
An Exploration of Tri-Axial Accelerometers in Assessing the Therapeutic Efficacy of Constraint-Induced Movement Therapy in Children with Unilateral Cerebral Palsy


Abstract
:1. Introduction
2. Materials and Methods
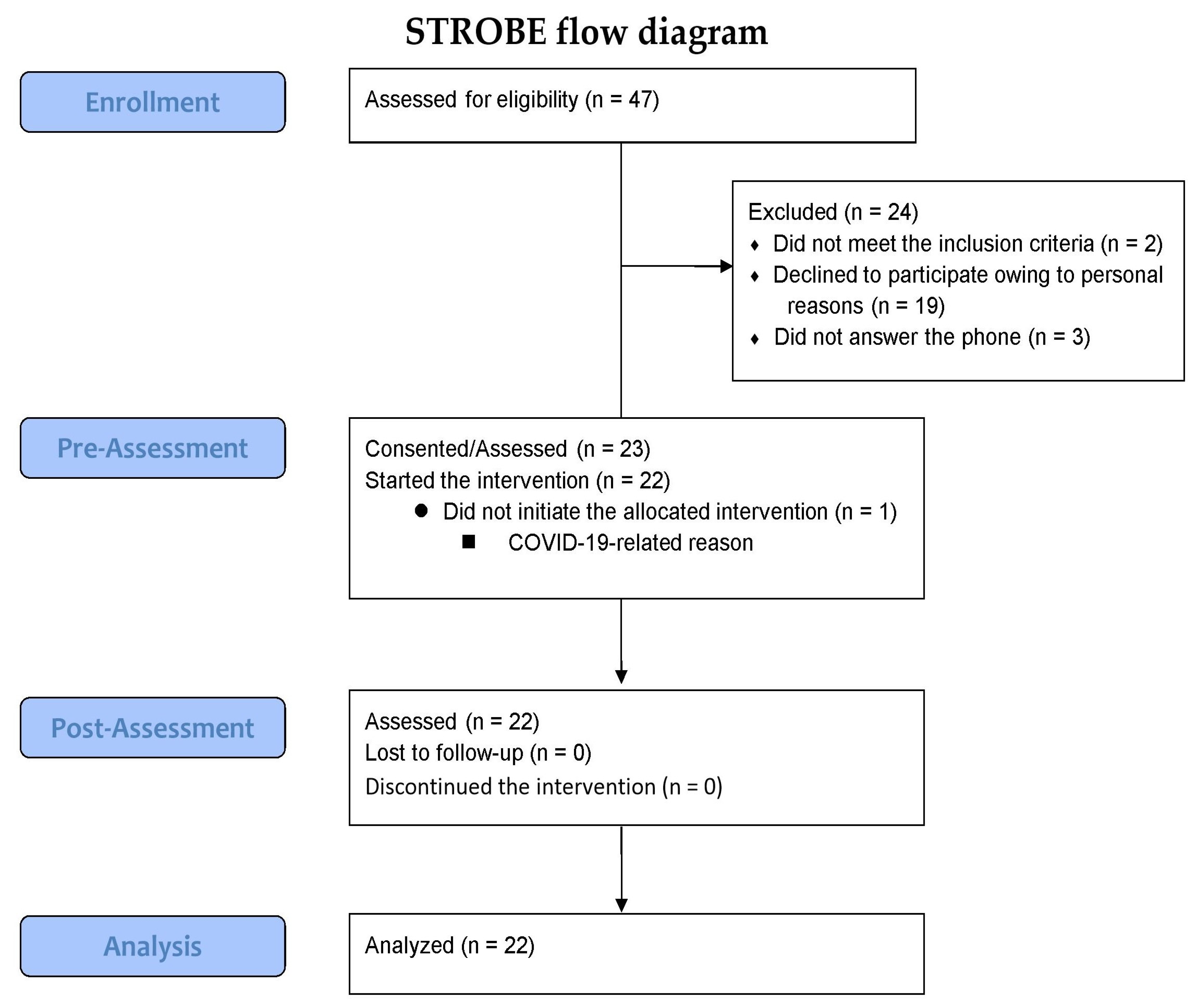
2.1. Study Design and Population
2.2. Procedure
2.3. Physical Activity Monitoring Using Accelerometer-Based Monitors
2.4. In-Laboratory Standardized Assessments
2.5. Statistical Analyses
3. Results
3.1. Correlation Analysis of Actigraphy Changes over the CIMT Sessions (ΔWeek3–Week1) with Pre-Post Differences in the Standardized Assessments (ΔT1–T0)
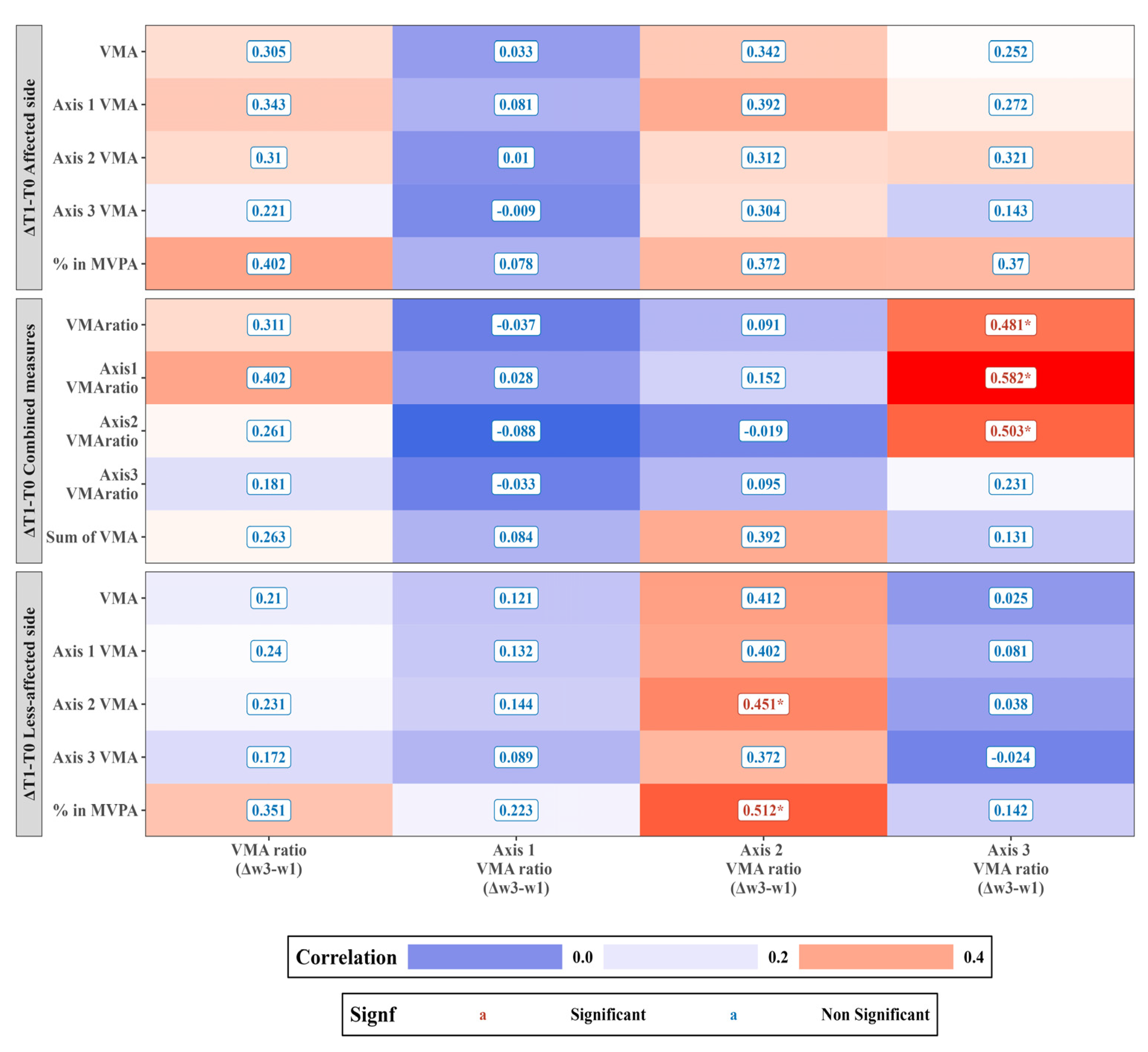
3.2. Correlations of Daily Life Actigraphy Alterations (ΔT1–T0) with Changes Observed over the CIMT Sessions (ΔWeek3–Week1) in a Clinical Setting
3.3. Comparison of the Vector Magnitude Average Counts (VMA) between the Baseline (T0) and Post-Intervention Time Point (T1)
3.4. Weekly Actigraphy Trends across the Three-Week CIMT Duration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stavsky, M.; Mor, O.; Mastrolia, S.A.; Greenbaum, S.; Than, N.G.; Erez, O. Cerebral palsy-trends in epidemiology and recent development in prenatal mechanisms of disease, treatment, and prevention. Front. Pediatr. 2017, 5, 21. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. Suppl. 2007, 109, 8–14. [Google Scholar] [PubMed]
- Odding, E.; Roebroeck, M.E.; Stam, H.J. The epidemiology of cerebral palsy: Incidence, impairments and risk factors. Disabil. Rehabil. 2006, 28, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.L.; Walter, S.D.; Hanna, S.E.; Palisano, R.J.; Russell, D.J.; Raina, P.; Wood, E.; Bartlett, D.J.; Galuppi, B.E. Prognosis for gross motor function in cerebral palsy: Creation of motor development curves. JAMA 2002, 288, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Cioni, G.; Sgandurra, G.; Muzzini, S.; Paolicelli, P.B.; Ferrari, A. Forms of hemiplegia. In The Spastic Forms of Cerebral Palsy: A Guide to the Assessment of Adaptive Functions; Cioni, G., Ferrari, A., Eds.; Springer: Milano, Italy, 2010; pp. 331–356. [Google Scholar]
- Novak, I.; Morgan, C.; Adde, L.; Blackman, J.; Boyd, R.N.; Brunstrom-Hernandez, J.; Cioni, G.; Damiano, D.; Darrah, J.; Eliasson, A.C.; et al. Early, accurate diagnosis and early intervention in cerebral palsy: Advances in diagnosis and treatment. JAMA Pediatr. 2017, 171, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Mailleux, L.; Jaspers, E.; Ortibus, E.; Simon-Martinez, C.; Desloovere, K.; Molenaers, G.; Klingels, K.; Feys, H. Clinical assessment and three-dimensional movement analysis: An integrated approach for upper limb evaluation in children with unilateral cerebral palsy. PLoS ONE 2017, 12, e0180196. [Google Scholar] [CrossRef] [PubMed]
- Taub, E.; Ramey, S.L.; DeLuca, S.; Echols, K. Efficacy of constraint-induced movement therapy for children with cerebral palsy with asymmetric motor impairment. Pediatrics 2004, 113, 305–312. [Google Scholar] [CrossRef]
- Gerber, C.N.; Plebani, A.; Labruyère, R. Translation, reliability, and clinical utility of the Melbourne assessment 2. Disabil. Rehabil. 2019, 41, 226–234. [Google Scholar] [CrossRef]
- Davids, J.R.; Peace, L.C.; Wagner, L.V.; Gidewall, M.A.; Blackhurst, D.W.; Roberson, W.M. Validation of the Shriners Hospital for Children upper extremity evaluation (SHUEE) for children with hemiplegic cerebral palsy. J. Bone Jt. Surg. Am. 2006, 88, 326–333. [Google Scholar] [CrossRef]
- Thorley, M.; Lannin, N.; Cusick, A.; Novak, I.; Boyd, R. Construct validity of the quality of upper extremity skills test for children with cerebral palsy. Dev. Med. Child Neurol. 2012, 54, 1037–1043. [Google Scholar] [CrossRef]
- Krumlinde-Sundholm, L.; Holmefur, M.; Kottorp, A.; Eliasson, A.C. The assisting hand assessment: Current evidence of validity, reliability, and responsiveness to change. Dev. Med. Child Neurol. 2007, 49, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Arnould, C.; Penta, M.; Renders, A.; Thonnard, J.L. ABILHAND-kids: A measure of manual ability in children with cerebral palsy. Neurology 2004, 63, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Rabuffetti, M.; Meriggi, P.; Pagliari, C.; Bartolomeo, P.; Ferrarin, M. Differential actigraphy for monitoring asymmetry in upper limb motor activities. Physiol. Meas. 2016, 37, 1798–1812. [Google Scholar] [CrossRef]
- Hwang, Y.S.; Kwon, J.Y. Effects of modified constraint-induced movement therapy in real-world arm use in young children with unilateral cerebral palsy: A single-blind randomized trial. Neuropediatrics 2020, 51, 259–266. [Google Scholar] [CrossRef]
- Coker-Bolt, P.; Downey, R.J.; Connolly, J.; Hoover, R.; Shelton, D.; Seo, N.J. Exploring the feasibility and use of accelerometers before, during, and after a camp-based CIMT program for children with cerebral palsy. J. Pediatr. Rehabil. Med. 2017, 10, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, B.M.; Sabelhaus, E.K.; Pan, Y.C.; Bjornson, K.F.; Pham, K.L.D.; Walker, W.O.; Steele, K.M. Accelerometer measurements indicate that arm movements of children with cerebral palsy do not increase after constraint-induced movement therapy (CIMT). Am. J. Occup. Ther. 2020, 74, 7405205100p1–7405205100p9. [Google Scholar] [CrossRef]
- Haley, S.M.; Coster, W.J.; Dumas, H.M.; Fragala-Pinkham, M.A.; Kramer, J.; Ni, P.; Tian, F.; Kao, Y.C.; Moed, R.; Ludlow, L.H. Accuracy and precision of the Pediatric Evaluation of Disability Inventory computer-adaptive tests (PEDI-CAT). Dev. Med. Child Neurol. 2011, 53, 1100–1106. [Google Scholar] [CrossRef]
- Uswatte, G.; Taub, E.; Griffin, A.; Vogtle, L.; Rowe, J.; Barman, J. The pediatric motor activity log-revised: Assessing real-world arm use in children with cerebral palsy. Rehabil. Psychol. 2012, 57, 149–158. [Google Scholar] [CrossRef]
- Randall, M.; Imms, C.; Carey, L.M.; Pallant, J.F. Rasch analysis of the Melbourne Assessment of Unilateral Upper Limb Function. Dev. Med. Child Neurol. 2014, 56, 665–672. [Google Scholar] [CrossRef]
- Holmefur, M.; Krumlinde-Sundholm, L.; Eliasson, A.C. Interrater and intrarater reliability of the Assisting Hand Assessment. Am. J. Occup. Ther. 2007, 61, 79–84. [Google Scholar] [CrossRef]
- Law, M.; Baptiste, S.; McColl, M.; Opzoomer, A.; Polatajko, H.; Pollock, N. The Canadian occupational performance measure: An outcome measure for occupational therapy. Can. J. Occup. Ther. 1990, 57, 82–87. [Google Scholar] [CrossRef]
- Klingels, K.; Jaspers, E.; Staudt, M.; Guzzetta, A.; Mailleux, L.; Ortibus, E.; Feys, H. Do mirror movements relate to hand function and timing of the brain lesion in children with unilateral cerebral palsy? Dev. Med. Child Neurol. 2016, 58, 735–742. [Google Scholar] [CrossRef]
- Tamboosi, M.E.; Al-Khathami, S.S.; El-Shamy, S.M. The effectiveness of tele-rehabilitation on improvement of daily living activities in children with cerebral palsy: Narrative review. Bull. Fac. Phys. Ther. 2021, 26, 40. [Google Scholar] [CrossRef]
- Jaspers, E.; Desloovere, K.; Bruyninckx, H.; Klingels, K.; Molenaers, G.; Aertbeliën, E.; Van Gestel, L.; Feys, H. Three-dimensional upper limb movement characteristics in children with hemiplegic cerebral palsy and typically developing children. Res. Dev. Disabil. 2011, 32, 2283–2294. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.Y.; Chang, W.H.; Chang, H.J.; Yi, S.H.; Kim, M.Y.; Kim, E.H.; Kim, Y.H. Changes in diffusion tensor tractographic findings associated with constraint-induced movement therapy in young children with cerebral palsy. Clin. Neurophysiol. 2014, 125, 2397–2403. [Google Scholar] [CrossRef] [PubMed]
- Vrigkas, M.; Nikou, C.; Kakadiaris, I.A. A review of human activity recognition methods. Front. Robot. AI 2015, 2, 28. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | ||
|---|---|---|
| Age, mean (SD), years | 5.48 (1.85) | |
| Sex, n (%) | Male | 12 (54.54) |
| Female | 10 (45.46) | |
| MACS level n (%) | 1 | 7 (31.83) |
| 2 | 10 (45.45) | |
| 3 | 5 (22.72) | |
| Side of involvement, n (%) | Right | 17 (77.27) |
| Left | 5 (22.73) | |
| T0 | T1 | p | |
|---|---|---|---|
| Affected side | |||
| VMA of all axes | 463.95 ± 145.56 | 497.35 ± 156.20 | 0.152 |
| VMA of Axis1 | 261.80 ± 83.66 | 278.74 ± 84.77 | 0.233 |
| VMA of Axis2 | 246.79 ± 78.65 | 265.41 ± 85.36 | 0.134 |
| VMA of Axis3 | 258.18 ± 88.12 | 279.58 ± 98.50 | 0.125 |
| Less-affected side | |||
| VMA of all axes | 772.66 ± 182.07 | 797.50 ± 185.74 | 0.367 |
| VMA of Axis1 | 421.20 ± 114.43 | 439.62 ± 112.14 | 0.279 |
| VMA of Axis2 | 407.42 ± 103.81 | 424.33 ± 104.72 | 0.251 |
| VMA of Axis3 | 449.98 ± 98.91 | 456.76 ± 107.25 | 0.681 |
| Combined measures | |||
| VMA Ratio | −0.54 ± 0.21 | −0.50 ± 0.23 | 0.09 |
| VMA Ratio Axis1 | −0.49 ± 0.17 | −0.48 ± 0.19 | 0.349 |
| VMA Ratio Axis2 | −0.53 ± 0.18 | −0.50 ± 0.22 | 0.28 |
| VMA Ratio Axis3 | −0.60 ± 0.29 | −0.53 ± 0.29 | 0.017 * |
| Sum of VMA | 1236.61 ± 313.89 | 1294.84 ± 323.21 | 0.236 |
| Week 1 | Week 2 | Week 3 | ||
|---|---|---|---|---|
| Less-affected side | VMA | 238.42 ± 148.54 | 222.79 ± 129.6 | 213.24 ± 125.28 |
| VMA Axis1 | 106.69 ± 75.67 | 94.21 ± 61.39 | 85.11 ± 56.33 | |
| VMA Axis2 | 132.70 ± 77.61 | 126.15 ± 69.64 | 120.6 ± 67.8 | |
| VMA Axis3 | 137.53 ± 96.94 | 127.77 ± 85.55 | 125.22 ± 83.99 | |
| Affected side | VMA | 552.35 ± 152.85 | 568.23 ± 153.07 | 565.67 ± 173.68 |
| VMA Axis1 | 310.35 ± 92.3 | 320.89 ± 90.28 | 317.26 ± 94.3 | |
| VMA Axis2 | 321.03 ± 92.05 | 330.82 ± 100.78 | 330.25 ± 108.67 | |
| VMA Axis3 | 269.81 ± 94.12 | 274.69 ± 94.82 | 275.63 ± 111.01 | |
| Ratio | VMA Ratio | 0.99 ± 0.54 | 1.08 ± 0.56 | 1.11 ± 0.56 |
| Axis1 | 1.25 ± 0.57 | 1.39 ± 0.58 | 1.48 ± 0.57 | |
| Axis2 | 1.01 ± 0.56 | 1.09 ± 0.58 | 1.15 ± 0.63 | |
| Axis3 | 0.85 ± 0.65 | 0.93 ± 0.68 | 0.92 ± 0.66 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, Y.; Kwon, J.-Y.; Na, Y. An Exploration of Tri-Axial Accelerometers in Assessing the Therapeutic Efficacy of Constraint-Induced Movement Therapy in Children with Unilateral Cerebral Palsy. Sensors 2023, 23, 9393. https://doi.org/10.3390/s23239393
Hwang Y, Kwon J-Y, Na Y. An Exploration of Tri-Axial Accelerometers in Assessing the Therapeutic Efficacy of Constraint-Induced Movement Therapy in Children with Unilateral Cerebral Palsy. Sensors. 2023; 23(23):9393. https://doi.org/10.3390/s23239393
Chicago/Turabian StyleHwang, Youngsub, Jeong-Yi Kwon, and Yoonju Na. 2023. "An Exploration of Tri-Axial Accelerometers in Assessing the Therapeutic Efficacy of Constraint-Induced Movement Therapy in Children with Unilateral Cerebral Palsy" Sensors 23, no. 23: 9393. https://doi.org/10.3390/s23239393
APA StyleHwang, Y., Kwon, J.-Y., & Na, Y. (2023). An Exploration of Tri-Axial Accelerometers in Assessing the Therapeutic Efficacy of Constraint-Induced Movement Therapy in Children with Unilateral Cerebral Palsy. Sensors, 23(23), 9393. https://doi.org/10.3390/s23239393