
Mitigating the Impact of the COVID-19 Pandemic on Adult Cancer Patients through Telehealth Adoption: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
3. Results
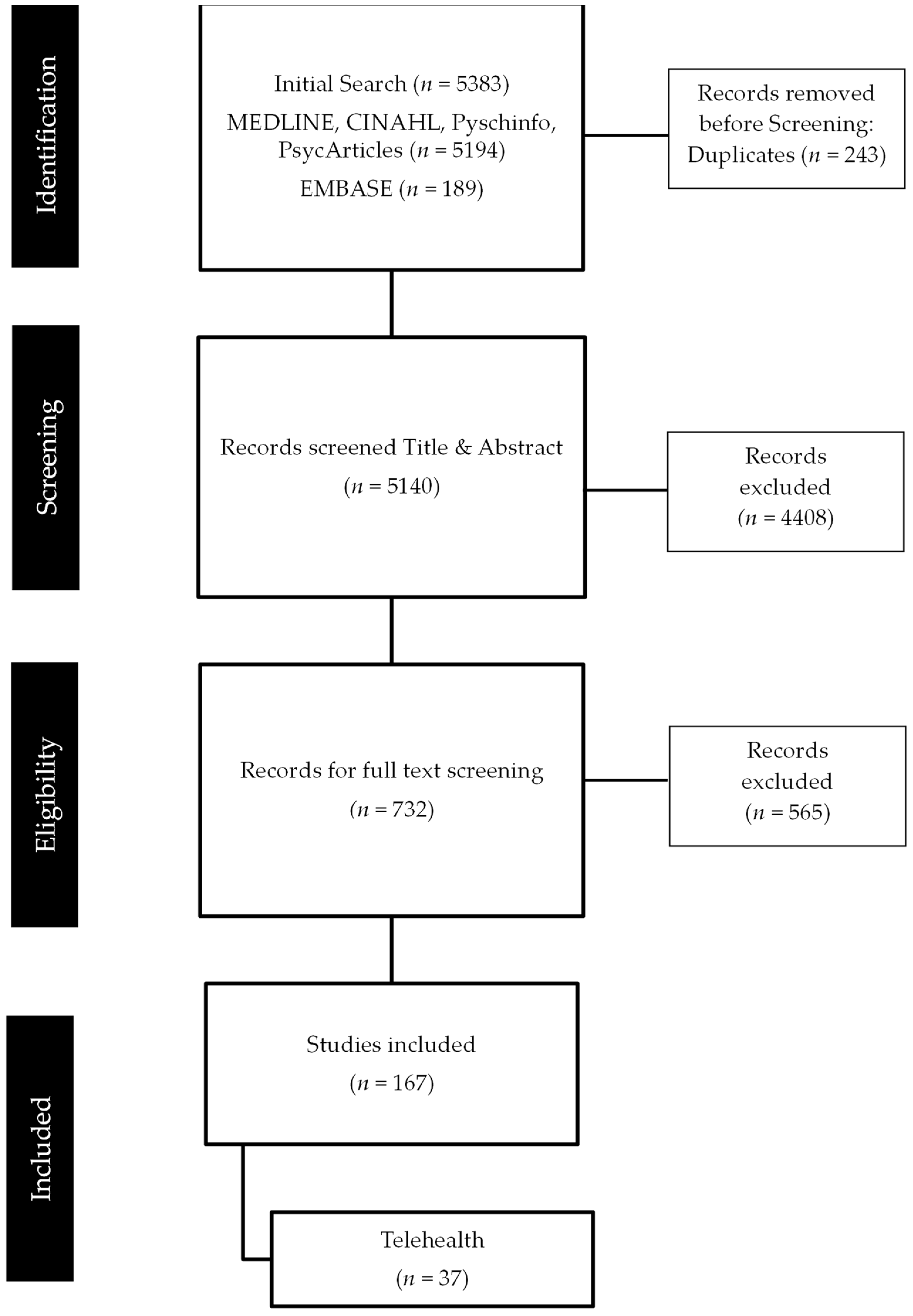
3.1. Overview of Search Results
3.2. Range of Telehealth Services Employed
3.3. Satisfaction with Telehealth
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Quality Review
I PREVALENCE STUDIES [27]
| |||||||||
| Author | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 |
| Atreya et al. (2020) [50] | NA | NA | NA | Y | Y | Y | Y | Y | NA |
| Alterio et al. (2020) [34] | UC | UC | UC | Y | Y | Y | Y | Y | NA |
| Biswas et al. (2020) [51] | Y | UC | UC | Y | Y | Y | Y | Y | UC |
| de Marinis et al. (2020) [36] | NA | NA | NA | Y | NA | Y | Y | Y | NA |
| Frey et al. (2020) [62] | N | UC | UC | Y | Y | Y | Y | Y | UC |
| Kwek et al. (2021) [47] | Y | UC | N | Y | Y | Y | Y | Y | N |
| Mahl et al. (2020) [63] | Y | UC | UC | Y | Y | N | Y | Y | UC |
| Merz et al. (2021) [43] | Y | UC | UC | Y | Y | N | Y | Y | UC |
| Mitra et al. (2020) [64] | Y | Y | UC | Y | Y | Y | Y | Y | Y |
| Patt et al. (2021) [53] | Y | UC | UC | Y | Y | N | Y | Y | UC |
| Patt et al. (2020b) [54] | Y | NA | UC | Y | Y | Y | Y | Y | UC |
| Rodler et al. (2020) [57] | Y | UC | Y | Y | Y | N | Y | Y | Y |
| Sawka et al. (2021) [37] | UC | UC | UC | Y | Y | Y | Y | Y | UC |
| Smrke et al. (2020) [55] | Y | UC | UC | Y | Y | Y | Y | Y | Y |
| Somani et al. (2020) [58] | Y | NA | NA | Y | Y | Y | Y | Y | NA |
| Sonagli et al. (2021) [46] | UC | UC | UC | Y | Y | Y | Y | Y | NA |
| Zuliani et al. (2020) [60] | Y | UC | UC | Y | Y | Y | Y | Y | UC |
II CROSS SECTIONAL ANALYTICAL STUDIES [27]
| ||||||||
| Author | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 |
| Goenka et al. (2021) [31] | NA | Y | Y | Y | Y | Y | Y | Y |
| Kamposioras et al. (2020) [59] | Y | Y | Y | Y | Y | Y | Y | Y |
| Kotsen et al. (2021) [42] | Y | Y | Y | Y | Y | Y | Y | Y |
| Lonergan et al. (2020) [15] | NA | Y | Y | Y | Y | Y | Y | Y |
III QUALITATIVE STUDIES [27]
| ||||||||||
| Author | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 |
| Lopez et al. (2021) [49] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Wu et al. (2020) [52] | UC | Y | Y | Y | Y | N | Y | Y | Y | Y |
IV COHORT STUDIES [27]
| |||||||||||
| Author | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 |
| Akhtar et al. (2021) [38] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Akuamoa-Boateng et al. (2020) [33] | UC | Y | NA | N | N | Y | Y | Y | Y | NA | Y |
| Araujo et al. (2020) [56] | UC | Y | NA | N | N | Y | Y | Y | Y | NA | Y |
| Brenes Sanchez et al. (2021) [39] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Caravatta et al. (2020) [35] | UC | Y | NA | N | N | Y | UC | Y | Y | UC | Y |
| Clark et al. (2021) [48] | UC | Y | NA | N | N | Y | Y | Y | Y | NA | Y |
| Earp et al. (2020) [40] | UC | Y | NA | N | N | Y | Y | Y | Y | NA | Y |
| Maganty et al. (2020) [30] | Y | Y | Y | Y | Y | Y | Y | Y | Y | NA | Y |
| Narayanan et al. (2021) [44] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Patt et al. (2020a) [65] | UC | Y | NA | N | N | Y | Y | Y | Y | NA | Y |
| Romani et al. (2021) [32] | UC | Y | NA | N | N | Y | Y | Y | Y | Y | Y |
| Shannon et al. (2020) [45] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Wai et al. (2021) [41] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| V Cost Analysis: Consensus on Health Economic Criteria (CHEC)-List (Evers, Goossens, De Vet, Van Tulder, and Ament, 2005) [28] | Parikh et al. (2020) [61] |
| 1. Is the study population clearly described? | Y |
| 2. Are competing alternatives clearly described? | Y |
| 3. Is a well-defined research question posed in answerable form? | Y |
| 4. Is the economic study design appropriate to the stated objective? | Y |
| 5. Is the chosen time horizon appropriate to include relevant costs and consequences? | Y |
| 6. Is the actual perspective chosen appropriate? | Y |
| 7. Are all important and relevant costs for each alternative identified? | Y |
| 8. Are all costs measured appropriately in physical units? | Y |
| 9. Are costs valued appropriately? | Y |
| 10. Are all important and relevant outcomes for each alternative identified? | NA |
| 11. Are all outcomes measured appropriately? | NA |
| 12. Are outcomes valued appropriately? | NA |
| 13. Is an incremental analysis of costs and outcomes of alternatives performed? | NA |
| 14. Are all future costs and outcomes discounted appropriately? | NA |
| 15. Are all important variables, whose values are uncertain, appropriately subjected to sensitivity analysis? | Y |
| 16. Do the conclusions follow from the data reported? | Y |
| 17. Does the study discuss the generalisability of the results to other settings and patient/client groups? | N |
| 18. Does the article indicate that there is no potential conflict of interest of study researcher(s) and funder(s)? | Y |
| 19. Are (a) ethical and (b) distributional issues discussed appropriately? | (a) N (b) Y |
| N = No, NA = Not applicable, UC = unclear, Y = Yes. | |
Appendix B. Thematic Overview
| Author | Highly Satisfied with Telehealth/Acceptance | Desire to Continue Telehealth | No Desire to Replace in-Person Visits with Telehealth | Increased Access to Care | Increased Use of Telehealth | Maintenance of Increased Attendance/Engagement | Challenges | TELEHEALTH Feasible |
| Akhtar et al. (2021) [38] | ✓ | |||||||
| Akuamoa-Boateng et al. (2020) [33] | ✓ | |||||||
| Alterio et al. (2020) [34] | ✓ | |||||||
| Araujo et al. (2020) [56] | ✓ | |||||||
| Atreya et al. (2020) [50] | ✓ | ✓ | ||||||
| Biswas et al. (2020) [51] | ✓ | ✓ | ||||||
| Brenes Sánchez et al. (2021) [39] | ✓ | |||||||
| Caravatta et al. (2020) [35] | ✓ | |||||||
| Clark et al. (2021) [48] | ✓ | |||||||
| De Marinis et al. (2020) [36] | ✓ | |||||||
| Earp et al. (2020) [40] | ✓ | |||||||
| Frey et al. (2020) [62] | ✓ | |||||||
| Goenka et al. (2021) [31] | ✓ | ✓ | ||||||
| Kamposioras et al. (2020) [59] | ✓ | |||||||
| Kotsen et al. (2021) [42] | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Kwek et al. (2021) [47] | ✓ | |||||||
| Lonergan et al. (2020) [15] | ✓ | ✓ | ||||||
| Lopez et al. (2021) [49] | ✓ | ✓ | ||||||
| Maganty, et al. (2020) [30] | ✓ | |||||||
| Mahl et al. (2020) [63] | ✓ | |||||||
| Merz et al. (2021) [43] | ✓ | ✓ | ||||||
| Mitra, et al. (2020) [64] | ✓ | |||||||
| Narayanan et al. (2021) [44] | ✓ | |||||||
| Parikh, et al. (2020) [61] | ✓ | |||||||
| Patt et al. (2020a) [65] | ✓ | |||||||
| Patt, et al. (2020b) [54] | ✓ | ✓ | ✓ | |||||
| Patt et al. (2021) [53] | ✓ | ✓ | ✓ | ✓ | ||||
| Rodler et al. (2020) [57] | ✓ | |||||||
| Romani et al. (2021) [32] | ✓ | |||||||
| Sawka, et al. (2021) [37] | ✓ | |||||||
| Shannon, et al. (2020) [45] | ✓ | |||||||
| Smrke, et al. (2020) [55] | ✓ | ✓ | ||||||
| Somani et al. (2020) [58] | ✓ | ✓ | ||||||
| Sonagli et al. (2021) [46] | ✓ | ✓ | ✓ | |||||
| Wai et al. (2020) [41] | ✓ | |||||||
| Wu et al. (2020) [52] | ✓ | ✓ | ||||||
| Zuliani et al. (2020) [60] | ✓ |
Appendix C. Description of Review Papers
| Author Year Country | Aim | Study Design Sample Size, Age | Context and Setting Study Timeframe | Data Source | Data Collection Data Analysis | Results |
| Akhtar et al. (2021) [38] India | To describe the hospital experience during the first 6 months of the COVID-19 pandemic including the functioning of the department, clinical outcomes, problems faced by patients, and lessons learned | Retrospective N = 1 institution NA | Hospital COVID-19 period: April to Sept 2020. Pre-COVID-19 period: April to Sept, 2019. | Secondary data; hospital record database Primary data; questionnaire |
|
|
| Akuamoa-Boateng et al. (2020) [33] Germany | To compare hospital management of 2019 and 2020 | Retrospective N = 1 institution NA | Hospital Pre-COVID-19: 18/03/19–10/05/19 COVID-19 period: 16/03/20–8/05/20 | Secondary data; hospital records |
|
|
| Alterio et al. (2020) [34] Italy | To report organisation strategies at a radiation oncology department, focusing on procedures and scheduling (i.e.: delays, interruptions) | Retrospective N = 1 institution N = 43 patients 57–74 years | Hospital Pre-COVID-19: 01/03 to 30/04/19 COVID-19 period: 01/03 to 30/04/20 | Secondary data; Electronic medical charts |
|
|
| Araujo et al. (2020) [56] Latin America | To evaluate the impact of COVID-19 pandemic on patient volume in a cancer centre in an epidemic of the pandemic | Provider Retrospective N = 1 institution NA | Hospital Pre-COVID-19: Mar–May 2019 COVID-19 period: Mar–May 2020 | Secondary data; electronic health record database |
|
|
| Atreya et al. (2020) [50] India | (1) To assess changes in the hospital-based practice of palliative care during the pandemic (2) Patient/caregivers perception about the provision of palliative telehealth services (which were in place since 2014) | Patient & caregivers Cross-sectional N = 50 >18 years old | Hospital 01/01–19/05/20 | Primary data; interview Secondary data; electronic medical records |
|
|
| Biswas et al. (2020) [51] India | (1) To assess expansion of telemedicine service in the palliative unit in the department of oncology (2) To assess patient satisfaction | Patient Prospective N = 314 Adults | Hospital 25/03/–13/05/20 | Primary data; Telephone calls | Telephone calls were recorded to collect data on:
|
|
| Brenes Sanchez et al. (2021) [39] Spain | To analyse the management of patients with breast cancer during the pandemic | Patients Retrospective observational N = 57 patients NA | Hospital Group A: 15/03/20–21/04/20 Group B: 22/04/20–06/05/20 | Primary data; questionnaire Secondary data; hospital data | Telephone questionnaire using:
|
|
| Caravatta et al. (2020) [35] Italy | To report the experience and organisational planning of radiotherapy during the first two phases of the emergency, lockdown phase 1 and post-lockdown phase II | Retrospective N = 1 institution NA | Hospital Pre-COVID-19: 09/03–04/05/19 COVID-19 period: 09/03–04/05/20 Lockdown I: 09/03 –04/05/20 Lockdown II: 25–31/05/20 | Secondary data; hospital records |
|
|
| Clark et al. (2021) [48] England | To assess the national impact of COVID-19 on the prescribing of systemic anti-cancer treatment | Retrospective NA NA | Hospital Pre-COVID-19: September, 2019, to February, 2020. COVID-19 period: April–June, 2020 | Secondary data; electronic health registry system |
| Uptake of teleconsultations at national level. Initially the number of registrations of new systemic anti-cancer treatments decreased but average monthly registrations had exceeded pre-pandemic levels by June, 2020, due to other risk-reducing measures such as telephone consultations, facemasks, and physical distancing. |
| De Marinis et al. (2020) [36] Italy | To prove that such proactive management allowed for the minimisation of contagion among patients with lung cancer through the maximisation of preventive measures | Patient and provider Prospective N = 1 institution N = 477 patients, 23–89 years old | Hospital 1 month; March 2020 | Secondary data; hospital records |
|
|
| Earp et al. (2020) [40] USA | Examine the early effect of hospital and state-mandated restrictions on orthopaedic surgery department | Retrospective N = 1 institution NA | Hospital COVID-19 period: 16/03–12/04/20 Study period: 14/02/–15/03/20 Control period: 16/03–12/04/19 | Secondary data; Billing database |
| Surgical department:
|
| Frey et al. (2020) [62] USA | (1) To evaluate the quality of life (QoL) of women with ovarian cancer during the pandemic (2) Evaluate the effects of the pandemic on cancer-related treatment. | Cross-sectional N = 555 20–85 years old | Web-based 30/03–13/04/20 | Primary data; survey |
|
|
| Goenka et al. (2021) [31] USA | Review implementation (1) Patient access to care (2) Billing implication | Provider Observational N = 1 institution 22–93 years old | Hospital 01/01–01/05/20 | Secondary data; hospital data |
|
|
| Kamposioras et al. (2020) [59] England | (1) To investigate the perceptions of service changes imposed by the COVID-19 pandemic. (2) To identify the determinant of anxiety in patients with colorectal cancer | Patient Cross-sectional N = 143 ≥18 years | Hospital 18/05–01/07/20 | Primary data; survey |
|
|
| Kotsen et al. (2021) [42] USA | To examine the effect of rapid scaling to tobacco treatment telehealth for tobacco-dependent cancer patient | Patient and provider Retrospective N = 418 Adults | Hospital: 01/01–30/04/20 | Secondary data; electronic medical records |
|
|
| Kwek et al. (2021) [47] Singapore | To describe outpatient attendance and treatment caseloads during COVID-19 compared with the corresponding period pre-COVID-19. | Retrospective N = 1 institution NA | Hospital COVID-19 period 03/02–23/05/20 Pre-COVID-19 period 03/02–23/05/19 | Secondary data; health records |
|
|
| Lonergan et al. (2020) [15] USA | To analyse the change in video visit volume | Provider Cross-sectional N = 17 departments NA | Hospital Pre-COVID period: 01/01–14/03/20 Post-COVID-19 period: 15/03– 05/04/20 | Secondary data; electronic medical records |
|
|
| Lopez et al. (2021) [49] Canada | To describe the adaptions made to implement virtual cancer rehabilitation at the onset of coronavirus disease 2019 | Multi-method N = 12 patients, N = 12 providers Adults | Hospital 16/03–12/06/20 | Primary data; interviews Secondary data; hospital data |
|
Re: Meeting support needs: sense of reassurance and felt supported, helped cope with worries, some felt isolated by telemedicine. Re: Confidence with assessment and care plan: lack of in-person examination, relying on self-report/assessment of patients, worried about accuracy of describing symptoms, agreed video better than telephone visits, both agreed preference for an initial in-person assessment |
| Maganty, et al. (2020) [30] USA | To evaluate differences in patient populations being evaluated for cancer before and during the COVID-19 pandemic | Retrospective N = 1 institution NA | Hospital Pre-COVID-19 period: 3–5 months prior to 17/03/20 COVID-19 period: 3 to 5 months after 17/03/20 | Secondary data; electronic health records |
|
|
| Mahl et al. (2020) [63] Brazil | To evaluate delays in care for patients with head and neck cancer (HNC) in post-treatment follow-up or palliative care during the COVID-19 pandemic, i.e.: self-perception of anxiety or sadness, fear of COVID-19 infection, cancer-related complications during social isolation, self-medication, diagnosis of COVID-19, and death between patients with and without delayed cancer care | Cross-sectional N = 1 institution N = 31 patients Adults | Hospital 01/01/–30/07/20 | Primary data; interview Secondary data; medical records |
|
|
| Merz et al. (2021) [43] Italy | To assess how breast cancer survivors perceived electronic medical record-assisted telephone follow-up | Prospective N = 137 34–89 years old | Hospital 09/03–02/06/20 | Primary data; survey |
|
|
| Mitra, et al. (2020) [64] India | To study the challenges faced by cancer patients in India during the COVID-19 pandemic | Cross-sectional N = 36 ≥18 years old | Hospital 01–15/05/20 | Primary data; survey |
|
|
| Narayanan et al. (2021) [44] USA | To report the feasibility of conducting integrative oncology (IO) physician consultations via telehealth in 2020 compared to the same period of the previous year. | Retrospective N = 1352 ≥18 years old | Hospital Cohort 1 (in person): 21/04–21/10/19 Cohort 2 (telehealth): 21/04–21/10/20 | Primary data; questionnaire Secondary data; electronic medical records |
|
|
| Parikh, et al. (2020) [61] USA | To evaluate the overall change in resource use associated with the transition to telemedicine in a radiation oncology department | Descriptive N = 1 patient NA | Hospital Using a patient undergoing 28-fraction treatment course, exact timeframe not specified. | Primary data; interviews and surveys of personnel |
|
|
| Patt et al. (2020a) [65] USA | To gain insight into the impact of COVID-19 on the US senior cancer population | Retrospective NA NA | Hospital Pre-COVID-19: March–July 2019 COVID-19 period: March–July 2020 | Secondary data; database |
|
|
| Patt, et al. (2020b) [54] USA | (1) To describe onboarding and utilisation of telemedicine across a large statewide community oncology practice (2) To evaluate trends, barriers, and opportunities in care delivery during the coronavirus disease 2019 pandemic | Cross-sectional N = 640 clinicians at 221 sites of service. N = 80 survey NA | Community setting February to April 2020 Survey: August 2020 | Secondary data; telehealth platform Primary data; survey |
|
|
| Patt et al. (2021) [53] USA | To assess the: (1) Implementation of multidisciplinary telemedicine in community oncology: (2) Level of satisfaction in providers and patients (3) Changes in clinic operations (4) Opportunities and barriers | Cross-sectional N = 640 clinicians at 221 sites of service N = 34 survey NA | Community setting March–September, 2020 | Secondary data; telehealth platform Primary data; survey |
|
|
| Rodler et al. (2020) [57] Germany | To determine patients’ perceptions on adoption of telehealth as a response to the pandemic and its sustainability in the future | Patient Cross-sectional N = 92 33–88 years old | Hospital 1 week | Primary data; survey |
|
|
| Romani et al. (2021) [32] Canada | (1) To examine the effect of the COVID-19 pandemic on the operation of satellite radiation oncology facility run completely virtually from April to May 2020 (2) Patient satisfaction | Patient Retrospective observational N = 1 institution NA | Hospital Pre-COVID-19 period April–May 2019 COVID-19 period April–May 2020 | Secondary data; health records Primary data; survey |
|
|
| Sawka, et al. (2021) [37] Canada | Describe the management of small low-risk papillary thyroid cancer during the COVID-19 pandemic | Prospective observational N = 181 >18 years old | Hospital 12/03–30/10/20 | Secondary data; electronic medical records |
|
|
| Shannon, et al. (2020) [45] USA | To determine how visit and genetic testing volume was impacted by new telephone genetic counselling and home testing. | NA Observational N = 1 institution NA | Hospital 6 weeks | Secondary data; electronic medical records, log entries |
|
|
| Smrke, et al. (2020) [55] UK | To evaluate the impact of telemedicine on patients, clinicians, care delivery | Patient and provider Cross-sectional N = 316 >18 years old | Hospital 23/03–24/04/20 | Primary data; survey Secondary data; electronic medical records |
|
|
| Somani et al. (2020) [58] UK | To assess outpatient and telemedicine (phone and video) volume during the pandemic. | NA Observational N = 1 institution NA | Hospital 13/03–07/05/20 | Secondary data; hospital data |
|
|
| Sonagli et al. (2021) [46] Brazil | To demonstrate how the use of telemedicine was an efficient tool to maintain outpatient appointments for breast cancer patients follow-up and surveillance | Patient Retrospective cohort N = 87 >18 years old | Hospital 05/06–10/10/20 | Secondary data; hospital data |
|
|
| Wai et al. (2020) [41] USA | To understand how the surgical care of head and neck cancer patients was affected, specifically assessing surgical case volume, time to care, safety of the patients, and clinical team | Retrospective N= 1 institution NA | Hospital Pre-COVID-19: 16/03–13/04/19 COVID-19 period: 16/03–16/04/20 | Secondary data; medical notes and database |
|
|
| Wu et al. (2020) [52] Taiwan | To assess smartphone-enabled telehealth model for palliative care family conferences | Patient and family members Pilot observational N = 14 (13 cancer patients, 1 stroke patient) >18 years old | Hospital February to April 2020 | Primary data; Discussion |
|
|
| Zuliani et al. (2020) [60] Italy | To analyse how organisational changes related to COVID-19 have impacted: (i) Volume of oncological activity (compared to same period of 2019) (ii) Hospital admissions of “active” oncological patients for SARS-CoV-2 | Retrospective N = 1 institution N = 241 surveyed NA | Hospital Pre-COVID-19: 01/01–31/03/19 COVID-19 period: 01/01–31/03/20 | Secondary data; health records Primary data; questionnaire |
|
|
References
- Basu, A.; Kuziemsky, C.; de Araújo Novaes, M.; Kleber, A.; Sales, F.; Al-Shorbaji, N.; Flórez-Arango, J.F.; Gogia, S.B.; Ho, K.; Hunter, I.; et al. Telehealth and the COVID-19 pandemic: International perspectives and a health systems framework for telehealth implementation to support critical response. Yearb. Med. Inform. 2021, 30, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1193. [Google Scholar] [CrossRef] [PubMed]
- Simcock, R.; Thomas, T.V.; Estes, C.; Filippi, A.R.; Katz, M.S.; Pereira, I.J.; Saeed, H. COVID-19: Global radiation oncology’s targeted response for pandemic preparedness. Clin. Transl. Radiat. Oncol. 2020, 22, 55–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zonneveld, M.; Patomella, A.-H.; Asaba, E.; Guidetti, S. The use of information and communication technology in healthcare to improve participation in everyday life: A scoping review. Disabil. Rehabil. 2020, 42, 3416–3423. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, P.; Daines, L.; Campbell, C.; McKinstry, B.; Weller, D.; Pinnock, H. Telehealth interventions to support self-management of long-term conditions: A systematic metareview of diabetes, heart failure, asthma, chronic obstructive pulmonary disease, and cancer. J. Med. Internet Res. 2017, 19, e6688. [Google Scholar] [CrossRef]
- Edwards, L.; Thomas, C.; Gregory, A.; Yardley, L.; O’Cathain, A.; Montgomery, A.A.; Salisbury, C. Are people with chronic diseases interested in using telehealth? A cross-sectional postal survey. J. Med. Internet Res. 2014, 16, e3257. [Google Scholar] [CrossRef] [Green Version]
- O’Cathain, A.; Drabble, S.J.; Foster, A.; Horspool, K.; Edwards, L.; Thomas, C.; Salisbury, C. Being human: A qualitative interview study exploring why a telehealth intervention for management of chronic conditions had a modest effect. J. Med. Internet Res. 2016, 18, e163. [Google Scholar] [CrossRef] [Green Version]
- Bradford, N.; Caffery, L.; Smith, A. Correction: Telehealth services in rural and remote Australia: A systematic review of models of care and factors influencing success and sustainability. Rural. Remote Health 2016, 16, 1–24. [Google Scholar]
- Colucci, M.; Baldo, V.; Baldovin, T.; Bertoncello, C. A “matter of communication”: A new classification to compare and evaluate telehealth and telemedicine interventions and understand their effectiveness as a communication process. Health Inform. J. 2019, 25, 446–460. [Google Scholar] [CrossRef]
- LeRouge, C.M.; Garfield, M.J.; Hevner, A.R. Patient perspectives of telemedicine quality. Patient Prefer. Adherence 2015, 9, 25. [Google Scholar] [CrossRef] [Green Version]
- Lindgreen, A. Corruption and unethical behavior: Report on a set of Danish guidelines. J. Bus. Ethics 2004, 51, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Moffatt, J.J.; Eley, D.S. Barriers to the up-take of telemedicine in Australia—A view from providers. Rural Remote Health 2011, 11, 116–121. [Google Scholar] [CrossRef]
- Wade, V.A.; Eliott, J.A.; Hiller, J.E. Clinician acceptance is the key factor for sustainable telehealth services. Qual. Health Res. 2014, 24, 682–694. [Google Scholar] [CrossRef] [PubMed]
- Steindal, S.A.; Nes, A.A.G.; Godskesen, T.E.; Dihle, A.; Lind, S.; Winger, A.; Klarare, A. Patients’ experiences of telehealth in palliative home care: Scoping review. J. Med. Internet Res. 2020, 22, e16218. [Google Scholar] [CrossRef]
- Lonergan, P.E.; Iii, S.L.W.; Branagan, L.; Gleason, N.; Pruthi, R.S.; Carroll, P.R.; Odisho, A.Y. Rapid Utilization of Telehealth in a Comprehensive Cancer Center as a Response to COVID-19: Cross-Sectional Analysis. J. Med. Internet Res. 2020, 22, e19322. [Google Scholar] [CrossRef]
- March, C.A.; Flint, A.; DeArment, D.; Gilliland, A.; Kelly, K.; Rizzitano, E.; Chrisman, A.; Muzumdar, R.H.; Libman, I.M. Paediatric diabetes care during the COVID-19 pandemic: Lessons learned in scaling up telemedicine services. Endocrinol. Diabetes Metab. 2021, 4, e00202. [Google Scholar] [CrossRef]
- O’Reilly, D.; Carroll, H.; Lucas, M.; Sui, J.; al Sendi, M.; McMahon, D.; Darwish, W.; McLaughlin, R.; Khan, M.R.; Sullivan, H.O. Virtual oncology clinics during the COVID-19 pandemic. Ir. J. Med. Sci 2021, 190, 1295–1301. [Google Scholar] [CrossRef]
- Powell, R.E.; Henstenburg, J.M.; Cooper, G.; Hollander, J.E.; Rising, K.L. Patient perceptions of telehealth primary care video visits. Ann. Fam. Med. 2017, 15, 225–229. [Google Scholar] [CrossRef] [Green Version]
- Valdez, R.S.; Rogers, C.C.; Claypool, H.; Trieshmann, L.; Frye, O.; Wellbeloved-Stone, C.; Kushalnagar, P. Ensuring full participation of people with disabilities in an era of telehealth. J. Am. Med. Inform. Assoc. 2021, 28, 389–392. [Google Scholar] [CrossRef]
- Bator, E.X.; Gleason, J.M.; Lorenzo, A.J.; Kanaroglou, N.; Farhat, W.A.; Bägli, D.J.; Koyle, M.A. The burden of attending a pediatric surgical clinic and family preferences toward telemedicine. J. Pediatr. Surg. 2015, 50, 1776–1782. [Google Scholar] [CrossRef]
- Ballantyne, M.; Benzies, K.; Rosenbaum, P.; Lodha, A. Mothers’ and health care providers’ perspectives of the barriers and facilitators to attendance at C anadian neonatal follow-up programs. Child Care Health Dev. 2015, 41, 722–733. [Google Scholar] [CrossRef] [PubMed]
- Rusinko, C. IT responses to COVID-19: Rapid innovation and strategic resilience in healthcare. Inf. Syst. Manag. 2020, 37, 332–338. [Google Scholar] [CrossRef]
- Drerup, B.; Espenschied, J.; Wiedemer, J.; Hamilton, L. Reduced no-show rates and sustained patient satisfaction of telehealth during the COVID-19 pandemic. Telemed. e-Health 2021, 27, 1409–1415. [Google Scholar] [CrossRef]
- Albarrak, A.I.; Mohammed, R.; Almarshoud, N.; Almujalli, L.; Aljaeed, R.; Altuwaijiri, S.; Albohairy, T. Assessment of physician’s knowledge, perception and willingness of telemedicine in Riyadh region, Saudi Arabia. J. Infect. Public Health 2021, 14, 97–102. [Google Scholar] [CrossRef]
- Hutton, B.; Catala-Lopez, F.; Moher, D. The PRISMA statement extension for systematic reviews incorporating network meta-analysis: PRISMA-NMA. Med. Clin. 2016, 147, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Davies, K.S. Formulating the evidence based practice question: A review of the frameworks. Evid. Based Libr. Inf. Pract. 2011, 6, 75–80. [Google Scholar] [CrossRef] [Green Version]
- JBI. Joanna Briggs Institute Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 10 December 2021).
- Evers, S.; Goossens, M.; de Vet, H.; van Tulder, M.; Ament, A. Criteria list for assessment of methodological quality of economic evaluations: Consensus on Health Economic Criteria. Int. J. Technol. Assess. Health Care 2005, 21, 240–245. [Google Scholar] [CrossRef] [Green Version]
- Murphy, A.; Lawlor, A.; Kirby, A.; Drummond, F.D. A Systematic Review of the Impact of COVID-19 Pandemic on Cancer Patients and Survivors from an Economic and Social Perspective; University Colelge Cork: Cork, Ireland, 2021. [Google Scholar]
- Maganty, A.; Yu, M.; Anyaeche, V.I.; Zhu, T.; Hay, J.M.; Davies, B.J.; Yabes, J.G.; Jacobs, B.L. Referral pattern for urologic malignancies before and during the COVID-19 pandemic. Urol. Oncol. Semin. Orig. Investig. 2020, 39, 268–276. [Google Scholar] [CrossRef]
- Goenka, A.; Ma, D.; Teckie, S.; Alfano, C.; Bloom, B.; Hwang, J.; Potters, L. Implementation of Telehealth in Radiation Oncology: Rapid Integration during COVID-19 and Its Future Role in Our Practice. Adv. Radiat. Oncol. 2021, 6, 100575. [Google Scholar] [CrossRef]
- Romani, C.; Conlon, M.; Oliver, M.; Leszczynski, K.; Hunter, M.; Lam, K.; Spadafora, S.; Pearce, A. The Operation of Canada’s Only Virtually Operated Radiation Oncology Service during the COVID-19 Pandemic. Adv. Radiat. Oncol. 2021, 6, 100634. [Google Scholar] [CrossRef]
- Akuamoa-Boateng, D.; Wegen, S.; Ferdinandus, J.; Marksteder, R.; Baues, C.; Marnitz, S. Managing patient flows in radiation oncology during the COVID-19 pandemic: Reworking existing treatment designs to prevent infections at a German hot spot area University Hospital. Strahlenther. Onkol. 2020, 196, 1080–1085. [Google Scholar] [CrossRef] [PubMed]
- Alterio, D.; Volpe, S.; Marvaso, G.; Turturici, I.; Ferrari, A.; Leonardi, M.C.; Lazzari, R.; Fiore, M.S.; Bufi, G.; Cattani, F.; et al. Head and neck cancer radiotherapy amid COVID-19 pandemic: Report from Milan, Italy. Head Neck 2020, 42, 1482–1490. [Google Scholar] [CrossRef] [PubMed]
- Caravatta, L.; Rosa, C.; di Sciascio, M.B.; Scaringi, A.T.; di Pilla, A.; Ursini, L.A.; Taraborrelli, M.; Vinciguerra, A.; Augurio, A.; di Tommaso, M.; et al. COVID-19 and radiation oncology: The experience of a two-phase plan within a single institution in central Italy. Radiat. Oncol. 2020, 15, 226. [Google Scholar] [CrossRef] [PubMed]
- de Marinis, F.; Attili, I.; Morganti, S.; Stati, V.; Spitaleri, G.; Gianoncelli, L.; del Signore, E.; Catania, C.; Rampinelli, C.; Salè, E.O.; et al. Results of Multilevel Containment Measures to Better Protect Lung Cancer Patients From COVID-19: The IEO Model. Front. Oncol. 2020, 10, 665. [Google Scholar] [CrossRef] [Green Version]
- Sawka, A.M.; Ghai, S.; Ihekire, O.; Jones, J.M.; Gafni, A.; Baxter, N.N.; Goldstein, D.P.; on behalf of the Canadian Thyroid Cancer Active Surveillance Study Group. Decision-making in surgery or active surveillance for low risk papillary thyroid cancer during the COVID-19 pandemic. Cancers 2021, 13, 371. [Google Scholar] [CrossRef]
- Akhtar, N.; Rajan, S.; Chakrabarti, D.; Kumar, V.; Gupta, S.; Misra, S.; Chaturvedi, A.; Azhar, T.; Parveen, S.; Qayoom, S.; et al. Continuing cancer surgery through the first six months of the COVID-19 pandemic at an academic university hospital in India: A lower-middle-income country experience. J. Surg. Oncol. 2021, 123, 1177–1187. [Google Scholar] [CrossRef]
- Brenes Sánchez, J.M.; Picado, A.L.; Crespo, M.E.O.; Sáenz, J.Á.G.; Merlo, R.M.d.; de la Muela, M.H. Breast Cancer Management during COVID-19 Pandemic in Madrid: Surgical Strategy. Clin. Breast Cancer 2021, 21, e128–e135. [Google Scholar] [CrossRef]
- Earp, B.E.; Zhang, D.; Benavent, K.A.; Byrne, L.; Blazar, P.E. The Early Effect of COVID-19 Restrictions on an Academic Orthopedic Surgery Department. Orthopedics 2020, 43, 228–232. [Google Scholar] [CrossRef]
- Wai, K.C.; Xu, M.J.; Lee, R.H.; El-Sayed, I.H.; George, J.R.; Heaton, C.M.; Knott, P.D.; Park, A.M.; Ryan, W.R.; Seth, R.; et al. Head and neck surgery during the coronavirus-19 pandemic: The University of California San Francisco experience. Head Neck 2021, 43, 622–629. [Google Scholar] [CrossRef]
- Kotsen, C.; Dilip, D.; Carter-Harris, L.; O’Brien, M.; Whitlock, C.W.; de Leon-Sanchez, S.; Ostroff, J.S. Rapid Scaling up of Telehealth Treatment for Tobacco-Dependent Cancer Patients during the COVID-19 Outbreak in New York City. Telemed. J. e-Health Off. J. Am. Telemed. Assoc. 2021, 27, 20–29. [Google Scholar] [CrossRef]
- Merz, V.; Ferro, A.; Piras, E.M.; Zanutto, A.; Caffo, O.; Messina, C. Electronic Medical Record-Assisted Telephone Follow-Up of Breast Cancer Survivors during the COVID-19 Pandemic: A Single Institution Experience. JCO Oncol. Pract. 2021, 17, e44–e52. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, S.; Lopez, G.; Powers-James, C.; Fellman, B.M.; Chunduru, A.; Li, Y.; Bruera, E.; Cohen, L. Integrative Oncology Consultations Delivered via Telehealth in 2020 and In-Person in 2019: Paradigm Shift during the COVID-19 World Pandemic. Integr. Cancer Ther. 2021, 20, 1534735421999101. [Google Scholar] [CrossRef] [PubMed]
- Shannon, K.M.; Emmet, M.M.; Rodgers, L.H.; Wooters, M.; Seidel, M.L. Transition to telephone genetic counseling services during the COVID-19 pandemic. J. Genet. Couns. 2020, 30, 984–988. [Google Scholar] [CrossRef] [PubMed]
- Sonagli, M.; Neto, R.C.; Leite, F.P.M.; Makdissi, F.B.A. The use of telemedicine to maintain breast cancer follow-up and surveillance during the COVID-19 pandemic. J. Surg. Oncol. 2021, 123, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Kwek, J.W.; Chan, J.J.; Kanesvaran, R.; Wang, M.L.C.; Neo, P.S.H.; Chia, C.S.; Tham, C.K.; Chew, L.S.T.; Tan, H.K.; Yap, S.P.; et al. Early Outcomes of a National Cancer Center’s Strategy Against COVID-19 Executed Through a Disease Outbreak Response Taskforce. JCO Oncol. Pract. 2021, 17, e343–e354. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.J.; Dwyer, D.; Pinwill, N.; Clark, P.; Johnson, P.; Hackshaw, A. The effect of clinical decision making for initiation of systemic anticancer treatments in response to the COVID-19 pandemic in England: A retrospective analysis. Lancet Oncol. 2021, 22, 66–73. [Google Scholar] [CrossRef]
- Lopez, C.J.; Edwards, B.; Langelier, D.M.; Chang, E.K.; Chafranskaia, A.; Jones, J.M. Delivering Virtual Cancer Rehabilitation Programming during the First 90 Days of the COVID-19 Pandemic: A Multimethod Study. Arch. Phys. Med. Rehabil. 2021, 102, 1283–1293. [Google Scholar] [CrossRef]
- Atreya, S.; Kumar, G.; Samal, J.; Bhattacharya, M.; Banerjee, S.; Mallick, P.; Chakraborty, D.; Gupta, S.; Sarkar, S. Patients’/Caregivers’ perspectives on telemedicine service for advanced cancer patients during the COVID-19 pandemic: An exploratory survey. Indian J. Palliat. Care 2020, 26, 40–44. [Google Scholar] [CrossRef]
- Biswas, S.; Adhikari, S.; Gupta, N.; Garg, R.; Bharti, S.; Kumar, V.; Mishra, S.; Bhatnagar, S. Smartphone-based telemedicine service at palliative care unit during nationwide lockdown: Our initial experience at a tertiary care cancer hospital. Indian J. Palliat. Care 2020, 26, 31–35. [Google Scholar]
- Wu, Y.-R.; Chou, T.-J.; Wang, Y.-J.; Tsai, J.-S.; Cheng, S.-Y.; Yao, C.-A.; Peng, J.-K.; Hu, W.-Y.; Chiu, T.-Y.; Huang, H.-L. Smartphone-Enabled, Telehealth-Based Family Conferences in Palliative Care during the COVID-19 Pandemic: Pilot Observational Study. JMIR Mhealth Uhealth 2020, 8, e22069. [Google Scholar] [CrossRef]
- Patt, D.A.; Wilfong, L.; Toth, S.; Broussard, S.; Kanipe, K.; Hammonds, J.; Allen, V.; Mautner, B.; Campbell, N.; Dubey, A.K.; et al. Telemedicine in Community Cancer Care: How Technology Helps Patients With Cancer Navigate a Pandemic. JCO Oncol. Pract. 2021, 17, e11–e15. [Google Scholar] [CrossRef] [PubMed]
- Patt, D.; Wilfong, L.; Kanipe, K.; Paulson, R.S. Telemedicine for cancer care: Implementation across a multicenter community oncology practice. Am. J. Manag. Care 2020, 26, SP330–SP332. [Google Scholar]
- Smrke, A.; Younger, E.; Wilson, R.; Husson, O.; Farag, S.; Merry, E.; Macklin-Doherty, A.; Cojocaru, E.; Arthur, A.; Benson, C.; et al. Telemedicine during the COVID-19 Pandemic: Impact on Care for Rare Cancers. JCO Glob. Oncol. 2020, 6, 1046–1051. [Google Scholar] [CrossRef] [PubMed]
- Araujo, S.r.E.A.; Leal, A.; Centrone, A.F.Y.; Teich, V.D.; Malheiro, D.T.; Cypriano, A.S.; Neto, M.C.; Klajner, S. Impact of COVID-19 pandemic on care of oncological patients: Experience of a cancer center in a Latin American pandemic epicenter. Einstein 2020, 19, eAO6282. [Google Scholar] [CrossRef] [PubMed]
- Rodler, S.; Apfelbeck, M.; Schulz, G.B.; Ivanova, T.; Buchner, A.; Staehler, M.; Heinemann, V.; Stief, C.; Casuscelli, J. Telehealth in Uro-oncology Beyond the Pandemic: Toll or Lifesaver? Eur. Urol. Focus 2020, 6, 1097–1103. [Google Scholar] [CrossRef]
- Somani, B.K.; Pietropaolo, A.; Coulter, P.; Smith, J. Delivery of urological services (telemedicine and urgent surgery) during COVID-19 lockdown: Experience and lessons learnt from a university hospital in United Kingdom. Scott. Med. J. 2020, 65, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Kamposioras, K.; Saunders, M.; Lim, K.H.J.; Marti, K.; Anderson, D.; Cutting, M.; McCool, D.; Connell, J.; Simpson, L.; Hasan, J.; et al. The Impact of Changes in Service Delivery in Patients with Colorectal Cancer during the Initial Phase of the COVID-19 Pandemic. Clin. Colorectal Cancer 2020, 20, e120–e128. [Google Scholar] [CrossRef]
- Zuliani, S.; Zampiva, I.; Tregnago, D.; Casalil, M.; Cavalierel, A.; Fumagallil, A.; Merlerl, S.; Rival, S.T.; Rossil, A.; Zacchil, F.; et al. Organisational challenges, volumes of oncological activity and patients’ perception during the severe acute respiratory syndrome coronavirus 2 epidemic. Eur. J. Cancer 2020, 135, 159–169. [Google Scholar] [CrossRef]
- Parikh, N.R.; Chang, E.M.; Kishan, A.U.; Kaprealian, T.B.; Steinberg, M.L.; Raldow, A.C. Time-Driven Activity-Based Costing Analysis of Telemedicine Services in Radiation Oncology. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 430–434. [Google Scholar] [CrossRef]
- Frey, M.K.; Ellis, A.E.; Zeligs, K.; Chapman-Davis, E.; Thomas, C.; Christos, P.J.; Kolev, V.; Prasad-Hayes, M.; Cohen, S.; Holcomb, K.; et al. Impact of the coronavirus disease 2019 pandemic on the quality of life for women with ovarian cancer. Am. J. Obstet. Gynecol. 2020, 223, 725.e1–725.e9. [Google Scholar] [CrossRef]
- Mahl, C.; Melo, L.s.R.S.d.; Almeida, M.H.A.; Carvalho, C.S.; Santos, L.L.S.; Nunes, P.S.; Quintans-JÚnior, L.J.; AraÚjo, A.A.d.S.; Santos, V.S.; Martins-Filho, P.R. Delay in head and neck cancer care during the COVID-19 pandemic and its impact on health outcomes. Braz. Oral Res. 2020, 34, e126. [Google Scholar] [CrossRef] [PubMed]
- Mitra, M.; Basu, M. A Study on Challenges to Health Care Delivery Faced by Cancer Patients in India during the COVID-19 Pandemic. J. Prim. Care Community Health 2020, 11, 2150132720942705. [Google Scholar] [CrossRef] [PubMed]
- Patt, D.; Gordan, L.; Diaz, M.; Okon, T.; Grady, L.; Harmison, M.; Markward, N.; Sullivan, M.; Peng, J.; Zhou, A. Impact of COVID-19 on Cancer Care: How the Pandemic Is Delaying Cancer Diagnosis and Treatment for American Seniors. JCO Clin. Cancer Inform. 2020, 4, 1059–1071. [Google Scholar] [CrossRef] [PubMed]
- Bestsennyy, O.; Gilbert, G.; Harris, A.; Rost, J. Telehealth: A Quarter-Trillion-Dollar Post-COVID-19 Reality. Available online: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-reality (accessed on 10 February 2022).

{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | Search Terms | |
|---|---|---|---|
| Population | Adult population (>18 years old) Current cancer patients and survivors (2 years post-diagnosis) | Caregivers, nursing and medical staff, and paediatric cancer patients | “cancer” OR “oncology” OR “malignant” OR “tumour” OR “metastasis” OR “neoplasm” |
| Intervention | COVID-19 pandemic | - | “COVID-19” OR “coronavirus” OR “2019-ncov” OR “SARS-CoV-2” OR “cov-19” OR “severe acute respiratory syndrome coronavirus-2” OR “pandemic” |
| Outcome | economic, social, health, and psychological implications of COVID-19 on cancer patients/survivors | - | “financial toxicity” OR “out-of-pocket” OR “productivity” OR “absenteeism” OR “unemployment” OR “cost” OR “waiting time” OR “expenses” OR “financial stress” OR “inconvenience” OR “opportunity cost” OR “income” OR “wellbeing” OR “social isolation” OR “exclusion” OR “loneliness” OR “happiness” OR “life satisfaction” OR “fatigue” OR “insomnia” OR “psychological distress” OR “emotional distress” OR “anxiety” OR “depression” OR “post-traumatic stress disorder” OR “psychological” OR “quality of life” OR “health-related quality of life” OR “survival” OR “mortality” OR “disease progression” OR “diagnosis” OR “screening” OR “recurrence” OR “disease stage” OR “delay” OR “support” OR “surgery” OR “treatment” OR “target therapy” OR “radiotherapy” OR “chemotherapy” OR “immunotherapy” OR “hormone therapy” OR “survivorship programme” OR “follow-up-care” |
| Context | Hospital and community setting | - | |
| Studies | Full-text articles Patient perspective, Observational, Cross-sectional, Prospective, Longitudinal Retrospective | Letters to the editor, editorials, case studies, reports, protocols, commentaries, short communications, reviews, opinions, perspectives, and discussions |
| Author Year Country | Aim | Telehealth Tool | Results |
|---|---|---|---|
| Akhtar et al. (2021) [38] India | Describe the hospital experience during the first 6 months of the COVID-19 pandemic. | Teleconsultations/virtual appointments for patients |
|
| Akuamoa-Boateng et al. (2020) [33] Germany | Compare hospital management in 2019 & 2020 | Teleconsultations/virtual appointments for patients Video conferencing for staff |
|
| Alterio et al. (2020) [34] Italy | Report organisation strategies at a radiation oncology department, focusing on procedures and scheduling (i.e.: delays, interruptions) | Teleconsultations/virtual appointments for patients |
|
| Araujo et al. (2020) [56] Latin America | Evaluate the impact of COVID-19 pandemic on patient volume in a cancer centre in an epidemic of the pandemic | Teleconsultations/virtual appointments for patients Video conferencing for staff |
|
| Atreya et al. (2020) [50] India | (1) Assess changes in the hospital-based practice of palliative care during the pandemic (2) Report patient/caregivers perception about the provision of palliative telehealth services (established 2014) | Teleconsultations/virtual appointments for patients |
|
| Biswas et al. (2020) [51] India | (1) Assess expansion of service telemedicine in the palliative unit in the department of oncology (2) Assess patient satisfaction. | Teleconsultations/virtual appointments (telephone, texts and video) for patients |
Patient satisfaction: 56 very satisfied; 152 satisfied; 59 partially satisfied; 47 unsatisfied; 42 patients believed that face-to-face consultations may be more useful for them |
| Brenes Sanchez et al. (2021) [39] Spain | Anlayse management breast cancer patients during the pandemic | Teleconsultations/virtual appointments for patients |
|
| Caravatta et al. (2020) [35] Italy | Report the experience and organisational planning of radiotherapy during pandemic | Telephone consultations. Telematics laboratory results Staff meetings on a telematic platform |
|
| Clark et al. (2021) [48] England | Assess the national impact of COVID-19 on the prescribing of systemic anti-cancer treatment | Teleconsultations/virtual appointments for patients |
|
| De Marinis et al. (2020) [36] Italy | Examine proactive management to minimise contagion among patients with lung cancer | Telephone consultations Telematics laboratory results |
|
| Earp et al. (2020) [40] USA | Examine the early effect of hospital and state mandated restrictions on an orthopedic surgery department | Teleconsultations/virtual appointments (telephone and video) for patients |
|
| Frey et al. (2020) [62] USA | (1) Evaluate the quality of life (QoL) of women with ovarian cancer during the pandemic (2) Evaluate the effects of the pandemic on cancer-related treatment. | Teleconsultations/virtual appointments for patients Online counselling Online networks |
|
| Goenka et al. (2021) [31] USA | Review implementation of patient access to care & billing implications | Teleconsultations/virtual appointments (telephone and video) for patients |
|
| Kamposioras et al. (2020) [59] England | (1) Investigate the perceptions of service changes imposed by the COVID-19 pandemic. (2) Identify the determinant of anxiety in patients with colorectal cancer | Teleconsultations/virtual appointments (telephone and video) for patients |
|
| Kotsen et al. (2021) [42] USA | Examine the effect of rapid scaling to tobacco treatment telehealth for tobacco dependent cancer patients | Teleconsultations/virtual appointments for patients |
|
| Kwek et al. (2021) [47] Singapore | Describe outpatient attendances and treatment caseloads during COVID-19 compared to pre COVID-19. | Teleconsultations/virtual appointments for patients and family members. Tele-counselling& psychosocial support. Medication delivery. |
|
| Lonergan et al. (2020) [15] USA | Analyse the change in video visit volume | Video consultations |
|
| Lopez et al. (2021) [49] Canada | Describe adaptions to implement virtual cancer rehabilitation at the onset of the coronavirus disease 2019 | Teleconsultations/virtual appointments (telephone and video) for patients |
Re: Meeting support needs: sense of reassurance and felt supported, helped cope with worries, some felt isolated by telemedicine. Re: Confidence with assessment and care plan: lack of in-person examination, relying on self-report/assessment of patients, worried about accuracy of describing symptoms, agreed video better than telephone visits, Both agreed preference for an initial in-person assessment. |
| Maganty, et al. (2020) [30] USA | Evaluate differences in patient populations being evaluated for cancer before and during the COVID-19 pandemic | Teleconsultations/virtual appointments for patients |
|
| Mahl et al. (2020) [63] Brazil | Evaluate delays in care for patients with head and neck cancer in post-treatment follow-up or palliative care during the COVID-19 pandemic | - |
|
| Merz et al. (2021) [43] Italy | Assess breast cancer survivors perceptions electronic medical record-assisted telephone follow-up | Electronic medical record-assisted telephone consulation/appointment. |
|
| Mitra, et al. (2020) [64] India | Study the challenges faced by cancer patients in India during the COVID-19 pandemic | Teleconsultations/virtual appointments for patients |
|
| Narayanan et al. (2021) [44] USA | Report on the feasibility of conducting Integrative Oncology physician consultations via telehealth | Teleconsultations/virtual appointments for patients |
|
| Parikh, et al. (2020) [61] USA | Evaluate changes in resource use associated with the transition to telemedicine in a radiation oncology department | Teleconsultations/virtual appointments for patients |
|
| Patt et al. (2020a) [65] USA | Gain insights into the impact of COVID-19 on the US senior cancer population | Teleconsultations/virtual appointments for patients |
|
| Patt, et al. (2020b) [54] USA | (1) Describe onboarding and utilization of telemedicine across a large statewide community oncology practice (2) Evaluate trends, barriers, and opportunities in care delivery during the coronavirus disease 2019 pandemic | Teleconsultations/virtual appointments for patients Virtual support groups (social workers provided) & tele-pharmacy |
|
| Patt et al (2021) [53] USA | Assess the implementation of multidisciplinary telemedicine in community oncology; providers and patients satisfaction; changes in clinic operations; opportunities and barriers | Teleconsultations/virtual appointments for patients |
|
| Rodler et al (2020) [57] Germany | Determine patients’ perceptions on adoption of telehealth as a response to the pandemic and its sustainability in the future | Teleconsultations/virtual appointments for patients Video conferencing |
|
| Romani et al. (2021) [32] Canada | Examine the effect of the COVID-19 pandemic on the operation of satellite radiation oncology facility and patient satisfaction | Teleconsultations/virtual appointments for patients |
|
| Sawka, et al. (2021) [37] Canada | Describe the management of small low risk papillary thyroid cancer during the COVID-19 pandemic | Telephone and video communciations. |
|
| Shannon, et al. (2020) [45] USA | Determine how visit and genetic testing volume was impacted by new telephone genetic counselling and home testing. | New telephone genetic counselling and home testing. |
|
| Smrke, et al. (2020) [55] UK | Evaluate the impact of telemedicine on patients, clinicians, care delivery | Teleconsultations/virtual appointments for patients |
|
| Somani et al. (2020) [58] UK | Assess outpatient and telemedicine (phone and video) volume during the pandemic. | Teleconsultations/virtual appointments (telephone and video) for patients |
|
| Sonagli et al. (2021) [46] Brazil | Demonstrate how telemedicine was an efficient tool to maintain outpatient appointments for breast cancer patients follow up and surveillance | Teleconsultations/virtual appointments (video) for patients |
|
| Wai et al. (2020) [41] USA | Explore the impact on surgical care of head & neck cancer patients |
| |
| Wu et al. (2020) [52] Taiwan | Assess smartphone enabled telehealth model for palliative care family conferences | Video conferencing |
|
| Zuliani et al. (2020) [60] Italy | Analyse COVID-19 related organisational changes. | Teleconsultations/virtual appointments (telephone) for patients |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murphy, A.; Kirby, A.; Lawlor, A.; Drummond, F.J.; Heavin, C. Mitigating the Impact of the COVID-19 Pandemic on Adult Cancer Patients through Telehealth Adoption: A Systematic Review. Sensors 2022, 22, 3598. https://doi.org/10.3390/s22093598
Murphy A, Kirby A, Lawlor A, Drummond FJ, Heavin C. Mitigating the Impact of the COVID-19 Pandemic on Adult Cancer Patients through Telehealth Adoption: A Systematic Review. Sensors. 2022; 22(9):3598. https://doi.org/10.3390/s22093598
Chicago/Turabian StyleMurphy, Aileen, Ann Kirby, Amy Lawlor, Frances J. Drummond, and Ciara Heavin. 2022. "Mitigating the Impact of the COVID-19 Pandemic on Adult Cancer Patients through Telehealth Adoption: A Systematic Review" Sensors 22, no. 9: 3598. https://doi.org/10.3390/s22093598
APA StyleMurphy, A., Kirby, A., Lawlor, A., Drummond, F. J., & Heavin, C. (2022). Mitigating the Impact of the COVID-19 Pandemic on Adult Cancer Patients through Telehealth Adoption: A Systematic Review. Sensors, 22(9), 3598. https://doi.org/10.3390/s22093598