossRef] [PubMed]
- Horemans, H.; Kooijmans, H.; van den Berg-Emons, R.; Bussmann, H. The Activ8 activity monitor: Validation of posture and movement classification. J. Rehabil. Assist. Technol. Eng. 2020, 7, 2055668319890535. [Google Scholar] [CrossRef]
- Anderson, J.L.; Green, A.J.; Yoward, L.S.; Hall, H.K. Validity and reliability of accelerometry in identification of lying, sitting, standing or purposeful activity in adult hospital inpatients recovering from acute or critical illness: A systematic review. Clin. Rehabil. 2018, 32, 233–242. [Google Scholar] [CrossRef]
- Wilkinson, M.D.; Dumontier, M.; Aalbersberg, I.J.; Appleton, G.; Axton, M.; Baak, A.; Blomberg, N.; Boiten, J.-W.; da Silva Santos, L.B.; Bourne, P.E. The FAIR Guiding Principles for scientific data management and stewardship. Sci. Data 2016, 3, 160018. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Video | Lying | Sitting | Sitting with movement | Sit-to-stand transfer | Standing | Standing with movement | Shuffling | Walking | Stair climbing | Cycling |
| Activ8 | Sedentary | Standing | Walking | Cycling |
| Sample Size | 31 |
| Age (m, sd) | 54.0, 17.0 |
| Gender (m/f) | 21/10 |
| Medical Department HPB/Lung | 18/13 |
| Surgical/Medical | 18/13 |
| Walking aid (Walker/IV pole/none) | 10/12/9 |
| Days since admission (m, sd) | 23.0, 37.3 |
| Walking speed on 3 MWT (m, sd) [km/h] | 2.10, 0.82 |
| Protocol | Activity | n |
|---|---|---|
| Basic | Walking | 23 |
| Standing | 27 | |
| Sitting on a chair | 30 | |
| Sitting on the edge of the bed | 25 | |
| Lying | 28 | |
| Functional | Hallway activities | 26 |
| (Bath)room activities | 24 | |
| Stair climbing | 8 |
| Type of Protocol | Type of Activity | Total Video | Total Activ8 | Absolute Difference | Relative Difference (%) | |
|---|---|---|---|---|---|---|
| Walking time 1 [s] | Total | 6694 | 6741 | 47 | 0.7 | |
| Basic | Walking | 2205 | 2181 | −24 | −1.1 | |
| Functional | Total | 4489 | 4497 | 8 | 0.2 | |
| Walking | 3518 | 3512 | −6 | −0.2 | ||
| Room | 557 | 610 | 53 | 9.5 | ||
| Stair climbing | 414 | 375 | −39 | −9.4 | ||
| Standing time 1 [s] | Total | 4806 | 4693 | −113 | −2.4 | |
| Basic | Standing | 2050 | 2005 | −45 | −2.2 * | |
| Functional | Total | 2695 | 2608 | −87 | −3.2 | |
| Walking | 1004 | 979 | −25 | −2.5 | ||
| Room | 1391 | 1323 | −68 | −4.9 | ||
| Stair climbing | 300 | 317 | 17 | 5.7 | ||
| Upright time 1 [s] | Total | 11,500 | 11,434 | −66 | −0.6 ** | |
| Basic | Walking + standing | 4289 | 4295 | 6 | 0.1 | |
| Functional | Total | 7184 | 7105 | −79 | −1.1 | |
| Walking | 4522 | 4491 | −31 | −0.7 # | ||
| Room | 1948 | 1922 | −22 | −3.1 | ||
| Stair climbing | 714 | 692 | −22 | −3.1 | ||
| Sedentary time 1 [s] | Total | 17,478 | 17,544 | 66 | 0.4 ** | |
| Basic | Total | 16,428 | 16,391 | −37 | −0.2 | |
| Sitting on chair | 5027 | 5029 | 2 | 0.0 | ||
| Sitting on bed | 2865 | 2870 | 5 | 0.2 | ||
| Lying | 8492 | 8536 | 44 | 0.5 | ||
| Functional | Total | 1047 | 1147 | 100 | 9.6 ** | |
| Walking | 530 | 561 | 31 | 5.8 ** | ||
| Room | 610 | 559 | −51 | −8.4 * | ||
| Stair climbing | 4 | 27 | 23 | NA | ||
| Transfers [nr] | Functional | Total | 98 | 101 | 3 | 3.1 |
| Walking | 51 | 55 | 4 | 7.8 # | ||
| Room | 46 | 45 | −1 | −2.2 | ||
| Stair climbing | 1 | 1 | 0 | 0.0 | ||
| Steps [nr] | Total | 8228 | 8214 | −14 | −0.2 | |
| Basic | Walking | 2823 | 2782 | −41 | −1.5 | |
| Functional | Total | 5403 | 5360 | −43 | −0.8 | |
| Walking | 4144 | 4237 | 93 | 2.2 | ||
| Room | 724 | 710 | −14 | −1.9 | ||
| Stair climbing | 442 | 456 | 14 | 3.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becker, M.L.; Hurkmans, H.L.P.; Verhaar, J.A.N.; Bussmann, J.B.J. Validation of the Activ8 Activity Monitor for Monitoring Postures, Motions, Transfers, and Steps of Hospitalized Patients. Sensors 2024, 24, 180. https://doi.org/10.3390/s24010180
Becker ML, Hurkmans HLP, Verhaar JAN, Bussmann JBJ. Validation of the Activ8 Activity Monitor for Monitoring Postures, Motions, Transfers, and Steps of Hospitalized Patients. Sensors. 2024; 24(1):180. https://doi.org/10.3390/s24010180
Chicago/Turabian StyleBecker, Marlissa L., Henri L. P. Hurkmans, Jan A. N. Verhaar, and Johannes B. J. Bussmann. 2024. "Validation of the Activ8 Activity Monitor for Monitoring Postures, Motions, Transfers, and Steps of Hospitalized Patients" Sensors 24, no. 1: 180. https://doi.org/10.3390/s24010180
APA StyleBecker, M. L., Hurkmans, H. L. P., Verhaar, J. A. N., & Bussmann, J. B. J. (2024). Validation of the Activ8 Activity Monitor for Monitoring Postures, Motions, Transfers, and Steps of Hospitalized Patients. Sensors, 24(1), 180. https://doi.org/10.3390/s24010180