

Assessment System for Child Head Injury from Falls Based on Neural Network Learning


Abstract
:1. Introduction
- A two-stage deep-learning-based architecture for high-precision detection is proposed. The LSTM neural network and 3D transform model can correct the coordinates of the omitted 2D skeleton points and derive the 3D stereo coordinates by combining the spatial and temporal information of the key points. We hope to decrease missed or inaccurate detections brought on by complicated environments, small target sizes, and density distributions. It seeks to bring intelligent child fall in-injury assessments one step closer to being convenient and speedy.
- A HIC-based approach for classifying damage degree is developed based on the triaxial acceleration of the human head center drop.
- A dataset of 500 video clips of children’s falls is generated using 200 real-time daily videos, and another test set of 300 video clips is used to evaluate the performance of the system. These videos encompass a range of lighting conditions, camera settings, and interior furnishings. It levels the dataset’s diversity and boosts the framework’s generalization ability.
- The feasibility of a real-time AI technique for assessing head injuries in falls is proven. After future upgrades and optimizations, it is implementable on hardware platforms such as intelligent surveillance cameras.
2. The Proposed Method
2.1. Open Pose Obtains Human Body Skeleton Information
2.2. 2D Key Points Inspection and Repair
| Algorithm 1: Correction of Skeleton Key Point Coordinates |
| Input: Bone point coordinate matrix’F’, size’ Output: Procedure: 1: Input: Enter key point data’F’; 2: Forget gate: is 0 or 1 If = 0, The input value is reserved Else: The input value is forgotten; 3: Input gate: By the sigmoid and tanh functions, determines the value affecting ; 4: Output gate: By the sigmoid function, output , then ; 5: Combine T results for linear regression and out the missing point’s coordinates. |
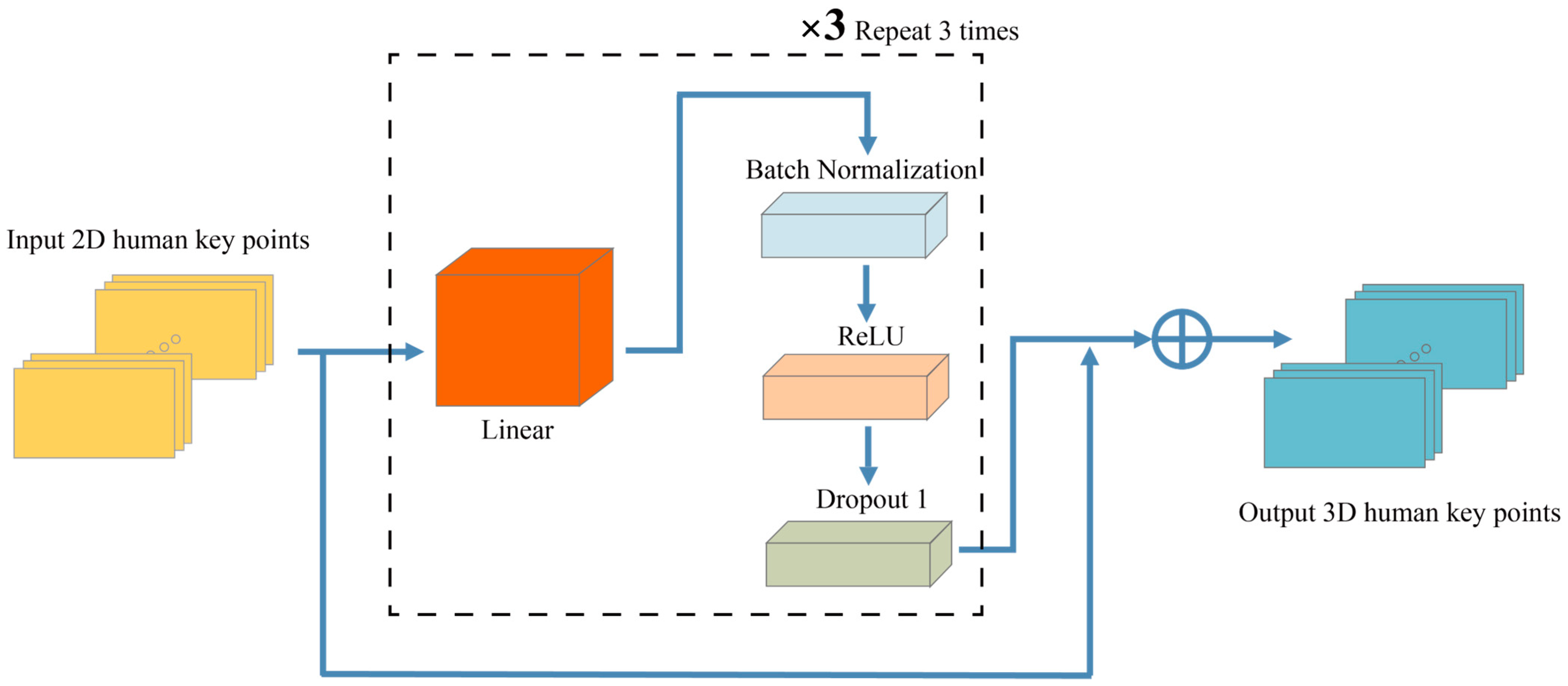
2.3. Map 2D Key Joint to 3D Positions
| Algorithm 2: Convert 2D to 3D coordinates |
| Input: 2D bone point coordinates Output: 1: Enter the linear layer and increase its dimension by 1024; 2: Standardize for batch processing and discard; 3: Enter ReLUs for activation processing; 4: Select the Z value with the minor error from it; 5: Entering the linear layer once more, generating an output of size 3 n; 6: Combine with input and output the result. |
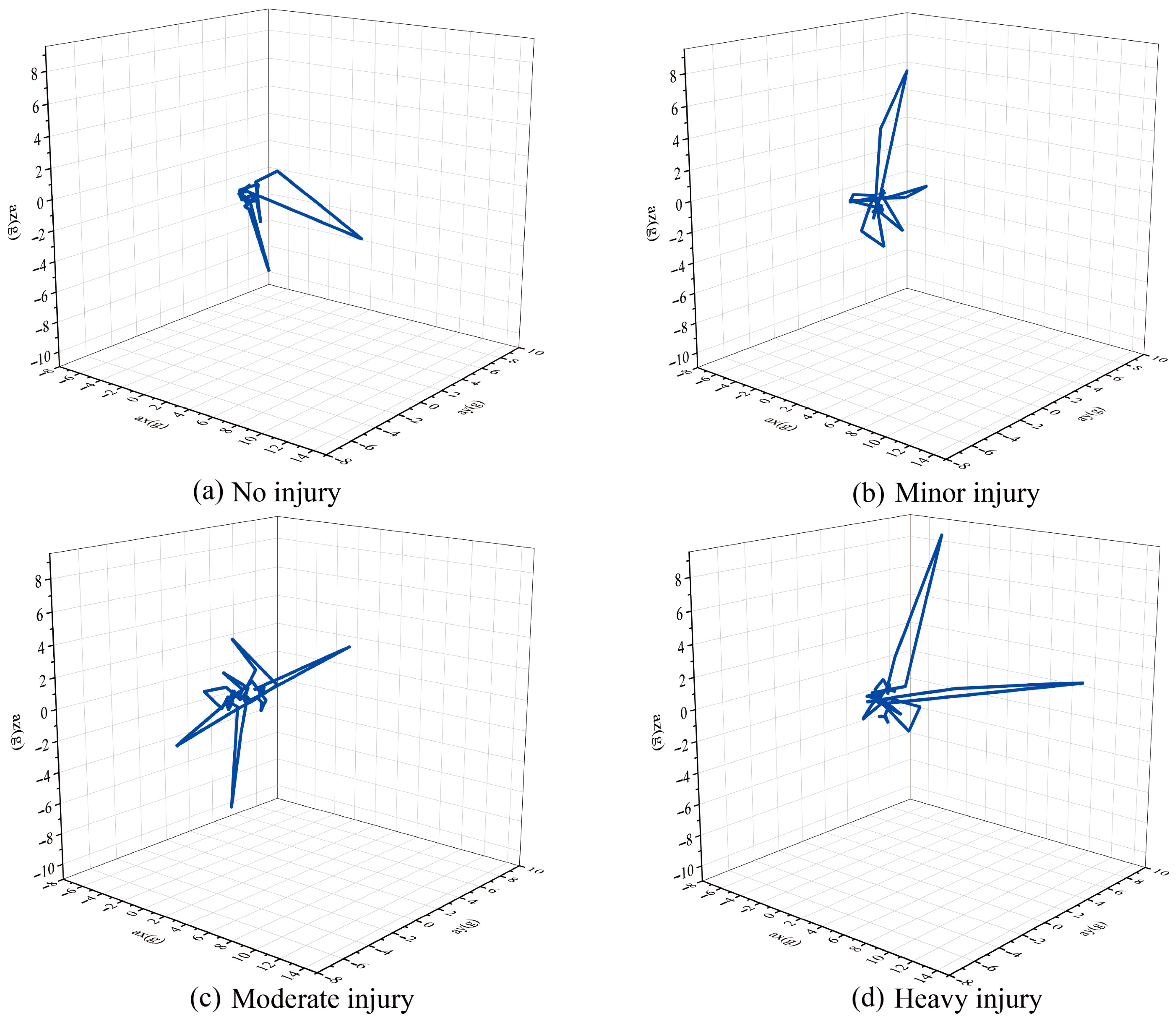
2.4. Values Calculated for Head Injuries
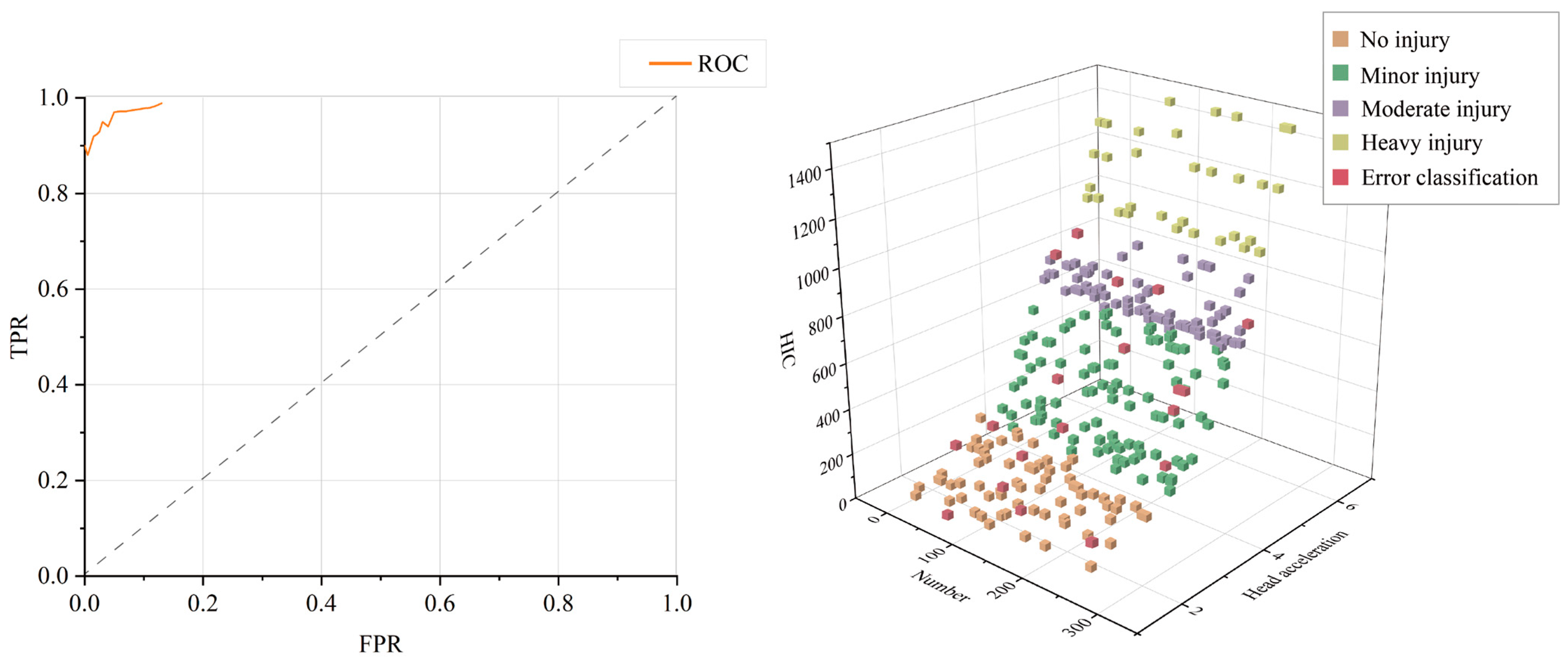
2.5. Classification Based on Machine Learning
3. Experimental Setup
3.1. Dataset and Test
3.2. Experimental Results Analysis
4. Discussions
- As we are using home environment monitoring, some interior furnishings obstruct the camera angles, resulting in insufficient data due to the absence of key joints. We will optimize the ability of our framework to repair small-size toddlers’ skeleton joints.
- Since our framework needs to be uploaded to the server for processing, we should also perform real-time optimization to increase the model’s inference efficiency. Throughout each iteration, the convergence rate of the optimization techniques should be improved.
- Our framework does not allow us to deduce how the stiffness of the ground affects the severity of injury. AI ground hardness identification via visual detection and the effect on the harm value is required in the coming work.
- In practice, it is necessary to determine whether a fall has occurred before deciding the presence of a head injury. So, a vision-based fall detection system is required in the framework in the future.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RGB | Red, green, blue |
| RNN | Recurrent Neural Network |
| LSTM | Long short-term memory |
| GRU | Gate Recurrent Unit |
| STGCN | Spatio-Temporal Graph Convolutional Network |
| CNN | Convolution neural network |
| FEM | Finite element method |
| WSM | Wearable sensor-based method |
| DANN | Deep Adversarial Neural Network |
| HIC | Head Impact Criteria |
| SIMG | Sensor-laden headbands |
| ReLU | Rectified Linear Unit |
| SVM | Support vector machine |
| RBF | Radial basis function |
| RF | Random forest |
| DT | Decision tree |
References
- Brown, C.W.; Akbar, S.P.; Cooper, J.G. Things that go bump in the day or night: The aetiology of infant head injuries presenting to a Scottish Paediatric Emergency Department. Eur. J. Emerg. Med. 2014, 21, 447–450. [Google Scholar] [CrossRef] [PubMed]
- Clayton, J.L.; Harris, M.B.; Weintraub, S.L.; Marr, A.B.; Timmer, J.; Stuke, L.E.; Mcswain, N.E.; Duchesne, J.C.; Hunt, J.P. Risk factors for cervical spine. Injury 2012, 43, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Crowe, L.M.; Catroppa, C.; Anderson, V.; Babl, F.E. Head injuries in children under 3 years. Inj.-Int. J. Care Inj. 2012, 43, 2141–2145. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.T.; Li, Z.; Li, Z.B. Maxillofacial Injuries in Infants and Preschools: A 2.5-Year Study. J. Craniofacial Surg. 2014, 25, 964–967. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, X.B.; Kan, S.L.; Ning, G.Z.; Li, Y.L.; Yang, B.; Li, Y.; Sun, J.C.; Feng, S.Q. Traumatic spinal cord injury in Tianjin, China: A single-center report of 354 cases. Spinal Cord 2016, 54, 670–674. [Google Scholar] [CrossRef]
- National Center for Chronic and Noncommunicable; Disease Control and Prevention China CDC, B. Review of Chinese Children and Adolescents; People’s Health Electronic Audio and Video Publishing House: Beijing, China, 2018; pp. 2–3.
- Flavin, M.P.; Dostaler, S.M.; Simpson, K.; Brison, R.J.; Pickett, W. Stages of development and injury patterns in the early years: A population-based analysis. BMC Public Health 2006, 6, 10. [Google Scholar] [CrossRef]
- Bertocci, G.; Smalley, C.; Brown, N.; Dsouza, R.; Hilt, B.; Thompson, A.; Bertocci, K.; McKinsey, K.; Cory, D.; Pierce, M.C. Head biomechanics of video recorded falls involving children in a childcare setting. Sci. Rep. 2022, 12, 13. [Google Scholar] [CrossRef]
- Kakara, H.; Nishida, Y.; Yoon, S.M.; Miyazaki, Y.; Koizumi, Y.; Mizoguchi, H.; Yamanaka, T. Development of childhood fall motion database and browser based on behavior measurements. Accid. Anal. Prev. 2013, 59, 432–442. [Google Scholar] [CrossRef]
- He, J.Y.; Yan, J.W.; Margulies, S.; Coats, B.; Spear, A.D. An adaptive-remeshing framework to predict impact-induced skull fracture in infants. Biomech. Model. Mechanobiol. 2020, 19, 1595–1605. [Google Scholar] [CrossRef]
- Hu, J.; Li, Z.; Zhang, J. Development and Preliminary Validation of a Parametric Pediatric Head Finite Element Model for Population-Based Impact Simulations. In Proceedings of the Asme Summer Bioengineering Conference, Farmington, PA, USA, 22–25 June 2011. [Google Scholar]
- Thompson, A.; Bertocci, G. Pediatric bed fall computer simulation model: Parametric sensitivity analysis. Med. Eng. Phys. 2014, 36, 110–118. [Google Scholar] [CrossRef]
- Fahlstedt, M.; Kleiven, S.; Li, X.G. Current playground surface test standards underestimate brain injury risk for children. J. Biomech. 2019, 89, 1–10. [Google Scholar] [CrossRef] [PubMed]
- D’Orazio, T.; Marani, R.; Reno, V.; Cicirelli, G. Recent trends in gesture recognition: How depth data has improved classical approaches. Image Vis. Comput. 2016, 52, 56–72. [Google Scholar] [CrossRef]
- Uddin, M.K.; Bhuiyan, A.; Bappee, F.K.; Islam, M.M.; Hasan, M. Person Re-Identification with RGB-D and RGB-IR Sensors: A Comprehensive Survey. Sensors 2023, 23, 29. [Google Scholar] [CrossRef] [PubMed]
- Shafay, M.; Ahmad, R.W.; Salah, K.; Yaqoob, I.; Jayaraman, R.; Omar, M. Blockchain for deep learning: Review and open challenges. Clust. Comput.-J. Netw. Softw. Tools Appl. 2023, 26, 197–221. [Google Scholar] [CrossRef]
- Shoaib, M.; Bosch, S.; Incel, O.D.; Scholten, H.; Havinga, P.J.M. Fusion of Smartphone Motion Sensors for Physical Activity Recognition. Sensors 2014, 14, 10146–10176. [Google Scholar] [CrossRef]
- Yang, C.G.; Chen, C.Z.; He, W.; Cui, R.X.; Li, Z.J. Robot Learning System Based on Adaptive Neural Control and Dynamic Movement Primitives. IEEE Trans. Neural Netw. Learn. Syst. 2019, 30, 777–787. [Google Scholar] [CrossRef]
- Girshick, R.; Donahue, J.; Darrell, T.; Malik, J.; IEEE. Rich feature hierarchies for accurate object detection and semantic segmentation. In Proceedings of the 27th IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Columbus, OH, USA, 23–28 June 2014; pp. 580–587. [Google Scholar]
- Wu, W.W.; Tu, F.B.; Niu, M.Q.; Yue, Z.H.; Liu, L.B.; Wei, S.J.; Li, X.Y.; Hu, Y.; Yin, S.Y. STAR: An STGCN ARchitecture for Skeleton-Based Human Action Recognition. IEEE Trans. Circuits Syst. I-Regul. Pap. 2023, 70, 2370–2383. [Google Scholar] [CrossRef]
- Amsaprabhaa, M.; Jane, Y.N.; Nehemiah, H.K. Multimodal spatiotemporal skeletal kinematic gait feature fusion for vision-based fall detection. Expert Syst. Appl. 2023, 212, 15. [Google Scholar] [CrossRef]
- Geun, S.B.; Ho, K.U.; Woo, L.S.; Young, Y.J.; Wongyum, K. Fall Detection Based on 2-Stacked Bi-LSTM and Human-Skeleton Keypoints of RGBD Camera. KIPS Trans. Softw. Data Eng. 2021, 10, 491–500. [Google Scholar]
- Han, K.; Yang, Q.Q.; Huang, Z.F. A Two-Stage Fall Recognition Algorithm Based on Human Posture Features. Sensors 2020, 20, 21. [Google Scholar] [CrossRef]
- Lin, C.B.; Dong, Z.; Kuan, W.K.; Huang, Y.F.J.A.S. A Framework for Fall Detection Based on OpenPose Skeleton and LSTM/GRU Models. Appl. Sci. 2020, 11, 329. [Google Scholar] [CrossRef]
- Anh, L.H.; Nguyen, P.T.L.; Vu, N.A. Effects of Impact Location, Impact Angle and Impact Speed on Head Injury Risk of Vietnamese Pedestrian Hit by a Sedan. Int. J. Automot. Technol. 2023, 24, 411–420. [Google Scholar] [CrossRef]
- Zhou, C.M.; Huang, T.; Luo, X.; Kaner, J.; Fu, X.M. Cluster analysis of kitchen cabinet operation posture based on OpenPose technology. Int. J. Ind. Ergon. 2022, 91, 12. [Google Scholar] [CrossRef]
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef] [PubMed]
- Shafiq, M.; Gu, Z.Q. Deep Residual Learning for Image Recognition: A Survey. Appl. Sci. 2022, 12, 43. [Google Scholar] [CrossRef]
- Mellander, H. HIC-the head injury criterion. Practical significance for the automotive industry. Acta Neurochir. Suppl. 1986, 36, 18–20. [Google Scholar]
- Long, K.J.; Gao, Z.B.; Yuan, Q.; Xiang, W.; Hao, W. Safety evaluation for roadside crashes by vehicle-object collision simulation. Adv. Mech. Eng. 2018, 10, 12. [Google Scholar] [CrossRef]
- Wang, F.; Wang, Z.; Hu, L.; Xu, H.Z.; Yu, C.; Li, F. Evaluation of Head Injury Criteria for Injury Prediction Effectiveness: Computational Reconstruction of Real-World Vulnerable Road User Impact Accidents. Front. Bioeng. Biotechnol. 2021, 9, 16. [Google Scholar] [CrossRef]
- Kimpara, H.; Iwamoto, M. Mild Traumatic Brain Injury Predictors Based on Angular Accelerations During Impacts. Ann. Biomed. Eng. 2012, 40, 114–126. [Google Scholar] [CrossRef]
- Thompson, A.K.; Bertocci, G.E. Paediatric bed fall computer simulation model development and validation. Comput. Methods Biomech. Biomed. Eng. 2013, 16, 592–601. [Google Scholar] [CrossRef]
- Kendrick, D.; Maula, A.; Reading, R.; Hindmarch, P.; Coupland, C.; Watson, M.; Hayes, M.; Deave, T. Risk and Protective Factors for Falls From Furniture in Young Children Multicenter Case-Control Study. JAMA Pediatr. 2015, 169, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Belgiu, M.; Drăguţ, L. Random forest in remote sensing: A review of applications and future directions. J. Photogramm. Remote Sens. 2016, 114, 24–31. [Google Scholar] [CrossRef]
- Rodriguez-Galiano, V.F.; Ghimire, B.; Rogan, J.; Chica-Olmo, M.; Rigol-Sanchez, J.P. An assessment of the effectiveness of a random forest classifier for land-cover classification. ISPRS-J. Photogramm. Remote Sens. 2012, 67, 93–104. [Google Scholar] [CrossRef]
- Liaw, A.; Wiener, M.J.R.N. Classification and Regression by randomForest. R News 2002, 23, 18–22. [Google Scholar]
- Jiang, P.; Lu, H.X.; Liu, Z.B. Drugs Identification Using Near-Infrared Spectroscopy Based on Random Forest and CatBoost. Spectrosc. Spectr. Anal. 2022, 42, 2148–2155. [Google Scholar] [CrossRef]
- Chen, F.X.; Yang, T.W.; Li, J.Q.; Liu, H.G.; Fan, M.P.; Wang, Y.Z. Identification of Boletus Species Based on Discriminant Analysis of Partial Least Squares and Random Forest Algorithm. Spectrosc. Spectr. Anal. 2022, 42, 549–554. [Google Scholar] [CrossRef]
- Lin, X.W.; Wang, L.Q.; Zeng, Y.G.; Chen, Y.Z.; Wang, M.Y.; Zhong, J.P.; Wang, X.H.; Xiong, H.L.; Chen, Y. Random Forest Retinal Segmentation in OCT Images Based on Principal Component Analysis. Prog. Biochem. Biophys. 2021, 48, 336–343. [Google Scholar] [CrossRef]
- dos Santos, C.M.; Escobedo, J.F.; Teramoto, E.T.; da Silva, S. Assessment of ANN and SVM models for estimating normal direct irradiation (H-b). Energy Convers. Manag. 2016, 126, 826–836. [Google Scholar] [CrossRef]
- Li, X.; Gao, W.K.; Gu, L.X.; Gong, C.L.; Jing, Z.; Su, H. A cooperative radial basis function method for variable-fidelity surrogate modeling. Struct. Multidiscip. Optim. 2017, 56, 1077–1092. [Google Scholar] [CrossRef]
- Aburomman, A.A.; Reaz, M.B. A novel weighted support vector machines multiclass classifier based on differential evolution for intrusion detection systems. Inf. Sci. 2017, 414, 225–246. [Google Scholar] [CrossRef]
- Chauhan, V.K.; Dahiya, K.; Sharma, A. Problem formulations and solvers in linear SVM: A review. Artif. Intell. Rev. 2019, 52, 803–855. [Google Scholar] [CrossRef]
- Tian, Y.J.; Shi, Y.; Liu, X.H. Recent advances on support vector machines research. Technol. Econ. Dev. Econ. 2012, 18, 5–33. [Google Scholar] [CrossRef]
- Singla, M.; Shukla, K.K. Robust statistics-based support vector machine and its variants: A survey. Neural Comput. Appl. 2020, 32, 11173–11194. [Google Scholar] [CrossRef]
- Jiang, Q.H.; Zhu, L.L.; Shu, C.; Sekar, V. An efficient multilayer RBF neural network and its application to regression problems. Neural Comput. Appl. 2022, 34, 4133–4150. [Google Scholar] [CrossRef]
- Dusenberry, M.W.; Brown, C.K.; Brewer, K.L. Artificial neural networks: Predicting head CT findings in elderly patients presenting with minor head injury after a fall. Am. J. Emerg. Med. 2017, 35, 260–267. [Google Scholar] [CrossRef]
- Sinha, M.; Kennedy, C.S.; Ramundo, M.L. Artificial neural network predicts CT scan abnormalities in pediatric patients with closed head injury. J. Trauma-Inj. Infect. Crit. Care 2001, 50, 308–312. [Google Scholar] [CrossRef]
- Yhdego, H.; Li, J.; Morrison, S.; Audette, M.; Paolini, C.; Sarkar, M.; Okhravi, H.; IEEE. Towards musculoskeletal simulation-aware fall injury mitigation: Transfer learning with deep cnn for fall detection. In Proceedings of the Spring Simulation Conference (SpringSim), Tucson, AZ, USA, 29 April–2 May 2019. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Head Injury Criterion | Injury Type |
|---|---|
| 250 | cerebral concussion |
| 700 | Serious injury probability: 5% (Ais = 4) |
| 1000 | The probability of developing a malignant skull fracture: 33% |
| Head Injury Criterion | Injury Type |
|---|---|
| α < 250 | No injury |
| 250 < α < 700 | Minor injury |
| 700 < α < 1000 | Moderate injury skull fracture: 33% |
| 1000 < α | Heavy injury |
| Sensitivity | Specificity | Accuracy | Precision | F-Score | |
|---|---|---|---|---|---|
| LibSVM | 92.38% | 96.67% | 93.67% | 98.48% | 95.33% |
| RBF | 91.43% | 94.44% | 92.33% | 97.46% | 94.35% |
| RF | 96.19% | 97.78% | 96.67% | 99.02% | 97.58% |
| Reference | Theme | Dataset | Approach | Accuracy |
|---|---|---|---|---|
| Dusenberry et al. [48] | predict head injury | self-built | ANN | 93.14% |
| M Sinha et al. [49] | predict head injury | self-built | ANN | 94.3% |
| Yhdego et al. [50] | fall detection | self-built | Sensor data + CNN | 96.43% |
| Amsaprabhaa et al. [21] | vision-based fall detection | URFD, self-built | STGCN+1D-CNN | 96.53%, 95.8% |
| Ours | head injury assessment | self-built | LSTM+3D transform model | 96.67% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Z.; Tsui, B.; Wu, Z. Assessment System for Child Head Injury from Falls Based on Neural Network Learning. Sensors 2023, 23, 7896. https://doi.org/10.3390/s23187896
Yang Z, Tsui B, Wu Z. Assessment System for Child Head Injury from Falls Based on Neural Network Learning. Sensors. 2023; 23(18):7896. https://doi.org/10.3390/s23187896
Chicago/Turabian StyleYang, Ziqian, Baiyu Tsui, and Zhihui Wu. 2023. "Assessment System for Child Head Injury from Falls Based on Neural Network Learning" Sensors 23, no. 18: 7896. https://doi.org/10.3390/s23187896
APA StyleYang, Z., Tsui, B., & Wu, Z. (2023). Assessment System for Child Head Injury from Falls Based on Neural Network Learning. Sensors, 23(18), 7896. https://doi.org/10.3390/s23187896