
A Bedside Method for Measuring Effects of a Sedative Drug on Cerebral Function in Newborn Infants
 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
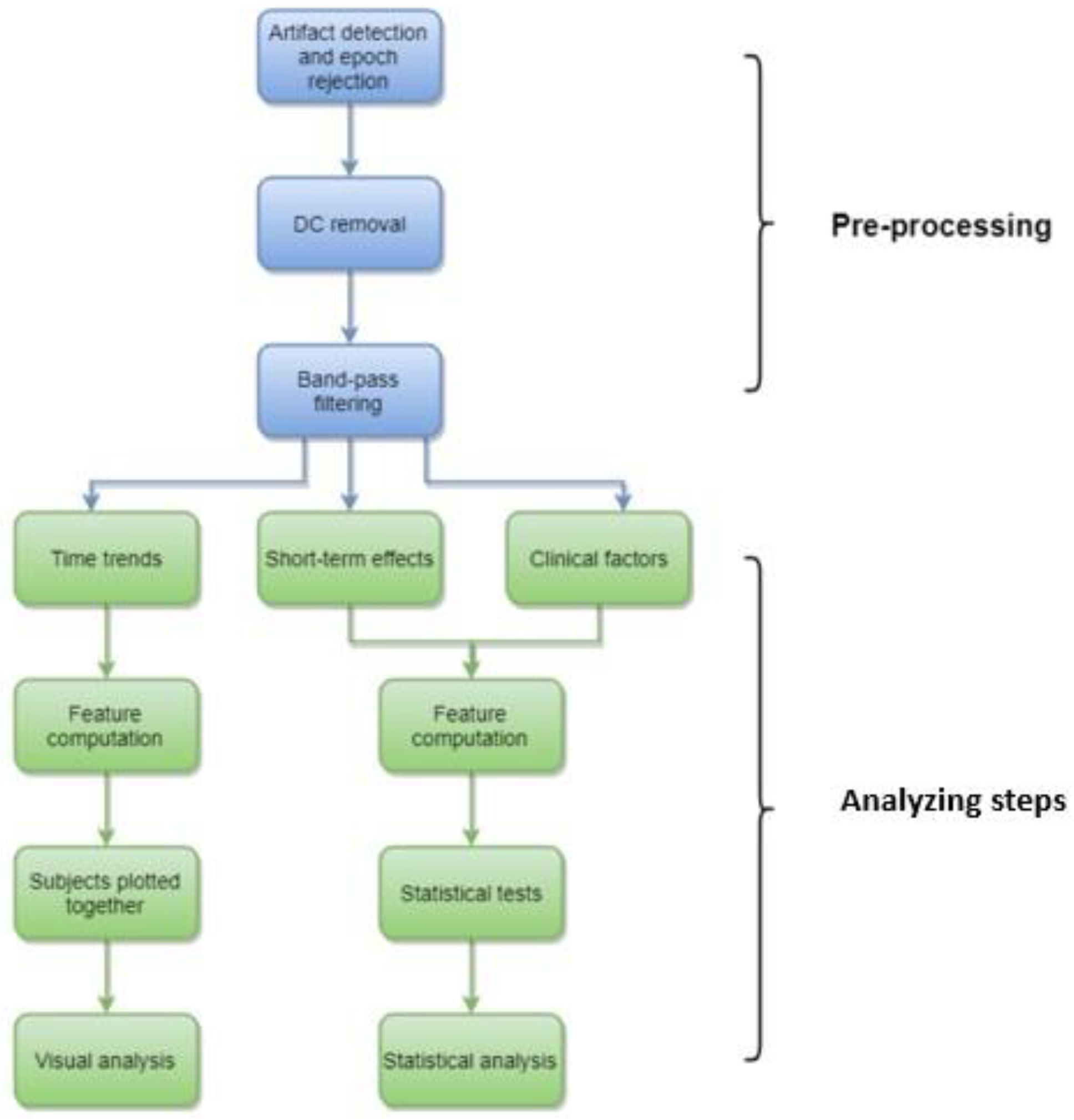
2.1. Computational Analyses
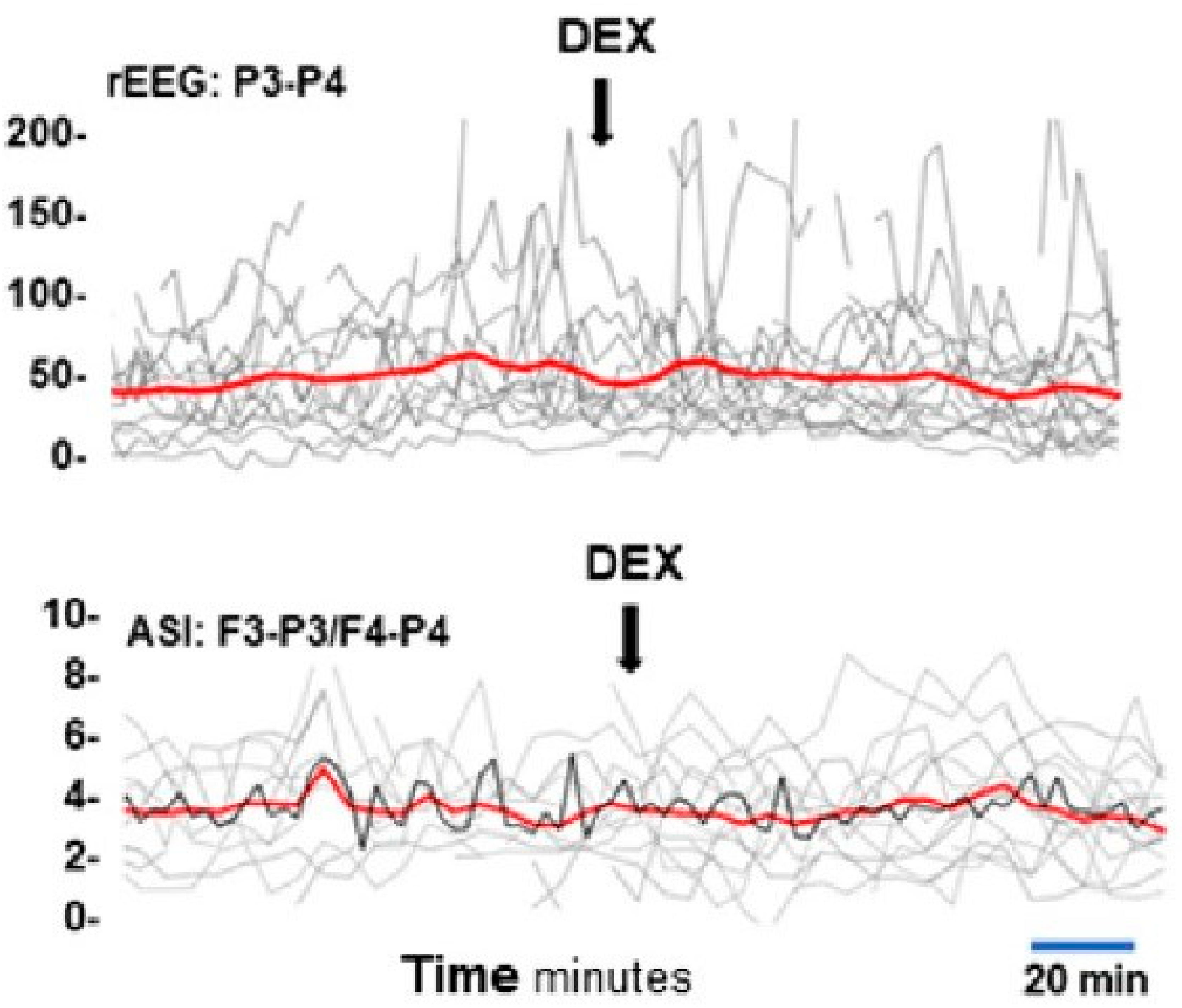
- Long-term effects
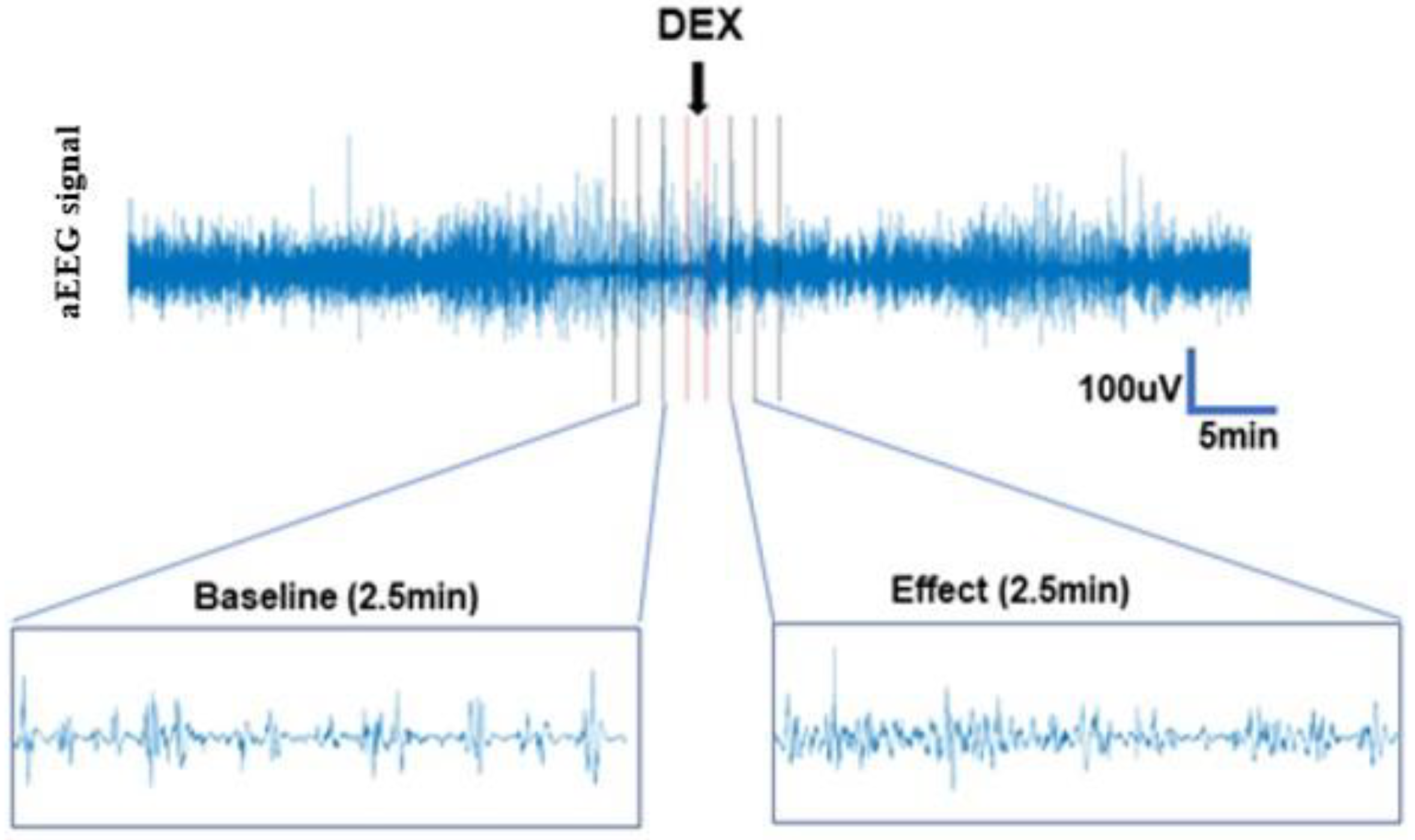
- Short-term effects
- Clinical factors
2.1.1. Long-Term Effects
2.1.2. Short-Term Effects
2.1.3. Clinical Factors
2.2. Statistical Analyses
3. Results
3.1. Long-Term Effects
3.2. Short-Term Effects
3.3. Clinical Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| aEEG | Amplitude-integrated EEG |
| ASI | Activation Synchrony Index |
| DEX | Dexmedetomidine |
| EEG | Electroencephalography |
| EMA | European Medicines Agency |
| GA | Gestational Age |
| NICU | Neonatal Intensive Care Unit |
| NIRS | Near-infrared Spectroscopy |
| rEEG | Range EEG |
References
- Brummelte, S.; Grunau, R.E.; Chau, V.; Poskitt, K.J.; Brant, R.; Vinall, J.; Ba, J.V.; Gover, A.; Synnes, A.R.; Miller, S. Procedural pain and brain development in premature newborns. Ann. Neurol. 2012, 71, 385–396. [Google Scholar] [CrossRef]
- Ranger, M.; Grunau, R.E. Early repetitive pain in preterm infants in relation to the developing brain. Pain Manag. 2014, 4, 57–67. [Google Scholar] [CrossRef]
- Schneider, J.; Duerden, E.G.; Guo, T.; Ng, K.; Hagmann, P.; Graz, M.B.; Grunau, R.E.; Chakravarty, M.M.; Hüppi, P.; Truttmann, A.C.; et al. Procedural pain and oral glucose in preterm neonates: Brain development and sex-specific effects. Pain 2017, 159, 515–525. [Google Scholar] [CrossRef]
- Doesburg, S.M.; Chau, C.M.; Cheung, T.P.; Moiseev, A.; Ribary, U.; Herdman, A.T.; Miller, S.P.; Cepeda, I.L.; Synnes, A.; Grunau, R.E. Neonatal pain-related stress, functional cortical activity and visual-perceptual abilities in school-age children born at extremely low gestational age. Pain 2013, 154, 1946–1952. [Google Scholar] [CrossRef]
- Bajic, D.; Commons, K.G.; Soriano, S.G. Morphine-enhanced apoptosis in selective brain regions of neonatal rats. Int. J. Dev. Neurosci. 2013, 31, 258–266. [Google Scholar] [CrossRef]
- Zwicker, J.G.; Miller, S.P.; Grunau, R.E.; Chau, V.; Brant, R.; Studholme, C.; Liu, M.; Synnes, A.; Poskitt, K.J.; Stiver, M.L.; et al. Smaller Cerebellar Growth and Poorer Neurodevelopmental Outcomes in Very Preterm Infants Exposed to Neonatal Morphine. J. Pediatr. 2016, 172, 81–87.e2. [Google Scholar] [CrossRef]
- Tataranno, M.L.; Gui, L.; Hellström-Westas, L.; Toet, M.; Groenendaal, F.; Claessens, N.H.P.; Schuurmans, J.; Sävman, K.; de Vrie, L.S. Morphine affects brain activity and volumes in preterms: An observational multi-center study. Early Hum Dev. 2020, 144, 104970. [Google Scholar] [CrossRef]
- Keating, G.M. Dexmedetomidine: A Review of Its Use for Sedation in the Intensive Care Setting. Drugs 2015, 75, 1119–1130. [Google Scholar] [CrossRef]
- Hunseler, C.; Balling, G.; Rohlig, C.; Blickheuser, R.; Trieschmann, U.; Lieser, U.; Dohna-Schwake, C.; Gebauer, C.; Möller, O.; Hering, F.; et al. Continuous infusion of clonidine in ventilated newborns and infants: A randomized controlled trial. Pediatr Crit Care Med. 2014, 15, 511–522. [Google Scholar] [CrossRef]
- Sellas, M.N.; Kyllonen, K.C.; Lepak, M.R.; Rodriguez, R.J. Dexmedetomidine for the Management of Postoperative Pain and Sedation in Newborns. J. Pediatr. Pharmacol. Ther. 2019, 24, 227–233. [Google Scholar] [CrossRef]
- Union, E. Regulation (EC) No 1901/2006 of the European Parliament and of the Council of 12 December 2006 on Medicinal Products for Paediatric Use and Amending Regulation (EEC) No 1768/92, Directive 2001/20/EC, Directive 2001/83/EC and Regulation (EC) No 726/2004. Available online: http://data.europa.eu/eli/reg/2006/1901/2019-01-282006 (accessed on 15 November 2022).
- Norman, E.; Wikstrom, S.; Rosen, I.; Fellman, V.; Hellström-Westas, L. Premedication for intubation with morphine causes prolonged depression of electrocortical background activity in preterm infants. Pediatr. Res. 2012, 73, 87–94. [Google Scholar] [CrossRef][Green Version]
- Malk, K.; Metsäranta, M.; Vanhatalo, S. Drug effects on endogenous brain activity in preterm babies. Brain Dev. 2014, 36, 116–123. [Google Scholar] [CrossRef]
- Bernet, V.; Latal, B.; Natalucci, G.; Doell, C.; Ziegler, A.; Wohlrab, G. Effect of sedation and analgesia on postoperative amplitude-integrated EEG in newborn cardiac patients. Pediatr. Res. 2010, 67, 650–655. [Google Scholar] [CrossRef]
- Cortes-Ledesma, C.; Arruza, L.; Sainz-Villamayor, A.; Martínez-Orgado, J. Dexmedetomidine affects cerebral activity in preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2022. [Google Scholar]
- Hellstrom-Westas, L.; Rosen, I. Continuous brain-function monitoring: State of the art in clinical practice. Semin. Fetal Neonatal Med. 2006, 11, 503–511. [Google Scholar] [CrossRef]
- Tsuchida, T.N.; Wusthoff, C.J.; Shellhaas, R.A.; Abend, N.S.; Hahn, C.D.; Sullivan, J.E.; Nguyen, S.; Weinstein, S.; Scher, M.S.; Riviello, J.J.; et al. American clinical neurophysiology society standardized EEG terminology and categorization for the description of continuous EEG monitoring in neonates: Report of the American Clinical Neurophysiology Society critical care monitoring committee. J. Clin. Neurophysiol. 2013, 30, 161–173. [Google Scholar] [CrossRef]
- Hochberg, O.; Berger, I. Bedside EEG Monitoring in the Neonatal Intensive Care Unit. Curr. Treat. Options Pediatr. 2022, 8, 295–307. [Google Scholar] [CrossRef]
- Variane, G.F.T.; Rodrigues, D.P.; Pietrobom, R.F.R.; França, C.N.; Netto, A.; Magalhães, M. Newborns at high risk for brain injury: The role of the amplitude-integrated electroencephalography. J. De Pediatr. 2022, 98, 565–571. [Google Scholar] [CrossRef]
- Failla, A.; Filatovaite, L.; Wang, X.; Vanhatalo, S.; Dudink, J.; de Vries, L.S.; Benders, M.; Stevenson, N.; Tataranno, M.L. The relationship between interhemispheric synchrony, morphine and microstructural development of the corpus callosum in extremely preterm infants. Hum. Brain Mapp. 2022, 43, 4914–4923. [Google Scholar] [CrossRef]
- van’t Westende, C.; Geraedts, V.J.; van Ramesdonk, T.; Dudink, J.; Schoonmade, L.J.; van der Knaap, M.S.; Van de Pol, L.A. Neonatal quantitative electroencephalography and long-term outcomes: A systematic review. Dev. Med. Child. Neurol. 2022, 64, 413–420. [Google Scholar] [CrossRef]
- Rasanen, O.; Metsaranta, M.; Vanhatalo, S. Development of a novel robust measure for interhemispheric synchrony in the neonatal EEG: Activation Synchrony Index (ASI). Neuroimage 2013, 69, 256–266. [Google Scholar] [CrossRef]
- O’Reilly, D.; Navakatikyan, M.A.; Filip, M.; Greene, D.; Van Marter, L.J. Peak-to-peak amplitude in neonatal brain monitoring of premature infants. Clin. Neurophysiol. 2012, 123, 2139–2153. [Google Scholar] [CrossRef] [PubMed]
- Suvisto, S. Effects of Dexmedetomidine on the Cortical Activity of Neonates. Aalto University, School of Electrical Engineering. 2018. Available online: http://urn.fi/URN:NBN:fi:aalto-201811135772 (accessed on 15 November 2022).
- Koolen, N.; Dereymaeker, A.; Rasanen, O.; Jansen, K.; Vervisch, J.; Matic, V.; De Vos, M.; Van Huffel, S.; Naulaers, G.; Vanhatalo, S. Interhemispheric synchrony in the neonatal EEG revisited: Activation synchrony index as a promising classifier. Front. Hum. Neurosci. 2014, 8, 1030. [Google Scholar] [CrossRef] [PubMed]
- Koolen, N.; Dereymaeker, A.; Rasanen, O.; Jansen, K.; Vervisch, J.; Matic, V.; Naulaers, G.; De Vos, M.; Van Huffel, S.; Vanhatalo, S. Early development of synchrony in cortical activations in the human. Neuroscience 2016, 322, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Korček, P.; Straňák, Z.; Širc, J.; Naulaers, G. The role of near-infrared spectroscopy monitoring in preterm infants. J. Perinatol. 2017, 37, 1070–1077. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | n = 21 |
|---|---|
| Gestational age, weeks | 38.7 (27–42) |
| Birthweight, g | 3200 (1150–4780) |
| Postnatal age at study, day | 2 (0–13) |
| Diagnosis groups; 0 = Other (MAS *, RDS *, PPHN *, infection) 1 = HIE * (mild or moderate) 2 = HIE * (severe) 3 = IVH * | 5 8 6 2 |
| Concurrent drugs affecting the brain during the examination (fentanyl, ketanest, phenobarbital, caffeine citrate) | 15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nilsson, S.; Tokariev, A.; Metsäranta, M.; Norman, E.; Vanhatalo, S. A Bedside Method for Measuring Effects of a Sedative Drug on Cerebral Function in Newborn Infants. Sensors 2023, 23, 444. https://doi.org/10.3390/s23010444
Nilsson S, Tokariev A, Metsäranta M, Norman E, Vanhatalo S. A Bedside Method for Measuring Effects of a Sedative Drug on Cerebral Function in Newborn Infants. Sensors. 2023; 23(1):444. https://doi.org/10.3390/s23010444
Chicago/Turabian StyleNilsson, Sofie, Anton Tokariev, Marjo Metsäranta, Elisabeth Norman, and Sampsa Vanhatalo. 2023. "A Bedside Method for Measuring Effects of a Sedative Drug on Cerebral Function in Newborn Infants" Sensors 23, no. 1: 444. https://doi.org/10.3390/s23010444
APA StyleNilsson, S., Tokariev, A., Metsäranta, M., Norman, E., & Vanhatalo, S. (2023). A Bedside Method for Measuring Effects of a Sedative Drug on Cerebral Function in Newborn Infants. Sensors, 23(1), 444. https://doi.org/10.3390/s23010444