
Label-Free Uric Acid Estimation of Spot Urine Using Portable Device Based on UV Spectrophotometry

 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
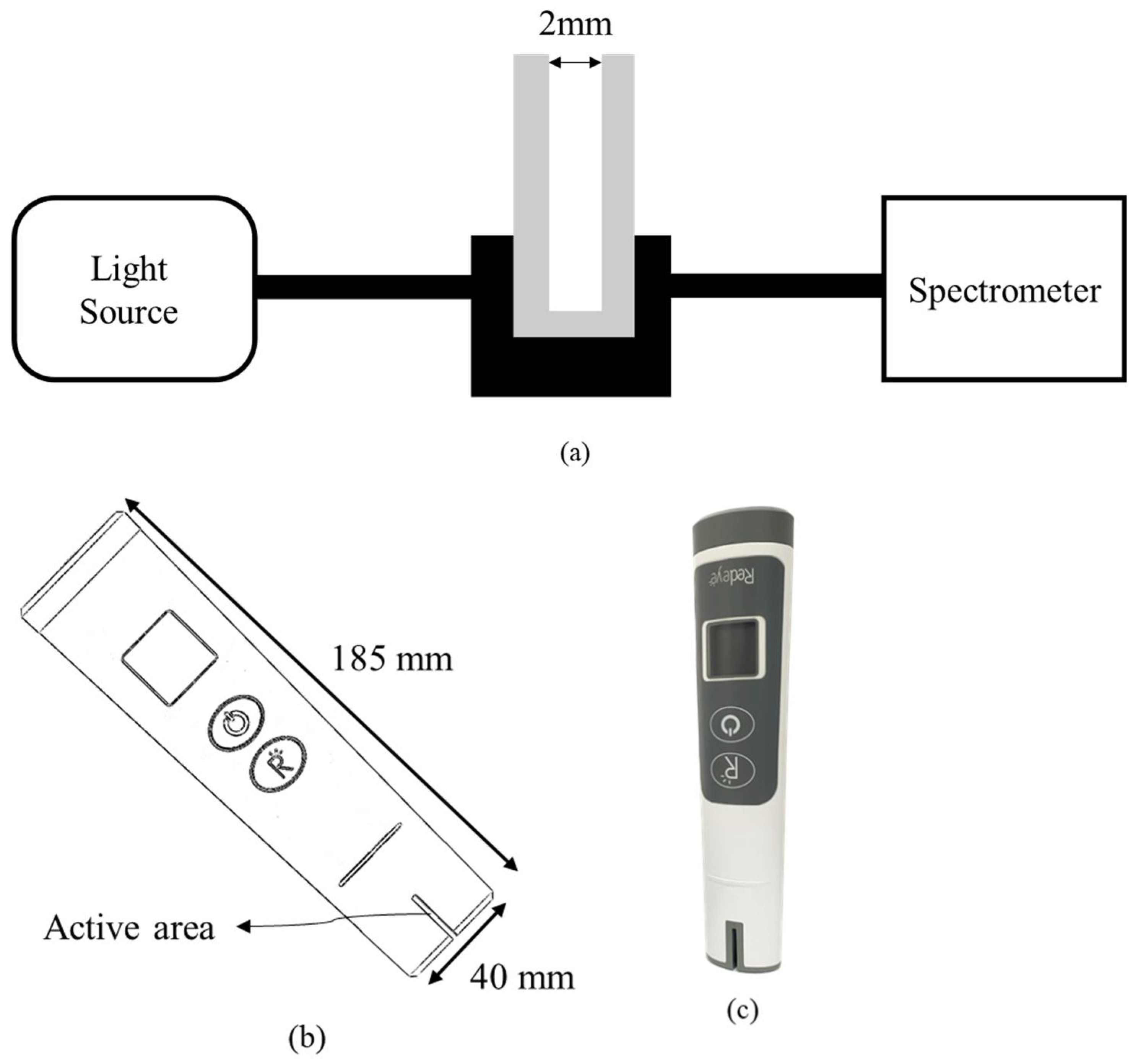
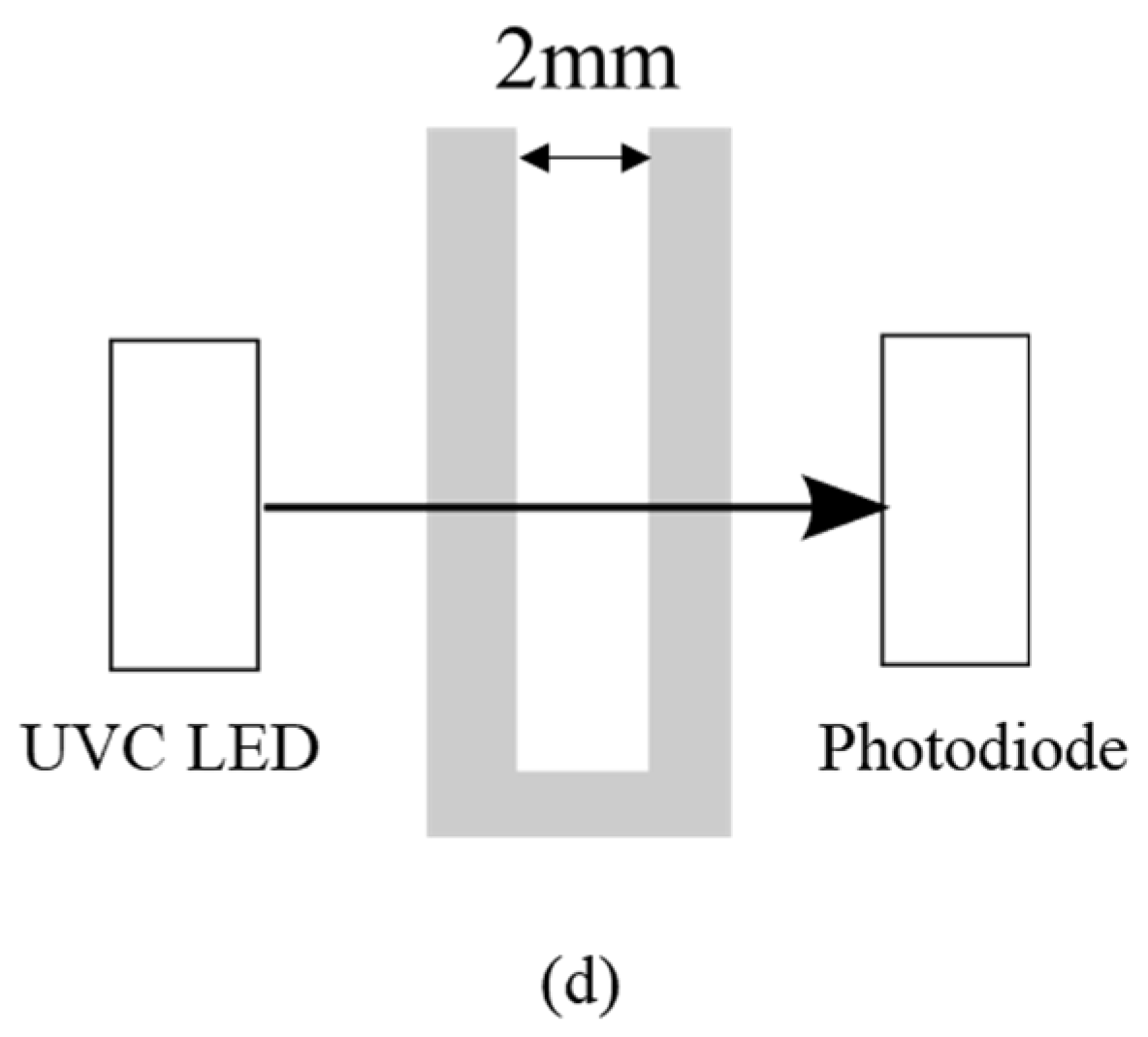
2. Materials and Methods
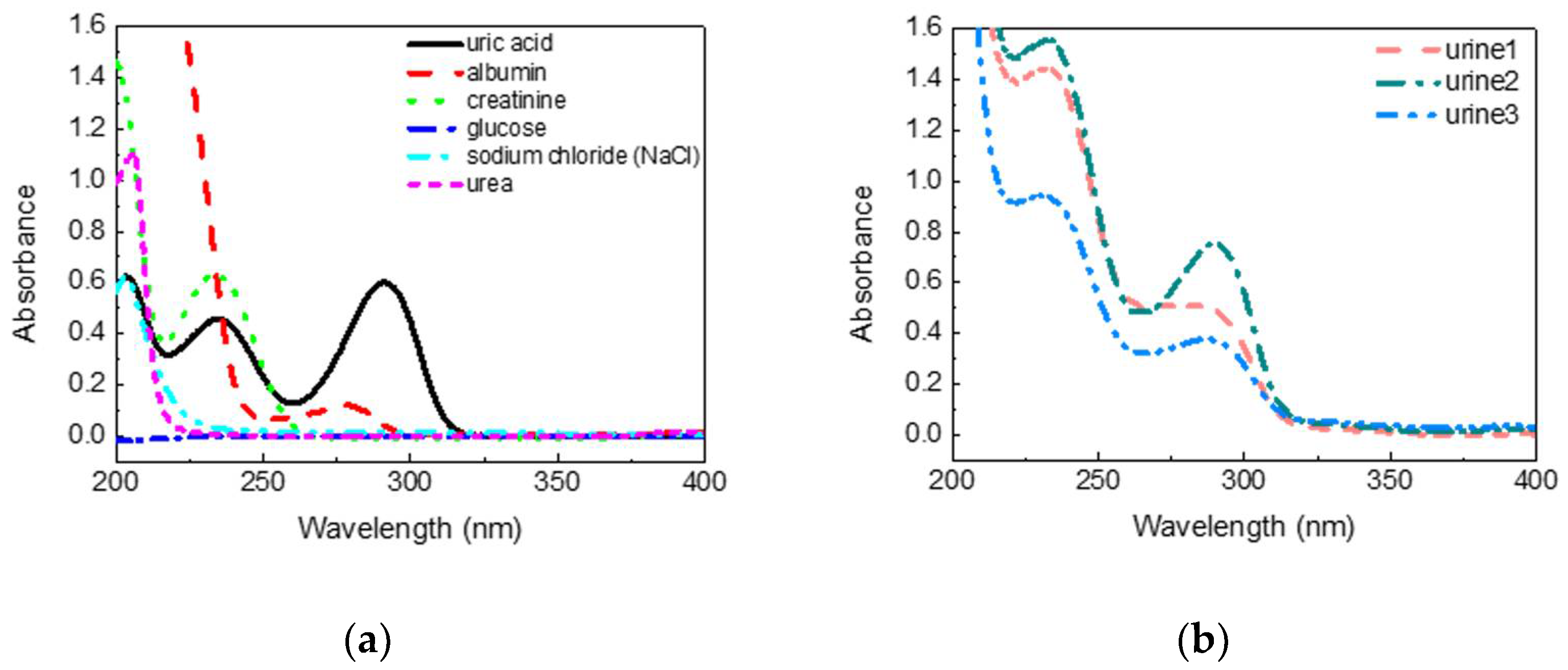
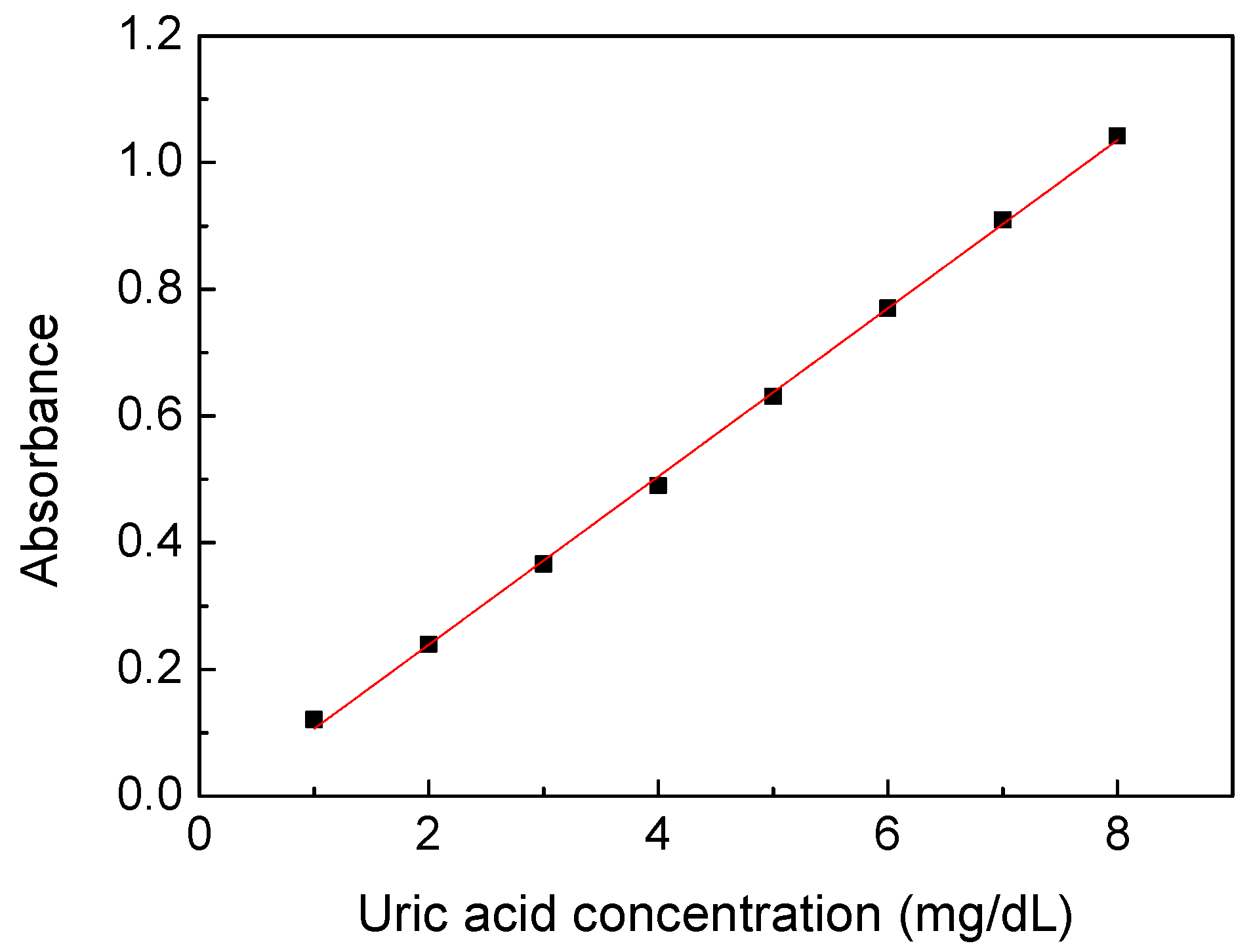
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dehlin, M.; Jacobsson, L.; Roddy, E. Global Epidemiology of Gout: Prevalence, Incidence, Treatment Patterns and Risk Factors. Nat. Rev. Rheumatol. 2020, 16, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Hainer, B.L.; Matheson, E.M.; Wilkes, R.T. Diagnosis, Treatment, and Prevention of Gout. AFP 2014, 90, 831–836. [Google Scholar] [PubMed]
- Johnson, R.J.; Kang, D.-H.; Feig, D.; Kivlighn, S.; Kanellis, J.; Watanabe, S.; Tuttle, K.R.; Rodriguez-Iturbe, B.; Herrera-Acosta, J.; Mazzali, M. Is There a Pathogenetic Role for Uric Acid in Hypertension and Cardiovascular and Renal Disease? Hypertension 2003, 41, 1183–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perticone, M.; Tripepi, G.; Maio, R.; Cimellaro, A.; Addesi, D.; Baggetta, R.; Sciacqua, A.; Sesti, G.; Perticone, F. Risk Reclassification Ability of Uric Acid for Cardiovascular Outcomes in Essential Hypertension. Int. J. Cardiol. 2017, 243, 473–478. [Google Scholar] [CrossRef]
- Liu, J.; Xu, C.; Ying, L.; Zang, S.; Zhuang, Z.; Lv, H.; Yang, W.; Luo, Y.; Ma, X.; Wang, L.; et al. Relationship of Serum Uric Acid Level with Non-Alcoholic Fatty Liver Disease and Its Inflammation Progression in Non-Obese Adults. Hepatol. Res. 2017, 47, E104–E112. [Google Scholar] [CrossRef] [Green Version]
- Pellecchia, M.T.; Savastano, R.; Moccia, M.; Picillo, M.; Siano, P.; Erro, R.; Vallelunga, A.; Amboni, M.; Vitale, C.; Santangelo, G.; et al. Lower Serum Uric Acid Is Associated with Mild Cognitive Impairment in Early Parkinson’s Disease: A 4-Year Follow-up Study. J. Neural Transm. 2016, 123, 1399–1402. [Google Scholar] [CrossRef]
- Sorensen, C.M.; Chandhoke, P.S. Hyperuricosuric Calcium Nephrolithiasis. Endocrinol. Metab. Clin. 2002, 31, 915–925. [Google Scholar] [CrossRef]
- Kaur, P.; Bhatt, H. Hyperuricosuria; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Clifford, A.J.; Riumallo, J.A.; Young, V.R.; Scrimshaw, N.S. Effect of Oral Purines on Serum and Urinary Uric Acid of Normal, Hyperuricemic and Gouty Humans. J. Nutr. 1976, 106, 428–434. [Google Scholar] [CrossRef]
- Choi, H.K.; Atkinson, K.; Karlson, E.W.; Willett, W.; Curhan, G. Purine-Rich Foods, Dairy and Protein Intake, and the Risk of Gout in Men. N. Engl. J. Med. 2004, 350, 1093–1103. [Google Scholar] [CrossRef] [Green Version]
- Shirish, M. Kawthalkar Essential of Clinical Pathology; Jaypee Brothers Medical Publishers (P) Ltd.: New Delhi, India, 2010; ISBN 978-93-80704-19-7. [Google Scholar]
- Yamakita, J.; Yamamoto, T.; Moriwaki, Y.; Takahashi, S.; Tsutsumi, Z.; Hada, T. Effect of Urine Storage on Urinary Uric Acid Concentrations. Ann. Clin. Biochem. 2000, 37, 355–359. [Google Scholar] [CrossRef]
- Shojaei-Far, Z.; Razi, F.; Bandarian, F.; Rambod, C.; Qorbani, M. A Detailed Comparison of Morning and Random Urine Specimen Levels with 24 Hour Urinary Excretion Levels of Seven Biochemical Parameters with a Proposed Formula. Ann. Clin. Lab. Sci. 2017, 47, 201–207. [Google Scholar] [PubMed]
- Fathallah-Shaykh, S.A.; Cramer, M.T. Uric Acid and the Kidney. Pediatr. Nephrol. 2014, 29, 999–1008. [Google Scholar] [CrossRef] [PubMed]
- Moriwaki, Y.; Yamamoto, T.; Takahashi, S.; Yamakita, J.; Tsutsumi, Z.; Hada, T. Spot Urine Uric Acid to Creatinine Ratio Used in the Estimation of Uric Acid Excretion in Primary Gout. J. Rheumatol. 2001, 28, 1306–1310. [Google Scholar] [PubMed]
- Choi, S.; Moon, S.-J.; Kang, E.-J.; Lee, K.-H. FRI0248 Validity of Random Urinary Uric Acid-to-Creatinine Ratio for Estimating 24-Hour Urine Uric Acid Excretion in Patients with Gout. Ann. Rheum. Dis. 2018, 77, 664–665. [Google Scholar] [CrossRef]
- Choi, S.T.; Song, J.S.; Kim, S.J.; Kim, C.H.; Moon, S.J. The Utility of the Random Urine Uric Acid-to-Creatinine Ratio for Patients with Gout Who Need Uricosuric Agents: Retrospective Cross-Sectional Study. J. Korean Med. Sci. 2020, 35, e95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, T.; Moriwaki, Y.; Takahashi, S.; Tsutsumi, Z.; Ka, T.; Fukuchi, M.; Hada, T. A Simple Method of Selecting Gout Patients for Treatment with Uricosuric Agents, Using Spot Urine and Blood Samples. J. Rheumatol. 2002, 29, 1937–1941. [Google Scholar]
- Decaux, G.; Musch, W. Estimated Daily Urine Volume and Solute Excretion from Spot Urine Samples to Guide the Therapy of Hyponatremia in SIADH. J. Clin. Med. 2019, 8, 1511. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Wen, X.; Kong, J. Recent Progress on Uric Acid Detection: A Review. Crit. Rev. Anal. Chem. 2020, 50, 359–375. [Google Scholar] [CrossRef]
- Fossati, P.; Prencipe, L.; Berti, G. Use of 3,5-Dichloro-2-Hydroxybenzenesulfonic Acid/4-Aminophenazone Chromogenic System in Direct Enzymic Assay of Uric Acid in Serum and Urine. Clin. Chem. 1980, 26, 227–231. [Google Scholar] [CrossRef]
- Bregnhøj, M.; Dichmann, L.; McLoughlin, C.K.; Westberg, M.; Ogilby, P.R. Uric Acid: A Less-than-Perfect Probe for Singlet Oxygen. Photochem. Photobiol. 2019, 95, 202–210. [Google Scholar] [CrossRef] [Green Version]
- Norazmi, N.; Rasad, Z.R.A.; Mohamad, M.; Manap, H. Uric Acid Detection Using Uv-Vis Spectrometer. In Proceedings of the IOP Conference Series: Materials Science and Engineering, Kuantan, Pahang, Malaysia, 1–2 August 2017; Volume 257, p. 012031. [Google Scholar] [CrossRef] [Green Version]
- Milena, J.-S.; Djurdjevic, P.; Dejan, S. Determination of Uric Acid in Human Serum by an Enzymatic Method Using N-Methyl-N-(4-Aminophenyl)-3-Methoxyaniline Reagent. J. Serb. Chem. Soc. 2003, 68. [Google Scholar] [CrossRef]
- Rose, C.; Parker, A.; Jefferson, B.; Cartmell, E. The Characterization of Feces and Urine: A Review of the Literature to Inform Advanced Treatment Technology. Crit. Rev. Environ. Sci. Technol. 2015, 45, 1827–1879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cockell, C.S.; Knowland, J. Ultraviolet Radiation Screening Compounds. Biol. Rev. 1999, 74, 311–345. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, T.-J.; Yen, K.-T.; Chen, C.-F.; Yan, S.-T.; Su, K.-W.; Chiang, Y.-L. Label-Free Uric Acid Estimation of Spot Urine Using Portable Device Based on UV Spectrophotometry. Sensors 2022, 22, 3009. https://doi.org/10.3390/s22083009
Lin T-J, Yen K-T, Chen C-F, Yan S-T, Su K-W, Chiang Y-L. Label-Free Uric Acid Estimation of Spot Urine Using Portable Device Based on UV Spectrophotometry. Sensors. 2022; 22(8):3009. https://doi.org/10.3390/s22083009
Chicago/Turabian StyleLin, Tsung-Jui, Kai-Ting Yen, Chien-Fan Chen, Shuo-Ting Yan, Kuan-Wei Su, and Ya-Ling Chiang. 2022. "Label-Free Uric Acid Estimation of Spot Urine Using Portable Device Based on UV Spectrophotometry" Sensors 22, no. 8: 3009. https://doi.org/10.3390/s22083009
APA StyleLin, T.-J., Yen, K.-T., Chen, C.-F., Yan, S.-T., Su, K.-W., & Chiang, Y.-L. (2022). Label-Free Uric Acid Estimation of Spot Urine Using Portable Device Based on UV Spectrophotometry. Sensors, 22(8), 3009. https://doi.org/10.3390/s22083009