1. Introduction
Today, most high-income countries’ economy has transitioned from the production of goods to the provision of services [
1]. This transition has resulted in an increasing number of people employed in sedentary occupations, in which work is primarily carried out while sitting down [
2]. In fact, a 2017 Eurostat report found that 39% of employees in the EU spent the majority of work hours seated(
https://ec.europa.eu/eurostat/web/products-eurostat-news/-/DDN-20190305-1, accessed on 10 March 2022).
According to the European Agency for Safety and Health at Work, office workers are by far the most at risk of prolonged static sitting [
3], with research showing these individuals can spend between 65% to more than 80% of work hours sitting [
4], where prolonged static sitting bouts account for 55% of total work hours [
5]. This places office workers at an increased risk for: Cardiovascular Diseases (CVDs) related to sedentary behavior [
6]; and Musculoskeletal Disorders (MSDs) in the back, neck, shoulders, and limbs, particularly when awkward/poor postures are adopted [
7,
8].
In the EU, up to 100 million citizens suffer from some type of MSD, of which over 40% are work-related, making these disorders the cause for almost 50% of absenteeism and 60% of permanent work incapacity, leading to direct and indirect costs estimated at €240k million annually [
9]. CVDs, on the other hand, are currently the leading cause of death worldwide, with the number of deaths expected to rise to 23 million by 2030, compared to 17 million in 2017 [
10], and the total global cost of treatment expected to increase from USD 863 k million in 2010 to approximately USD 1 billion by 2030 [
11].
The aforementioned effects, associated with prolonged static sitting in the workplace, ultimately represent a serious economic and social issue for both employers and overall society, due to increased absenteeism, health care, disability, and worker’s compensation costs, as well as lost productivity.
In light of these issues, there has been a growing interest in the development of systems capable of continuously monitoring either employees’ sitting behavior and posture, or cardiovascular health, but, as of now, no system proposed in the literature has integrated both of these monitoring modules. Sitting Posture Monitoring Systems (SPMSs) can be roughly divided into three main categories: computer vision based systems, wearable sensor systems and sensory chairs [
12]. Even within each of these categories, system design and sitting posture classification approaches vary widely, but sensory chair-based SPMSs are by far the most ubiquitous in terms of sensor integration, user comfort and practicality.
In addition, taking into account that CVDs are a leading cause of death worldwide in developing and developed countries alike, early detection is key to prevent severe and disabling events. The Electrocardiogram (ECG) is a first-line clinical diagnosis exam for cardiovascular health assessment, in particular for the diagnosis of cardiac arrythmias, typically acquired through self-adhesive pre-gelled electrodes placed on the body. However, existing approaches are either extremely impractical in the context of office work or require collaboration of the users (e.g., touching a smartwatch worn by the user to enable measurement). Rather than requiring sensors to be placed explicitly on the user’s body, “invisible” systems, which incorporate sensors in everyday use objects or in the the environment around the user, are much better suited, especially for the early diagnosis and treatment of CVDs [
13], and sensory chair-based SPMSs have the potential to easily incorporate sensors with the capacity for “invisible” ECG signal acquisition [
14,
15].
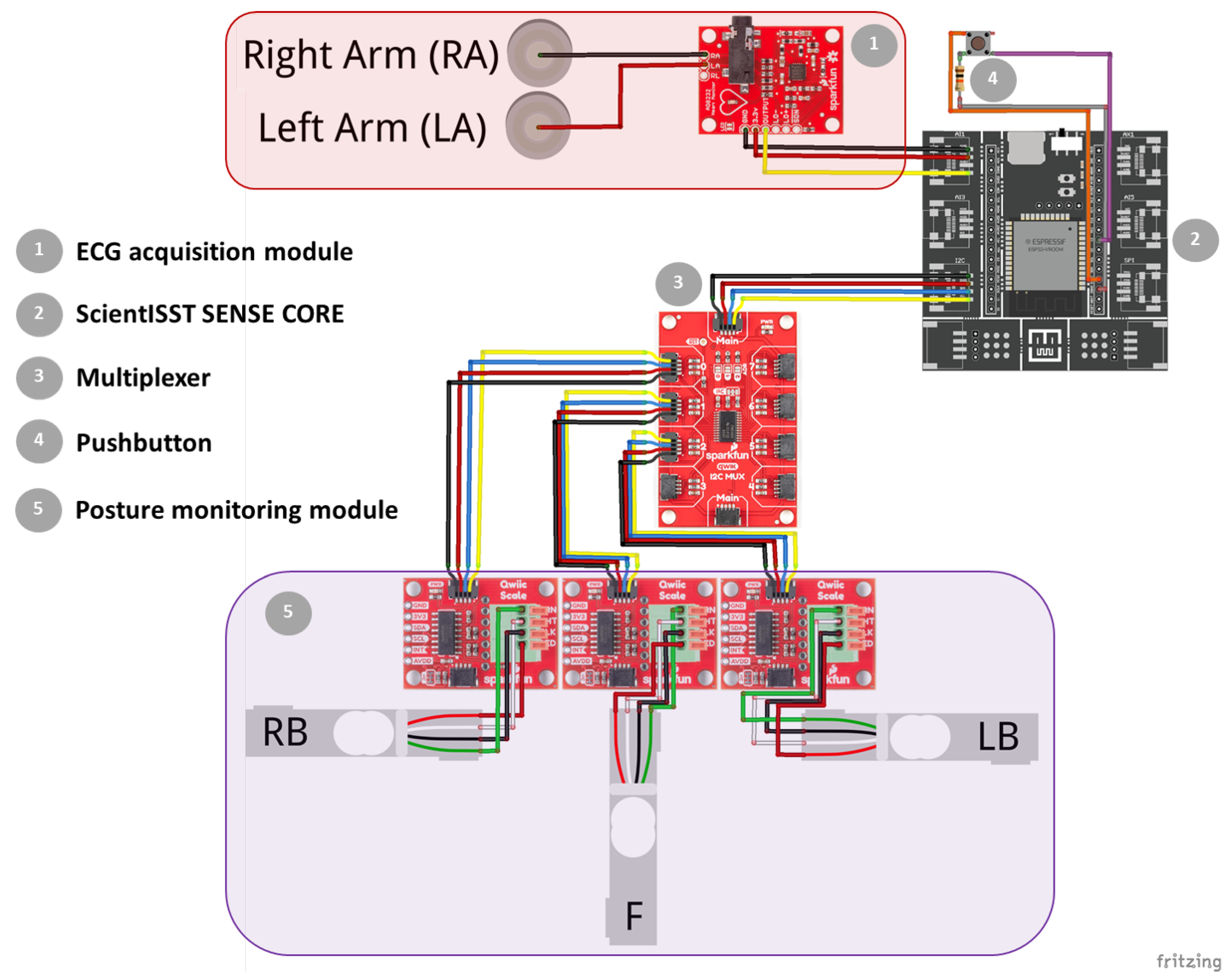
As such, this article proposes a smart chair system that, through an “invisible” sensing approach, can monitor conditions found to impact workers’ productivity, well-being and health, such as the user’s sitting behavior, posture, and ECG signal, without interfering in their daily activities. Thus, the focus of this work was to build upon the state-of-the-art by developing a SPMS and ECG monitoring module, which could be easily incorporated into an office chair (using low-cost hardware to facilitate large scale deployment), and to validate and evaluate the performance of these modules using data collected from them, including novel datasets for training and testing machine learning models for posture classification.
The remainder of the work is organized as follows.
Section 2 describes previous work found in literature and addressing related topics.
Section 3 presents our proposed approach to sensory chair-based SPMS.
Section 4 summarizes the experimental evaluation results, and
Section 5 discusses the performance of the proposed approach with other systems in the literature. Finally,
Section 6 highlights the main conclusions and future work perspectives.
2. State-of-the-Art
SPMSs can be divided into three main categories, according to how relevant information to classify sitting posture is gathered. Each category has its advantages and drawbacks, but interest in the development of sensory chair-based SPMSs has grown significantly more comparatively to the other two. This growing interest can be explained by these systems’ “invisible” sensing approach, wherein sensors are ubiquitously integrated into the chair, without affecting the person’s comfort or work, enabling near-continuous and highly pervasive posture monitoring, while simultaneously avoiding the limitations of wearable systems (e.g., discomfort, users needing to remember wearing them, increased risk of damage to the sensors due to wear or external factors, abandonment issues) and computer vision based systems (e.g., image quality and camera position effect on performance, privacy concerns, incorrect detection when multiple people are in view).
The concept of sensory chairs to monitor sitting posture was first introduced in 2001 by Tan et al. [
16], who integrated sensor arrays on a chair’s seat and backrest to gather pressure distribution patterns, used to classify posture. Over the years, numerous sensory chair-based SPMSs have been proposed in the literature, using a variety of sensors and classification methods with a myriad of features, extracted from the sensor data, to recognize several types of sitting positions.
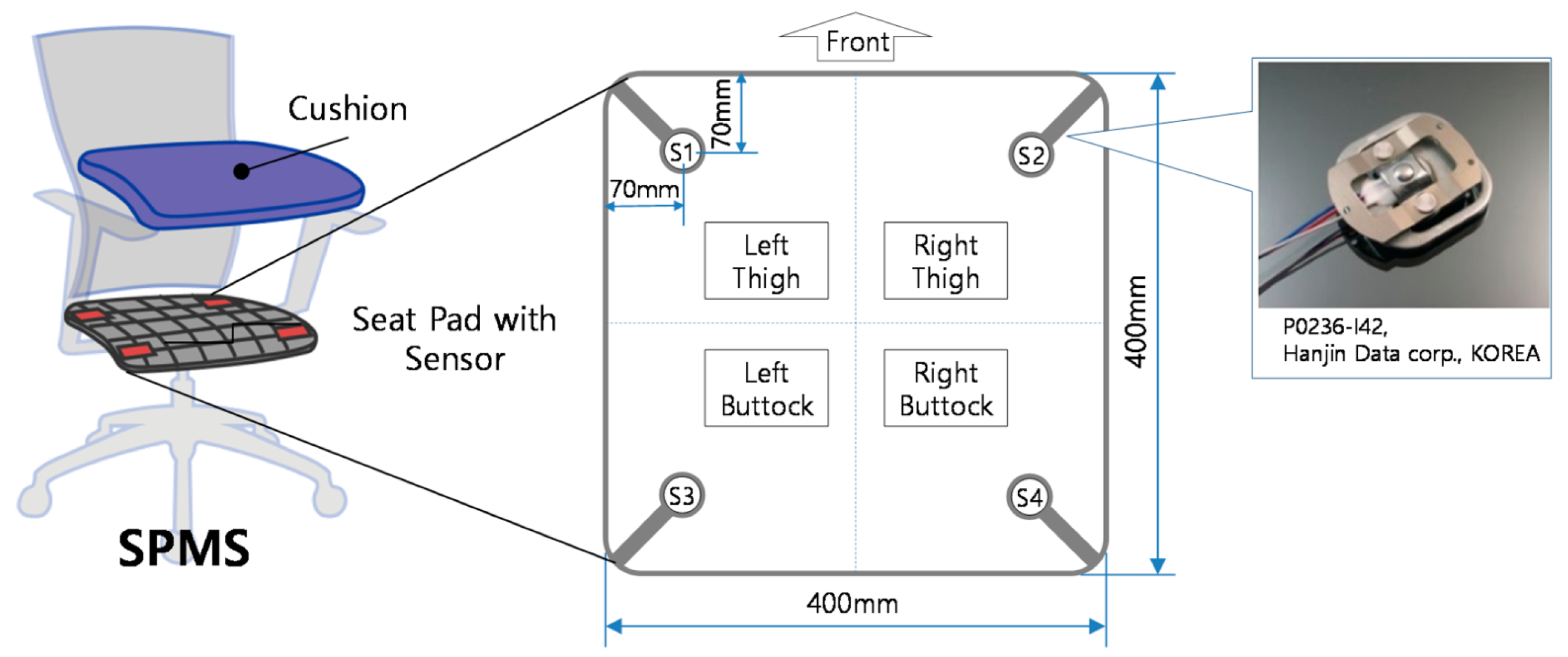
Roh et al. (2018) [
17] developed a SPMS using four beam-type load cells integrated into the seat frame, as shown in
Figure 1, to classify six postures using a feature vector composed by the ratio of total weight measured by the sensors to body weight, and of weight distribution in the medial-lateral and the anterior-posterior directions. Using a Support Vector Machine (SVM) with the radial basis function kernel, an average accuracy rate of 97.20% was obtained in the classification of postures from nine subjects.
Huang et al. (2017) [
18] also used pressure sensors in their SPMS, but in the form of a 52 × 44 piezo-resistive sensor array, to measure the pressure patterns in the chair seat of eight sitting positions, used as input for an Artificial Neural Network (ANN) classifier. The average accuracy obtained was 92.2%, lower than the accuracy obtained by Roh et al. (2018) [
17]. One may argue that, by evaluating more sitting positions, the system’s posture monitoring capacity increases by being prepared to distinguish between more postures, which ultimately is preferable for the promotion of dynamic sitting, i.e., the periodic alteration of sitting position. This is the currently recommended guideline by OSH agencies, in detriment of maintaining a posture that is ‘as upright as possible’ at all times, which is no longer considered ideal [
3]. However, in this case, the likelihood of having positions which the SPMS might struggle to differentiate between, e.g. due to their similarity in the feature space, also increases. This trade-off is an important factor to take into consideration in the development of a SPMS.
The SPMSs mentioned above all used pressure sensors in their approach, but there are other systems that employ instead sensors capable of measuring the chair seat and backrest tilt to classify sitting posture. Otoda et al. (2018) [
19] uses a total of eight accelerometers (six on the seat and two on the backrest) to measure the inclination angle variation in the
X,
Y and
Z axis, which forms the feature vector used to train a Random Forest model to classify 19 postures. However, the average accuracy rate, evaluated in data collected from 20 subjects, was only 80.1%, potentially due to the higher number of postures evaluated. Additionally, using this type of sensors is only feasible, if the chair is more prone to tilting or deformable with movement, such as chairs with mesh instead of foam cushions.
There are also mixed sensor SPMSs, as is the case of the system proposed by Jeong et al. (2021) [
20], which combines six pressure sensors in the seat with six infrared distance sensors in the backrest, granting it a higher capability to classify postures that only differ in terms of distance between the user’s back and the chair’s backrest (e.g., positions with trunk rotation). As such, for eleven sitting positions, this system was still able to achieve an overall accuracy rate of 92.0% using a k-Nearest Neighbor (k-NN) model, but this does come at the expense of higher system complexity and cost.
A number of SPMSs proposed in the literature (including those that have already been mentioned above) have been summarized in
Table 1 and
Table 2, according to the type and location of sensors used, the number of sitting positions considered, and the classification method employed. By analyzing these tables, it can be concluded that the classification accuracy achieved by sensory chair-based SPMSs varies widely, depending on the overall approach taken, which includes the sensor type and location, the number of sitting positions evaluated, and the classification methods used. Nevertheless, there is a clear trend towards the use of pressure sensors and machine learning models for posture classification.
Additionally, more complex and high-precision SPMSs that use pressure sensor mats in their approach are oftentimes able to maintain high accuracy scores when trained to classify a considerable amount of sitting positions, some of them very similar to each other, as is the case in the work developed by Huang et al. (2017) [
18]. However, using these sensors can hinder large scale deployment of the SPMS, since pressure sensor mats can be very expensive (e.g., the CER2 CONFORMat
™ sensor with 2048 sensing elements from Tekscan
™ is commercially available for USD 3000), and may need to be replaced as a whole, if individual sensing elements in the array are damaged, which becomes more likely in the context of everyday use in an office environment. Furthermore, computing features from the high dimensional data generated by these sensors in real-time also has a high computational cost. As such, this work sought to develop a simpler SPMS, more suitable for deployment at scale, using fewer, inexpensive and more easily replaceable sensors, which could achieve similar or better accuracy scores considering more sitting positions than other SPMSs proposed in the literature.
4. Results
4.1. Electrocardiography Performance Evaluation
The results of the comparative analysis between the ECG signals acquired with the proposed and reference systems are summarized in
Table 3.
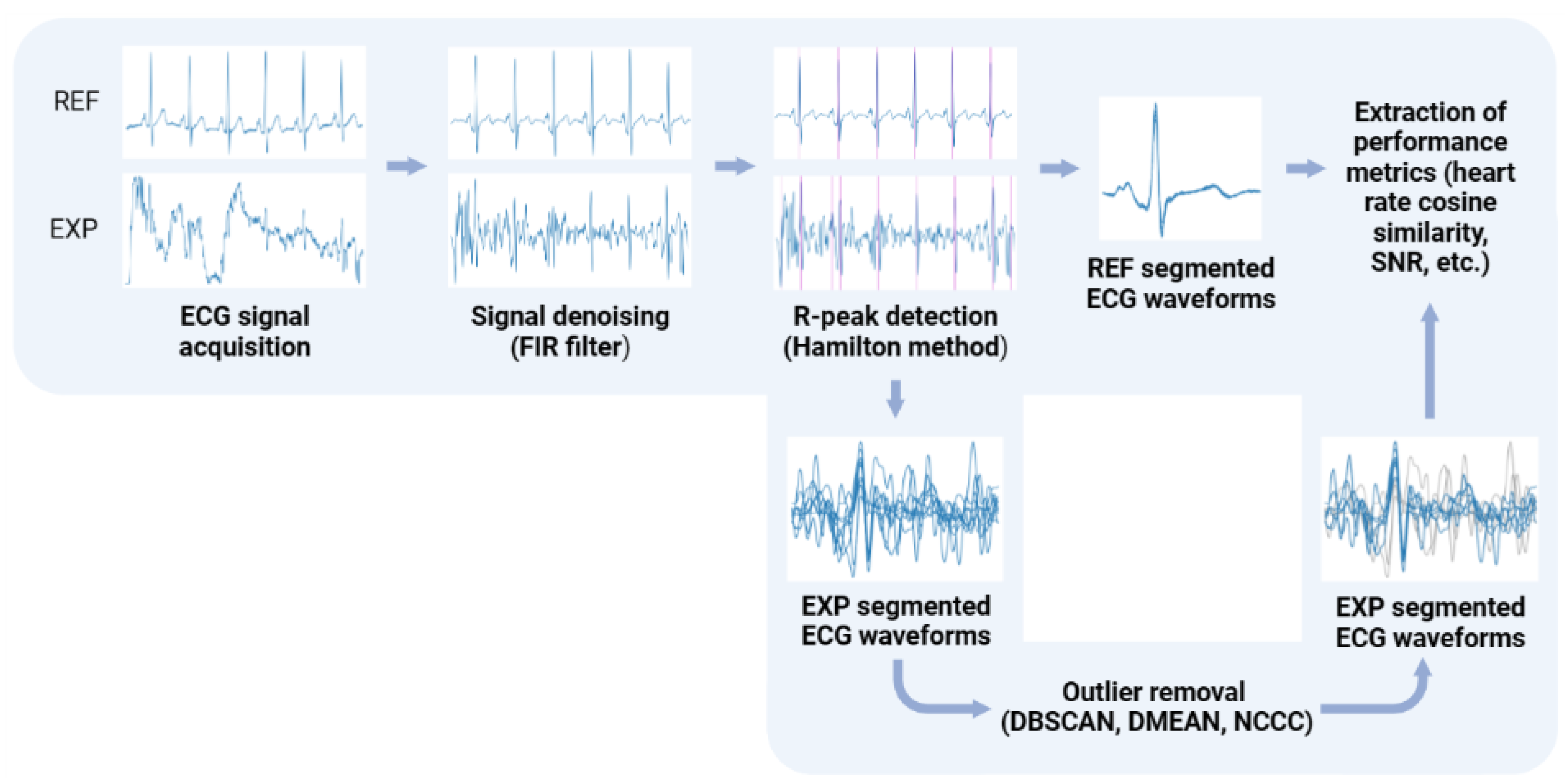
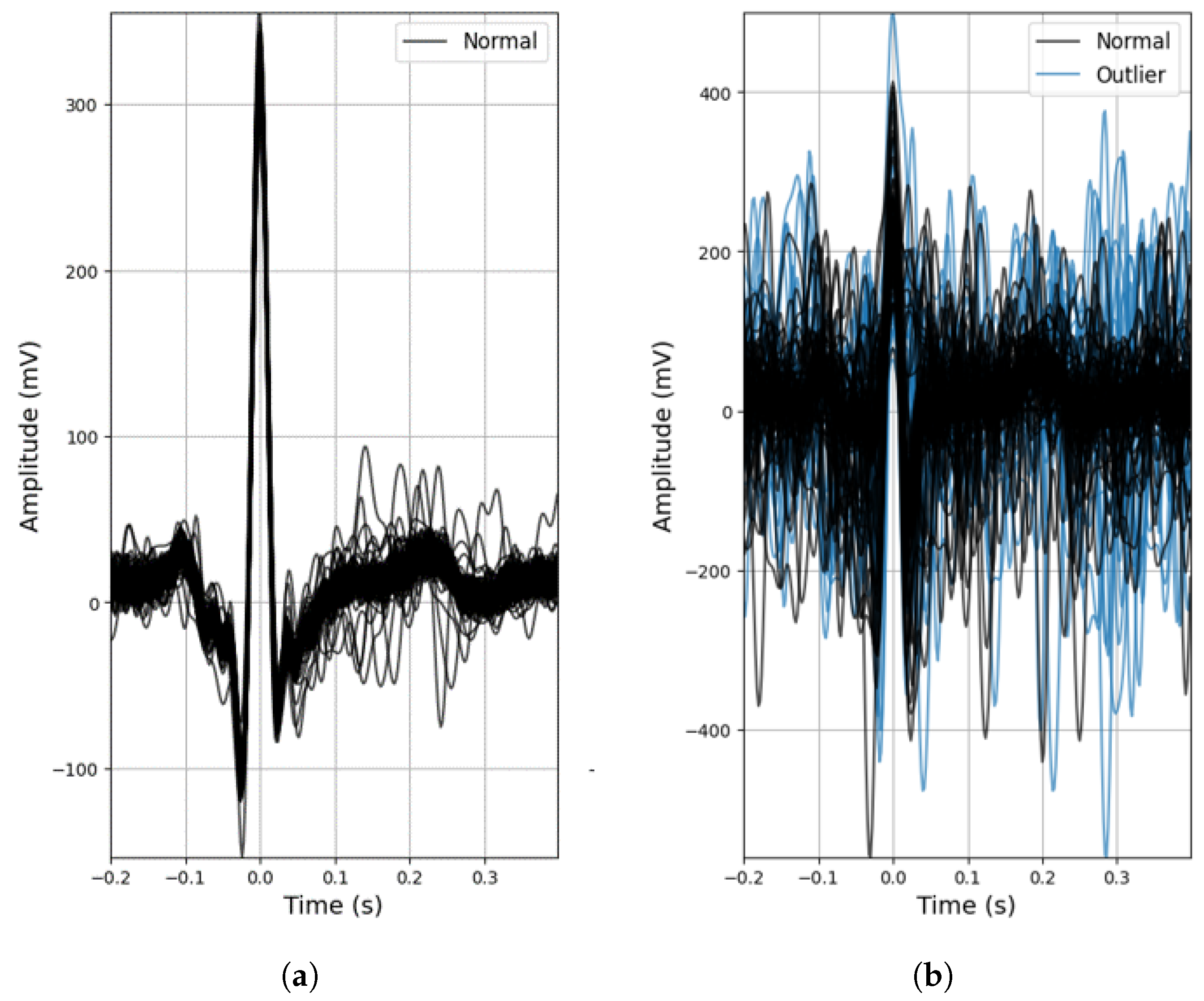
As mentioned beforehand, the conductive nappa and use of two active electrodes are more prone to noise (
Figure 6b), but even so, despite the lower R-peak amplitudes (expected due to the increased impedance) and the effect of noise, for the majority of the ECG signals acquired with the conductive nappa, the general morphology of the ECG signal was maintained, as can be observed in
Figure 6a, with some signals even achieving a SNR of 12.17 dB. In fact, even without any outlier detection algorithm applied to the extracted heartbeat waveforms, both the mean performance and accuracy rate of the proposed ECG system are quite high (
and
, respectively), but the standard deviation of these metrics is also quite high, again indicating that some of the processed ECG signals are still contaminated by noise.
Observing the column for the heart rate metric in
Table 3, without outlier removal, this noise leads leads to an overestimation of the average heart rate value and a high standard deviation, indicating the presence of false positives in R-peak detection. By disregarding these false positives using outlier removal methods, the average heart rate comes closer to the one obtained from a reference sensor with pre-gelled electrodes and the standard deviation drops significantly, with NCCC exhibiting heart rate values quite comparable to those of the reference sensor.
Overall, by applying the outlier detection algorithms, the performance of ECG segmentation decreased, meaning that these methods are removing both erroneously and correctly identified R-peaks. The extent of this decrease varied between these algorithms, depending on their sensitivity to noise. DBSCAN showed the lowest decrease (only ), reason for which it was integrated into the processing pipeline of the acquired ECG signals in the final prototype.
4.2. Center of Mass Evaluation
The dataset of CM coordinates, resulting from the data processing and feature extraction described in
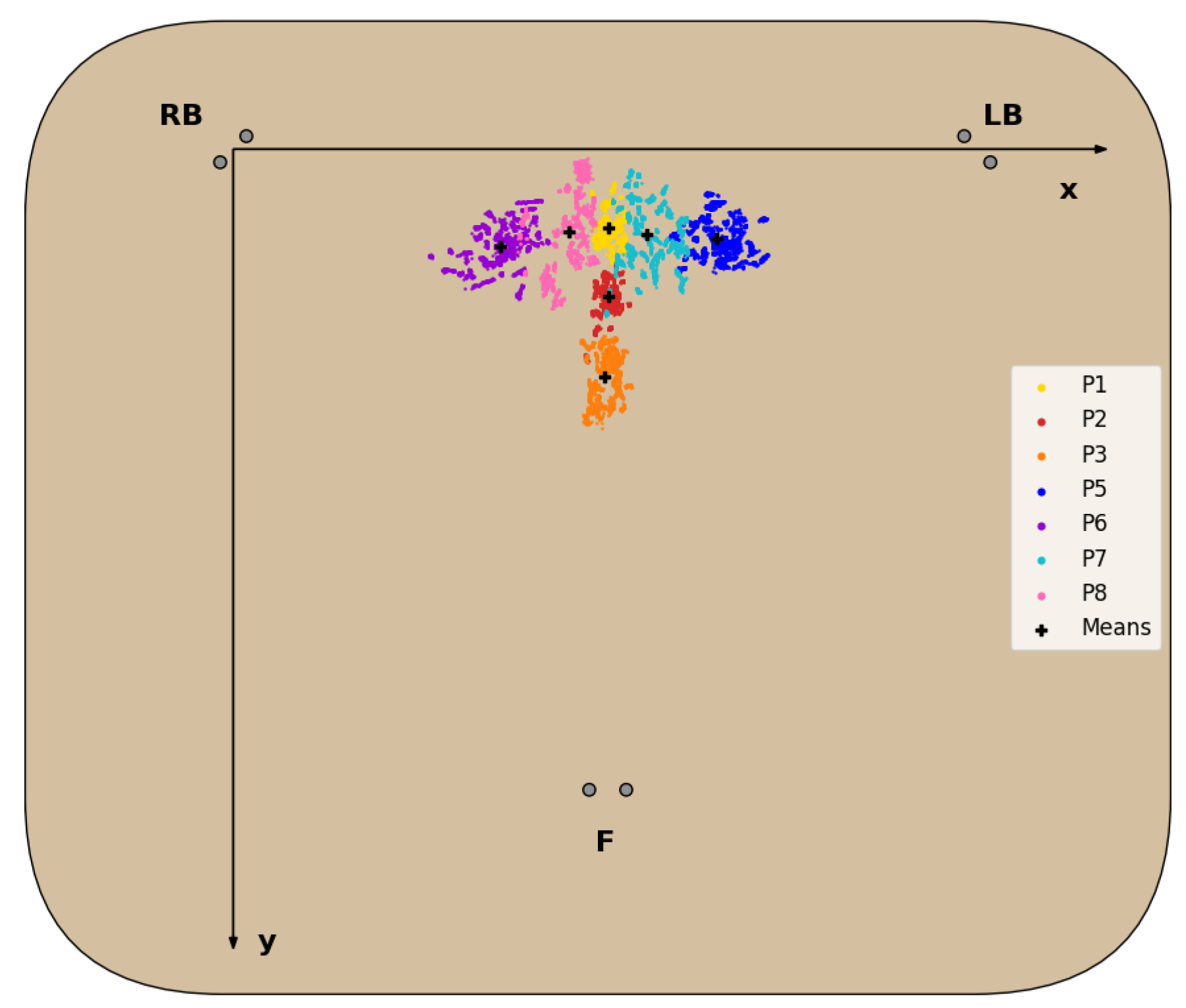
Section 3.3.2, for each sitting position (with the exception of P4 for reasons detailed next) is represented in the chair seat diagram in
Figure 7, and the statistical analysis of the CM coordinates obtained is detailed in
Table 4.
For all sitting positions evaluated, with the exception of P4, the corresponding CM positions obtained formed clusters in the 2D seat plane with little overlap between these clusters, as seen in
Figure 7 and confirmed by the statistical data analysis in
Table 4. Regarding the P4 posture, the CM positions obtained failed to form a defined cluster, due to the chair’s characteristics, which made it unable for subjects to properly and comfortably lean back, resulting in the disproportionately higher standard deviation of the
, seen in
Table 4, and its exclusion from the dataset.
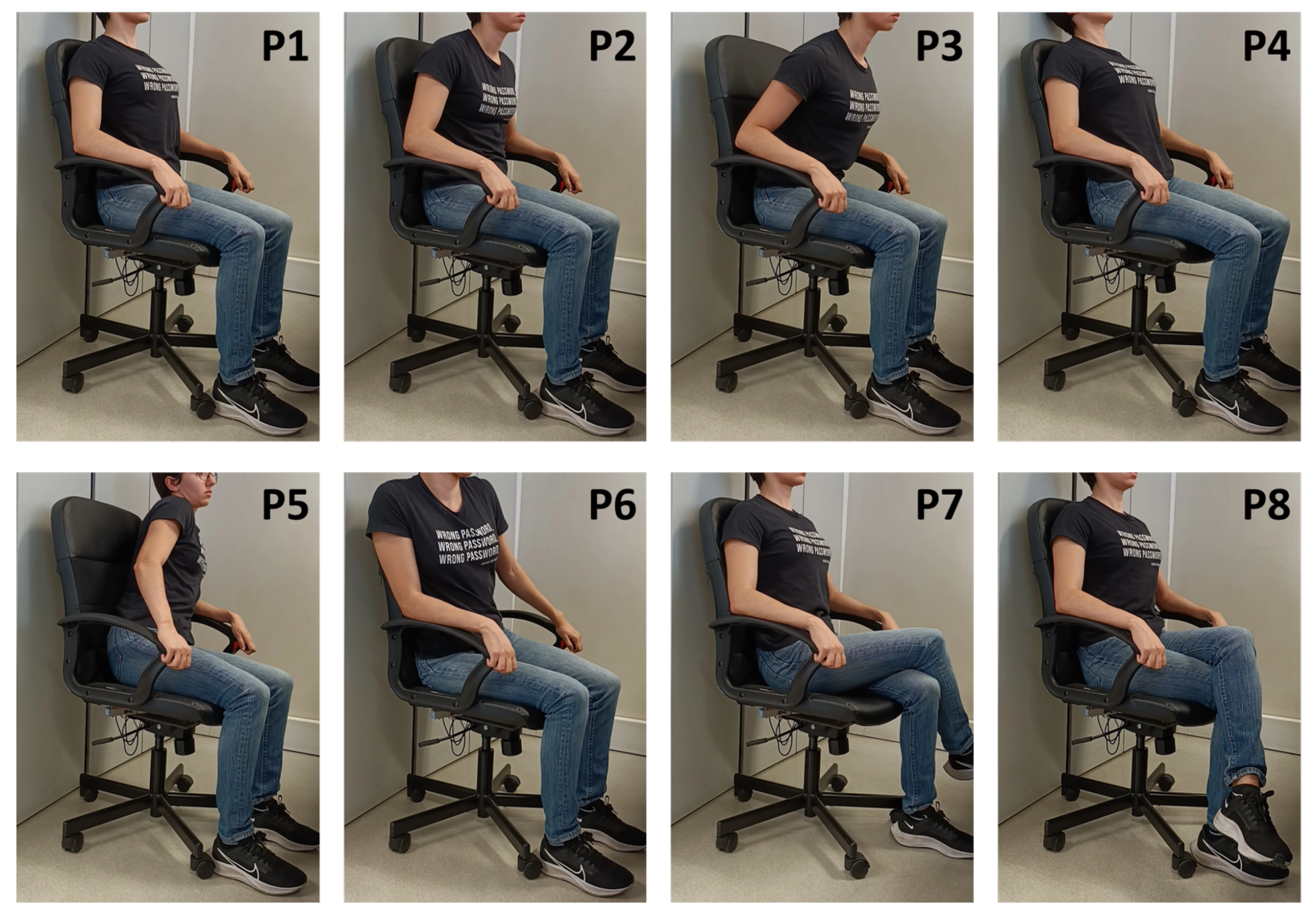
For all other seated postures, the corresponding clusters fall on the expected areas of the chair seat. Positions involving no lateral movement and differing only in the degree of back support (P1,P2,P3) form clusters around the midpoint of the chair seat in the X-axis, as readings from the LB and RB sensors should be fairly similar. In the Y-axis, these clusters are closer to the front of the seat, the lesser the degree of back support, as more weight is shifted towards the F cell. The same logic applies to positions involving only lateral movement (P5 and P6), but in this case weight is shifted towards the left or right side, while the weight in the front remains roughly the same, resulting in the clusters most externally located in the X-axis. Lastly, the clusters for the P7 and P8 positions appear between the clusters of the more central and external positions mentioned above, since the leg crossing motion requires some lateral movement, but not at the same level as fully leaning to the sides.
4.3. Posture Classification Model Training
The optimal hyperparameters obtained from the stratified 5-fold CV process are summarized in
Table 5. For five classes, the trained classifiers all display excellent validation accuracy scores (>99.5%), which was to be expected, taking into consideration the very little overlap between the clusters for these positions. On the other hand, for seven classes, the validation accuracy score of each trained classifier decreased, ranging from 88.95% to 98.72%.
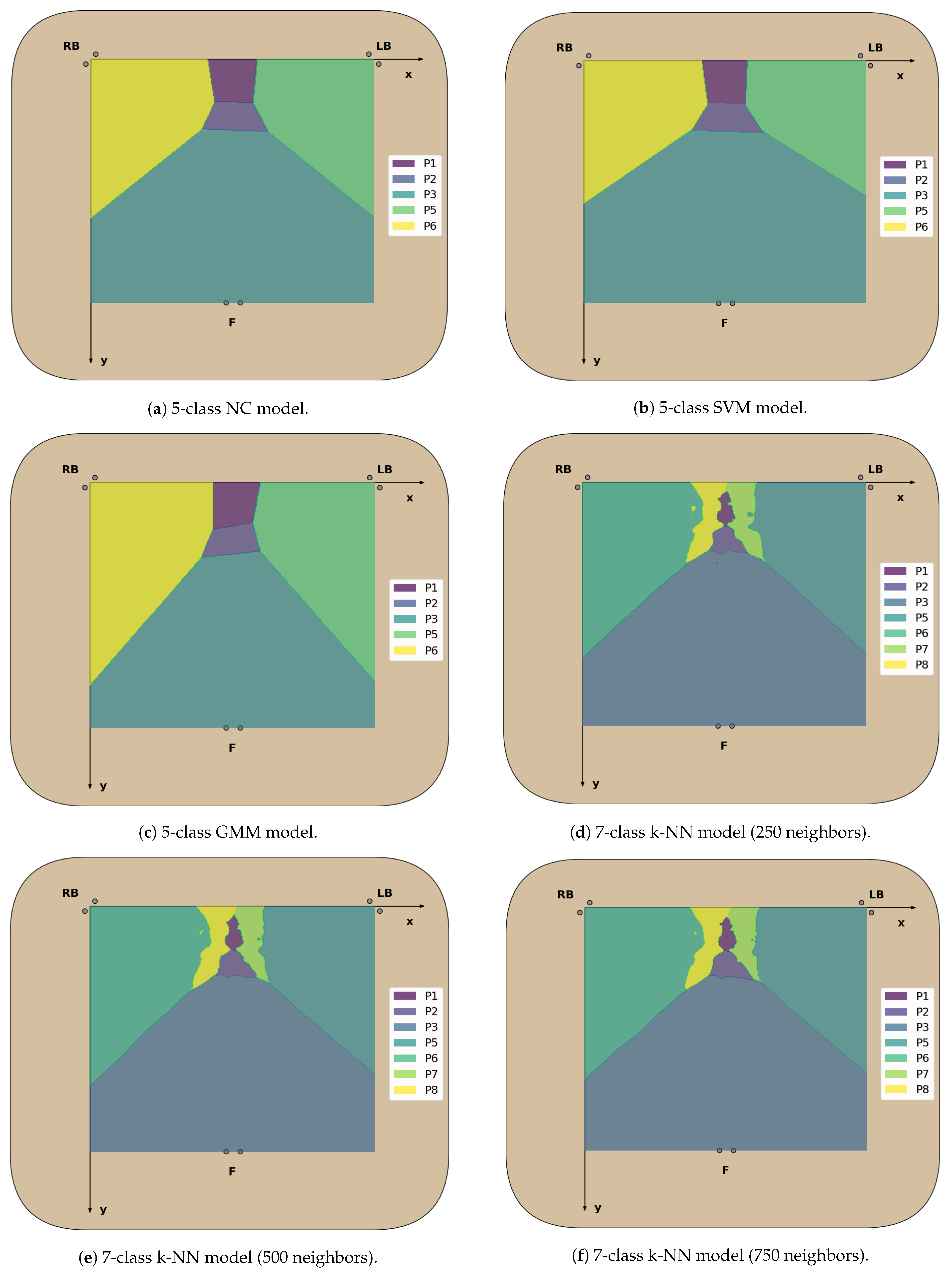
Overall, the k-NN models have the highest validation accuracy scores for both five and seven classes, showing an inverse relationship with the number of neighbors used in the model. The reason behind this relationship is the formation of small “islands” in the decision regions of sitting positions where cluster overlap occurs or outliers simply exist, as in those areas the majority of neighboring samples will correspond to another sitting position, leading to correct classification in the training dataset but potential misclassification for unseen data. This behavior is a disadvantage of this model, which can be reduced by increasing the number of neighbors. The other supervised classification models (NC and SVM) generate more homogeneous decision areas, which is preferred to avoid overfitting.
Furthermore, while the validation accuracy obtained by the GMM model may seem very satisfactory for both five (99.52%) and seven classes (88.95%), this model is not suitable to classify sitting positions from unseen data when considering seven classes. This is because the GMM is a probabilistic model that assumes all data points are generated from a mixture of a finite number of Gaussian distributions with unknown parameters, so if the clusters found in the CM dataset do not approximately follow this distribution, the model will not be able to identify them from the unlabelled data, as is the case here.
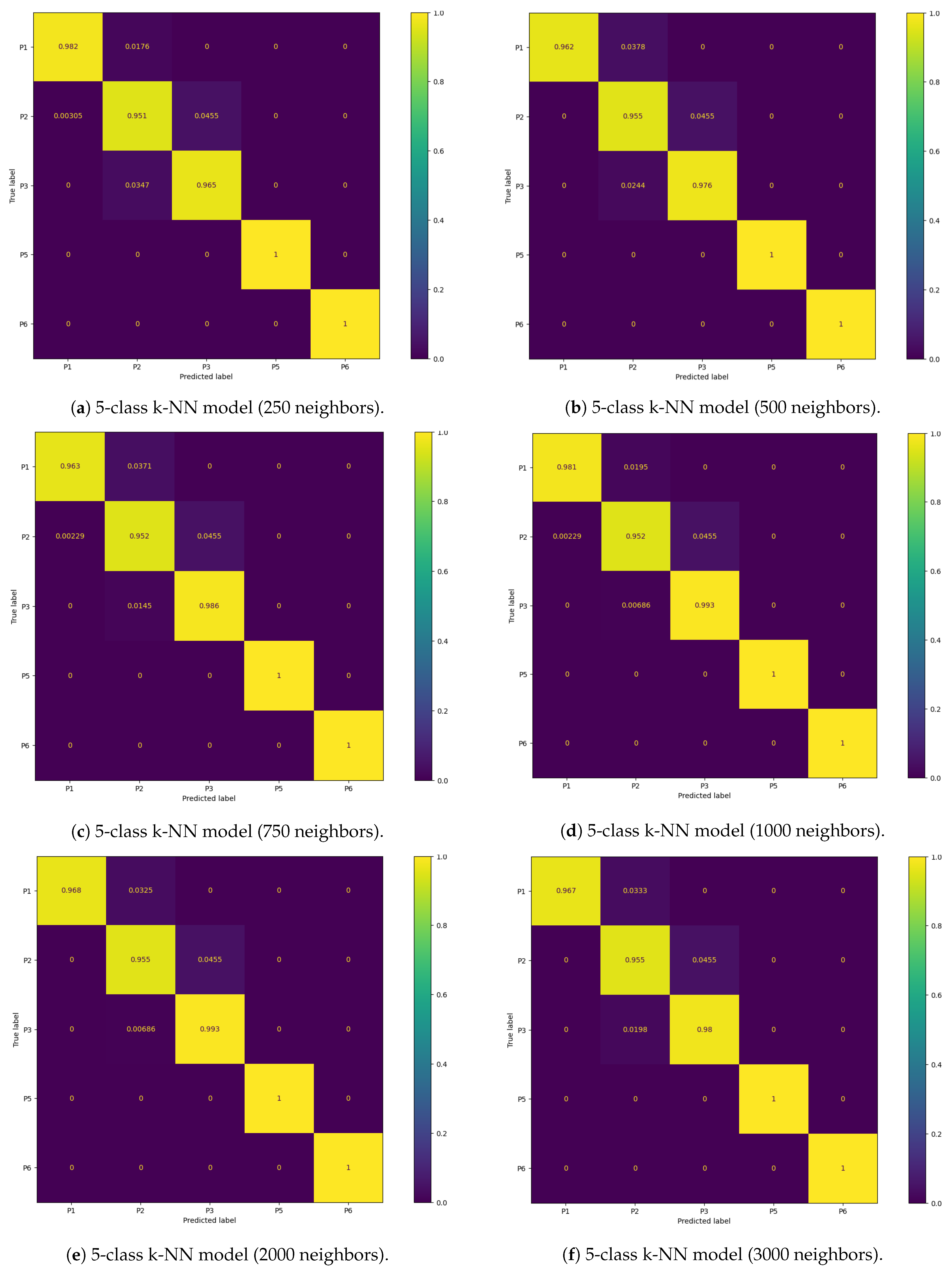
4.4. Performance Evaluation of the Posture Classification Models
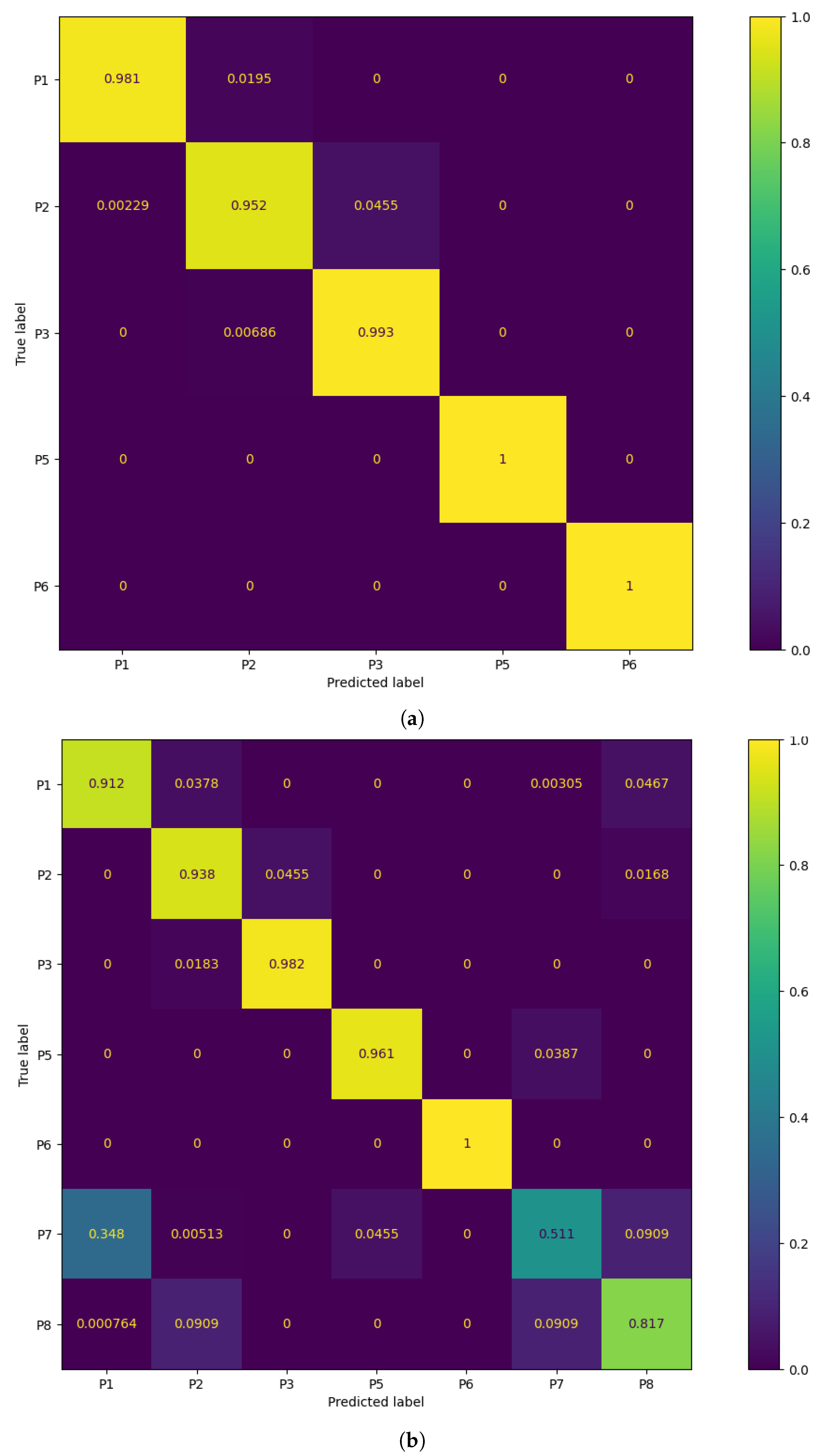
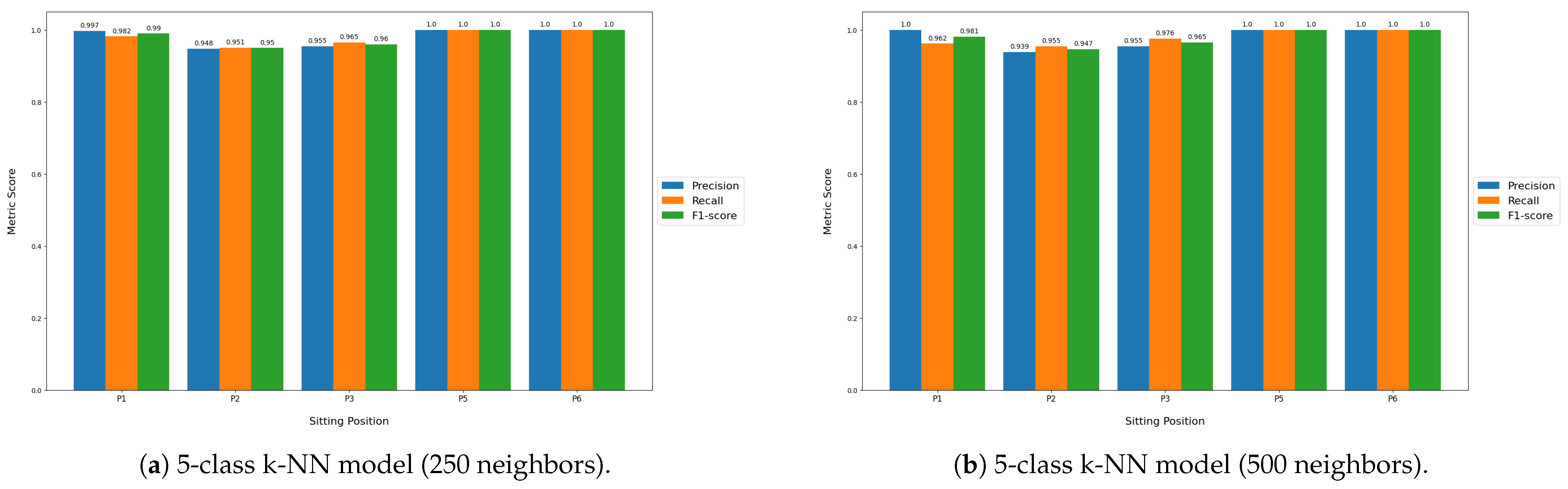
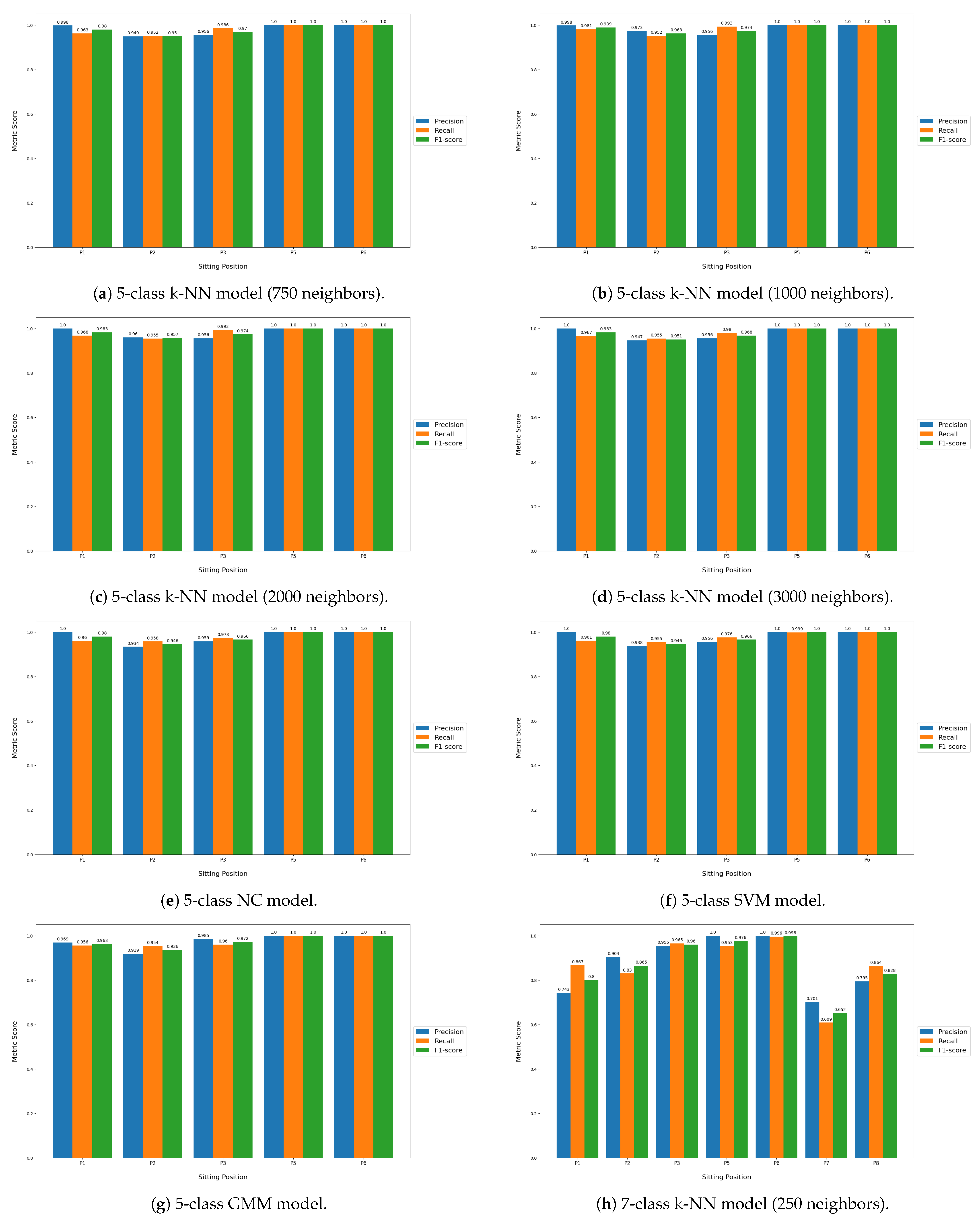
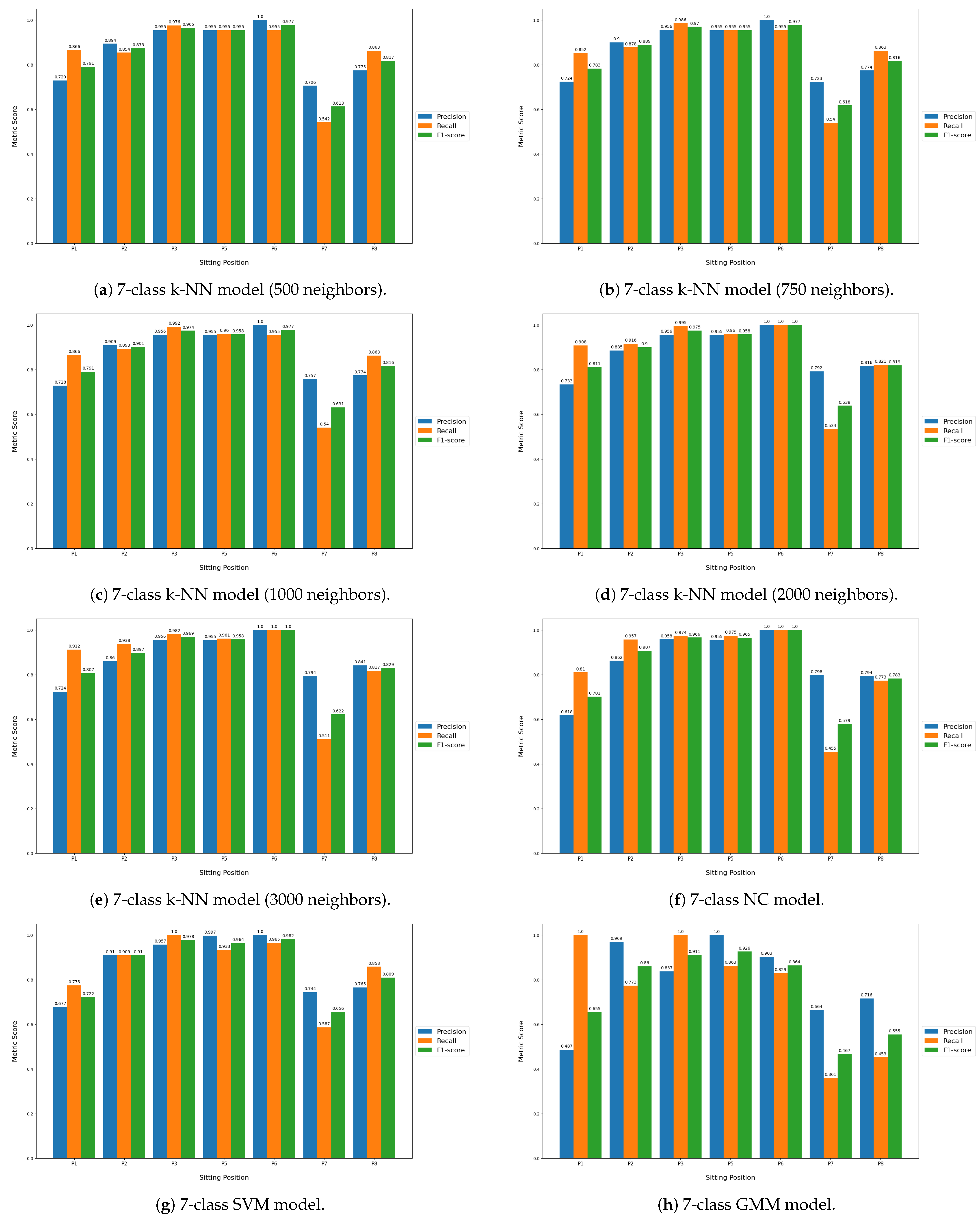
Table 6 displays the classification performance metrics obtained using the test dataset, for each model trained. As a multilabel classification task, the precision, recall and F1-score values were obtained by averaging these metrics’ unweighted mean per label, which can be found in
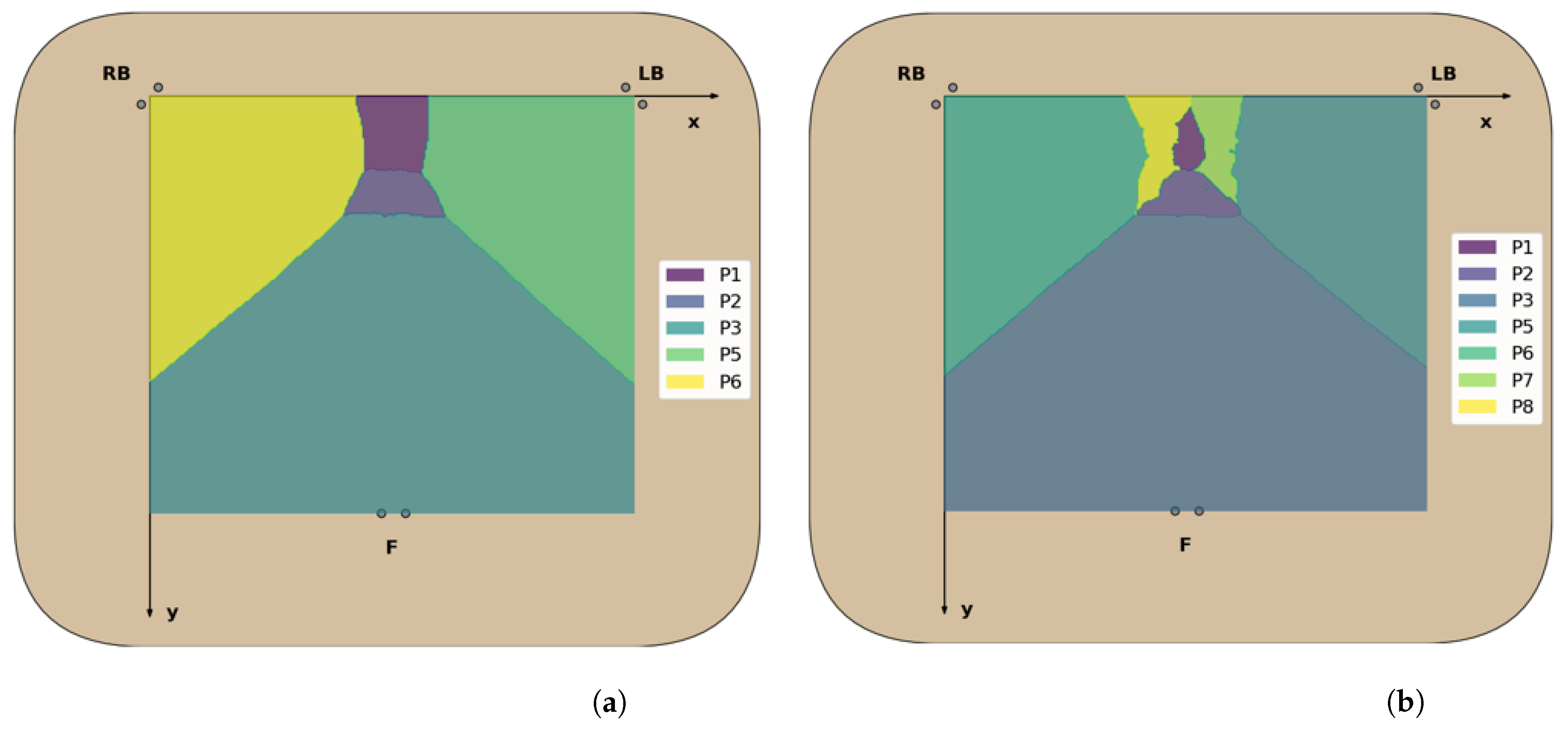
Appendix B.1 displayed in bar plots. Furthermore, in order to better evaluate the classification accuracy per sitting position, confusion matrices were created for each posture classifier evaluated, but only the matrices for the best performing five- and seven-class posture classifiers are displayed here (
Figure 8). For a better insight into each classifier evaluated, all confusion matrices obtained can be found in
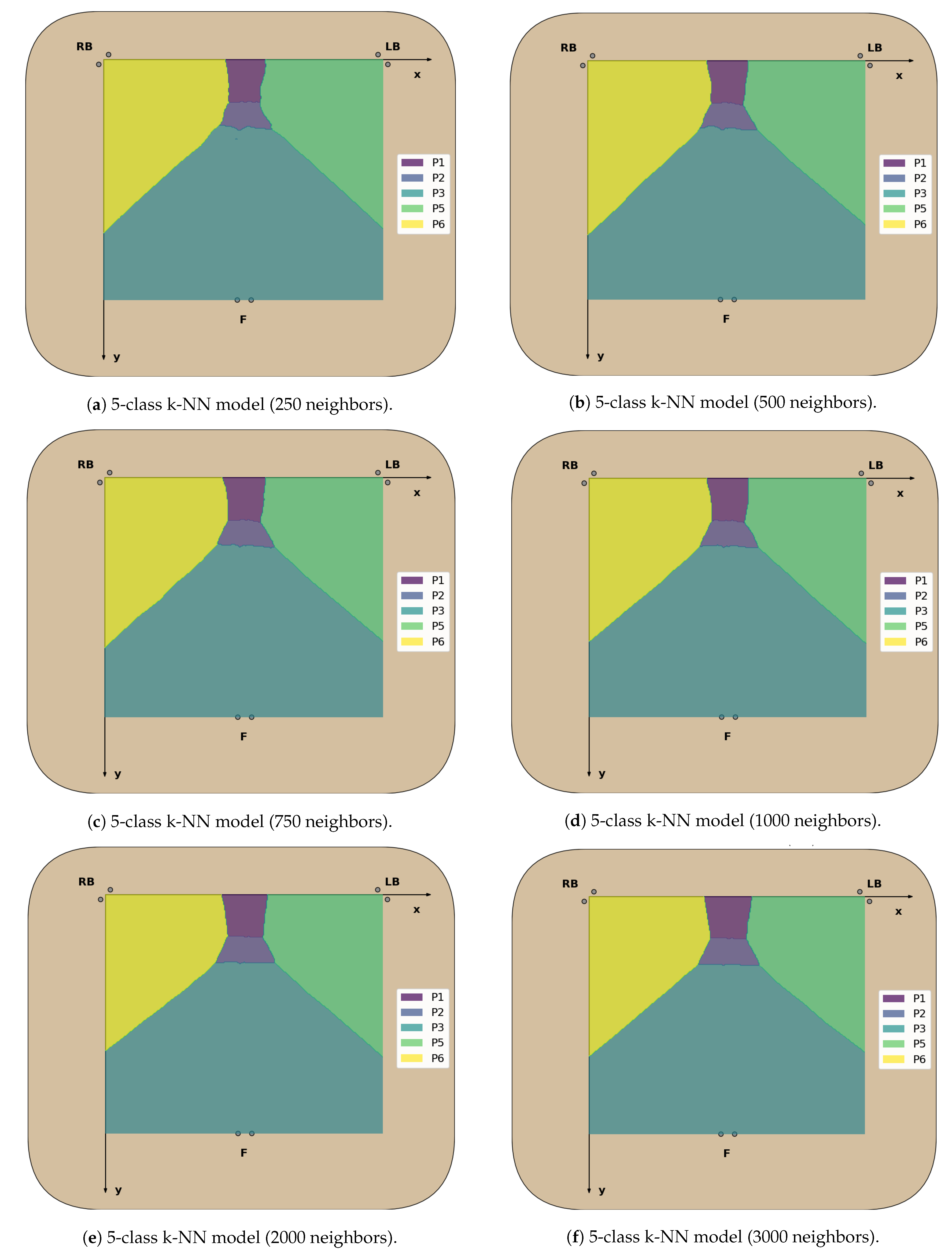
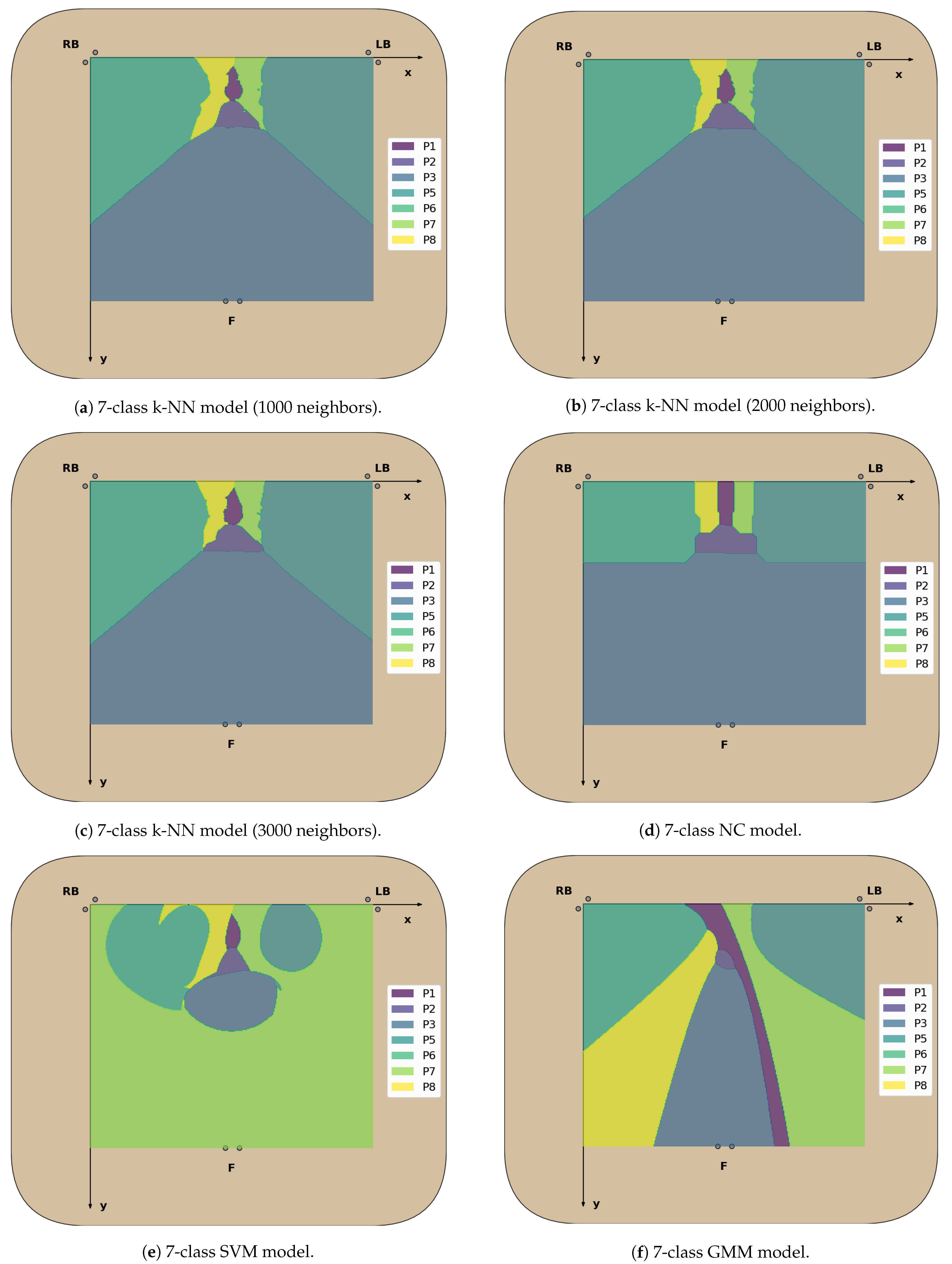
Appendix B.2. Similarly, the decision boundaries in the chair seat plane of these two models are also represented here (
Figure 9), but the decision boundaries of all models can be found in
Appendix B.3.
Overall, for five classes, the classification models exhibit excellent values for each of the evaluated performance metrics (>97.4%), with no significant differences between the accuracy in the test dataset and the validation accuracy. This was to be expected, taking into consideration the little overlap between the clusters of CM coordinates for these positions, leading to high classification accuracy rates across all classes (
Figure 8). The k-NN models had once again the best classification performance, but here the ones using a greater number of neighbors performed better than those using fewer neighbors, as was predicted in the previous section. In particular, using 1000 neighbors yielded the best performance metrics and decision boundaries (
Figure 8) across all models, as using fewer did not completely eliminate the small “islands” caused by cluster overlap, and using more led to more rigid decision boundaries.
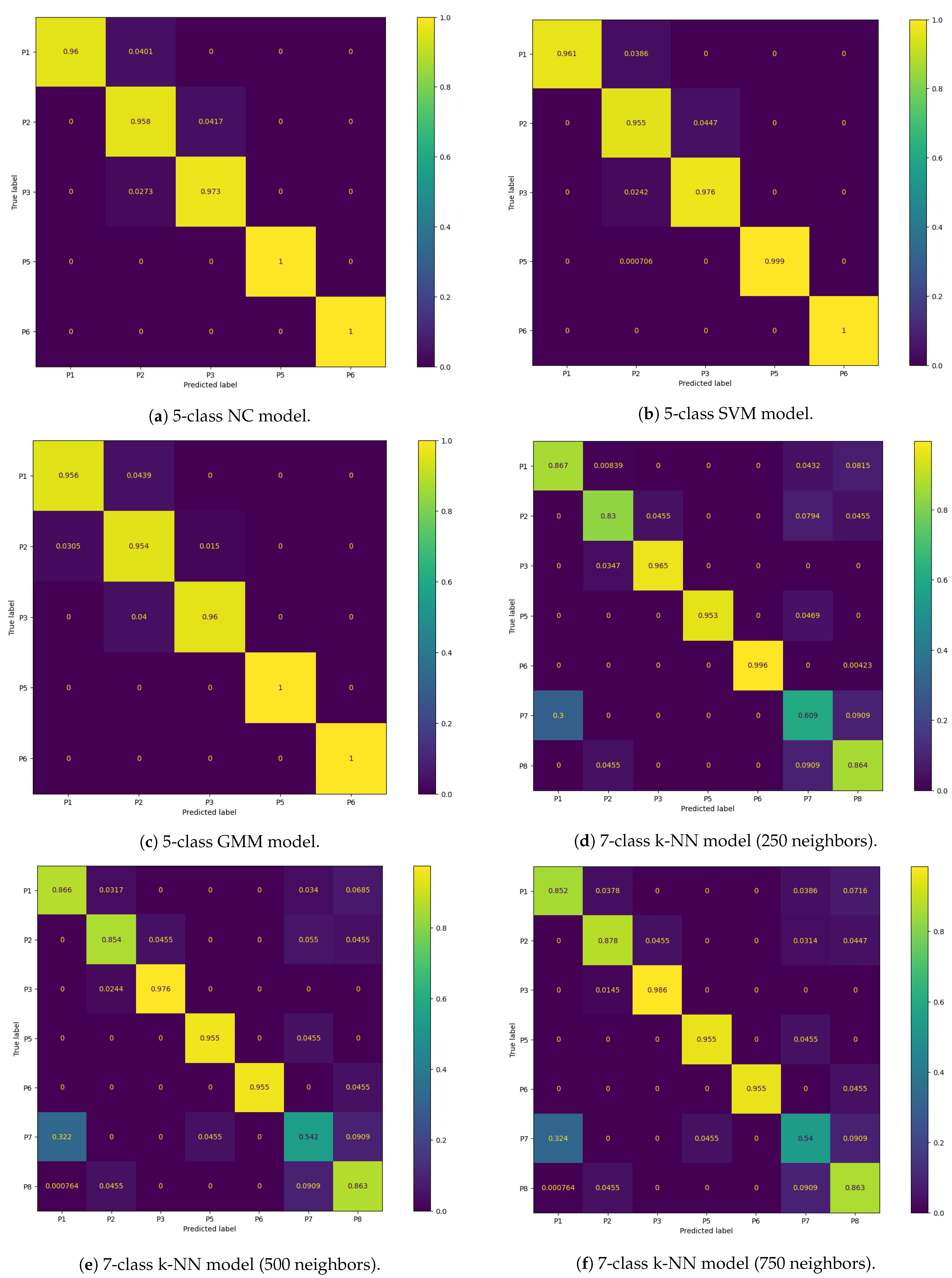
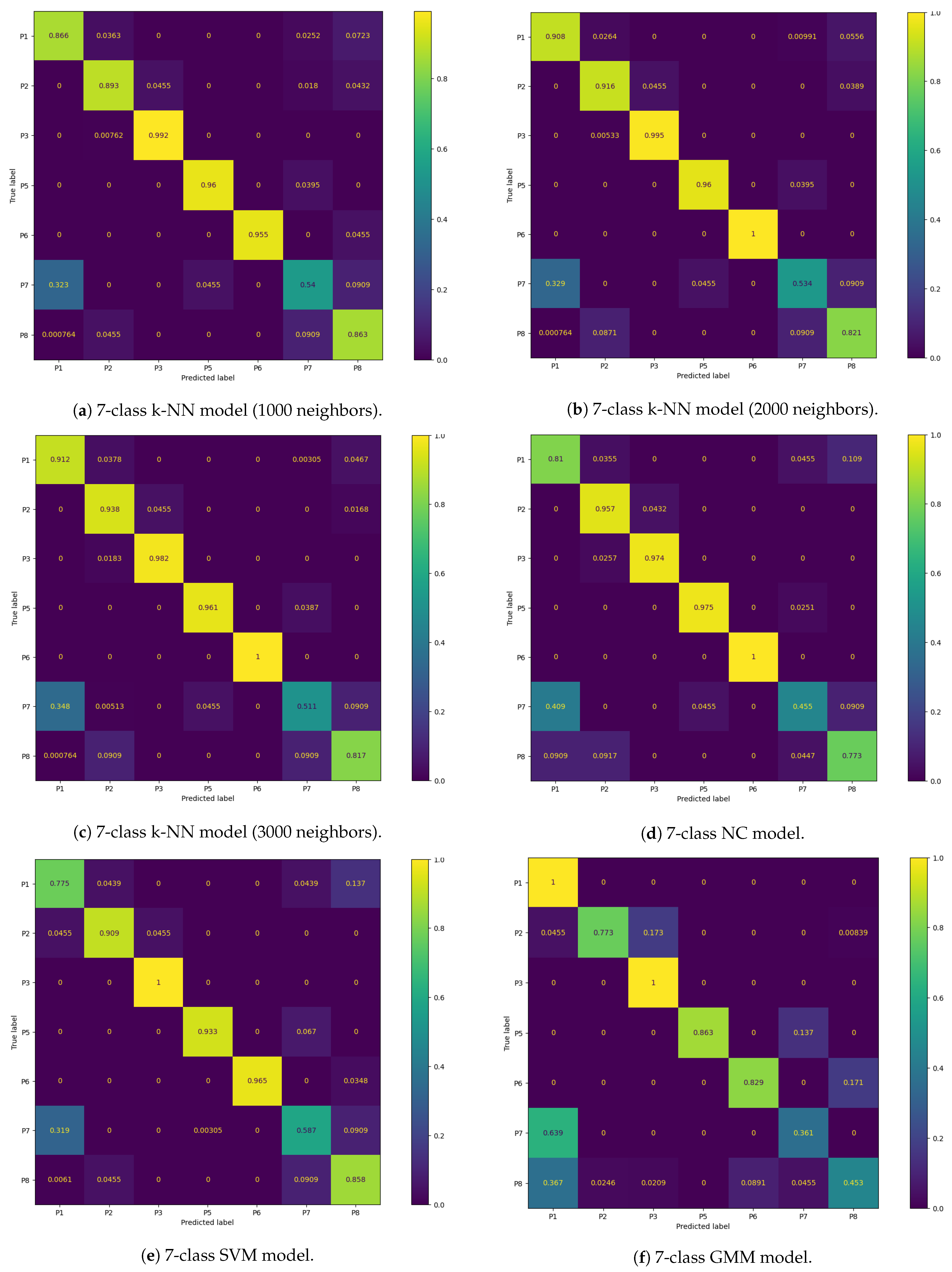
On the other hand, for the models trained to classify seven classes, there was a marked decreased in the overall accuracy comparatively to the validation accuracy, which was mostly caused by the misclassification of the P7 and P8 positions (the percentage of P7 and P8 samples labeled correctly ranged from 36.1% to 60.9% and 45.3% to 86.4%, respectively) and, to a lesser degree, of the P1 and P2 positions (77.5% to 100% and 77.3% to 93.8%, respectively). Again, this was expected due to the inherent overlap between the CM clusters of the P1/P2 and P7/P8 positions. However, overall, the classification performance metrics obtained for the supervised learning models were still satisfactory.
Furthermore, all seven-class supervised models had similar recall and precision values, leading to close F1-score values, which indicates that, on average, the classifiers’ ability to correctly label data from a specific sitting position was similar to their ability to not label data as a given sitting position which does not coincide with its true label. However, the higher standard deviation values of the precision and recall metrics compared to the five-class supervised models also indicate that the aforementioned abilities become significantly hampered for certain classes, in particular the added P7 and P8 positions, as can be seen from the bar plots displayed in
Appendix B.1.
The best performing classifiers for seven sitting positions were the k-NN models, with accuracy ranging from 85.8% to 87.6%. Similar to what occurred with five positions, these models exhibited better accuracy when using a higher number of neighbors, in particular 2000 (87.6%) and 3000 (87.5%), as this leads to the definition of more homogeneous decision areas (
Figure 9).
Overall, the models trained with seven sitting positions struggled in particular with the classification of P7 and P8 samples, but, while not as accurate, these models have a superior posture monitoring capacity compared to those only trained with five positions, which are consequently more limited in their implementation in a real-world environment and ability to verify dynamic sitting. As a result, the classifier chosen for the final prototype was the seven-class k-NN model with 3000 neighbors. While using 2000 neighbors with this model yielded a marginally better accuracy score, it was decided to use the model with 3000 neighbors instead, due to its higher accuracy for the P1 and P2 positions, which are the most commonly found sitting postures in the office environment among all of the evaluated positions (
Figure 8).
Table 7 shows the relative frequency of the predicted label in each transition period obtained from the final posture classifier chosen, averaged across all participants. With this final model, it was verified that, during the transition periods between sitting positions, the classification was for the most part stable, with the predicted label changing from the start to the end position. Only occasionally, the predicted label changed briefly to other positions, corresponding to periods where movement occurs during the changing of position, resulting in more or less weight being applied to certain load cells.
5. Discussion
As was mentioned in
Section 1, the focus of this work was to develop a SPMS and ECG signal acquisition module incorporated into an office chair, using an “invisible” sensing approach, and to validate and evaluate the performance of these modules. The main aim was to ensure that the system was able to record usable ECG signals and the posture classification approach taken (i.e., type and location of sensors, extracted features, classification model, evaluated sitting positions) was adequate, with accuracy surpassing or on par with other systems proposed in the literature.
For the evaluation of the proposed ECG acquisition scheme, several metrics were extracted from the signals acquired by this system and compared to those obtained by reference sensors. After the analysis of these results, we concluded that, although the proposed system is more prone to noise, the results are quite satisfactory. Even though systems that use an analogous RLD scheme are more robust to this noise, such as the one proposed by Su et al. (2021) [
14], who were able to achieve a SNR between 15.02 and 25.02 dB (depending on the placement of the conductive textile electrodes on the backrest), the majority of signals acquired with the ground-free system proposed in this work still maintained the morphology of the ECG signal, achieving a SNR as high as 12.17 dB.
Additionally, without outlier removal algorithms, the average performance and accuracy rates of ECG segmentation highlight this observation, with obtained results above 90% and 85%, respectively, demonstrating this system’s feasibility. However, as expected, some of the acquired signals were contaminated with intense noise, leading to erroneous R-peak detection and overestimation of the heart rate. In the system proposed by Silva et al. (2021) [
30], which used the same conductive nappa employed here (albeit wrapped around the main areas of a gaming keyboard armrest and mouse that come in contact with the hand), the average performance achieved was 99.99% and 95.83% when using two active electrodes on the keyboard armrest and one on the armrest with another on the mouse, respectively. However, the first value fell to 77.03% and 75.14% when subjects had low and high density skin moisturizers applied to their skin, respectively, leading us to conclude that these products could be a potential source of noise in the acquired signals.
Using three methods of outlier detection to the extracted heartbeat waveforms, we were able to mitigate this noise, leading to increased accuracy (ranging from around 5% to 10%) by discarding erroneously detected R-peaks in noisier segments of the signal. However, the performance also decreased (ranging from around 2% to 20%), due to the removal of correctly detected R-peaks in segments contaminated with noise. This decrease was dependent on the algorithms’ sensitivity to variance between heartbeat waveforms, with the obtained results corroborating previous studies that found DBSCAN to be the least sensitive and NCCC the most [
31,
35].
Nevertheless, the proposed ECG acquisition system was able to record usable signals, from which the heart rate, a metric that can be clinically relevant, can be accurately derived from. For example, this metric can be used to detect cardiac arrhythmias, especially when taking into consideration the “invisible” nature of this system, that allows for pervasive monitoring, as opposed to sporadic signal acquisition.
Additionally, this metric varies with both physical and cognitive exertion, leading to it being often treated as a surrogate for sympathetic activity and has also been found to be helpful to assess stress. Adding to this all the work conducted around the study of the heart rate variability, the heart rate has been successfully used for enhanced risk assessment in low- to intermediate-risk individuals without known coronary artery disease [
37].
It is also relevant to highlight that, at least in a first deployment stage, this type of system can aid in triage of potential cardiovascular disorders rather than performing a full-featured diagnosis. This is illustrated by recent developments on the detection of atrial fibrillation (the most common type of cardiac arrhythmia globally) from single-lead ECG recordings, exhibiting excellent diagnostic accuracy, such as the algorithms used by Apple and AliveCor [
38,
39], as well as a morphology-based deep learning model with visualization of the ECG segments most relevant for the detection of this pathology [
40]. Nevertheless, ultimately, the purpose of this ECG acquisition module is not to replace the medical professional, who is the best suited individual to diagnose cardiovascular disease, but to help their work by providing them with more data to aid in making a diagnosis.
For the SPMS proposed in this work, several posture classification models were created, trained and tested with novel datasets of CM coordinates in the 2D seat plane, in order to distinguish between five and seven sitting positions. Although the original dataset covered eight positions, the P4 position was excluded, as it was the only position to not form a cluster in the feature space. Several metrics (precision, recall, accuracy) were evaluated to find the best performing classification model, which turned out to be the k-NN model with 1000 and 3000 neighbors, for the five-class and seven-class models, respectively.
Compared with other sensory chair-based SPMSs proposed in the literature, the five-class model achieved superior classification accuracy results (
), which was to be expected taking into consideration the very little overlap between the clusters of these positions. Even high-precision SPMSs did not perform this well, such as the one proposed by Kim et al. (2018) [
26], who used a pressure sensor mat to generate heat map images of the body pressure distribution in the chair seat, with which to classify the same number of sitting positions using a deep learning model (CNN), achieving an accuracy of
.
On the other hand, the seven-class model exhibited decreased accuracy compared to the five-class ones, due to the overlap of P7 and P8 with the remaining positions. Even so, the classification accuracy achieved (
) did not deviate significantly from other SPMSs proposed in the literature, particularly for the postures most commonly adopted in the office workplace (P1 and P2). These results are a significant contribution to the state-of-the-art, especially, when taking into consideration the overall simpler approach taken in terms of sensor and computational complexity. For instance, the accuracy achieved by the high-precision SPMS proposed by Huang et al. (2017) [
18], which evaluated the same seven sitting positions considered in this work, with high-dimensional pressure maps of the chair seat, surpassed the one achieved by our system by only 5% approximately.
Furthermore, we found that even during transition periods between sitting positions, the classification with the best performing seven-class model was for the most part stable, highlighting this system’s capacity to evaluate dynamic sitting in the workplace. We also found that the execution time of this classifier was approximately milliseconds, when evaluating CM coordinates ranging from 0 to 30.3 cm in the X-axis and 0 to 26.1 cm in the Y-axis, with a 0.1 cm step, in the chair seat reference frame. Thus, this model has been found to be adequate for real-time posture classification in a future real world deployment.
Nevertheless, in the future, we plan to also increase this system’s posture monitoring capacity by evaluating more sitting positions, such as the one used by Roh et al. (2018) [
17], who achieved a high classification accuracy, using a SPMS similar to the one proposed in this work. Additionally, to try and increase the performance of posture classification, especially for the P7 and P8 positions, we will experiment adding new inexpensive sensors (e.g., infrared reflective distance sensors as proposed in [
20]) and features to the dataset.
As a final note, this is one of the first smart chair systems proposed in the literature, that integrates both validated sitting posture monitoring and ECG signal acquisition modules. The overall cost of the hardware required to develop this system is only approximately 150 euros, markedly less than most systems that only integrate posture monitoring (e.g., the CER2 CONFORMat sensor with 2048 sensing elements from Tekscan
™ used in some SPMSs is commercially available for USD 3000 [
41]), facilitating its large scale deployment in the future.
6. Conclusions
In this work, a smart chair system was developed, with integrated sitting posture monitoring and ECG signal acquisition, following an “invisible” sensing approach.
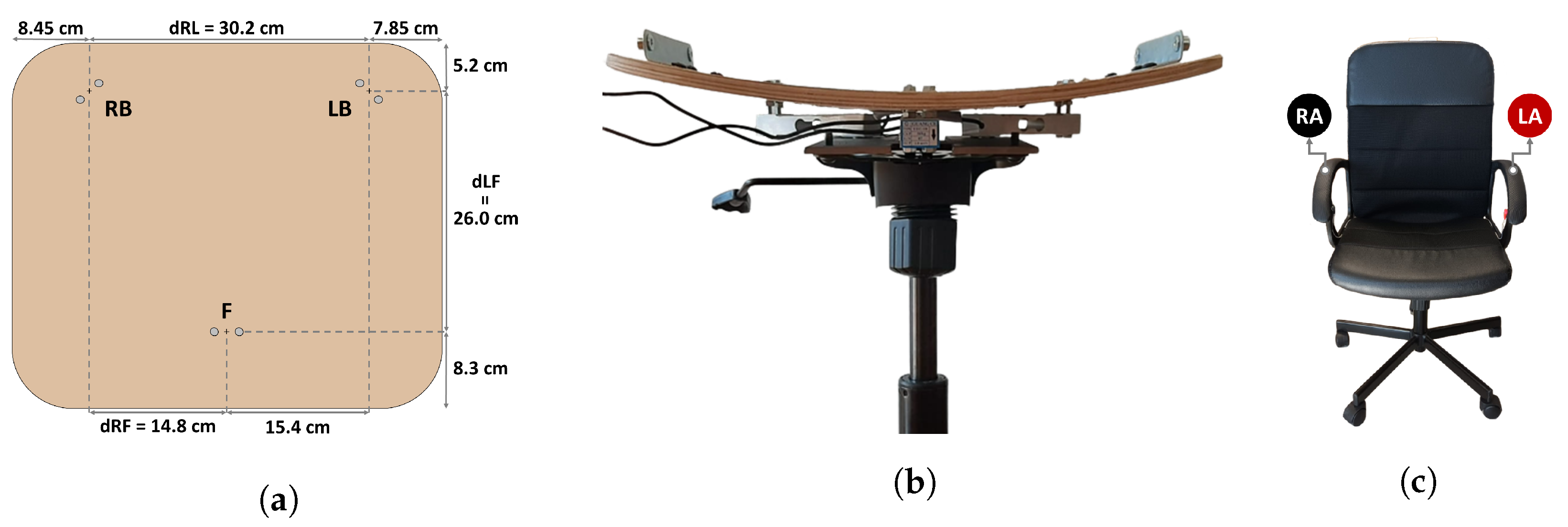
For posture monitoring, a sensory chair-based SPMS was developed using single point load cells integrated under the seat to measure the weight applied at specific points. Posture classification was performed using the CM coordinates computed from the average weight values, in a 1 second non-overlapping window, as feature vectors, which were found to form distinct clusters for seven of the eight evaluated sitting positions. Two datasets were created: one for training and the other for testing various classifiers, considering five or seven postures. For both five and seven-class models, the best performance was achieved by the k-NN model in all evaluated metrics, and, as expected, the five-class model had higher classification accuracy () than the seven-class (), as some positions considered by the latter (P7 and P8) have their CM in close proximity or overlapping the clusters of other positions (P1, P2, P5 and P6). In the end, the posture classifier chosen for the final prototype was the seven-class k-NN with 3000 neighbors, due to its higher classification accuracy for the P1 and P2 positions (commonly adopted by workers), and capability to identify a broader set of postures, making this prototype better suited to promote dynamic sitting.
Additionally, we were able to achieve these results using a much simpler approach both in terms of sensor and computational complexity compared to other SPMSs proposed in the literature, facilitating large scale deployment of the proposed system.
For ECG signal acquisition, results show that, while the signals acquired with the conductive nappa had decreased quality comparatively to the reference, they still maintained the morphology of the ECG signal for the most part, and, while certain noise sources could not be removed with filtering, using DBSCAN lead to an increase in R-peak detection accuracy that compensated the loss in performance.
In conclusion, the aforementioned experimental results indicate that the smart chair system proposed in this work is both feasible and well performing in its various monitoring modules. Despite the results obtained, future work will seek to further increase the performance of the various subsystems and facilitate the incorporation of the developed smart chair into the office environment. This includes: experimenting with other inexpensive sensors (e.g., infrared distance sensors) and adding new features to the dataset, to try and increase the posture classification accuracy and include more sitting positions; the development of a platform to wirelessly charge the smart chair, guaranteeing its complete independence from cabled connections to external devices; incorporating ECG leads-off detection at the hardware level, so as to avoid needless continuous ECG signal acquisition, which will occur as a natural extension of the user’s normal sitting activities; development of a web app to provide feedback to the user on their sitting posture and cardiovascular health, using the sensor data wirelessly transmitted by the SENSE to a real-time database, where they are processed on arrival and extracted metrics are stored; and usability experiments.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

















