
Advances in Diagnostic Tools and Therapeutic Approaches for Gliomas: A Comprehensive Review



Abstract
:1. Introduction
2. Diagnostic Tools
2.1. Colorimetric Technique for Brain Cancer Diagnostic: Tumor Markers
2.2. Electrochemical Biosensors for Brain Cancer Diagnosis Using Tumor Biomarkers
2.3. Optical Coherence Tomography
2.4. Surface-Enhanced Raman Spectroscopy
2.5. Reflectometric Interference Spectroscopy
2.6. Optical Biosensors
3. Biotechnology Tools
3.1. Drug Delivery System
3.2. Gene Circuits
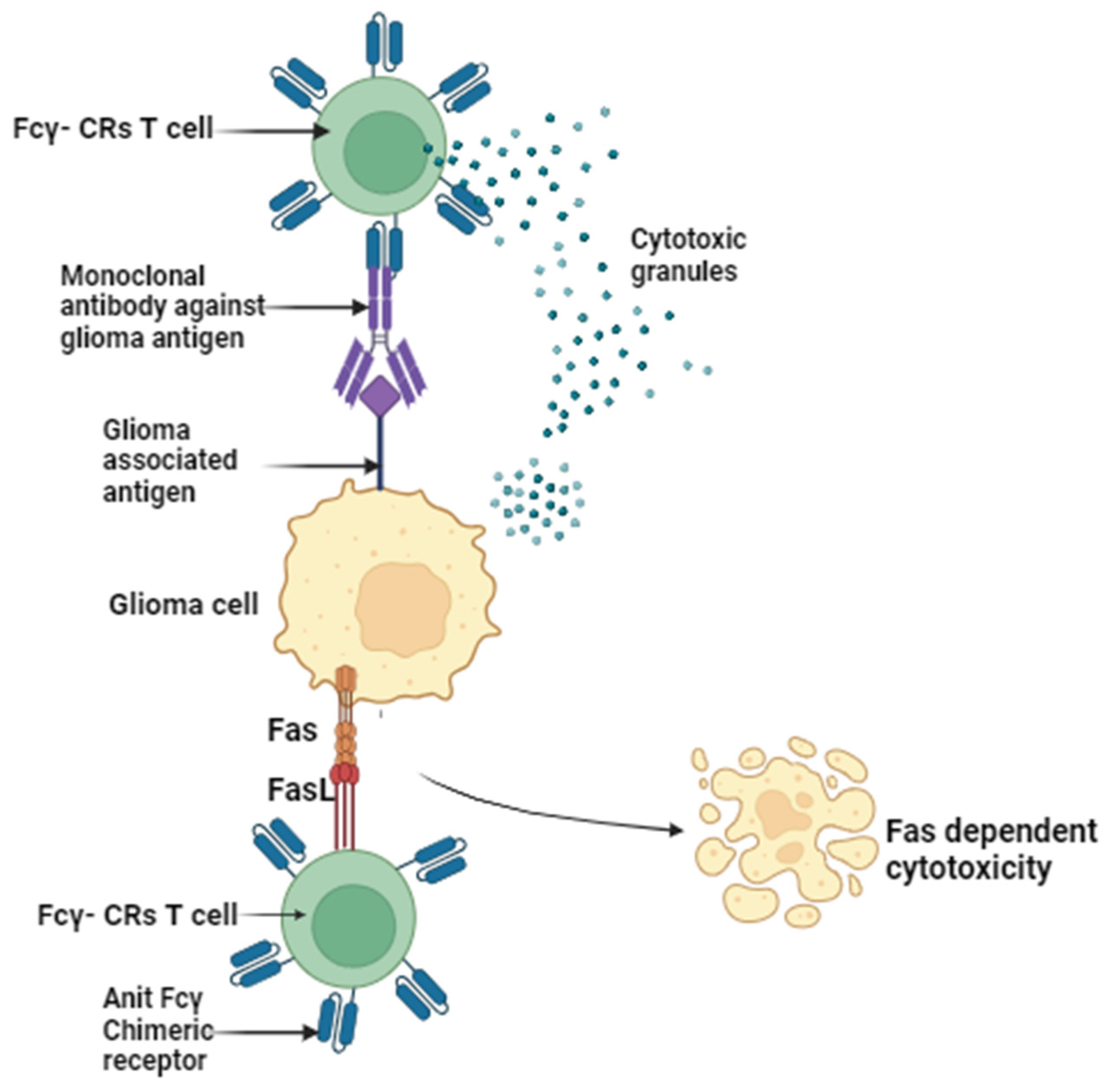
3.3. Fcγ-CR T-Cell Immunotherapy
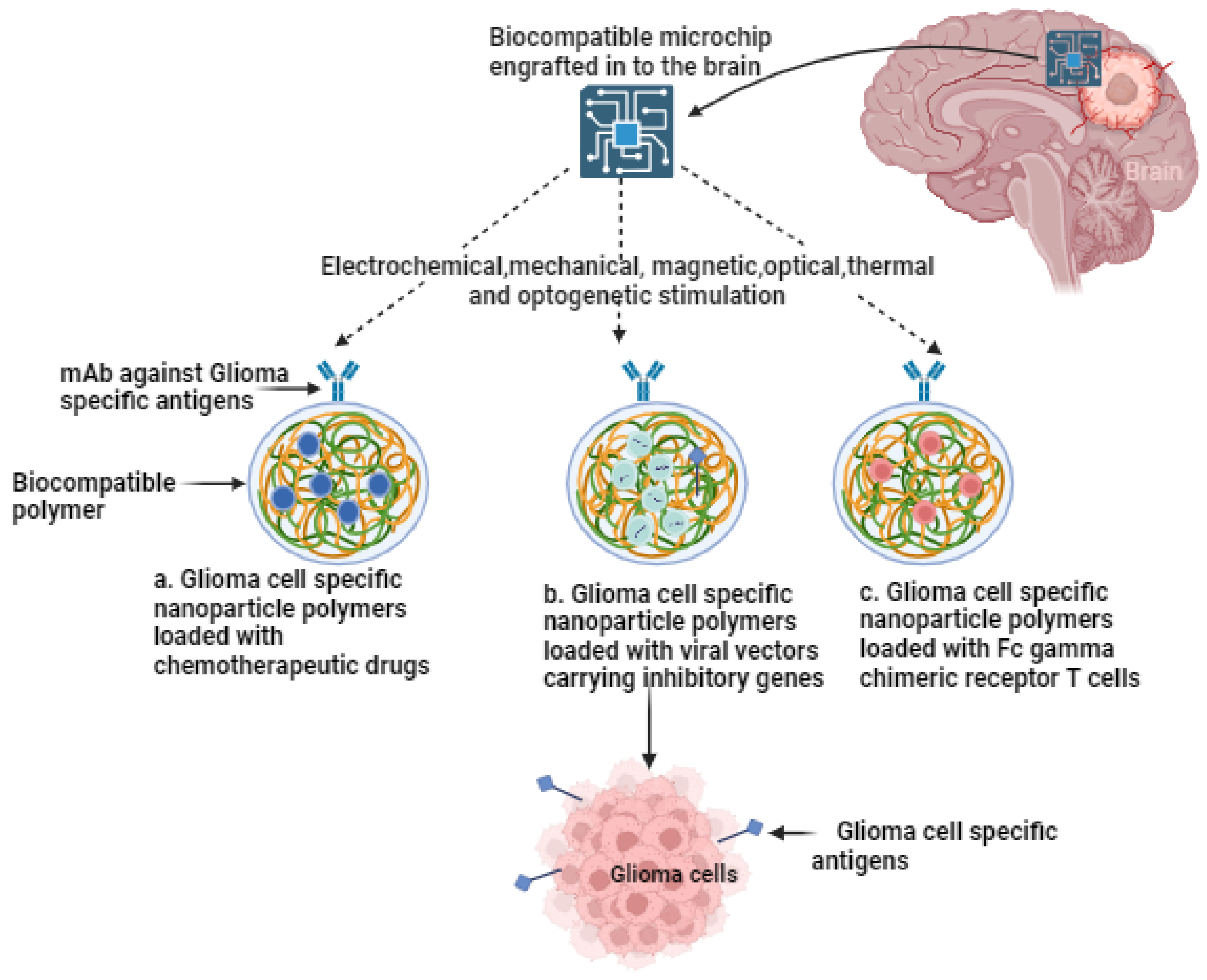
3.4. Targeted Treatment, Cytokine Release Syndrome Management, and Advanced Nanoplatform Systems
4. Bioelectronic Sensors
4.1. Nanomaterials as an Interface for Targeting Gliomas
4.2. Ultraminiaturized, Wirelessly Charged, and Biocompatible Implantable Electronics
4.3. Neuromorphic and Memristive Computing
- Low power consumption: this solution is characterized by low power consumption, ensuring energy efficiency.
- Intrinsic non-volatile memory: the system’s intrinsic non-volatile memory enables the encoding of “artificial synaptic forces”, even in the absence of electrical power, preserving weight and parameter information.
- High scalability: the approach is highly scalable, allowing for the storage of multiple bits within a single device. This scalability enhances the storage density and conserves space, moving closer to the computing power-to-volume ratio observed in mammalian brains.
- Low latency: with fast write and read times, the system achieves very low latency results, resulting in a quicker system response. Additionally, it eliminates the physical separation between the computer and memory unit.
- Minimal electricity consumption: this approach consumes minimal electricity, further enhancing its energy efficiency.
4.4. Multimodal, Multi-Site, and Adaptive in-Brain Glioma Therapeutics
4.5. Microchip Hardware Development
4.6. Cytokine Sensor Development
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, S.; Xu, H.; Zhang, A.; Ni, Y.; Xu, Y.; Meng, T.; Wang, M.; Lou, M. Prognosis Analysis and Validation of m6A Signature and Tumor Immune Microenvironment in Glioma. Front. Oncol. 2020, 10, 541401. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Packer, R.J. The 2021 WHO Classification of Tumors of the Central Nervous System: Clinical Implications. Neuro-oncology 2021, 23, 1215–1217. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, J.P.; Dolecek, T.A.; Horbinski, C.; Ostrom, Q.T.; Lightner, D.D.; Barnholtz-Sloan, J.S.; Villano, J.L. Epidemiologic and Molecular Prognostic Review of Glioblastoma. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 1985–1996. [Google Scholar] [CrossRef] [PubMed]
- Silantyev, A.S.; Falzone, L.; Libra, M.; Gurina, O.I.; Kardashova, K.S.; Nikolouzakis, T.K.; Nosyrev, A.E.; Sutton, C.W.; Mitsias, P.D.; Tsatsakis, A. Current and Future Trends on Diagnosis and Prognosis of Glioblastoma: From Molecular Biology to Proteomics. Cells 2019, 8, 863. [Google Scholar] [CrossRef]
- Koshy, M.; Villano, J.L.; Dolecek, T.A.; Howard, A.; Mahmood, U.; Chmura, S.J.; Weichselbaum, R.R.; McCarthy, B.J. Improved survival time trends for glioblastoma using the SEER 17 population-based registries. J. Neuro-Oncol. 2012, 107, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Lara-Velazquez, M.; Al-Kharboosh, R.; Jeanneret, S.; Vazquez-Ramos, C.; Mahato, D.; Tavanaiepour, D.; Rahmathulla, G.; Quinones-Hinojosa, A. Advances in Brain Tumor Surgery for Glioblastoma in Adults. Brain Sci. 2017, 7, 166. [Google Scholar] [CrossRef]
- Boyd, N.H.; Tran, A.N.; Bernstock, J.D.; Etminan, T.; Jones, A.B.; Gillespie, G.Y.; Friedman, G.K.; Hjelmeland, A.B. Glioma Stem Cells and Their Roles within the Hypoxic Tumor Microenvironment. Theranostics 2021, 11, 665. [Google Scholar] [CrossRef] [PubMed]
- Prager, B.C.; Bhargava, S.; Mahadev, V.; Hubert, C.G.; Rich, J.N. Glioblastoma Stem Cells: Driving Resilience through Chaos. Trends Cancer 2020, 6, 223–235. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, N.; Delbridge, C.; Gempt, J.; Feuchtinger, A.; Walch, A.; Schirmer, L.; Bunk, W.; Aschenbrenner, T.; Liesche-Starnecker, F.; Schlegel, J. The Intratumoral Heterogeneity Reflects the Intertumoral Subtypes of Glioblastoma Multiforme: A Regional Immunohistochemistry Analysis. Front. Oncol. 2020, 10, 494. [Google Scholar] [CrossRef]
- McClellan, B.L.; Haase, S.; Nunez, F.J.; Alghamri, M.S.; Dabaja, A.A.; Lowenstein, P.R.; Castro, M.G. Impact of epigenetic reprogramming on antitumor immune responses in glioma. J. Clin. Investig. 2023, 133, 2. [Google Scholar] [CrossRef]
- Daneman, R.; Prat, A. The blood–brain barrier. Cold Spring Harb. Perspect. Biol. 2015, 7, a020412. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Zepeda, D.; Taghi, M.; Scherrmann, J.M.; Decleves, X.; Menet, M.C. ABC transporters at the blood–brain interfaces, their study models, and drug delivery implications in gliomas. Pharmaceutics 2019, 12, 20. [Google Scholar] [CrossRef] [PubMed]
- Robey, R.W.; Pluchino, K.M.; Hall, M.D.; Fojo, A.T.; Bates, S.E.; Gottesman, M.M. Revisiting the role of ABC transporters in multidrug-resistant cancer. Nat. Rev. Cancer 2018, 18, 452–464. [Google Scholar] [CrossRef]
- Agarwal, S.; Sane, R.; Oberoi, R.; Ohlfest, J.R.; Elmquist, W.F. Delivery of molecularly targeted therapy to malignant glioma, a disease of the whole brain. Expert Rev. Mol. Med. 2011, 13, e17. [Google Scholar] [CrossRef]
- Lim, M.; Xia, Y.; Bettegowda, C.; Weller, M. Current state of immunotherapy for glioblastoma. Nat. Rev. Clin. Oncol. 2018, 15, 422–442. [Google Scholar] [CrossRef]
- Brahm, C.G.; van Linde, M.E.; Enting, R.H.; Schuur, M.; Otten, R.H.; Heymans, M.W.; Verheul, H.M.; Walenkamp, A.M. The current status of immune checkpoint inhibitors in neuro-oncology: A systematic review. Cancers 2020, 12, 586. [Google Scholar] [CrossRef]
- Castillo, M. History and evolution of brain tumor imaging: Insights through radiology. Radiology 2014, 273, S111–S125. [Google Scholar] [CrossRef]
- Liguori, C.; Frauenfelder, G.; Massaroni, C.; Saccomandi, P.; Giurazza, F.; Pitocco, F.; Marano, R.; Schena, E. Emerging clinical applications of computed tomography. Med. Devices Evid. Res. 2015, 8, 265–278. [Google Scholar] [CrossRef]
- Kerr, P.B.; Caputy, A.J.; Horwitz, N.H. A history of cerebral localization. Neurosurg. Focus 2005, 18, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Bernstock, J.D.; Gary, S.E.; Klinger, N.; Valdes, P.A.; Ibn Essayed, W.; Olsen, H.E.; Chagoya, G.; Elsayed, G.; Yamashita, D.; Schuss, P.; et al. Standard clinical approaches and emerging modalities for glioblastoma imaging. Neuro-Oncol. Adv. 2022, 4, vdac080. [Google Scholar] [CrossRef]
- Upadhyay, N.; Waldman, A. Conventional MRI evaluation of gliomas. Br. J. Radiol. 2011, 84, S107–S111. [Google Scholar] [CrossRef] [PubMed]
- Sawlani, V.; Patel, M.D.; Davies, N.; Flintham, R.; Wesolowski, R.; Ughratdar, I.; Pohl, U.; Nagaraju, S.; Petrik, V.; Kay, A.; et al. Multiparametric MRI: Practical approach and pictorial review of a useful tool in the evaluation of brain tumors and tumor-like lesions. Insights Imaging 2020, 11, 84. [Google Scholar] [CrossRef]
- Drake, L.R.; Hillmer, A.T.; Cai, Z. Approaches to PET imaging of glioblastoma. Molecules 2020, 25, 568. [Google Scholar] [CrossRef]
- Verger, A.; Langen, K.J. PET Imaging in glioblastoma: Use in clinical practice. In Glioblastoma; De Vleeschouwer, S., Ed.; Codon Publications: Brisbane, Australia, 2017; pp. 155–174. [Google Scholar] [CrossRef]
- Law, I.; Albert, N.L.; Arbizu, J.; Boellaard, R.; Drzezga, A.; Galldiks, N.; La Fougère, C.; Langen, K.J.; Lopci, E.; Lowe, V.; et al. Joint EANM/EANO/RANO practice guidelines/SNMMI procedure standards for imaging of gliomas using PET with radio-labelled amino acids and [18F] FDG: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 540–557. [Google Scholar] [CrossRef] [PubMed]
- Herrlinger, U.; Tzaridis, T.; Mack, F.; Steinbach, J.P.; Schlegel, U.; Sabel, M.; Hau, P.; Kortmann, R.D.; Krex, D.; Grauer, O.; et al. Lomustine-temozolomide combination therapy versus standard temozolomide therapy in patients with newly diagnosed glioblastoma with methylated MGMT promoter (CeTeG/NOA–09): A randomised, open-label, phase 3 trial. Lancet 2019, 393, 678–688. [Google Scholar] [CrossRef] [PubMed]
- Omuro, A.; Vlahovic, G.; Lim, M.; Sahebjam, S.; Baehring, J.; Cloughesy, T.; Voloschin, A.; Ramkissoon, S.H.; Ligon, K.L.; Latek, R.; et al. Nivolumab with or without ipilimumab in patients with recurrent glioblastoma: Results from exploratory phase I cohorts of CheckMate 143. Neuro-Oncology 2018, 20, 674–686. [Google Scholar] [CrossRef]
- Wen, P.Y.; Stein, A.; van den Bent, M.; De Greve, J.; Wick, A.; de Vos, F.Y.; von Bubnoff, N.; van Linde, M.E.; Lai, A.; Prager, G.W.; et al. Dabrafenib plus trametinib in patients with BRAFV600E-mutant low-grade and high-grade glioma (ROAR): A multicentre, open-label, single-arm, phase 2, basket trial. Lancet Oncol. 2022, 23, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Lassman, A.B.; Wen, P.Y.; van den Bent, M.J.; Plotkin, S.R.; Walenkamp, A.M.; Green, A.L.; Li, K.; Walker, C.J.; Chang, H.; Tamir, S.; et al. A phase II study of the efficacy and safety of oral selinexor in recurrent glioblastoma. Clin. Cancer Res. 2022, 28, 452–460. [Google Scholar] [CrossRef]
- Sonabend, A.M.; Gould, A.; Amidei, C.; Ward, R.; Schmidt, K.A.; Zhang, D.Y.; Gomez, C.; Bebawy, J.F.; Liu, B.P.; Bouchoux, G.; et al. Repeated blood–brain barrier opening with an implantable ultrasound device for delivery of albumin-bound paclitaxel in patients with recurrent glioblastoma: A phase 1 trial. Lancet Oncol. 2023, 24, 509–522. [Google Scholar] [CrossRef]
- Patil, V.M.; Menon, N.; Chatterjee, A.; Tonse, R.; Choudhari, A.; Mahajan, A.; Puranik, A.D.; Epari, S.; Jadhav, M.; Pathak, S.; et al. Mebendazole plus lomustine or temozolomide in patients with recurrent glioblastoma: A randomised open-label phase II trial. eClinicalMedicine 2022, 49, 101449. [Google Scholar] [CrossRef]
- Reardon, D.A.; Brandes, A.A.; Omuro, A.; Mulholland, P.; Lim, M.; Wick, A.; Baehring, J.; Ahluwalia, M.S.; Roth, P.; Bähr, O.; et al. Effect of Nivolumab vs Bevacizumab in Patients with Recurrent Glioblastoma: The CheckMate 143 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Todo, T.; Ino, Y.; Ohtsu, H.; Shibahara, J.; Tanaka, M. A phase I/II study of triple-mutated oncolytic herpes virus G47∆ in patients with progressive glioblastoma. Nat. Commun. 2022, 13, 4119. [Google Scholar] [CrossRef] [PubMed]
- Todo, T.; Ito, H.; Ino, Y.; Ohtsu, H.; Ota, Y.; Shibahara, J.; Tanaka, M. Intratumoral oncolytic herpes virus G47∆ for residual or recurrent glioblastoma: A phase 2 trial. Nat. Med. 2022, 28, 1630–1639. [Google Scholar] [CrossRef]
- Chiocca, E.A.; Gelb, A.B.; Chen, C.C.; Rao, G.; Reardon, D.A.; Wen, P.Y.; Bi, W.L.; Peruzzi, P.; Amidei, C.; Triggs, D.; et al. Combined immunotherapy with controlled interleukin-12 gene therapy and immune checkpoint blockade in recurrent glioblastoma: An open-label, multi-institutional phase I trial. Neuro-Oncology 2022, 24, 951–963. [Google Scholar] [CrossRef]
- Safi, F.; Kohler, I.; Beger, H.G.; Röttinger, E. The value of the tumor marker CA 15-3 in diagnosing and monitoring breast cancer. A comparative study with carcinoembryonic antigen. Cancer 1991, 68, 574–582. [Google Scholar] [CrossRef]
- Yin, Y.; Cao, Y.; Xu, Y.; Li, G. Colorimetric immunoassay for detection of tumor markers. Int. J. Mol. Sci. 2010, 11, 5077–5094. [Google Scholar] [CrossRef]
- McNamara, C.; Mankad, K.; Thust, S.; Dixon, L.; Limback-Stanic, C.; D’Arco, F.; Jacques, T.S.; Löbel, U. 2021 WHO classification of tumours of the central nervous system: A review for the neuroradiologist. Neuroradiology 2022, 64, 1919–1950. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.; Redfield, J.; Ballo, M.; Michael, M.; Sorenson, J.; Dibaba, D.; Wan, J.; Ramos, G.D.; Pandey, M. Identifying the optimal cutoff point for MGMT promoter methylation status in glioblastoma. CNS Oncol. 2021, 10, CNS74. [Google Scholar] [CrossRef]
- Preusser, M.; Charles Janzer, R.; Felsberg, J.; Reifenberger, G.; Hamou, M.F.; Diserens, A.C.; Stupp, R.; Gorlia, T.; Marosi, C.; Heinzl, H.; et al. Anti-O6-methylguanine-methyltransferase (MGMT) immunohistochemistry in glioblastoma multiforme: Observer variability and lack of association with patient survival impede its use as clinical biomarker. Brain Pathol. 2008, 18, 520–532. [Google Scholar] [CrossRef] [PubMed]
- Arita, H.; Narita, Y.; Fukushima, S.; Tateishi, K.; Matsushita, Y.; Yoshida, A.; Miyakita, Y.; Ohno, M.; Collins, V.P.; Kawahara, N.; et al. Upregulating mutations in the TERT promoter commonly occur in adult malignant gliomas and are strongly associated with total 1p19q loss. Acta Neuropathol. 2013, 126, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Liu, Z.; Zhang, X.; Wang, H.; Friedman, G.K.; Ding, Q.; Zhao, X.; Li, H.; Kim, K.; Yu, X.; et al. Generation of chromosome 1p/19q co-deletion by CRISPR/Cas9-guided genomic editing. Neuro-Oncol. Adv. 2022, 4, vdac131. [Google Scholar] [CrossRef] [PubMed]
- Hu, N.; Richards, R.; Jensen, R. Role of chromosomal 1p/19q co-deletion on the prognosis of oligodendrogliomas: A systematic review and meta-analysis. Interdiscip. Neurosurg. 2016, 5, 58–63. [Google Scholar] [CrossRef]
- Qin, T.; McNamara, C.; Mankad, K.; Thust, S.; Dixon, L.; Limback-Stanic, C.; D’Arco, F.; Jacques, T.S.; Löbel, U. ATRX loss in glioma results in dysregulation of cell-cycle phase transition and ATM inhibitor radiosensitization. Cell Rep. 2022, 38, 110216. [Google Scholar] [CrossRef]
- Li, D.; Patel, C.B.; Xu, G.; Iagaru, A.; Zhu, Z.; Zhang, L.; Cheng, Z. Visualization of diagnostic and therapeutic targets in glioma with molecular imaging. Front. Immunol. 2020, 11, 592389. [Google Scholar] [CrossRef]
- Śledzińska, P.; Bebyn, M.G.; Furtak, J.; Kowalewski, J.; Lewandowska, M.A. Prognostic and predictive biomarkers in gliomas. Int. J. Mol. Sci. 2021, 22, 10373. [Google Scholar] [CrossRef]
- Marei, H.E.; Althani, A.; Afifi, N.; Hasan, A.; Caceci, T.; Cifola, I.; Caratelli, S.; Sconocchia, G.; D’Agnano, I.; Cenciarelli, C. Glioma extracellular vesicles for precision medicine: Prognostic and theragnostic application. Discover Oncol. 2022, 13, 49. [Google Scholar] [CrossRef]
- Bagley, S.J.; Nabavizadeh, S.A.; Mays, J.J.; Till, J.E.; Ware, J.B.; Levy, S.; Sarchiapone, W.; Hussain, J.; Prior, T.; Guiry, S.; et al. Clinical utility of plasma cell-free DNA in adult patients with newly diagnosed glioblastoma: A pilot prospective study. Clin. Cancer Res. 2020, 26, 397–407. [Google Scholar] [CrossRef]
- Kang, Y.; Lin, X.; Kang, D. Diagnostic value of circulating tumor DNA in molecular characterization of glioma: A meta-analysis. Medicine 2020, 99, e21196. [Google Scholar] [CrossRef]
- Krol, I.; Castro-Giner, F.; Maurer, M.; Gkountela, S.; Szczerba, B.M.; Scherrer, R.; Coleman, N.; Carreira, S.; Bachmann, F.; Anderson, S.; et al. Detection of circulating tumour cell clusters in human glioblastoma. Br. J. Cancer 2018, 119, 487–491. [Google Scholar] [CrossRef]
- Knecht, M.R.; Sethi, M. Bio-inspired colorimetric detection of Hg2+ and Pb2+ heavy metal ions using Au nanoparticles. Anal. Bioanal. Chem. 2009, 394, 33–46. [Google Scholar] [CrossRef]
- Wu, Y.; Feng, J.; Hu, G.; Zhang, E.; Yu, H.H. Colorimetric Sensors for Chemical and Biological Sensing Applications. Sensors 2023, 23, 2749. [Google Scholar] [CrossRef]
- Suntornsuk, W.; Suntornsuk, L. Recent applications of paper-based point-of-care devices for biomarker detection. Electrophoresis 2020, 41, 287–305. [Google Scholar] [CrossRef]
- Yu, L.; Song, Z.; Peng, J.; Yang, M.; Zhi, H.; He, H. Progress of gold nanomaterials for colorimetric sensing based on different strategies. TrAC Trends Anal. Chem. 2020, 127, 115880. [Google Scholar] [CrossRef]
- Zhou, W.; Gao, X.; Liu, D.; Chen, X. Gold nanoparticles for in vitro diagnostics. Chem. Rev. 2015, 115, 10575–10636. [Google Scholar] [CrossRef]
- Wang, J.; Cao, Y.; Xu, Y.; Li, G. Colorimetric multiplexed immunoassay for sequential detection of tumor markers. Biosens. Bioelectron. 2009, 25, 532–536. [Google Scholar] [CrossRef]
- Lu, W.; Arumugam, S.R.; Senapati, D.; Singh, A.K.; Arbneshi, T.; Khan, S.A.; Yu, H.; Ray, P.C. Multifunctional oval-shaped gold-nanoparticle-based selective detection of breast cancer cells using simple colorimetric and highly sensitive two-photon scattering assay. ACS Nano 2010, 4, 1739–1749. [Google Scholar] [CrossRef]
- Liu, L.; Hao, Y.; Deng, D.; Xia, N. Nanomaterials-based colorimetric immunoassays. Nanomaterials 2019, 9, 316. [Google Scholar] [CrossRef]
- Choate, K.A.; Raack, E.J.; Line, V.F.; Jennings, M.J.; Belton, R.J., Jr.; Winn, R.J.; Mann, P.B. Rapid extraction-free detection of the R132H isocitrate dehydrogenase mutation in glioma using colorimetric peptide nucleic acid-loop mediated isothermal amplification (CPNA-LAMP). PLoS ONE 2023, 18, e0291666. [Google Scholar] [CrossRef]
- Daneshpour, M.; Omidfar, K.; Ghanbarian, H. A novel electrochemical nanobiosensor for the ultrasensitive and specific detection of femtomolar-level gastric cancer biomarker miRNA-106a. Beilstein J. Nanotechnol. 2016, 7, 2023–2036. [Google Scholar] [CrossRef]
- Monsef, R.; Salavati-Niasari, M. Hydrothermal architecture of Cu5V2O10 nanostructures as new electro-sensing catalysts for voltammetric quantification of mefenamic acid in pharmaceuticals and biological samples. Biosens. Bioelectron. 2021, 178, 113017. [Google Scholar] [CrossRef]
- Wang, L.; Yue, X.; Sun, Q.; Zhang, L.; Ren, G.; Lu, G.; Yu, H.-D.; Huang, W. Flexible organic electrochemical transistors for chemical and biological sensing. Nano Res. 2021, 15, 2433–2464. [Google Scholar] [CrossRef]
- Grieshaber, D.; MacKenzie, R.; Vörös, J.; Reimhult, E. Electrochemical biosensors-sensor principles and architectures. Sensors 2008, 8, 1400–1458. [Google Scholar] [CrossRef]
- Hasan, M.R.; Ahommed, M.S.; Daizy, M.; Bacchu, M.S.; Ali, M.R.; Al-Mamun, M.R.; Aly, M.A.; Khan, M.Z.; Hossain, S.I. Recent development in electrochemical biosensors for cancer biomarkers detection. Biosens. Bioelectron. X 2021, 8, 100075. [Google Scholar] [CrossRef]
- Topkaya, S.N.; Azimzadeh, M.; Ozsoz, M. Electrochemical biosensors for cancer biomarkers detection: Recent advances and challenges. Electroanalysis 2016, 28, 1402–1419. [Google Scholar] [CrossRef]
- Chikkaveeraiah, B.V.; Bhirde, A.A.; Morgan, N.Y.; Eden, H.S.; Chen, X. Electrochemical immunosensors for detection of cancer protein biomarkers. ACS Nano 2012, 6, 6546–6561. [Google Scholar] [CrossRef]
- Uygun, Z.O.; Uygun, H.D. A short footnote: Circuit design for faradaic impedimetric sensors and biosensors. Sens. Actuators B Chem. 2014, 202, 448–453. [Google Scholar] [CrossRef]
- Sun, Z.; Wang, L.; Wu, S.; Pan, Y.; Dong, Y.; Zhu, S.; Yang, J.; Yin, Y.; Li, G. An electrochemical biosensor designed by using Zr-based metal–organic frameworks for the detection of glioblastoma-derived exosomes with practical application. Anal. Chem. 2020, 92, 3819–3826. [Google Scholar] [CrossRef]
- Lin, H.Y.; Huang, C.H.; Hsu, P.W.; Lu, Y.J.; Chou, P.C.; Chen, H.C.; Liu, V.Y. INNV-15. Protein Typing and mRNA Analysis of Circulating Exosomes for Glioblastoma Therapy Using Plasmonic-Enhanced Integrated Magneto-Electrochemical Sensor. Neuro-Oncology 2021, 23 (Suppl. S6), vi108. [Google Scholar] [CrossRef]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef]
- Yashin, K.; Bonsanto, M.M.; Achkasova, K.; Zolotova, A.; Wael, A.M.; Kiseleva, E.; Moiseev, A.; Medyanik, I.; Kravets, L.; Huber, R.; et al. OCT-guided surgery for gliomas: Current concept and future perspectives. Diagnostics 2022, 12, 335. [Google Scholar] [CrossRef] [PubMed]
- Falkner-Radler, C.I.; Glittenberg, C.; Gabriel, M.; Binder, S. Intrasurgical microscope-integrated spectral domain optical coherence tomography–assisted membrane peeling. Retina 2015, 35, 2100–2106. [Google Scholar] [CrossRef] [PubMed]
- Yashin, K.S.; Karabut, M.M.; Fedoseeva, V.V.; Khalansky, A.S.; Matveev, L.A.; Elagin, V.V.; Kuznetsov, S.S.; Kiseleva, E.B.; Kravets, L.Y.; Medyanik, I.A.; et al. Multimodal optical coherence tomography in visualization of brain tissue structure at glioblastoma (experimental study). Sovrem. Tekhnologii Meditsine 2016, 8, 73–80. [Google Scholar] [CrossRef]
- Kiseleva, E.B.; Yashin, K.S.; Moiseev, A.A.; Sirotkina, M.A.; Timofeeva, L.B.; Fedoseeva, V.V.; Alekseeva, A.I.; Medyanik, I.A.; Karyakin, N.N.; Kravets, L.Y.; et al. Cross-polarization optical coherent tomography in comparative in vivo and ex vivo studies of optical properties of normal and tumorous brain tissues. Sovrem. Tekhnologii Meditsine 2017, 9, 177–185. [Google Scholar] [CrossRef]
- Kim, J.; Brown, W.; Maher, J.R.; Levinson, H.; Wax, A. Functional optical coherence tomography: Principles and progress. Phys. Med. Biol. 2015, 60, R211. [Google Scholar] [CrossRef]
- Wang, H.; Akkin, T.; Magnain, C.; Wang, R.; Dubb, J.; Kostis, W.J.; Yaseen, M.A.; Cramer, A.; Sakadžić, S.; Boas, D. Polarization sensitive optical coherence microscopy for brain imaging. Opt. Lett. 2016, 41, 2213–2216. [Google Scholar] [CrossRef]
- Li, Y.; Chen, J.; Chen, Z. Advances in Doppler optical coherence tomography and angiography. Transl. Biophotonics 2019, 1, e201900005. [Google Scholar] [CrossRef]
- Strenge, P.; Lange, B.; Draxinger, W.; Grill, C.; Danicke, V.; Theisen-Kunde, D.; Hagel, C.; Spahr-Hess, S.; Bonsanto, M.M.; Handels, H.; et al. Differentiation of different stages of brain tumor infiltration using optical coherence tomography: Comparison of two systems and histology. Front. Oncol. 2022, 12, 896060. [Google Scholar] [CrossRef]
- Han, J.H.; Cha, J. Intraoperative imaging based on common-path time-domain reflectometry for brain tumor surgery. Opt. Appl. 2020, 50, 223–227. [Google Scholar] [CrossRef]
- Assayag, O.; Grieve, K.; Devaux, B.; Harms, F.; Pallud, J.; Chretien, F.; Boccara, C.; Varlet, P. Imaging of non-tumorous and tumorous human brain tissues with full-field optical coherence tomography. NeuroImage Clin. 2013, 2, 549–557. [Google Scholar] [CrossRef]
- Yashin, K.S.; Kiseleva, E.B.; Moiseev, A.A.; Kuznetsov, S.S.; Timofeeva, L.B.; Pavlova, N.P.; Gelikonov, G.V.; Medyanik, I.A.; Kravets, L.Y.; Zagaynova, E.V.; et al. Quantitative nontumorous and tumorous human brain tissue assessment using microstructural co-and cross-polarized optical coherence tomography. Sci. Rep. 2019, 9, 2024. [Google Scholar] [CrossRef]
- Kut, C.; Chaichana, K.L.; Xi, J.; Raza, S.M.; Ye, X.; McVeigh, E.R.; Rodriguez, F.J.; Quiñones-Hinojosa, A.; Li, X. Detection of human brain cancer infiltration ex vivo and in vivo using quantitative optical coherence tomography. Sci. Transl. Med. 2015, 7, 292ra100. [Google Scholar] [CrossRef]
- Böhringer, H.J.; Lankenau, E.; Stellmacher, F.; Reusche, E.; Huettmann, G.; Giese, A. Imaging of human brain tumor tissue by near-infrared laser coherence tomography. Acta Neurochir. 2009, 151, 507–517. [Google Scholar] [CrossRef]
- Yashin, K.S.; Kiseleva, E.B.; Gubarkova, E.V.; Moiseev, A.A.; Kuznetsov, S.S.; Shilyagin, P.A.; Gelikonov, G.V.; Medyanik, I.A.; Kravets, L.Y.; Potapov, A.A.; et al. Cross-polarization optical coherence tomography for brain tumor imaging. Front. Oncol. 2019, 9, 201. [Google Scholar] [CrossRef]
- Achkasova, K.A.; Moiseev, A.A.; Yashin, K.S.; Kiseleva, E.B.; Bederina, E.L.; Loginova, M.M.; Medyanik, I.A.; Gelikonov, G.V.; Zagaynova, E.V.; Gladkova, N.D. Nondestructive label-free detection of peritumoral white matter damage using cross-polarization optical coherence tomography. Front. Oncol. 2023, 13, 1133074. [Google Scholar] [CrossRef]
- Andleeb, F.; Katta, N.; Gruslova, A.; Muralidharan, B.; Estrada, A.; McElroy, A.B.; Ullah, H.; Brenner, A.J.; Milner, T.E. Differentiation of brain tumor microvasculature from normal vessels using optical coherence angiography. Lasers Surg. Med. 2021, 53, 1386–1394. [Google Scholar] [CrossRef]
- Dammers, R.; Schouten, J.W.; Haitsma, I.K.; Vincent, A.J.; Kros, J.M.; Dirven, C.M. Towards improving the safety and diagnostic yield of stereotactic biopsy in a single centre. Acta Neurochir. 2010, 152, 1915–1921. [Google Scholar] [CrossRef]
- Gralla, J.; Nimsky, C.; Buchfelder, M.; Fahlbusch, R.; Ganslandt, O. Frameless stereotactic brain biopsy procedures using the Stealth Station: Indications, accuracy and results. Zentralblatt Neurochir. 2003, 64, 166–170. [Google Scholar] [CrossRef]
- Kiseleva, E.B.; Shilyagin, P.A.; Romashov, V.N.; Korzhimanova, Y.V.; Sirotkina, M.A.; Yashin, K.S.; Zagaynova, E.V.; Gelikonov, G.V.; Gladkova, N.D. Cross-polarization OCT needle probe for combined blood vessels detection and tissue differentiation during stereotactic biopsy of brain tumors. In Proceedings of the European Conference on Biomedical Optics, Munich, Germany, 23–25 June 2019; p. 11079. [Google Scholar] [CrossRef]
- Ramakonar, H.; Quirk, B.C.; Kirk, R.W.; Li, J.; Jacques, A.; Lind, C.R.; McLaughlin, R.A. Intraoperative detection of blood vessels with an imaging needle during neurosurgery in humans. Sci. Adv. 2018, 4, eaav4992. [Google Scholar] [CrossRef]
- Krishnan, R.S.; Shankar, R.K. Raman effect: History of the discovery. J. Raman Spectrosc. 1981, 10, 1–8. [Google Scholar] [CrossRef]
- Wang, X.; Huang, S.C.; Hu, S.; Yan, S.; Ren, B. Fundamental understanding and applications of plasmon-enhanced Raman spectroscopy. Nat. Rev. Phys. 2020, 2, 253–271. [Google Scholar] [CrossRef]
- Auner, G.W.; Koya, S.K.; Huang, C.; Broadbent, B.; Trexler, M.; Auner, Z.; Elias, A.; Mehne, K.C.; Brusatori, M.A. Applications of Raman spectroscopy in cancer diagnosis. Cancer Metastasis Rev. 2018, 37, 691–717. [Google Scholar] [CrossRef] [PubMed]
- Djaker, N.; Gachet, D.; Sandeau, N.; Lenne, P.F.; Rigneault, H. Refractive effects in coherent anti-Stokes Raman scattering microscopy. Appl. Opt. 2006, 45, 7005–7011. [Google Scholar] [CrossRef] [PubMed]
- Verma, P. Tip-enhanced Raman spectroscopy: Technique and recent advances. Chem. Rev. 2017, 117, 6447–6466. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.L.; Li, Q.H.; Ren, B.; Tian, Z.Q. Tunable SERS from aluminium nanohole arrays in the ultraviolet region. Chem. Commun. 2011, 47, 3909–3911. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.R.; Hooper, D.C.; Zhang, L.; Wolverson, D.; Valev, V.K. Raman techniques: Fundamentals and frontiers. Nanoscale Res. Lett. 2019, 14, 231. [Google Scholar] [CrossRef]
- Higa, N.; Akahane, T.; Yokoyama, S.; Yonezawa, H.; Uchida, H.; Takajo, T.; Kirishima, M.; Hamada, T.; Matsuo, K.; Fujio, S.; et al. A tailored next-generation sequencing panel identified distinct subtypes of wildtype IDH and TERT promoter glioblastomas. Cancer Sci. 2020, 111, 3902–3911. [Google Scholar] [CrossRef]
- Xue, H.; Han, Z.; Li, H.; Li, X.; Jia, D.; Qi, M.; Zhang, H.; Zhang, K.; Gong, J.; Wang, H.; et al. Application of intraoperative rapid molecular diagnosis in precision surgery for Glioma: Mimic the World Health Organization CNS5 integrated diagnosis. Neurosurgery 2023, 92, 762–771. [Google Scholar] [CrossRef]
- Sciortino, T.; Secoli, R.; d’Amico, E.; Moccia, S.; Conti Nibali, M.; Gay, L.; Rossi, M.; Pecco, N.; Castellano, A.; De Momi, E.; et al. Raman spectroscopy and machine learning for IDH genotyping of unprocessed glioma biopsies. Cancers 2021, 13, 4196. [Google Scholar] [CrossRef]
- Hu, S.; Kang, H.; Baek, Y.; El Fakhri, G.; Kuang, A.; Choi, H.S. Real-time imaging of brain tumor for image-guided surgery. Adv. Healthc. Mater. 2018, 7, 1800066. [Google Scholar] [CrossRef]
- Karabeber, H.; Huang, R.; Iacono, P.; Samii, J.M.; Pitter, K.; Holland, E.C.; Kircher, M.F. Guiding brain tumor resection using surface-enhanced Raman scattering nanoparticles and a hand-held Raman scanner. ACS Nano 2014, 8, 9755–9766. [Google Scholar] [CrossRef] [PubMed]
- Burgio, F.; Piffaretti, D.; Schmidt, F.; Pieles, U.; Reinert, M.; Ritz, M.F.; Saxer, S. Tuning the Surface Chemistry of Gold Nanoparticles to Specifically Image Glioblastoma Cells Using Surface-Enhanced Raman Spectroscopy. ACS Appl. Nano Mater. 2020, 3, 2447–2454. [Google Scholar] [CrossRef]
- Premachandran, S.; Haldavnekar, R.; Das, S.; Venkatakrishnan, K.; Tan, B. DEEP surveillance of brain cancer using self-functionalized 3D nanoprobes for noninvasive liquid biopsy. ACS Nano 2022, 16, 17948–17964. [Google Scholar] [CrossRef] [PubMed]
- Kircher, M.F.; De La Zerda, A.; Jokerst, J.V.; Zavaleta, C.L.; Kempen, P.J.; Mittra, E.; Pitter, K.; Huang, R.; Campos, C.; Habte, F.; et al. A brain tumor molecular imaging strategy using a new triple-modality MRI-photoacoustic-Raman nanoparticle. Nat. Med. 2012, 18, 829–834. [Google Scholar] [CrossRef]
- Neuschmelting, V.; Harmsen, S.; Beziere, N.; Lockau, H.; Hsu, H.T.; Huang, R.; Razansky, D.; Ntziachristos, V.; Kircher, M.F. Dual-modality surface-enhanced resonance Raman scattering and multispectral optoacoustic tomography nanoparticle approach for brain tumor delineation. Small 2018, 14, 1800740. [Google Scholar] [CrossRef]
- Li, J.; Wang, C.; Yao, Y.; Zhu, Y.; Yan, C.; Zhuge, Q.; Qu, L.; Han, C. Label-free discrimination of glioma brain tumors in different stages by surface enhanced Raman scattering. Talanta 2020, 216, 120983. [Google Scholar] [CrossRef]
- Bury, D.; Morais, C.L.; Ashton, K.M.; Dawson, T.P.; Martin, F.L. Ex vivo Raman spectrochemical analysis using a handheld probe demonstrates high predictive capability of brain tumor status. Biosensors 2019, 9, 49. [Google Scholar] [CrossRef]
- Hollon, T.C.; Pandian, B.; Adapa, A.R.; Urias, E.; Save, A.V.; Khalsa, S.S.S.; Eichberg, D.G.; D’Amico, R.S.; Farooq, Z.U.; Lewis, S.; et al. Near real-time intraoperative brain tumor diagnosis using stimulated Raman histology and deep neural networks. Nat. Med. 2020, 26, 52–58. [Google Scholar] [CrossRef]
- Desroches, J.; Jermyn, M.; Pinto, M.; Picot, F.; Tremblay, M.A.; Obaid, S.; Marple, E.; Urmey, K.; Trudel, D.; Soulez, G.; et al. A new method using Raman spectroscopy for in vivo targeted brain cancer tissue biopsy. Sci. Rep. 2018, 8, 1792. [Google Scholar] [CrossRef]
- Proll, G.; Markovic, G.; Fechner, P.; Proell, F.; Gauglitz, G. Reflectometric interference spectroscopy. In Biosensors Biodetection; Humana Press: New York, NY, USA, 2017; pp. 207–220. [Google Scholar] [CrossRef]
- Diltemiz, S.E.; Yağmuroğlu, O. PARAOKSON TAYİNİNE YÖNELİK REFLEKTOMETRİK GİRİŞİM SPEKTROSKOPİSİ TEMELLİ SENSÖR GELİŞTİRİLMESİ. Eskişehir Tek. Üniversitesi Bilim Teknol. Derg.-C Yaşam Bilim. Biyoteknoloji 2019, 8, 12–22. [Google Scholar]
- De Boer, L.L.; Bydlon, T.M.; Van Duijnhoven, F.; Vranken Peeters, M.J.T.; Loo, C.E.; Winter-Warnars, G.A.; Sanders, J.; Sterenborg, H.J.; Hendriks, B.H.; Ruers, T.J. Towards the use of diffuse reflectance spectroscopy for real-time in vivo detection of breast cancer during surgery. J. Transl. Med. 2018, 16, 367. [Google Scholar] [CrossRef] [PubMed]
- Diltemiz, S.E.; Uslu, O. A reflectometric interferometric nanosensor for sarcosine. Biotechnol. Prog. 2015, 31, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.W.; Sakata, Y.; Kurihara, Y.; Ooya, T.; Takeuchi, T. Label-free detection of C-reactive protein using reflectometric interference spectroscopy-based sensing system. Anal. Chim. Acta 2012, 728, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Kumeria, T.; Parkinson, L.; Losic, D. A nanoporous interferometric microsensor for biomedical detection of volatile sulfur compounds. Nanoscale Res. Lett. 2011, 6, 634. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Wu, Q.; Feng, S.; Zhao, H.; Jin, W.; Qiu, H.; Gu, Y.; Chen, D. In situ detection of human glioma based on tissue optical properties using diffuse reflectance spectroscopy. J. Biophotonics 2023, 16, e202300195. [Google Scholar] [CrossRef] [PubMed]
- Skyrman, S.; Burström, G.; Lai, M.; Manni, F.; Hendriks, B.; Frostell, A.; Edström, E.; Persson, O.; Elmi-Terander, A. Diffuse reflectance spectroscopy sensor to differentiate between glial tumor and healthy brain tissue: A proof-of-concept study. Biomed. Opt. Express 2022, 13, 6470–6483. [Google Scholar] [CrossRef]
- Baria, E.; Pracucci, E.; Pillai, V.; Pavone, F.S.; Ratto, G.M.; Cicchi, R. In vivo detection of murine glioblastoma through Raman and reflectance fiber-probe spectroscopies. Neurophotonics 2020, 7, 045010. [Google Scholar] [CrossRef]
- Hosseinzadeh, M.; Salmani, S.; Ara, M.M. Interferometric optical testing to discriminate benign and malignant brain tumors. J. Photochem. Photobiol. B 2019, 199, 111590. [Google Scholar] [CrossRef]
- Du Le, V.N.; Provias, J.; Murty, N.; Patterson, M.S.; Nie, Z.; Hayward, J.E.; Farrell, T.J.; McMillan, W.; Zhang, W.; Fang, Q. Dual-modality optical biopsy of glioblastomas multiforme with diffuse reflectance and fluorescence: Ex vivo retrieval of optical properties. J. Biomed. Opt. 2017, 22, 027002. [Google Scholar] [CrossRef]
- Singh, A.K.; Mittal, S.; Das, M.; Saharia, A.; Tiwari, M. Optical biosensors: A decade in review. Alex. Eng. J. 2020, 67, 673–691. [Google Scholar] [CrossRef]
- García-Milán, V.; Franco, A.; Zvezdanova, M.E.; Marcos, S.; Martin-Laez, R.; Moreno, F.; Velasquez, C.; Fernandez-Luna, J.L. Discriminating Glioblastoma from Peri-tumoral Tissue by a Nanohole Array-Based Optical and Label-Free Biosensor. Biosensors 2023, 13, 591. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Qiu, L.; Qiao, Y.; Xue, M.; Dong, X.; Meng, Z. Recent advances in sensing applications of molecularly imprinted photonic crystals. Front. Chem. 2021, 9, 665119. [Google Scholar] [CrossRef]
- Nouman, W.M.; Abd El-Ghany, S.E.S.; Sallam, S.M.; Dawood, A.F.B.; Aly, A.H. Biophotonic sensor for rapid detection of brain lesions using 1D photonic crystal. Opt. Quantum Electron. 2020, 52, 287. [Google Scholar] [CrossRef]
- Asuvaran, A.; Elatharasan, G. Design of two-dimensional photonic crystal-based biosensor for abnormal tissue analysis. Silicon 2022, 14, 7203–7210. [Google Scholar] [CrossRef]
- Mohammed, N.A.; Khedr, O.E.; El-Rabaie, E.S.M.; Khalaf, A.A. Brain tumors biomedical sensor with high-quality factor and ultra-compact size based on nanocavity 2D photonic crystal. Alex. Eng. J. 2023, 64, 527–540. [Google Scholar] [CrossRef]
- Morris, M.C. A Toolbox of Fluorescent Peptide Biosensors to Highlight Protein Kinases in Complex Samples: Focus on Cyclin-Dependent Kinases. Eur. J. Org. Chem. 2022, 2022, e202200120. [Google Scholar] [CrossRef]
- Peyressatre, M.; Laure, A.; Pellerano, M.; Boukhaddaoui, H.; Soussi, I.; Morris, M.C. Fluorescent biosensor of CDK5 kinase activity in glioblastoma cell extracts and living cells. Biotechnol. J. 2020, 15, 1900474. [Google Scholar] [CrossRef]
- Karki, K.; Ewing, J.R.; Ali, M.M. Targeting glioma with a dual mode optical and paramagnetic nanoprobe across the blood-brain tumor barrier. J. Nanomed. Nanotechnol. 2016, 7, 395. [Google Scholar] [CrossRef]
- Helmerhorst, E.; Chandler, D.J.; Nussio, M.; Mamotte, C.D. Real-time and label-free bio-sensing of molecular interactions by surface plasmon resonance: A laboratory medicine perspective. Clin. Biochem. Rev. 2012, 33, 161. [Google Scholar]
- Qiu, G.; Thakur, A.; Xu, C.; Ng, S.P.; Lee, Y.; Wu, C.M.L. Detection of Glioma-Derived Exosomes with the Biotinylated Antibody-Functionalized Titanium Nitride Plasmonic Biosensor. Adv. Funct. Mater. 2019, 29, 1806761. [Google Scholar] [CrossRef]
- Martinez-Moro, M.; Jenczyk, J.; Giussi, J.M.; Jurga, S.; Moya, S.E. Kinetics of the Thermal Response of Poly(N-isopropylacrylamide co Methacrylic Acid) Hydrogel Microparticles under Different Environmental Stimuli: A Time-Lapse NMR Study. J. Colloid Interface Sci. 2020, 580, 439–448. [Google Scholar] [CrossRef]
- Brachi, G.; Ruiz-Ramirez, J.; Dogra, P.; Wang, Z.; Cristini, V.; Ciardelli, G.; Rostomily, R.C.; Ferrari, M.; Mikheev, A.M.; Blanco, E.; et al. Intratumoral Injection of Hydrogel-Embedded Nanoparticles Enhances Retention in Glioblastoma. Nanoscale 2020, 12, 23838–23850. [Google Scholar] [CrossRef]
- Xu, B.; Huo, Z.; Huang, H.; Ji, W.; Bian, Z.; Jiao, J.; Sun, J.; Shao, J. The Expression and Prognostic Value of the Epidermal Growth Factor Receptor Family in Glioma. BMC Cancer 2021, 21, 451. [Google Scholar] [CrossRef] [PubMed]
- Christensen, S.C.; Hudecz, D.; Jensen, A.; Christensen, S.; Nielsen, M.S. Basigin Antibodies with Capacity for Drug Delivery Across Brain Endothelial Cells. Mol. Neurobiol. 2021, 58, 4392–4403. [Google Scholar] [CrossRef] [PubMed]
- Suh, S.S.; Yoo, J.Y.; Nuovo, G.J.; Jeon, Y.J.; Kim, S.; Lee, T.J.; Kim, T.; Bakàcs, A.; Alder, H.; Kaur, B.; et al. MicroRNAs/TP53 Feedback Circuitry in Glioblastoma Multiforme. Proc. Natl. Acad. Sci. USA 2012, 109, 5316–5321. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Bertoni, H.; Lal, B.; Michelson, N.; Guerrero-Cázares, H.; Quiñones-Hinojosa, A.; Li, Y.; Laterra, J. Epigenetic Modulation of a miR-296-5p:HMGA1 Axis Regulates Sox2 Expression and Glioblastoma Stem Cells. Oncogene 2016, 35, 4903–4913. [Google Scholar] [CrossRef] [PubMed]
- Ofek, P.; Calderón, M.; Mehrabadi, F.S.; Krivitsky, A.; Ferber, S.; Tiram, G.; Yerushalmi, N.; Kredo-Russo, S.; Grossman, R.; Ram, Z.; et al. Restoring the Oncosuppressor Activity of MicroRNA-34a in Glioblastoma Using a Polyglycerol-Based Polyplex. Nanomed. Nanotechnol. Biol. Med. 2016, 12, 2201–2214. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Liu, Y.; Yang, W.; Han, X.; Li, S.; Liu, H.; Gerweck, L.E.; Fukumura, D.; Leoffler, J.S.; Yang, B.B.; et al. MicroRNA-378 Enhances Radiation Response in Ectopic and Orthotopic Implantation Models of Glioblastoma. J. Neuro-Oncol. 2018, 136, 63–71. [Google Scholar] [CrossRef]
- Shatsberg, Z.; Zhang, X.; Ofek, P.; Malhotra, S.; Krivitsky, A.; Scomparin, A.; Tiram, G.; Calderón, M.; Haag, R.; Satchi-Fainaro, R. Functionalized Nanogels Carrying an Anticancer MicroRNA for Glioblastoma Therapy. J. Control. Release 2016, 239, 159–168. [Google Scholar] [CrossRef]
- Shi, L.; Yuan, Y.; Li, H.Y. MicroRNA-139-3p Suppresses Growth and Metastasis of Glioblastoma via Inhibition of NIN1/RPNI2 Binding Protein 1 Homolog. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 10. [Google Scholar]
- Wang, K.; Kumar, U.S.; Sadeghipour, N.; Massoud, T.F.; Paulmurugan, R. A Microfluidics-Based Scalable Approach to Generate Extracellular Vesicles with Enhanced Therapeutic MicroRNA Loading for Intranasal Delivery to Mouse Glioblastomas. ACS Nano 2021, 15, 18327–18346. [Google Scholar] [CrossRef]
- Nieland, L.; van Solinge, T.S.; Cheah, P.S.; Morsett, L.M.; El Khoury, J.; Rissman, J.I.; Kleinstiver, B.P.; Broekman, M.L.; Breakefield, X.O.; Abels, E.R. CRISPR-Cas Knockout of miR21 Reduces Glioma Growth. Mol. Ther.-Oncolytics 2022, 25, 121–136. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Srivastava, N.; Yadav, A.; Ateeq, B. Targeting AGTR1/NF-κB/CXCR4 Axis by miR-155 Attenuates Oncogenesis in Glioblastoma. Neoplasia 2020, 22, 497–510. [Google Scholar] [CrossRef] [PubMed]
- Zurlo, M.; Romagnoli, R.; Oliva, P.; Gasparello, J.; Finotti, A.; Gambari, R. Synergistic Effects of a Combined Treatment of Glioblastoma U251 Cells with an Anti-miR-10b-5p Molecule and an Anticancer Agent Based on 1-(3′,4′,5′-Trimethoxyphenyl)-2-Aryl-1H-Imidazole Scaffold. Int. J. Mol. Sci. 2022, 23, 5991. [Google Scholar] [CrossRef]
- Wang, L.B.; Karpova, A.; Gritsenko, M.A.; Kyle, J.E.; Cao, S.; Li, Y.; Rykunov, D.; Colaprico, A.; Rothstein, J.H.; Hong, R.; et al. Proteogenomic and Metabolomic Characterization of Human Glioblastoma. Cancer Cell 2021, 39, 509–528.e20. [Google Scholar] [CrossRef] [PubMed]
- Simion, V.; Loussouarn, C.; Laurent, Y.; Roncali, L.; Gosset, D.; Reverchon, F.; Rousseau, A.; Martin, F.; Midoux, P.; Pichon, C.; et al. LentiRILES, a miRNA-ON Sensor System for Monitoring the Functionality of miRNA in Cancer Biology and Therapy. RNA Biol. 2021, 18 (Suppl. 1), 198–214. [Google Scholar] [CrossRef] [PubMed]
- Shah, D.; Comba, A.; Faisal, S.M.; Kadiyala, P.; Baker, G.J.; Alghamri, M.S.; Doherty, R.; Zamler, D.; Nuñez, G.; Castro, M.G.; et al. A Novel miR1983-TLR7-IFNβ Circuit Licenses NK Cells to Kill Glioma Cells, and Is Under the Control of Galectin-1. Oncoimmunology 2021, 10, 1939601. [Google Scholar] [CrossRef]
- Lazutkin, A.; Podgorny, O.; Enikolopov, G. Modes of Division and Differentiation of Neural Stem Cells. Behav. Brain Res. 2019, 374, 112118. [Google Scholar] [CrossRef] [PubMed]
- Marei, H.E.; Althani, A.; Afifi, N.; Hasan, A.; Caceci, T.; Pozzoli, G.; Cenciarelli, C. Current Progress in Chimeric Antigen Receptor T Cell Therapy for Glioblastoma Multiforme. Cancer Med. 2021, 10, 5019–5030. [Google Scholar] [CrossRef]
- Cenciarelli, C.; Caratelli, S.; Arriga, R.; Lanzilli, G.; Ottaviani, A.; Sconocchia, T.; Spagnoli, G.C.; Venditti, A.; Iezzi, G.; Roselli, M.; et al. EGFR+ Glioblastoma Stem Cells Targeting by CD16158V-Chimeric Receptor T Cells and Cetuximab. J. Res. 2021, 1, 24–35. [Google Scholar] [CrossRef]
- Clémenceau, B.; Congy-Jolivet, N.; Gallot, G.; Vivien, R.; Gaschet, J.; Thibault, G.; Vié, H. Antibody-Dependent Cellular Cytotoxicity (ADCC) Is Mediated by Genetically Modified Antigen-Specific Human T Lymphocytes. Blood 2006, 107, 4669–4677. [Google Scholar] [CrossRef] [PubMed]
- Caratelli, S.; Arriga, R.; Sconocchia, T.; Ottaviani, A.; Lanzilli, G.; Pastore, D.; Cenciarelli, C.; Venditti, A.; Del Principe, M.I.; Lauro, D.; et al. In Vitro Elimination of Epidermal Growth Factor Receptor-Overexpressing Cancer Cells by CD32A-Chimeric Receptor T Cells in Combination with Cetuximab or Panitumumab. Int. J. Cancer 2020, 146, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Däster, S.; Eppenberger-Castori, S.; Hirt, C.; Soysal, S.D.; Delko, T.; Nebiker, C.A.; Weixler, B.; Amicarella, F.; Iezzi, G.; Governa, V.; et al. Absence of Myeloperoxidase and CD8 Positive Cells in Colorectal Cancer Infiltrates Identifies Patients with Severe Prognosis. Oncoimmunology 2015, 4, e1050574. [Google Scholar] [CrossRef] [PubMed]
- Caratelli, S.; Sconocchia, T.; Arriga, R.; Coppola, A.; Lanzilli, G.; Lauro, D.; Venditti, A.; Del Principe, M.I.; Buccisano, F.; Maurillo, L.; et al. FCγ Chimeric Receptor-Engineered T Cells: Methodology, Advantages, Limitations, and Clinical Relevance. Front. Immunol. 2017, 8, 457. [Google Scholar] [CrossRef]
- Sconocchia, G.; Zlobec, I.; Lugli, A.; Calabrese, D.; Iezzi, G.; Karamitopoulou, E.; Patsouris, E.S.; Peros, G.; Horcic, M.; Tornillo, L.; et al. Tumor Infiltration by FcγRIII (CD16)+ Myeloid Cells Is Associated with Improved Survival in Patients with Colorectal Carcinoma. Int. J. Cancer 2011, 128, 2663–2672. [Google Scholar] [CrossRef]
- Murthy, H.; Iqbal, M.; Chavez, J.C.; Kharfan-Dabaja, M.A. Cytokine Release Syndrome: Current Perspectives. ImmunoTargets Ther. 2019, 2019, 43–52. [Google Scholar] [CrossRef]
- Janjua, T.I.; Rewatkar, P.; Ahmed-Cox, A.; Saeed, I.; Mansfeld, F.M.; Kulshreshtha, R.; Kumeria, T.; Ziegler, D.S.; Kavallaris, M.; Mazzieri, R.; et al. Frontiers in the Treatment of Glioblastoma: Past, Present and Emerging. Adv. Drug Deliv. Rev. 2021, 171, 108–138. [Google Scholar] [CrossRef]
- Gonçalves, A.; Machado, R.; Gomes, A.C.; Costa, A.D. Nanotechnology Solutions for Controlled Cytokine Delivery: An Applied Perspective. Appl. Sci. 2020, 10, 7098. [Google Scholar] [CrossRef]
- Barzegar Behrooz, A.; Talaie, Z.; Syahir, A. Nanotechnology-Based Combinatorial Anti-Glioblastoma Therapies: Moving from Terminal to Treatable. Pharmaceutics 2022, 14, 1697. [Google Scholar] [CrossRef]
- Zhao, S.; Caruso, F.; Dähne, L.; Decher, G.; De Geest, B.G.; Fan, J.; Feliu, N.; Gogotsi, Y.; Hammond, P.T.; Hersam, M.C.; et al. The future of layer-by-layer assembly: A tribute to ACS Nano associate editor Helmuth Mohwald. ACS Nano 2019, 13, 6151–6169. [Google Scholar] [CrossRef]
- Deisseroth, K.; Hegemann, P. The form and function of channelrhodopsin. Science 2017, 357, eaan5544. [Google Scholar] [CrossRef]
- Signorelli, L.; Hescham, S.A.; Pralle, A.; Gregurec, D. Magnetic nano-materials for wireless thermal and mechanical neuromodulation. iScience 2022, 25, 105401. [Google Scholar] [CrossRef]
- Rajagopal, P.; Duraiswamy, S.; Sethuraman, S.; Giridhara Rao, J.; Krishnan, U.M. Polymer-coated viral vectors: Hybrid nanosystems for gene therapy. J. Gene Med. 2018, 20, e3011. [Google Scholar] [CrossRef]
- Burke, R.C.; Bardet, S.M.; Carr, L.; Romanenko, S.; Arnaud-Cormos, D.; Leveque, P.; O’Connor, R.P. Nanosecond pulsed electric fields depolarize transmembrane potential via voltage-gated K+, Ca2+ and TRPM8 channels in U87 glioblastoma cells. Biochim. Biophys. Acta (BBA)—Biomembr. 2017, 1859, 2040–2050. [Google Scholar] [CrossRef]
- Gregurec, D.; Senko, A.W.; Chuvilin, A.; Reddy, P.D.; Sankararaman, A.; Rosenfeld, D.; Chiang, P.H.; Garcia, F.; Tafel, I.; Varnavides, G.; et al. Magnetic vortex nanodiscs enable remote magnetomechanical neural stimulation. ACS Nano 2020, 14, 8036–8045. [Google Scholar] [CrossRef]
- Richardson, H.H.; Carlson, M.T.; Tandler, P.J.; Hernandez, P.; Govorov, A.O. Experimental and Theoretical Studies of Light-to-Heat Conversion and Collective Heating Effects in Metal Nanoparticle Solutions. Nano Lett. 2009, 9, 1139–1146. [Google Scholar] [CrossRef]
- Sharma, A.; Rao, V.K. Synthetic Applications of Gold Nanoparticles in Research Advancement of Electrochemical Immunosensors. Trends Appl. Sci. Res. 2020, 15, 151–167. [Google Scholar] [CrossRef]
- Frtús, A.; Smolková, B.; Uzhytchak, M.; Lunova, M.; Jirsa, M.; Kubinová, Š.; Dejneka, A.; Lunov, O. Analyzing the mechanisms of iron oxide nanoparticles interactions with cells: A road from failure to success in clinical applications. J. Control. Release 2020, 328, 59–77. [Google Scholar] [CrossRef] [PubMed]
- Minudri, D.; Mantione, D.; Dominguez-Alfaro, A.; Moya, S.; Maza, E.; Bellacanzone, C.; Antognazza, M.R.; Mecerreyes, D. Water-soluble cationic poly(3,4-ethylenedioxythiophene) PEDOT-N as a versatile conducting polymer for bioelectronics. Adv. Electron. Mater. 2020, 6, 2000510. [Google Scholar] [CrossRef]
- Ma, X.; Wang, M.; Ran, Y.; Wu, Y.; Wang, J.; Gao, F.; Liu, Z.; Xi, J.; Ye, L.; Feng, Z. Design and fabrication of polymeric hydrogel carrier for nerve repair. Polymers 2022, 14, 1549. [Google Scholar] [CrossRef]
- Cheong, G.M.; Lim, K.S.; Jakubowicz, A.; Martens, P.J.; Poole-Warren, L.A.; Green, R.A. Conductive hydrogels with tailored bioactivity for implantable electrode coatings. Acta Biomater. 2014, 10, 1216–1226. [Google Scholar] [CrossRef]
- Ahmed, E.M. Hydrogel: Preparation, Characterization, and Applications: A Review. J. Adv. Res. 2015, 6, 105–121. [Google Scholar] [CrossRef]
- Yang, Y.; Wu, M.; Vázquez-Guardado, A.; Wegener, A.J.; Grajales-Reyes, J.G.; Deng, Y.; Wang, T.; Avila, R.; Moreno, J.A.; Minkowicz, S.; et al. Wireless multilateral devices for optogenetic studies of individual and social behaviors. Nat. Neurosci. 2021, 24, 1035–1045. [Google Scholar] [CrossRef]
- Li, Y.; Li, N.; De Oliveira, N.; Wang, S. Implantable bioelectronics toward long-term stability and sustainability. Matter 2021, 4, 1125–1141. [Google Scholar] [CrossRef]
- Zhou, Y.; Liu, C.; Huang, Y. Wireless Power Transfer for Implanted Medical Application: A Review. Energies 2020, 13, 2837. [Google Scholar] [CrossRef]
- Peruzzi, P.; Dominas, C.; Fell, G.; Bernstock, J.D.; Blitz, S.; Mazzetti, D.; Zdioruk, M.; Dawood, H.Y.; Triggs, D.V.; Ahn, S.W.; et al. Intratumoral Drug-Releasing Microdevices Allow In Situ High-Throughput Pharmaco Phenotyping in Patients with Gliomas. Sci. Transl. Med. 2023, 15, eadi0069. [Google Scholar] [CrossRef]
- Milo, V.; Malavena, G.; Monzio Compagnoni, C.; Ielmini, D. Memristive and CMOS Devices for Neuromorphic Computing. Materials 2020, 13, 166. [Google Scholar] [CrossRef]
- Mohanty, S.P.; Srivastava, A. Nano-CMOS and Post-CMOS Electronics: Devices and Modelling; IET: London, UK, 2016. [Google Scholar]
- Pham, M.D.; D’Angiulli, A.; Dehnavi, M.M.; Chhabra, R. From Brain Models to Robotic Embodied Cognition: How Does Biological Plausibility Inform Neuromorphic Systems? Brain Sci. 2023, 13, 1316. [Google Scholar] [CrossRef]
- Trensch, G.; Morrison, A. A System-on-Chip Based Hybrid Neuromorphic Compute Node Architecture for Reproducible Hyper-Real-Time Simulations of Spiking Neural Networks. Front. Neuroinform. 2022, 16, 884033. [Google Scholar] [CrossRef]
- Yang, D.; Shin, Y.I.; Hong, K.S. Systemic Review on Transcranial Electrical Stimulation Parameters and EEG/fNIRS Features for Brain Diseases. Front. Neurosci. 2021, 15, 629323. [Google Scholar] [CrossRef]
- Wang, C.; He, T.; Zhou, H.; Zhang, Z.; Lee, C. Artificial Intelligence Enhanced Sensors-Enabling Technologies to Next-Generation Healthcare and Biomedical Platform. Bioelectron. Med. 2023, 9, 17. [Google Scholar] [CrossRef]
- Gilbert, F.; Dodds, S. Is There Anything Wrong with Using AI Implantable Brain Devices to Prevent Convicted Offenders from Reoffending? In Neurointerventions and the Law: Regulating Human Mental Capacity; Vincent, N.A., Nadelhoffer, T., McCay, A., Eds.; Oxford University Press: Oxford, UK, 2020. [Google Scholar]
- Govindan, B.; Sabri, M.A.; Hai, A.; Banat, F.; Haija, M.A. A Review of Advanced Multifunctional Magnetic Nanostructures for Cancer Diagnosis and Therapy Integrated into an Artificial Intelligence Approach. Pharmaceutics 2023, 15, 868. [Google Scholar] [CrossRef]
- Stadtmauer, E.A.; Fraietta, J.A.; Davis, M.M.; Cohen, A.D.; Weber, K.L.; Lancaster, E.; Mangan, P.A.; Kulikovskaya, I.; Gupta, M.; Chen, F.; et al. CRISPR-Engineered T Cells in Patients with Refractory Cancer. Science 2020, 367, eaba7365. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | Phase | Concentration/Dose | Sample Size | Result | Country | Year | Reference |
|---|---|---|---|---|---|---|---|
| Lomustine (CCNU)–temozolomide (TMZ) combination therapy vs. standard temozolomide | Phase III Open-label, randomized NCT01149109 | Standard TMZ chemoradiotherapy: TMZ: 75 mg/m2 per day; Radiotherapy (59–60 Gy); Followed by six courses TMZ: Dose: 150–200 mg/m2 per day. Combination therapy (TMZ+CCNU): CCNU: 100 mg/m2 on day 1; TMZ: 100–200 mg/m2 per day; In addition to radiotherapy (59–60 Gy). | 141 patients: TMZ: 63 TMZ+CCNU: 66 |
TMZ+CCNU: 48.1 months.
| Germany | 2011–2014 | [27] |
| Nivolumab monotherapy (NIVO) and combination with ipilimumab (IPI) for recurrent glioblastomas | Phase I NCT02017717 | NIVO monotherapy (NIVO3): 3 mg/kg; Every 2 weeks. Combination therapy (NIVO1+IPI3): 1 mg/kg + 3 mg/kg; Every 3 weeks for 4 doses. Alternative combination therapy (NIVO3+IPI1): 3 mg/kg+1 mg/kg; Every 3 weeks for 4 doses. | 40 patients: NIVO3: n = 10; NIVO1+IPI3: n = 10; NIVO3+IPI1: n = 20. |
| USA | 2017 | [28] |
| Dabrafenib and trametinib combination therapy in patients with BRAFV600E-mutant low-grade and high-grade gliomas | Phase II Basket trial Open-label, single-arm NCT02034110 | Dabrafenib: 150 mg twice daily orally. Trametinib: 2 mg once daily orally. | 45 patients: 31-high-grade glioma cohort; 13-low-grade glioma cohort. |
| Part of an ongoing study, basket trial including 13 countries: Austria, Belgium, Canada, France, Germany, Italy, Japan, Netherlands, Norway, Republic of Korea, Spain, Sweden, and USA. | 2014–2018 | [29] |
| Selinexor monotherapy in recurrent glioblastomas | Phase II open-label study NCT01986348 | Arm A (Pre-surgical selinexor): 3 preoperative selinexor doses. Median selinexor concentration in resected tumors: 105.4 nmol/L. Arms B, C, and D (post-operative selinexor): Arm B: selinexor 50 mg/m2 twice weekly. Arm C: selinexor 60 mg twice weekly. Arm D: selinexor 80 mg once weekly. | 76 patients: Arm A: 8; Arm B: 24; Arm C: 14; Arm D: 30. |
Arm C: 7.7%; Arm D: 17.2%.
varied from 7.7% to 10% across arms.
| USA; Denmark; Netherlands. | 2020 | [30] |
| Repetitive blood–brain barrier opening via implantable ultrasound device for albumin-bound paclitaxel delivery in recurrent glioblastomas | Phase I | Low-intensity pulsed ultrasound with concomitant intravenous microbubbles (LIPU-MBs) with intravenous albumin-bound paclitaxel infusion. Frequency: every 3 weeks. Duration: up to six cycles. Dose escalation: Six dose levels of albumin-bound paclitaxel were evaluated: 40 mg/m2; 80 mg/m2; 135 mg/m2; 175 mg/m2; 215 mg/m2; 260 mg/m2. Primary endpoint: The evaluation of the dose-limiting toxicity during the first cycle of sonication and chemotherapy | 17 patients |
| USA | 2020–2022 | [31] |
| Mebendazole (MBZ) combination therapy with lomustine (CCNU) or temozolomide (TMZ) in recurrent glioblastomas | Phase II Randomized open-label trial CTRI/2018/01/011542 | CCNU+MBZ (mebendazole) arm: CCNU: 110 mg/m2 every 6 weeks; MBZ: 800 mg thrice daily. TMZ+MBZ arm: TMZ: 200 mg/m2 once daily on days 1–5 of a 28-day cycle; MBZ: 1600 mg thrice daily. | 44 patients randomized in each arm |
| India | 2019–2021 | [32] |
| Nivolumab vs. bevacizumab in patients with recurrent glioblastomas | Phase III Randomized open-label trial NCT02017717 | Nivolumab: 3 mg/kg every 2 weeks; Bevacizumab: 10 mg/kg every 2 weeks. | 369 patients: nivolumab: 184; bevacizumab: 185. |
| 12 countries: USA; Australia; Belgium; Denmark; France; Germany; Italy; Netherlands; Poland; Spain; Switzerland; UK. | 2014–2015 | [33] |
| Triple-mutated oncolytic herpes virus G47∆ in patients with progressive glioblastomas | Phase I/II UMIN000002661 | Cohort 1: G47Δ of 3 × 108 pfu (total of 6 × 108 pfu). Cohort 2 and the phase II part: G47Δ at a dose of 1 × 109 pfu (total of 2 × 109 pfu). Administration protocol: Total volume: 1 mL. G47∆ injected into two different sites. Each site received 0.5 mL. | 13 patients: Cohort 1: 3; Cohort 2 and the phase II part: 10. |
| Japan | 2009–2014 | [34] |
| Intratumoral oncolytic herpes virus G47∆ for residual or recurrent glioblastomas | Phase II Single-arm trial UMIN000015995 | G47∆ administered intratumorally First and second doses: 5–14-day intervals; Third and subsequent doses: up to six doses at 4 ± 2-week intervals; Dosage: 1 × 109 pfu per dose in a 1 mL solution. | 30 patients | Primary endpoint (1-year survival rate): 84.2% (95% CI, 60.4–96.6). Secondary endpoints: median overall survival: 20.2 months after G47∆ initiation; 28.8 months from initial surgery. Enlargement and contrast-enhancement clearing in the target lesion after each G47∆ administration. Increase in tumor-infiltrating CD4+/CD8+ lymphocytes. Persistent low numbers of Foxp3+ cells. Demonstrated survival benefit. Good safety profile. Led to the approval of G47∆ as the first oncolytic virus product in Japan. | Japan | 2015–2018 | [35] |
| Combined immunotherapy with controlled interleukin-12 gene therapy and immune checkpoint blockade in recurrent glioblastomas (rGBMs) | Phase I trial, open-label, multi-institutional, dose-escalation NCT03636477 | Nivolumab administration: 7 (±3) days before the resection of the rGBM Ongoing every 2 weeks after surgery. Dosages in cohorts: 1 mg/kg; 3 mg/kg. VDX administration: 3 h before surgery Continued for 14 days after surgery. Dosages in cohorts: 10 mg; 20 mg. IL-12 gene therapy: Peritumoral injection after the resection of the rGBM. | 21 patients | VDX 10 mg with nivolumab: 16.9 months. For all subjects: 9.8 months. Controlled IL-12 gene therapy with nivolumab was safe in recurrent GBM patients. This combination immunotherapy increased tumor IFNγ, suggesting immune activation. The safety of combining immunotherapy was confirmed, prompting the initiation of a Phase II clinical trial (NCT04006119). | USA | 2018–2019 | [36] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thenuwara, G.; Curtin, J.; Tian, F. Advances in Diagnostic Tools and Therapeutic Approaches for Gliomas: A Comprehensive Review. Sensors 2023, 23, 9842. https://doi.org/10.3390/s23249842
Thenuwara G, Curtin J, Tian F. Advances in Diagnostic Tools and Therapeutic Approaches for Gliomas: A Comprehensive Review. Sensors. 2023; 23(24):9842. https://doi.org/10.3390/s23249842
Chicago/Turabian StyleThenuwara, Gayathree, James Curtin, and Furong Tian. 2023. "Advances in Diagnostic Tools and Therapeutic Approaches for Gliomas: A Comprehensive Review" Sensors 23, no. 24: 9842. https://doi.org/10.3390/s23249842
APA StyleThenuwara, G., Curtin, J., & Tian, F. (2023). Advances in Diagnostic Tools and Therapeutic Approaches for Gliomas: A Comprehensive Review. Sensors, 23(24), 9842. https://doi.org/10.3390/s23249842