

The r’-Wave Algorithm: A New Diagnostic Tool to Predict the Diagnosis of Brugada Syndrome after a Sodium Channel Blocker Provocation Test

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
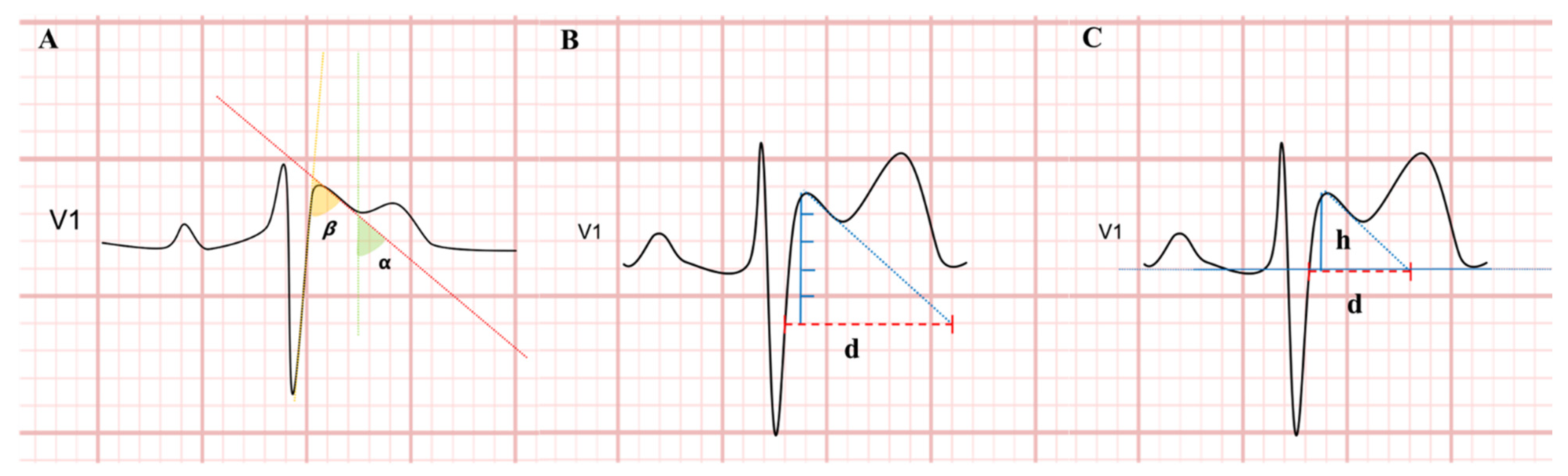
2.2. Electrocardiographic Analysis
2.3. Statistical Analysis
3. Results
3.1. Overall Population
3.2. Test Cohort
3.3. Validation Cohort
3.4. Intra- and Inter-Observer Variability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Antzelevitch, C.; Yan, G.-X.; Ackerman, M.J.; Borggrefe, M.; Corrado, D.; Guo, J.; Gussak, I.; Hasdemir, C.; Horie, M.; Huikuri, H.; et al. J-Wave Syndromes Expert Consensus Conference Report: Emerging Concepts and Gaps in Knowledge. Europace 2017, 19, 665–694. [Google Scholar] [CrossRef] [PubMed]
- Therasse, D.; Sacher, F.; Petit, B.; Babuty, D.; Mabo, P.; Martins, R.; Jesel, L.; Maury, P.; Pasquie, J.L.; Mansourati, J.; et al. Sodium-Channel Blocker Challenge in the Familial Screening of Brugada Syndrome: Safety and Predictors of Positivity. Heart Rhythm 2017, 14, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Brugada, J.; Campuzano, O.; Arbelo, E.; Sarquella-Brugada, G.; Brugada, R. Present Status of Brugada Syndrome: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 1046–1059. [Google Scholar] [CrossRef] [PubMed]
- Chevallier, S.; Forclaz, A.; Tenkorang, J.; Ahmad, Y.; Faouzi, M.; Graf, D.; Schlaepfer, J.; Pruvot, E. New Electrocardiographic Criteria for Discriminating between Brugada Types 2 and 3 Patterns and Incomplete Right Bundle Branch Block. J. Am. Coll. Cardiol. 2011, 58, 2290–2298. [Google Scholar] [CrossRef] [PubMed]
- Serra, G.; Baranchuk, A.; Bayés-De-Luna, A.; Brugada, J.; Goldwasser, D.; Capulzini, L.; Arazo, D.; Boraita, A.; Heras, M.-E.; Garcia-Niebla, J.; et al. New Electrocardiographic Criteria to Differentiate the Type-2 Brugada Pattern from Electrocardiogram of Healthy Athletes with r’-Wave in Leads V1/V2. Europace 2014, 16, 1639–1645. [Google Scholar] [CrossRef] [PubMed]
- van der Ree, M.H.; Vendrik, J.; Verstraelen, T.E.; Kors, J.A.; Amin, A.S.; Wilde, A.A.M.; Tan, H.L.; Postema, P.G. The β-Angle Can Help Guide Clinical Decisions in the Diagnostic Work-up of Patients Suspected of Brugada Syndrome: A Validation Study of the β-Angle in Determining the Outcome of a Sodium Channel Provocation Test. Europace 2021, 23, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Ohkubo, K.; Watanabe, I.; Okumura, Y.; Ashino, S.; Kofune, M.; Nagashima, K.; Nakai, T.; Kunimoto, S.; Kasamaki, Y.; Hirayama, A. A New Criteria Differentiating Type 2 and 3 Brugada Patterns from Ordinary Incomplete Right Bundle Branch Block. Int. Heart J. 2011, 52, 159–163. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Brugada, P.; Brugada, J. Right Bundle Branch Block, Persistent ST Segment Elevation and Sudden Cardiac Death: A Distinct Clinical and Electrocardiographic Syndrome. A Multicenter Report. J. Am. Coll. Cardiol. 1992, 20, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Milman, A.; Andorin, A.; Gourraud, J.-B.; Postema, P.G.; Sacher, F.; Mabo, P.; Kim, S.-H.; Juang, J.J.M.; Maeda, S.; Takahashi, Y.; et al. Profile of Patients with Brugada Syndrome Presenting with Their First Documented Arrhythmic Event: Data from the Survey on Arrhythmic Events in BRUgada Syndrome (SABRUS). Heart Rhythm 2018, 15, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Crea, P.; Rivetti, L.; Bitto, R.; Nicotera, A.; Zappia, L.; Caracciolo, A.; Scalise, R.; Salito, A.; Mazzone, P.; Pellegrino, N.; et al. Diagnosis of Type 2 Brugada Pattern: Insights from a Pilot Survey. Minerva Cardiol. Angiol. 2021, 69, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Baranchuk, A.; Nguyen, T.; Ryu, M.H.; Femenía, F.; Zareba, W.; Wilde, A.A.M.; Shimizu, W.; Brugada, P.; Pérez-Riera, A.R. Brugada Phenocopy: New Terminology and Proposed Classification. Ann. Noninvasive Electrocardiol. 2012, 17, 299–314. [Google Scholar] [CrossRef] [PubMed]
- Wilde, A.A.M.; Postema, P.G.; Di Diego, J.M.; Viskin, S.; Morita, H.; Fish, J.M.; Antzelevitch, C. The Pathophysiological Mechanism Underlying Brugada Syndrome: Depolarization versus Repolarization. J. Mol. Cell Cardiol. 2010, 49, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Nagase, S.; Hiramatsu, S.; Morita, H.; Nishii, N.; Murakami, M.; Nakamura, K.; Kusano, K.F.; Ito, H.; Ohe, T. Electroanatomical Correlation of Repolarization Abnormalities in Brugada Syndrome: Detection of Type 1 Electrocardiogram in the Right Ventricular Outflow Tract. J. Am. Coll. Cardiol. 2010, 56, 2143–2145. [Google Scholar] [CrossRef] [PubMed]
- Gottschalk, B.H.; Garcia-Niebla, J.; Anselm, D.D.; Jaidka, A.; De Luna, A.B.; Baranchuk, A. New Methodologies for Measuring Brugada ECG Patterns Cannot Differentiate the ECG Pattern of Brugada Syndrome from Brugada Phenocopy. J. Electrocardiol. 2016, 49, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Vetta, G.; Magnocavallo, M.; Polselli, M.; Parlavecchio, A.; Caminiti, R.; Cauti, F.M.; Lo Savio, A.; Vetta, F. The Role of the β-Angle in the Management of Patients with Suspected Brugada Syndrome: A Metanalysis. JAFib-EP. 2022, 24, 91. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (n = 395) | Negative SCBPT (n = 300) | Positive SCBPT (n = 95) | p Value | |
|---|---|---|---|---|
| Age, years | 44.7 ± 13.5 | 44.1 ± 13.6 | 46.8 ± 12.9 | 0.090 |
| Sex male, % (n) | 72.4 (286) | 73.3 (220) | 69.5 (29) | 0.463 |
| LVEF, % | 58.7 ± 4.7 | 58.3 ± 5.3 | 59.3 ± 4.3 | 0.436 |
| Flecainide administered, mg | 122 ± 13 | 130 ± 15 | 100 ± 12 | <0.0001 |
| Indication for test | ||||
| Suspicious ECG, % (n) | 24.2 (96) | 21.7 (65) | 32.6 (31) | 0.03 |
| Symptoms, % (n) | 7.1 (28) | 6.7 (20) | 8.4 (8) | 0.561 |
| Family history of BrS, % (n) | 49.5 (196) | 48.3 (145) | 52.6 (50) | 0.465 |
| Family history of sudden cardiac death, % (n) | 19.2 (76) | 23.3 (70) | 6.3 (6) | <0.0001 |
| Overall (n = 198) | Negative SCBPT (n = 150) | Positive SCBPT (n = 48) | p Value | |
|---|---|---|---|---|
| Age, years | 44.5 ± 13.3 | 44.1 ± 13.6 | 45.8 ± 12.2 | 0.455 |
| Sex Male, % (n) | 70.2 (139) | 73.3 (110) | 60.4 (29) | 0.089 |
| LVEF, % | 58.9 ± 4.3 | 58.2 ± 5.2 | 59.6 ± 4.1 | 0.463 |
| Flecainide administered, mg | 123 ± 12 | 129 ± 14 | 101 ± 11 | <0.0001 |
| Indication for test | ||||
| Suspicious ECG, % (n) | 24.2 (48) | 23.3 (35) | 27.1 (13) | 0.598 |
| Symptoms, % (n) | 6.1 (12) | 6.7 (10) | 4.2 (2) | 0.528 |
| Family history of BrS, % (n) | 59.1 (117) | 60 (90) | 56.3 (27) | 0.646 |
| Family history of sudden cardiac death, % (n) | 10.6 (21) | 10 (15) | 12.5 (6) | 0.624 |
| Overall (n = 198) | Negative SCBPT (n = 150) | Positive SCBPT (n = 48) | p Value | |
|---|---|---|---|---|
| Heart rate, bpm | 73.2 ± 14.2 | 73.7 ± 15.1 | 71.6 ± 11.2 | 0.368 |
| p-wave, ms | 104 ± 12.4 | 103.4 ± 12.4 | 106.2 ± 12.4 | 0.178 |
| PR interval, ms | 159.1 ± 23.6 | 157.9 ± 23.5 | 162.8 ± 23.9 | 0.209 |
| QRS duration, ms | 97.4 ± 7.4 | 97.2 ± 6.2 | 98.2 ± 10.4 | 0.410 |
| QT interval, ms | 386.5 ± 25.2 | 385.6 ± 25.9 | 389.5 ± 23.2 | 0.358 |
| QTc interval, ms | 418.8 ± 31.2 | 417.6 ± 33.2 | 422 ± 23.9 | 0.328 |
| P axis, ° | 56.3 ± 21.4 | 57.2 ± 21.7 | 53.4 ± 20.4 | 0.291 |
| QRS axis, ° | 41.4 ± 32.6 | 43.3 ± 34.3 | 36 ± 26.8 | 0.184 |
| T axis, ° | 46.6 ± 21.5 | 45.80 ± 28.9 | 49.06 ± 23.2 | 0.360 |
| Measurability of r’-wave at: | ||||
| IV° ic, % (n) | 7.6 (15) | 4 (6) | 18.8 (9) | 0.001 |
| III° ic, % (n) | 20.2 (40) | 16.7 (25) | 31.3 (15) | 0.029 |
| II° ic, % (n) | 33.3 (66) | 22.7 (34) | 66.7 (32) | <0.0001 |
| Majorβ-angle | 43.3 ± 16.7 | 34.3 ± 14.9 | 53.1 ± 12.6 | <0.0001 |
| Majorα-angle | 32.9 ± 14.9 | 25.3 ± 12.5 | 41.4 ± 12.7 | <0.0001 |
| Major DBT- 5 mm | 196.1 ± 126.2 | 149 ± 144.1 | 247.5 ± 76.9 | <0.0001 |
| Major DBT- iso | 90.5 ± 34.5 | 74.6 ± 24.4 | 107.9 ± 35.8 | <0.0001 |
| Major triangle base/height | 1.3 ± 0.7 | 1.1 ± 0.6 | 1.4 ± 0.7 | 0.03 |
| Overall (n = 197) | Negative SCBPT (n = 150) | Positive SCBPT (n = 47) | p Value | |
|---|---|---|---|---|
| Age, years | 44.9 ± 13.7 | 44.1 ± 13.6 | 47.9 ± 13.7 | 0.101 |
| Sex Male, % (n) | 74.6 (147) | 73.3 (110) | 78.7 (37) | 0.459 |
| LVEF, % | 58.5 ± 4.6 | 58.2 ± 5.2 | 59.6 ± 4.1 | 0.463 |
| Flecainide administered, mg | 122 ± 11 | 128 ± 15 | 102 ± 12 | <0.0001 |
| Indication for test | ||||
| Suspicious ECG, % (n) | 24.4 (48) | 20 (30) | 38.3 (18) | 0.01 |
| Symptoms, % (n) | 8.1 (16) | 6.7 (10) | 12.8 (6) | 0.182 |
| Family history of BrS, % (n) | 39.6 (78) | 36.7 (55) | 48.9 (23) | 0.133 |
| Family history of sudden cardiac death, % (n) | 27.9 (55) | 36.7 (55) | 0 (0) | <0.0001 |
| Overall (n = 197) | Negative SCBPT (n = 150) | Positive SCBPT (n = 47) | p Value | |
|---|---|---|---|---|
| Heart rate, bpm | 73.9 ± 15.1 | 73.7 ± 15.1 | 70.1 ± 14.8 | 0.150 |
| p-wave, ms | 103.8 ± 12.7 | 103.4 ± 12.4 | 105.2 ± 13.8 | 0.392 |
| PR interval, ms | 158.6 ± 24.7 | 157.9 ± 23.5 | 161 ± 28.3 | 0.451 |
| QRS duration, ms | 97.8 ± 9.1 | 97.2 ± 6.2 | 99.7 ± 15.1 | 0.104 |
| QT interval, ms | 385.8 ± 28.3 | 385.6 ± 25.9 | 386.3 ± 35.1 | 0.890 |
| QTc interval, ms | 416.2 ± 30.8 | 417.6 ± 33.2 | 411.9 ± 21.1 | 0.280 |
| P axis, ° | 55.5 ± 20.1 | 57.2 ± 21.7 | 50.1 ± 12.1 | 0.06 |
| QRS axis, ° | 40.1 ± 34.5 | 43.3 ± 34.3 | 30.6 ± 33.7 | 0.06 |
| T axis, ° | 44.3 ± 20.8 | 45.8 ± 28.9 | 39.7 ± 20.1 | 0.079 |
| Measurability of r’-wave at: | ||||
| IV° ic, % (n) | 11.2 (22) | 6 (9) | 27.7 (13) | <0.0001 |
| III° ic, % (n) | 27.9 (55) | 18 (27) | 59.6 (28) | <0.0001 |
| II° ic, % (n) | 34 (67) | 22.7 (34) | 70.2 (33) | <0.0001 |
| Majorβ-angle | 41.4 ± 15.5 | 32.9 ± 8.7 | 50.4 ± 16.2 | <0.0001 |
| Majorα-angle | 30.8 ± 12.4 | 24.6 ± 6.9 | 37.6 ± 13.5 | <0.0001 |
| Major DBT- 5 mm | 151.3 ± 85.9 | 115.4 ± 54.5 | 189.2 ± 97.1 | <0.0001 |
| Major DBT- iso | 89.9 ± 46.9 | 69.8 ± 20.5 | 112 ± 57.1 | <0.0001 |
| Major triangle base/height | 1.2 ± 0.7 | 1.1 ± 0.6 | 1.3 ± 0.7 | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vetta, G.; Parlavecchio, A.; Pistelli, L.; Desalvo, P.; Lo Savio, A.; Magnocavallo, M.; Caminiti, R.; Tribuzio, A.; Vairo, A.; La Maestra, D.; et al. The r’-Wave Algorithm: A New Diagnostic Tool to Predict the Diagnosis of Brugada Syndrome after a Sodium Channel Blocker Provocation Test. Sensors 2023, 23, 3159. https://doi.org/10.3390/s23063159
Vetta G, Parlavecchio A, Pistelli L, Desalvo P, Lo Savio A, Magnocavallo M, Caminiti R, Tribuzio A, Vairo A, La Maestra D, et al. The r’-Wave Algorithm: A New Diagnostic Tool to Predict the Diagnosis of Brugada Syndrome after a Sodium Channel Blocker Provocation Test. Sensors. 2023; 23(6):3159. https://doi.org/10.3390/s23063159
Chicago/Turabian StyleVetta, Giampaolo, Antonio Parlavecchio, Lorenzo Pistelli, Paolo Desalvo, Armando Lo Savio, Michele Magnocavallo, Rodolfo Caminiti, Anna Tribuzio, Alessandro Vairo, Diego La Maestra, and et al. 2023. "The r’-Wave Algorithm: A New Diagnostic Tool to Predict the Diagnosis of Brugada Syndrome after a Sodium Channel Blocker Provocation Test" Sensors 23, no. 6: 3159. https://doi.org/10.3390/s23063159
APA StyleVetta, G., Parlavecchio, A., Pistelli, L., Desalvo, P., Lo Savio, A., Magnocavallo, M., Caminiti, R., Tribuzio, A., Vairo, A., La Maestra, D., Vetta, F., Dattilo, G., Luzza, F., Di Bella, G., Rossini, R., Della Rocca, D. G., & Crea, P. (2023). The r’-Wave Algorithm: A New Diagnostic Tool to Predict the Diagnosis of Brugada Syndrome after a Sodium Channel Blocker Provocation Test. Sensors, 23(6), 3159. https://doi.org/10.3390/s23063159