




A PPG-Based Calibration-Free Cuffless Blood Pressure Estimation Method Using Cardiovascular Dynamics


Abstract
1. Introduction
2. Materials and Methods
2.1. Bio-Signal Datasets
- The original data are divided into fixed size signal blocks. Each block is processed through a simple averaging filter to smoothen the signal;
- Any block with irregular blood pressure value or heart rate is removed;
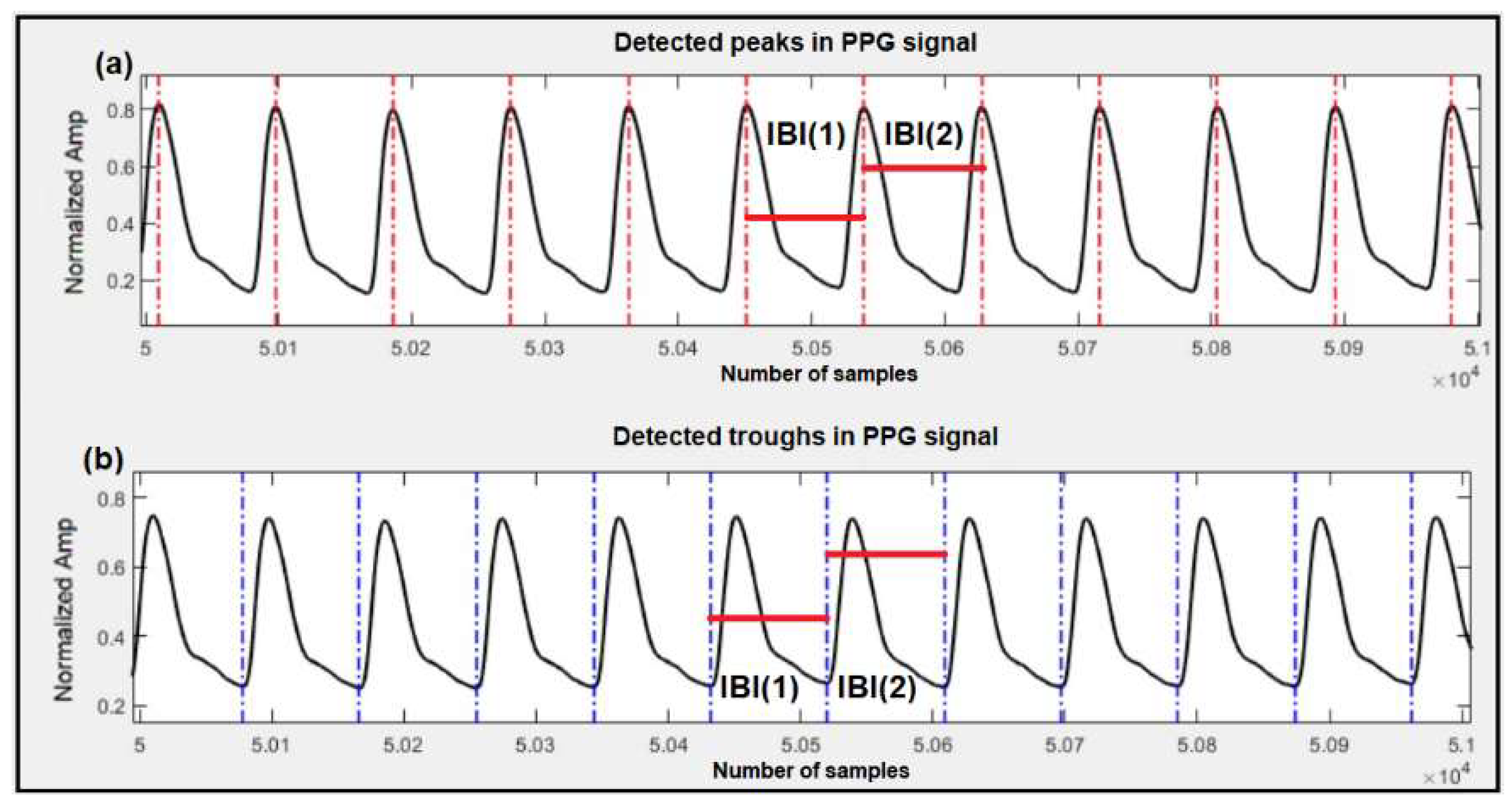
- Autocorrelation is calculated for PPG signal to indicate the degree of similarity between successive pulses in a block;
- Any block with high alteration between successive pulses, based on the calculated autocorrelation in the previous step, is removed [28].
2.2. Morphology-Based Estimation
2.2.1. Feedforward Artificial Neural Network Model
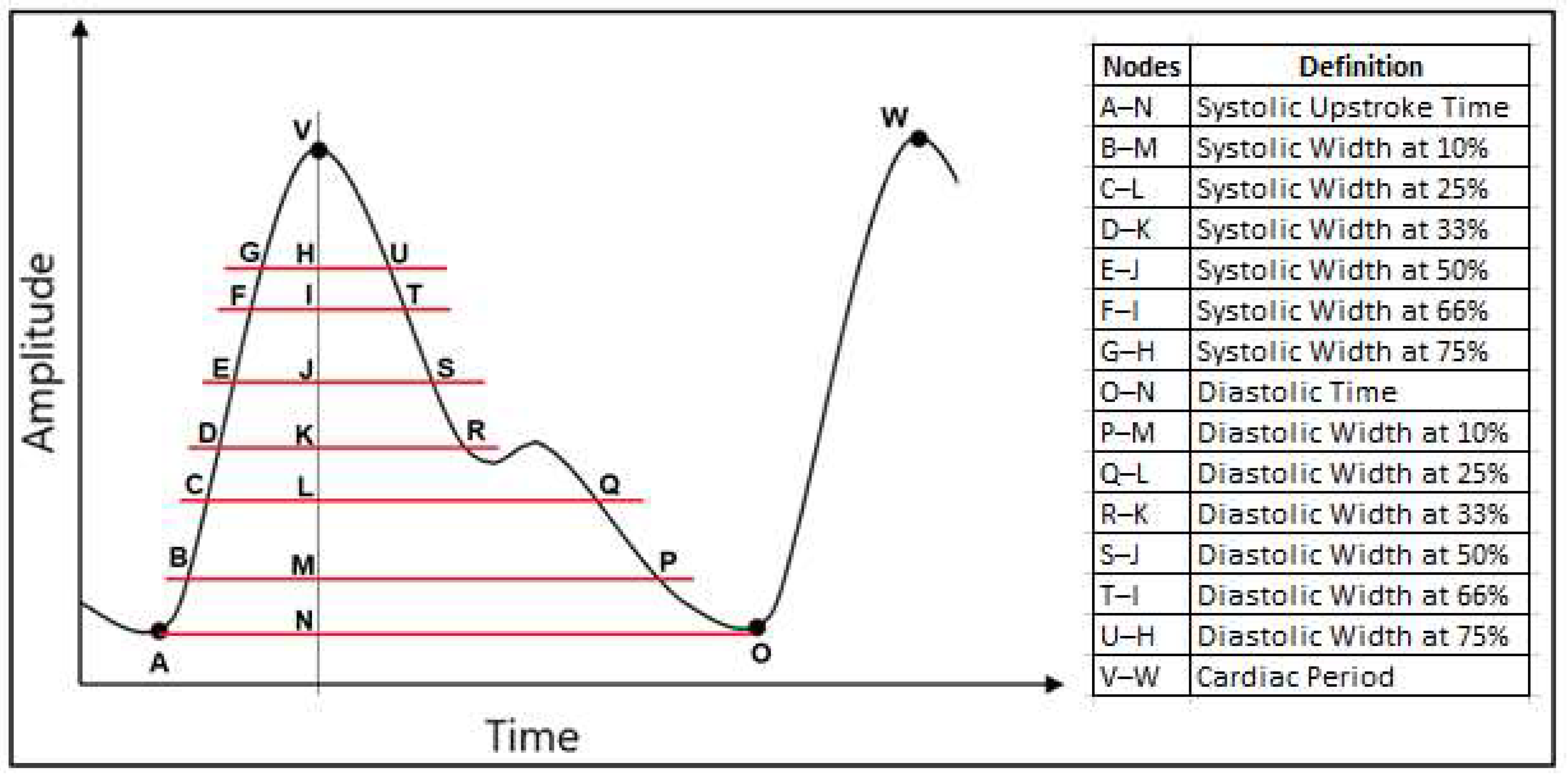
- Cardiac period;
- Systolic upstroke time;
- Diastolic time;
- Diastolic width at 10%, 25%, 33%, 50%, 66% and 75% of the pulse height;
- Sum of systolic width and diastolic width at 10%, 25%, 33%, 50%, 66% and 75% of the pulse height;
- Ratio of diastolic width to systolic width at 10%, 25%, 33%, 50%, 66% and 75% of the pulse height.
2.2.2. Deep Learning Model
- Cardiac period;
- Diastolic time;
- Diastolic width at 25% and 75% of the pulse height;
- Sum of systolic width and diastolic width at 33% and 75% of the pulse height;
- Ratio of diastolic width to systolic width at 10% of the pulse height.
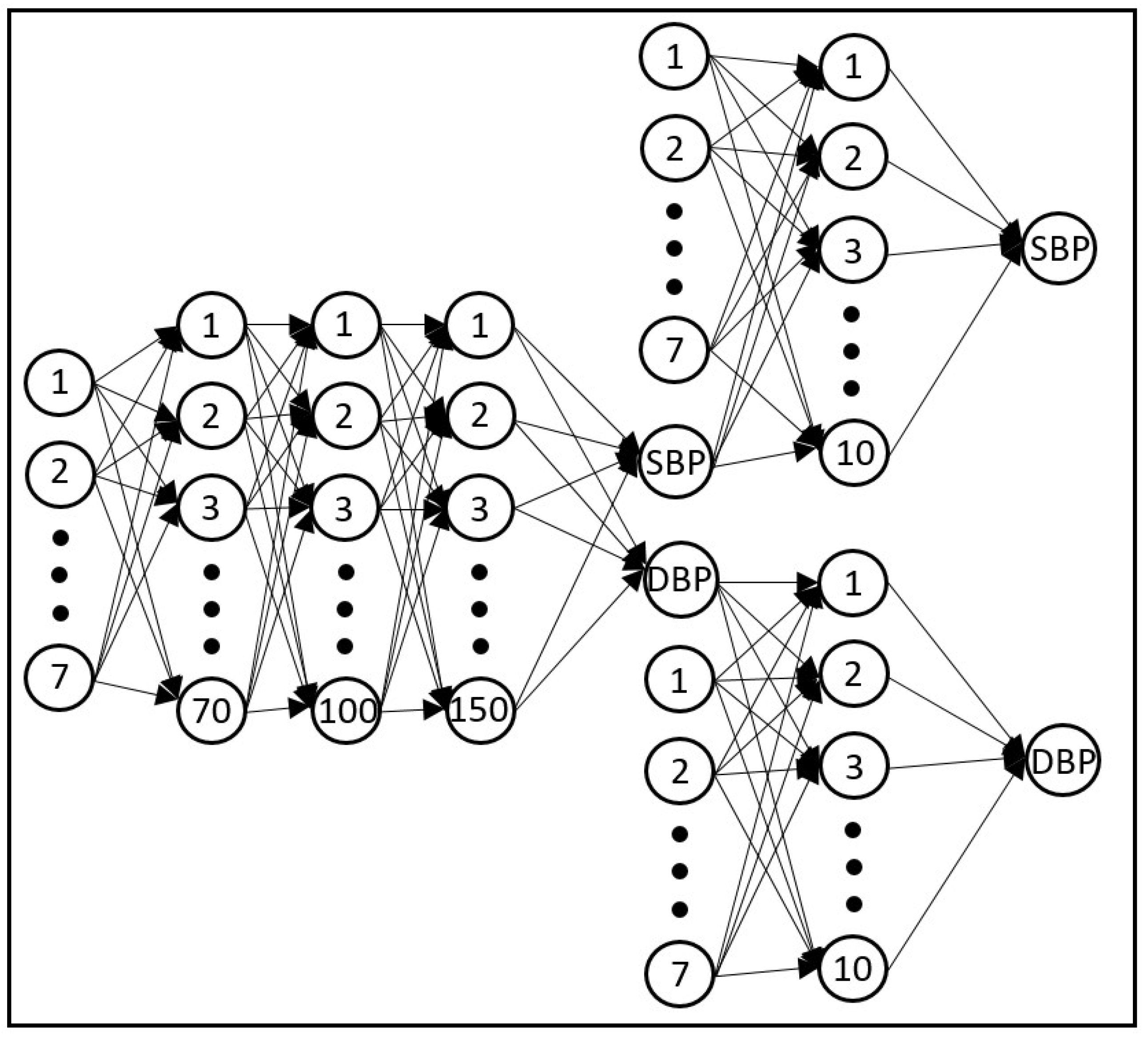
- Feedforward deep neural network: This model is similar to the one used in Section 2.2.1, which consisted of non-recurrent feedforward connections between the neurons, and it was constructed with three hidden layers containing 70, 100 and 150 neurons for Layers 1, 2 and 3 respectively [10];
- LSTM: Long short-term memory uses feedback connections to process sequential time domain data. It was originally developed to overcome the vanishing gradient problem during the training of the recurrent neural network due to long term prediction [10]. The LSTM used in this work was constructed with two hidden layers of 64 and 512 neurons;
- GRU: The gated recurrent unit is similar to the LSTM but since it uses fewer parameters, it is somewhat less computationally expensive. It has also shown better performance on certain smaller datasets compared to LSTM [10]. The network used here was constructed with three hidden layers of 128, 256 and 512 neurons in consecutive layers.
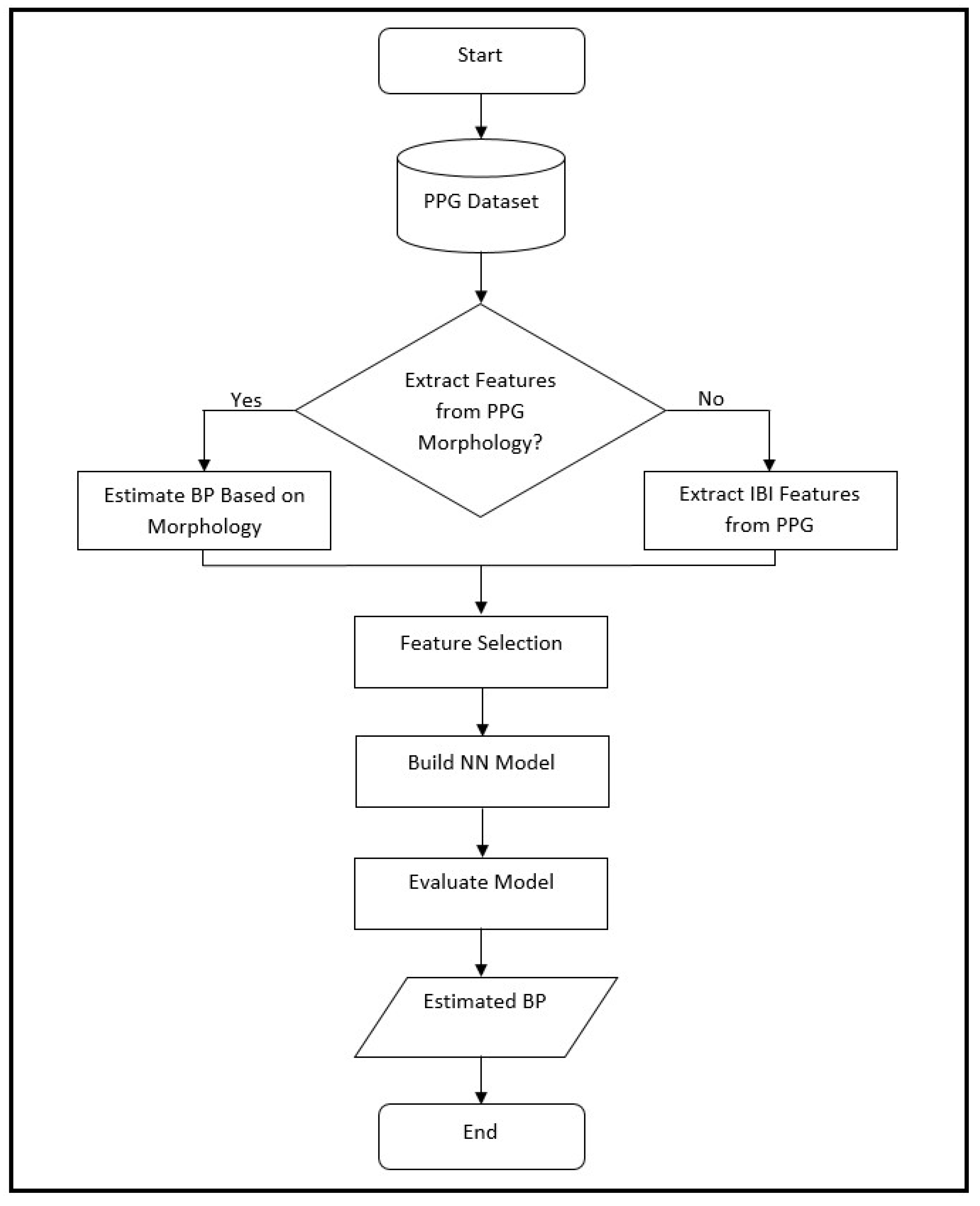
2.3. Blood Pressure Estimation Model
3. Results
3.1. Estimation of BP with 30 Patients from the University of Queensland Dataset
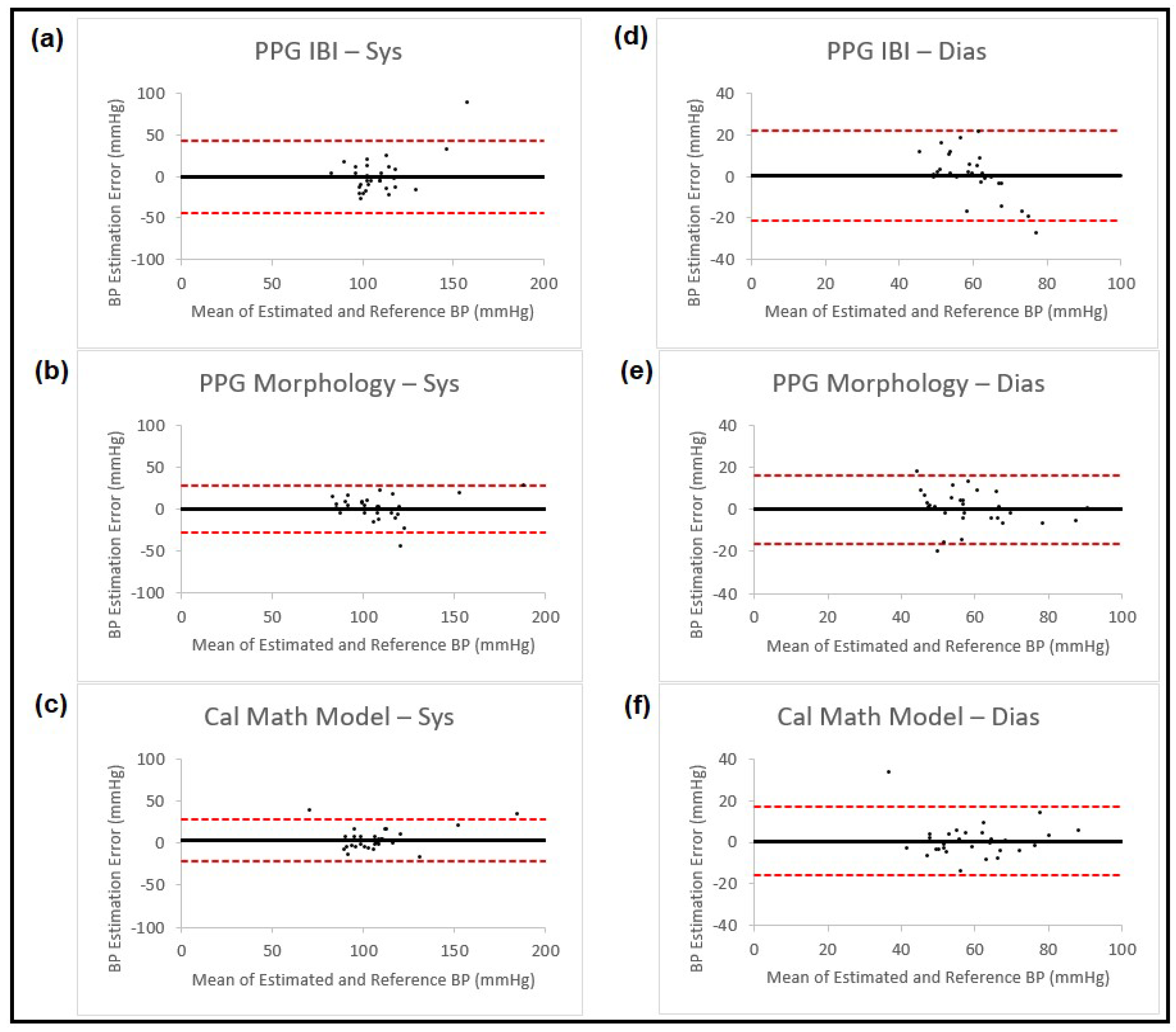
- Features from cardiovascular dynamics extracted from PPG signal. This is a calibration-free method that we developed in [17];
- Information based on PPG morphology features. Estimation for both SBP and DBP was performed based on 21 extracted morphology features;
- A calibrated mathematical model. This is part of our previous work [11], where we used a mathematical model to calibrate the blood pressure estimator.
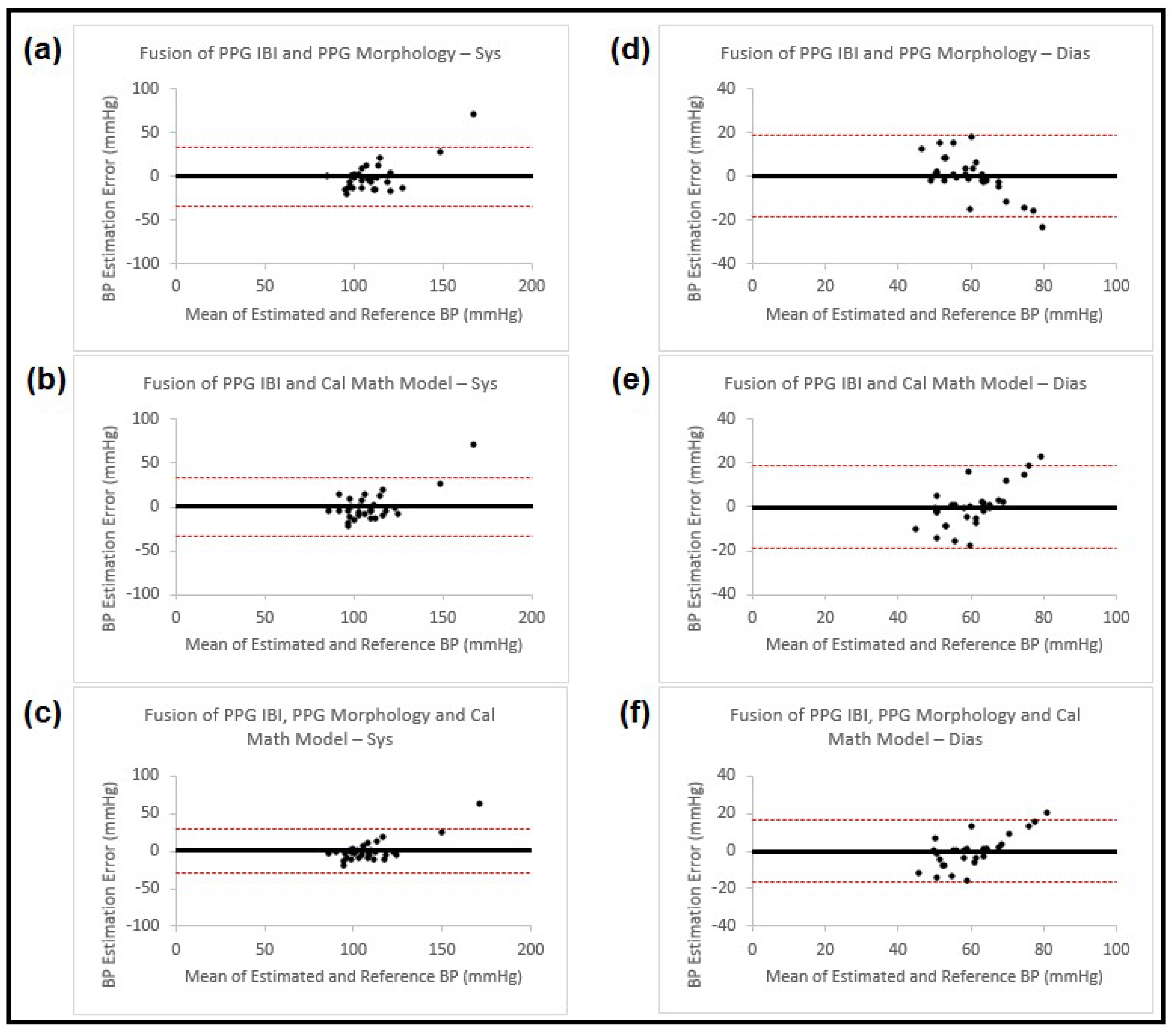
- Fusion technique;
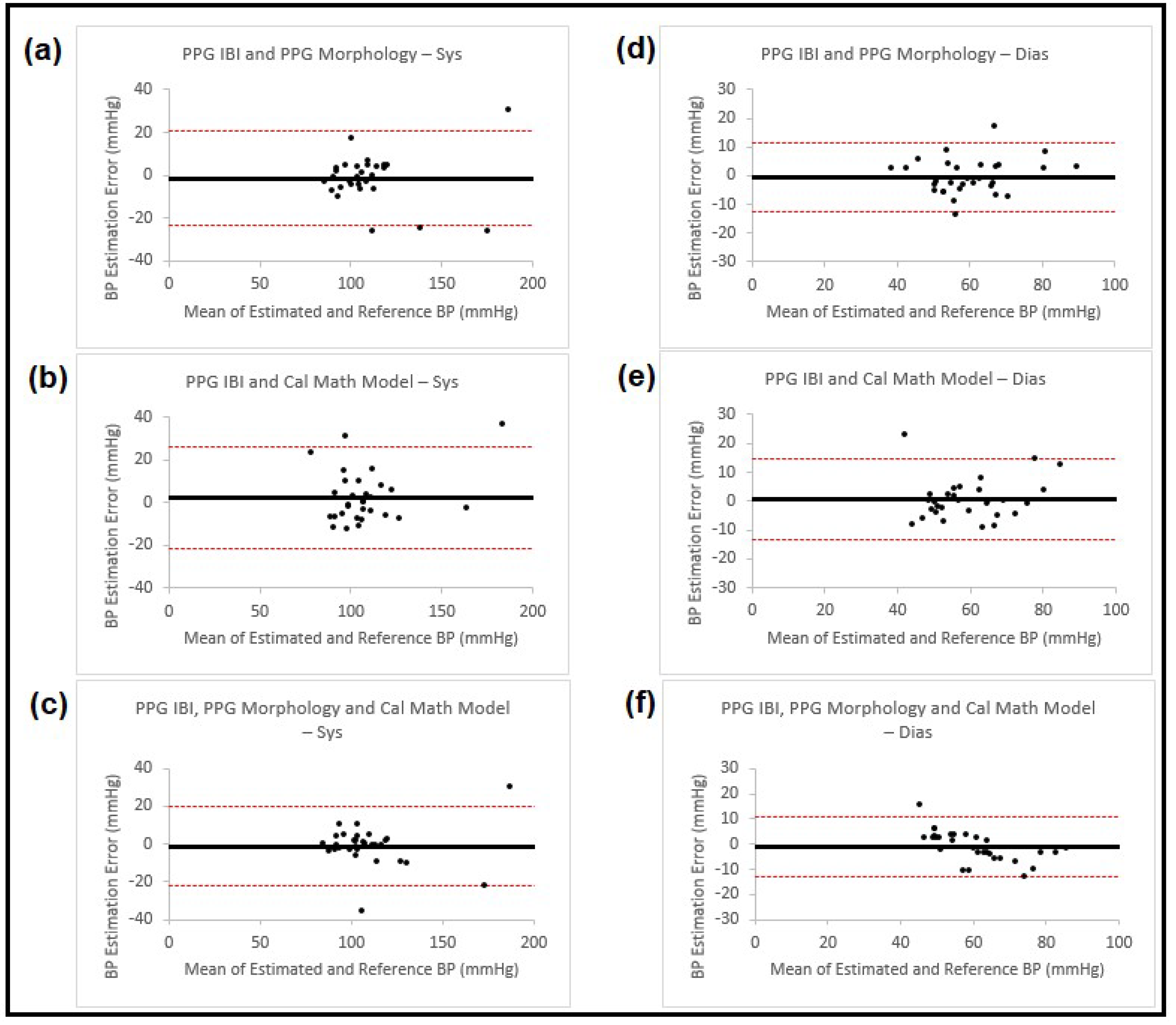
- Feature combination.
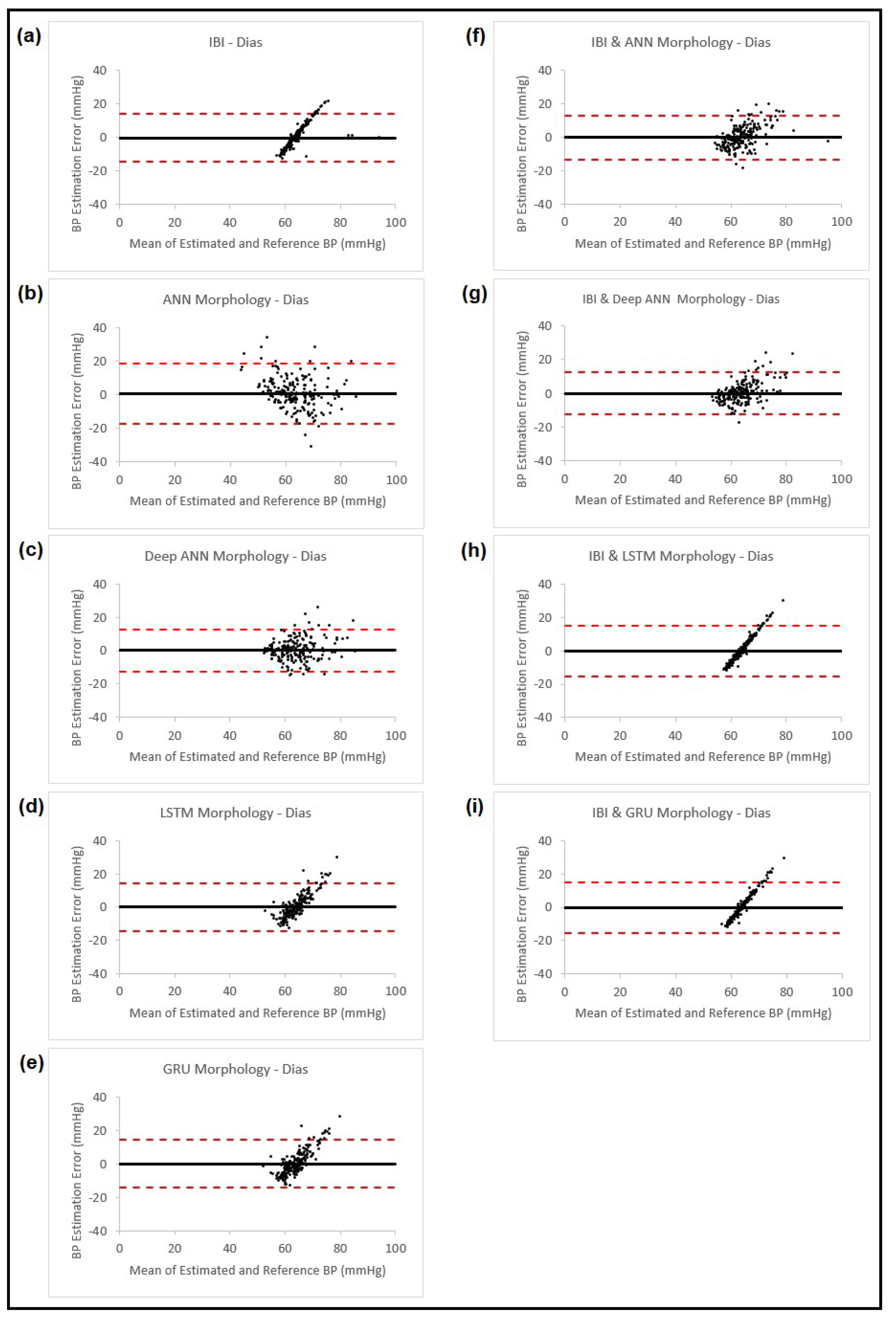
3.2. Estimation of BP with 200 Patients from the UCI Dataset
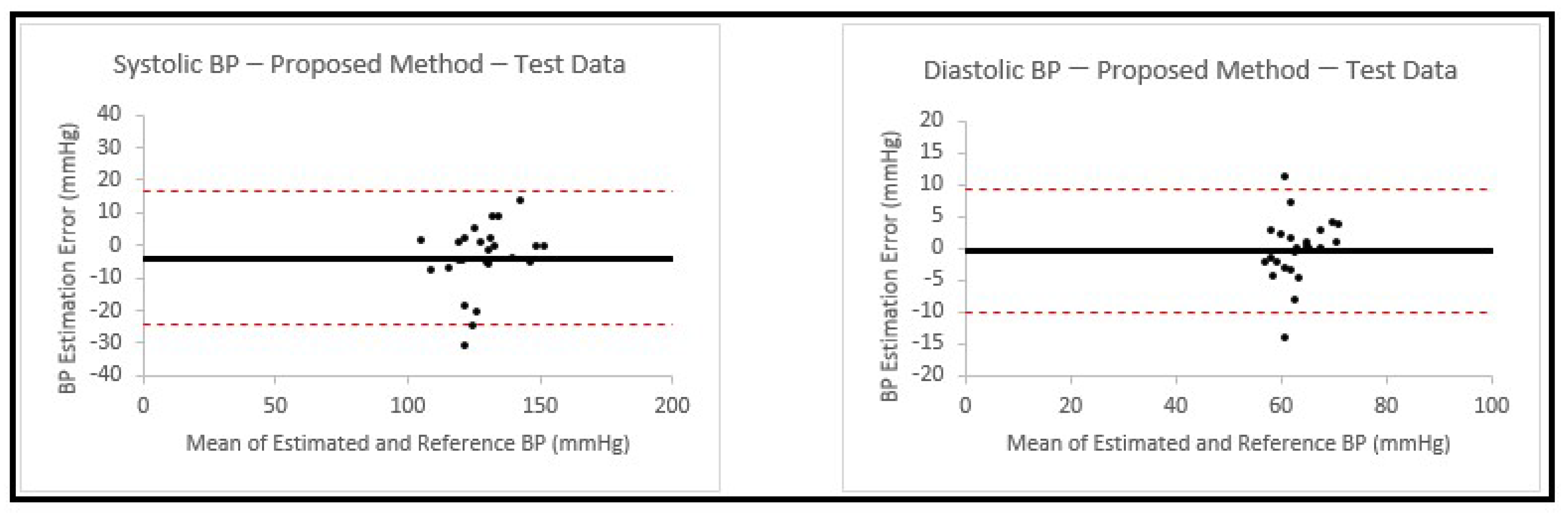
3.3. Estimation of BP with 25 New Patients from the UCI Dataset
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, L.; Zhou, W.; Xing, Y.; Zhou, X. A novel neural network model for blood pressure estimation using photoplethesmography without electrocardiogram. J. Healthc. Eng. 2018, 2018, 7804243. [Google Scholar] [CrossRef] [PubMed]
- Agham, N.; Chaskar, U. An advanced LAN model based on optimized feature algorithm: Towards hypertension interpretability. Biomed. Signal Process. Control 2021, 68, 102760. [Google Scholar] [CrossRef]
- World Health Organization. WHO Reveals Leading Causes of Death and Disability Worldwide: 2000–2019. Available online: https://www.who.int/news/item/09-12-2020-who-reveals-leading-causes-of-death-and-disability-worldwide-2000-2019 (accessed on 18 January 2023).
- Yamakoshi, T.; Rolfe, P.; Yamakoshi, K.I. Cuffless blood pressure estimation based on haemodynamic principles progress towards mobile healthcare. Peer J. 2021, 9, e11479. [Google Scholar] [CrossRef] [PubMed]
- Xing, X.; Ma, Z.; Zhang, M.; Zhou, Y.; Dong, W.; Song, M. An unobtrusive and calibration-free blood pressure estimation method using photoplethysmography and biometrics. Sci. Rep. 2019, 9, 8611. [Google Scholar] [CrossRef] [PubMed]
- Slapnicar, G.; Mlakar, N.; Lustrek, M. Blood pressure estimation from photoplethysmogram using a spectro-temporal deep neural network. Sensors 2019, 19, 3420. [Google Scholar] [CrossRef]
- Hassani, A.; Foruzan, A.H. Improved PPG-based estimation of the blood pressure using latent space features. Signal Image Video Process. 2019, 13, 1141–1147. [Google Scholar] [CrossRef]
- Ruiz-Rodriguez, J.C.; Ruiz-Sanmartin, A.; Caballero, J.; Garcia-Roche, A.; Riera, J.; Nuvials, X.; de Nadal, M.; de Sola-Morales, O.; Serra, J.; Rello, J. Innovative continuous non-invasive cuffless blood pressure monitoring based on photoplethysmography technology. Intensive Care Med. 2013, 39, 1618–1625. [Google Scholar] [CrossRef]
- Mohebbian, M.R.; Dinh, A.; Wahid, K.; Alam, M.S. Blind, cuff-less, calibration-free and continuous blood pressure estimation using optimized inductive group method of data handling. Biomed. Signal Process. Control 2020, 57, 101682. [Google Scholar] [CrossRef]
- El-Hajj, C.; Kyriacou, P.A. Deep learning models for cuffless blood pressure monitoring from PPG signals attention mechanism. Biomed. Signal Process. Control 2021, 65, 102301. [Google Scholar] [CrossRef]
- Samimi, H.; Dajani, H.R. Cuffless blood pressure estimation using calibrated cardiovascular dynamics in the photoplethysmogram. Bioengineering 2022, 9, 446. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, Y. A novel frequency domain method for estimating blood pressure from photoplethysmogram. In Proceedings of the 9th International Conference on Signal Processing Systems, Auckland, New Zealand, 27–30 November 2017; pp. 201–206. [Google Scholar]
- Fukushima, H.; Kawanaka, H.; Bhuiyan, M.S.; Oguri, K. Cuffless blood pressure estimation using only photoplethysmography based on cardiovascular parameters. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Osaka, Japan, 3–7 July 2013; pp. 2132–2135. [Google Scholar]
- Fati, S.M.; Muneer, A.; Akbar, N.A.; Taib, S.M. A continuous cuffless blood pressure estimation using tree-based pipeline optimization tool. Symmetry 2021, 13, 686. [Google Scholar] [CrossRef]
- Pan, J.; Zhang, Y. Improved blood pressure estimation using photoplethysmography based on ensemble method. In Proceedings of the 14th International Symposium on Pervasive Systems, Algorithms and Networks, I-SPAN, 11th International Conference on Frontier of Computer Science and Technology, FCST and 3rd International Symposium of Creative Computing, ISCC 2017, Exeter, UK, 21–23 June 2017; pp. 105–111. [Google Scholar]
- Li, P.; Laleg-Kirati, T.M. Central blood pressure estimation from distal PPG measurement using semiclassical signal analysis features. IEEE Access 2021, 9, 44963–44973. [Google Scholar] [CrossRef]
- Samimi, H.; Dajani, H.R. Cuffless Blood Pressure Estimation Using Cardiovascular Dynamics. In Proceedings of the International Conference on Electrical, Computer and Energy Technologies (ICECET 2022), Prague, Czech Republic, 20–22 July 2022; Available online: https://ieeexplore-ieee-org.proxy.bib.uottawa.ca/document/9872800 (accessed on 5 February 2023).
- Sulochana, C.H. A review of photoplethysmography based measurement of blood pressure and heart rate variability. J. Bioeng. Biomed. Sci. 2021, 11, 862. [Google Scholar]
- Sagirova, Z.; Kuznetsova, N.; Gogiberidze, N.; Gognieva, D.; Suvorov, A.; Chomakhidze, P.; Omboni, S.; Saner, H.; Kopylov, P. Cuffless blood pressure measurement using a smartphone-case based ECG monitor with photoplethysmography in hypertensive patients. Sensors 2021, 21, 3525. [Google Scholar] [CrossRef]
- Kurylyak, Y.; Lamonaca, F.; Grimaldi, D. A neural network-based method for continuous blood pressure estimation from a PPG signal. In Proceedings of the 2013 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Minneapolis, MN, USA, 6–9 May 2013. [Google Scholar]
- Malayeri, A.B.; Khodabakhshi, M.B. Concatenated convolutional neural network model for cuffless blood pressure estimation using fuzzy recurrence properties of photoplethysmogram signals. Sci. Rep. 2022, 12, 6633. [Google Scholar] [CrossRef] [PubMed]
- Soh, D.C.K.; Ng, E.Y.K.; Jahmunah, V.; Oh, S.L.; Tan, R.S.; Acharya, U.R. Automated diagnostic tool for hypertension using convolutional neural network. Comput. Biol. Med. 2020, 126, 103999. [Google Scholar] [CrossRef] [PubMed]
- Paviglianiti, A.; Randazzo, V.; Villata, S.; Cirrincione, G.; Pasero, E. A comparison of deep learning techniques for arterial blood pressure prediction. Cogn. Comput. 2022, 14, 1689–1710. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.Y.; Xie, S.; Gallagher, P.; Zhang, Z.; Tu, Z. Deeply-supervised nets. In Proceedings of the Artificial Intelligence and Statistics, Valencia, Spain, 28–30 March 2015; pp. 562–570. [Google Scholar]
- Ibtehaz, N.; Mahmud, S.; Chowdhury, M.E.H.; Khandakar, A.; Salman Khan, M.; Ayari, M.A.; Tahir, A.M.; Rahman, M.S. PPG2ABP: Translating photoplethysmogram (PPG) signals to arterial blood pressure (ABP) waveforms. Bioengineering 2022, 9, 692. [Google Scholar] [CrossRef]
- Chao, P.C.P.; Wu, C.C.; Nguyen, D.H.; Nguyen, B.S.; Huang, P.C.; Le, V.H. The machine learnings leading the cuffless PPG blood pressure sensors into the next stage. IEEE Sens. J. 2021, 21, 12498–12510. [Google Scholar] [CrossRef]
- Liu, D.; Gorges, M.; Jenkins, S.A. University of Queensland vital signs dataset: Development of an accessible repository of anesthesia patient monitoring data for research. Anesth. Analg. 2012, 114, 584–589. [Google Scholar] [CrossRef]
- Kachuee, M.; Kiani, M.M.; Mohammadzadeh, H.; Shabany, M. Cuffless high-accuracy calibration-free blood pressure estimation using pulse transit time. In Proceedings of the IEEE International Symposium on Circuit and Systems (ISCAS”15), Lisbon, Portugal, 24–27 May 2015. [Google Scholar]
- Hameed, S.S.; Petinrin, O.O.; Hashi, A.O.; Saeed, F. Filter-wrapper combination and embedded feature selection for gene expression data. Int. J. Adv. Soft Comput. Its Appl. 2018, 10, 90–105. [Google Scholar]
- Shao, J.; Shi, P.; Hu, S.; Yu, H. A revised point-to-point calibration approach with adaptive errors correction to weaken initial sensitivity of cuff-less blood pressure estimation. Sensors 2020, 20, 2205. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Rosasco, L.; Caponnetto, A. On early stopping in gradient descent learning. Constr. Approx. 2007, 26, 289–315. [Google Scholar] [CrossRef]
- Wang, Q.; Zeng, Q.; Tao, J.; Sun, L.; Zhang, L.; Gu, T.; Wang, Z.; Chen, L. Estimating PM2.5 concentrations based on MODIS AOD and NAQPMS data over Beijing–Tianjin–Hebei. Sensors 2019, 19, 1207. [Google Scholar] [CrossRef] [PubMed]
- Ribezzo, S.; Spina, E.; Di Bartolomeo, S.; Sanson, G. Noninvasive techniques for blood pressure measurement are not reliable alternative to direct measurement: A randomized crossover train in ICU. Sci. World J. 2014, 2014, 353628. [Google Scholar] [CrossRef]
- Kaur, B.; Kaur, S.; Yaddanapudi, L.N.; Singh, N.V. Comparison between invasive and noninvasive blood pressure measurements in critically ill patients receiving inotropes. Blood Press. Monit. 2019, 24, 24–29. [Google Scholar] [CrossRef]
- Shimada, K.; Kario, K.; Kushiro, T.; Teramukai, S.; Ishikawa, Y.; Kobayashi, H.; Saito, I. Differences between clinic blood pressure and morning home blood pressure, as shown by Bland-Altman plots, in a large observational study (HONEST study). Hypertens. Res. 2015, 38, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Verberk, W.J.; Kroon, A.A.; Kessels, A.G.H.; de Leeuw, P.W. Home blood pressure measurement. J. Am. Coll. Cardiol. 2005, 46, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Saito, I.; Eguchi, E.; Maruyama, K.; Kato, T.; Tanigawa, T. Heart rate variability and blood pressure among Japanese men and women: A community-based cross-sectional study. Hypertens. Res. 2014, 37, 779–784. [Google Scholar] [CrossRef]
- Takalo, R.; Korhonen, I.; Turjanmaa, V.; Majahalme, S.; Tuomisto, M.; Uusitalo, A. Short-term variability of blood pressure and heart rate in borderline and mildly hypertensive subjects. Hypertension 1994, 23, 18–24. [Google Scholar] [CrossRef]
- Kan, A.W.; Hussain, T.; Carson, K.A.; Purnell, T.S.; Yeh, H.C.; Albert, M.; Cooper, L.A. The contribution of age and weight to blood pressure levels among blacks and whites receiving care in community-based primary care practices. Prev. Chronic Dis. 2015, 12, 150069. [Google Scholar] [CrossRef] [PubMed]
- Reckelhoff, J.F. Gender differences in the regulation of blood pressure. Hypertension 2001, 37, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Barbedo, J.G.A. Impact of dataset size and variety on the effectiveness of deep learning and transfer learning for plant disease classification. Comput. Electron. Agric. 2018, 153, 46–53. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Systolic BP (mmHg) | Diastolic BP (mmHg) | |||||
|---|---|---|---|---|---|---|
| ME | SDE | MAE | ME | SDE | MAE | |
| PPG IBI | −0.39 | 22.16 | 15.26 | 0.14 | 10.97 | 7.54 |
| PPG Morphology | 0.06 | 14.22 | 10.10 | 0.01 | 8.32 | 6.16 |
| Calibrated Mathematical Model | 3.18 | 12.49 | 9.11 | 0.45 | 8.36 | 5.47 |
| Systolic BP (mmHg) | Diastolic BP (mmHg) | |||||
|---|---|---|---|---|---|---|
| ME | SDE | MAE | ME | SDE | MAE | |
| Fusion of PPG IBI and PPG Morphology | −0.25 | 17.54 | 11.16 | 0.11 | 9.42 | 6.60 |
| Fusion of PPG IBI and Calibrated Mathematical Model | 0.70 | 17.22 | 11.03 | −0.03 | 9.60 | 6.76 |
| Fusion of PPG IBI, PPG Morphology and Calibrated Mathematical Model | 0.58 | 14.85 | 8.95 | −0.03 | 8.52 | 6.09 |
| Systolic BP (mmHg) | Diastolic BP (mmHg) | |||||
|---|---|---|---|---|---|---|
| ME | SDE | MAE | ME | SDE | MAE | |
| PPG IBI and PPG Morphology | −1.51 | 11.23 | 7.50 | −0.42 | 6.14 | 4.94 |
| PPG IBI and Calibrated Mathematical Model | 2.52 | 12.15 | 8.89 | 0.59 | 7.07 | 4.92 |
| PPG IBI, PPG Morphology and Calibrated Mathematical Model | −1.15 | 10.69 | 7.41 | −1.11 | 6.07 | 4.90 |
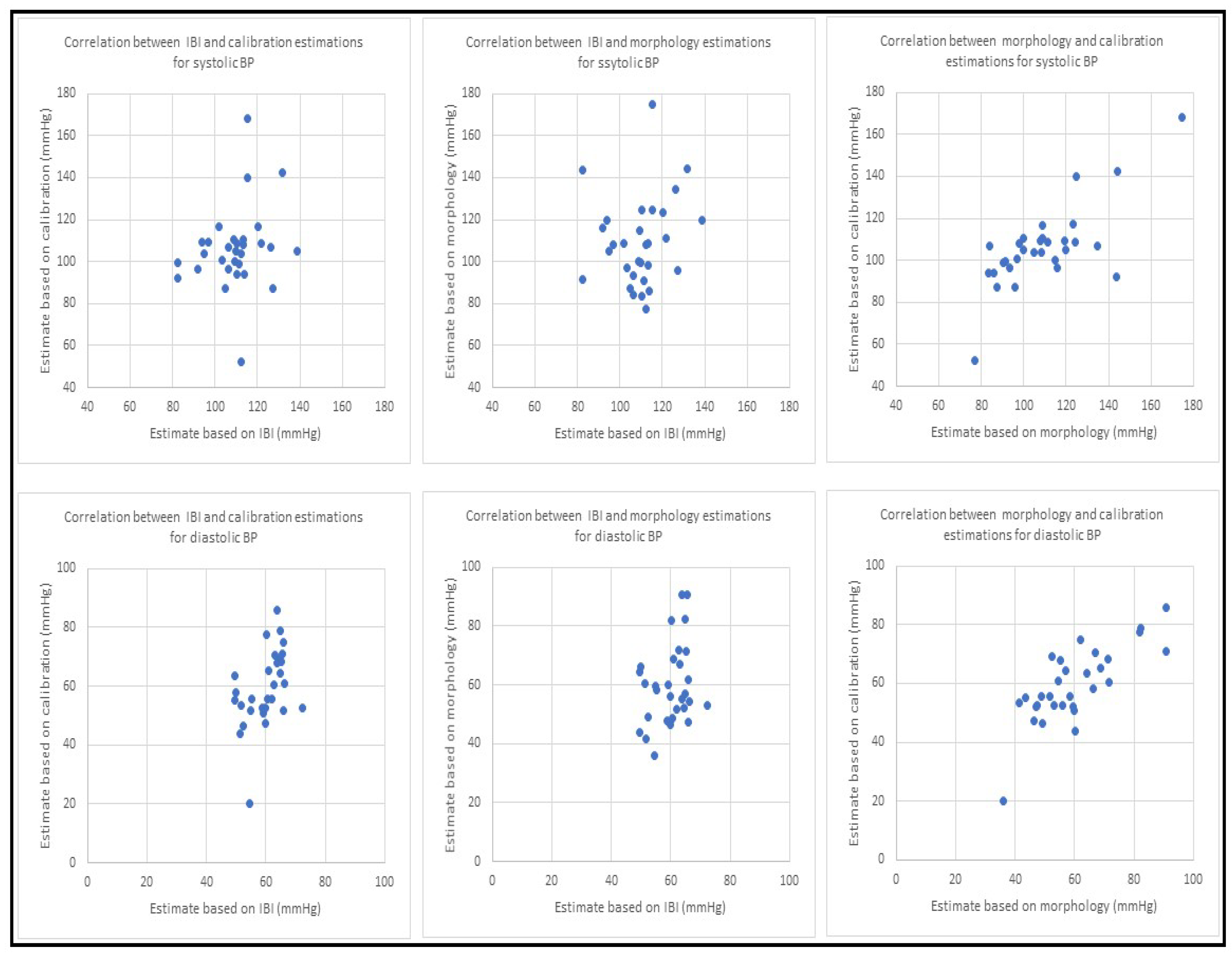
| Correlation between BP Estimation Using Different Methods for PPG Signals | |||
|---|---|---|---|
| IBI and Calibration | IBI and Morphology | Morphology and Calibration | |
| Systolic BP | 0.23 | 0.16 | 0.74 |
| Diastolic BP | 0.45 | 0.29 | 0.78 |
| Systolic BP (mmHg) | Diastolic BP (mmHg) | |||||
|---|---|---|---|---|---|---|
| ME | SDE | MAE | ME | SDE | MAE | |
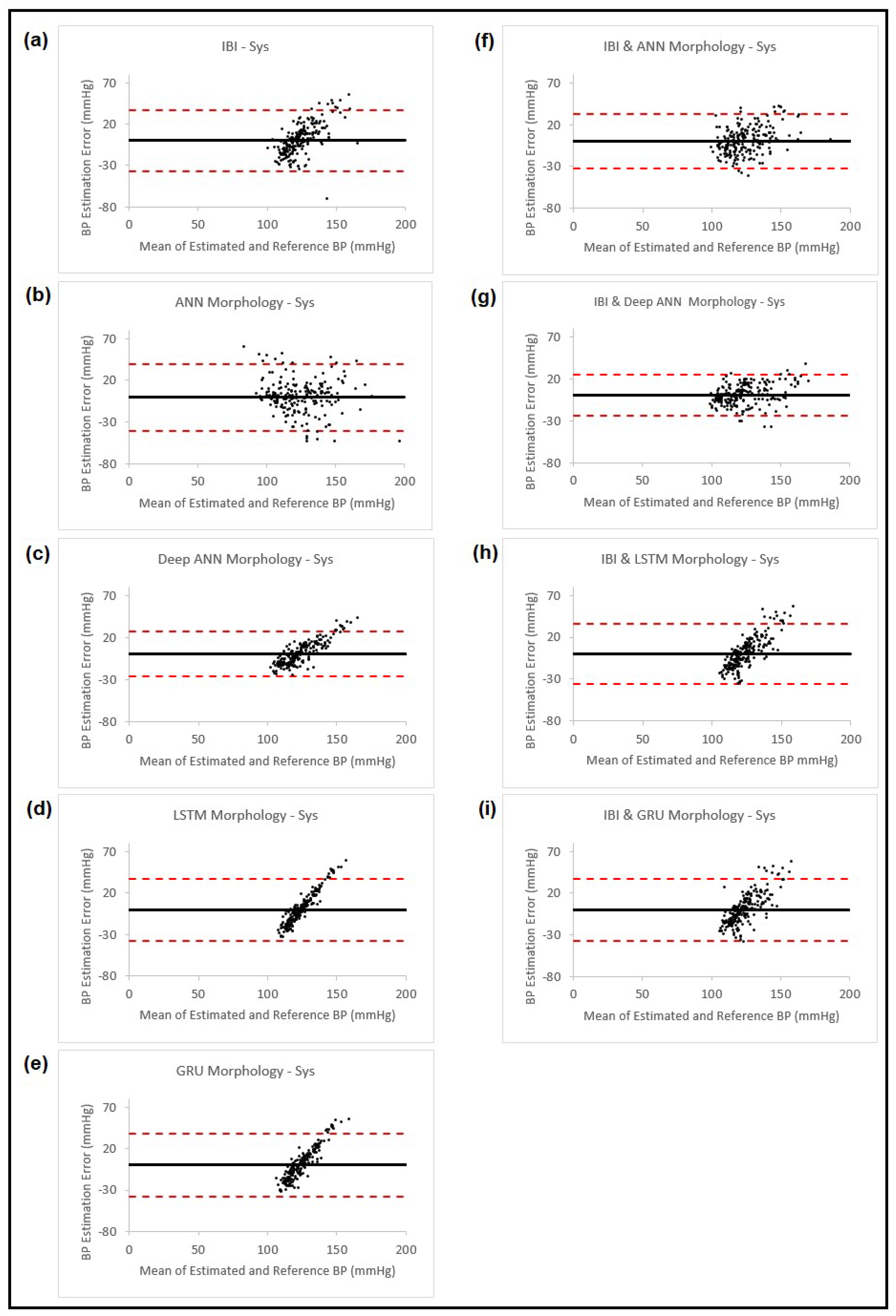
| PPG IBI | 0.09 | 18.81 | 14.49 | 0.03 | 7.91 | 5.75 |
| PPG Morphology using Feedforward Neural Network Model | −0.52 | 20.30 | 14.51 | 0.64 | 9.29 | 6.78 |
| PPG Morphology using Feedforward Deep Neural Network Model | 0.36 | 13.81 | 11.24 | 0.12 | 6.49 | 4.75 |
| PPG Morphology using LTSM Model | −0.17 | 19.11 | 15.20 | −0.05 | 7.35 | 5.59 |
| PPG Morphology using GRU Model | 0.07 | 19.22 | 15.30 | 0.10 | 7.29 | 5.59 |
| PPG Morphology using Feedforward NN Model and PPG IBI | 0.01 | 16.38 | 13.04 | −0.30 | 6.67 | 5.31 |
| PPG Morphology using Feedforward Deep NN Model and PPG IBI | 0.15 | 12.40 | 9.74 | −0.01 | 6.29 | 4.65 |
| PPG Morphology using LSTM Model and PPG IBI | 0.11 | 18.49 | 14.63 | −0.04 | 7.77 | 6.05 |
| PPG Morphology using GRU Model and PPG IBI | 0.10 | 18.87 | 14.90 | −0.04 | 7.78 | 6.07 |
| IBI and Estimation from Feedforward Deep NN with ANN Model | |||
|---|---|---|---|
| ME (mmHg) | SDE (mmHg) | MAE (mmHg) | |
| Systolic BP | −4.02 | 10.40 | 7.41 |
| Diastolic BP | −0.31 | 4.89 | 3.32 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samimi, H.; Dajani, H.R. A PPG-Based Calibration-Free Cuffless Blood Pressure Estimation Method Using Cardiovascular Dynamics. Sensors 2023, 23, 4145. https://doi.org/10.3390/s23084145
Samimi H, Dajani HR. A PPG-Based Calibration-Free Cuffless Blood Pressure Estimation Method Using Cardiovascular Dynamics. Sensors. 2023; 23(8):4145. https://doi.org/10.3390/s23084145
Chicago/Turabian StyleSamimi, Hamed, and Hilmi R. Dajani. 2023. "A PPG-Based Calibration-Free Cuffless Blood Pressure Estimation Method Using Cardiovascular Dynamics" Sensors 23, no. 8: 4145. https://doi.org/10.3390/s23084145
APA StyleSamimi, H., & Dajani, H. R. (2023). A PPG-Based Calibration-Free Cuffless Blood Pressure Estimation Method Using Cardiovascular Dynamics. Sensors, 23(8), 4145. https://doi.org/10.3390/s23084145