
Development of a Prototype Overground Pelvic Obliquity Support Robot for Rehabilitation of Hemiplegia Gait

 , , ,
, , , 
Abstract
1. Introduction
2. Design Objective and Requirements
2.1. Research Background: Hemiplegia Patients Gait
2.2. Design Objective for Body Weight Support, Pelvic Obliquity Motion Support, and Multiple Degrees-of-Freedom Movements
2.3. Design Objective for Overground Gait Rehabilitation
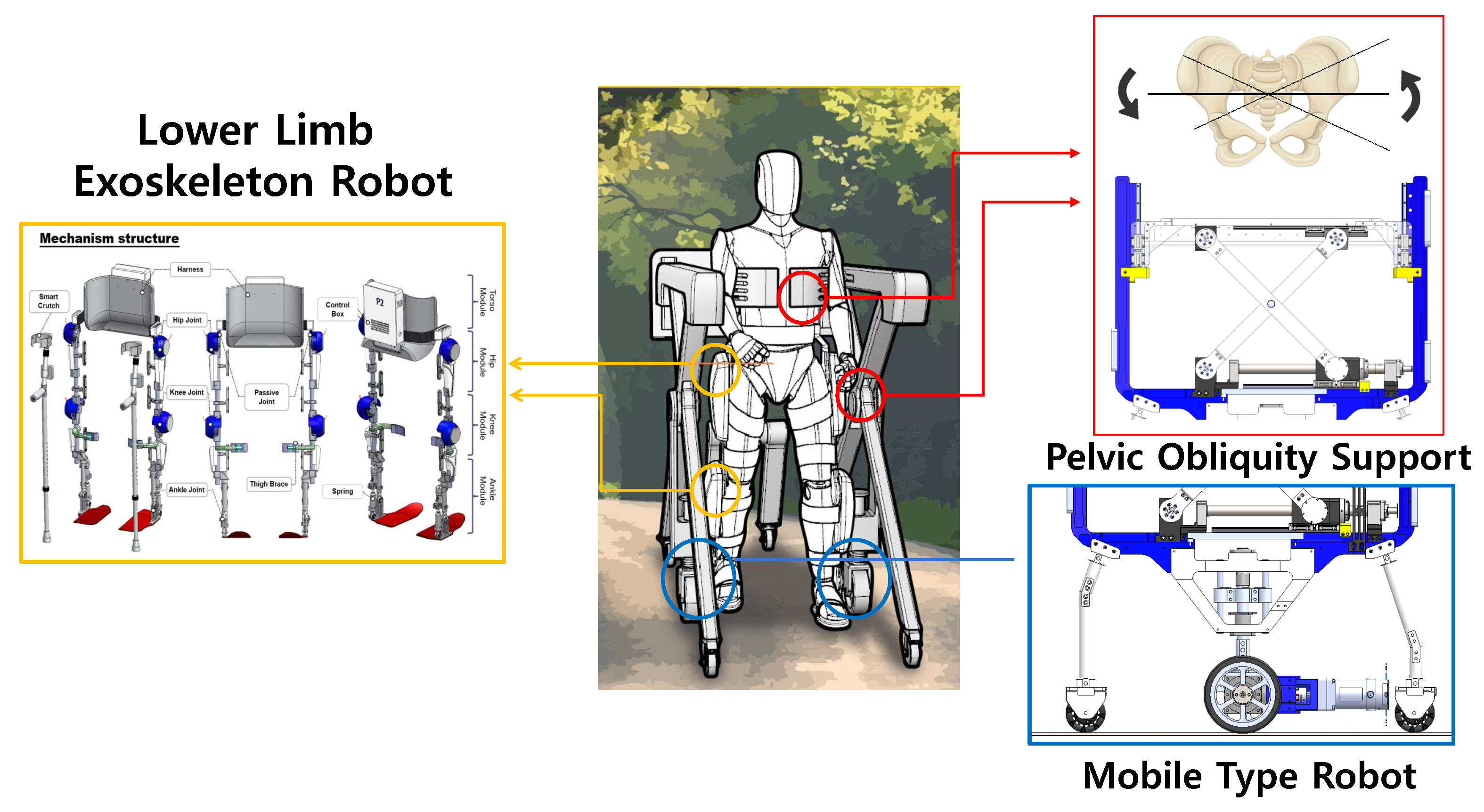
3. Pelvic Obliquity Support Robot Design
3.1. Detailed Design of Scissor Mechanism for BWS and Pelvic Obliquity Support
3.2. Detailed Design of Mobile Type Robot for Overground Gait Rehabilitation
3.3. Detailed Design of the Lower-Limb Exoskeleton Robot for Multiple Degrees of Freedom
4. System Verification and Result
4.1. CAE Verification of Scissor Mechanism and Mobile Driving
4.2. Multiple Degrees-of-Freedom Gait Rehabilitation Motion Control Verification of Scissor Mechanism with Lower-Limb Exoskeleton Robot
5. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart disease and stroke statistics—2020 update: A report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Whittle, M.W. Gait Analysis: An Introduction; Butterworth-Heinemann: Oxford, UK, 2014. [Google Scholar]
- Perry, J.; Burnfield, J. Gait Analysis: Normal and Pathological Function; Slack Inc.: Thorofare, NJ, USA, 1992. [Google Scholar]
- Murtagh, E.M.; Murphy, M.H.; Boone-Heinonen, J. Walking–the first steps in cardiovascular disease prevention. Curr. Opin. Cardiol. 2010, 25, 490. [Google Scholar] [CrossRef] [PubMed]
- Nas, K.; Yazmalar, L.; Şah, V.; Aydın, A.; Öneş, K. Rehabilitation of spinal cord injuries. World J. Orthop. 2015, 6, 8. [Google Scholar] [CrossRef] [PubMed]
- Pamungkas, D.S.; Caesarendra, W.; Soebakti, H.; Analia, R.; Susanto, S. Overview: Types of lower limb exoskeletons. Electronics 2019, 8, 1283. [Google Scholar] [CrossRef]
- Asbeck, A.T.; Schmidt, K.; Walsh, C.J. Soft exosuit for hip assistance. Robot. Auton. Syst. 2015, 73, 102–110. [Google Scholar] [CrossRef]
- Park, Y.L.; Chen, B.R.; Young, D.; Stirling, L.; Wood, R.J.; Goldfield, E.; Nagpal, R. Bio-inspired active soft orthotic device for ankle foot pathologies. In Proceedings of the 2011 IEEE/RSJ International Conference on Intelligent Robots and Systems, Daejeon, Korea, 9–14 October 2011; pp. 4488–4495. [Google Scholar]
- Kuo, A.D.; Donelan, J.M. Dynamic principles of gait and their clinical implications. Phys. Ther. 2010, 90, 157–174. [Google Scholar] [CrossRef]
- Wang, C.Y.E.; Bobrow, J.E.; Reinkensmeyer, D.J. Swinging from the hip: Use of dynamic motion optimization in the design of robotic gait rehabilitation. In Proceedings of the 2001 ICRA, IEEE International Conference on Robotics and Automation (Cat.No. 01CH37164), Seoul, Korea, 21–26 May 2001; Volume 2, pp. 1433–1438. [Google Scholar]
- Sjödahl, C.; Jarnlo, G.B.; Söderberg, B.; Persson, B. Pelvic motion in trans-femoral amputees in the frontal and transverse plane before and after special gait re-education. Prosthetics Orthot. Int. 2003, 27, 227–237. [Google Scholar] [CrossRef][Green Version]
- Mun, K.R.; Guo, Z.; Yu, H. Development and evaluation of a novel overground robotic walker for pelvic motion support. In Proceedings of the 2015 IEEE International Conference on Rehabilitation Robotics (ICORR), Singapore, 11–14 August 2015; pp. 95–100. [Google Scholar]
- Aoyagi, D.; Ichinose, W.E.; Harkema, S.J.; Reinkensmeyer, D.J.; Bobrow, J.E. A robot and control algorithm that can synchronously assist in naturalistic motion during body-weight-supported gait training following neurologic injury. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 387–400. [Google Scholar] [CrossRef]
- Stauffer, Y.; Allemand, Y.; Bouri, M.; Fournier, J.; Clavel, R.; Metrailler, P.; Brodard, R.; Reynard, F. Pelvic motion measurement during over ground walking, analysis and implementation on the WalkTrainer reeducation device. In Proceedings of the 2008 IEEE/RSJ International Conference on Intelligent Robots and Systems, Nice, France, 22–26 September 2008; pp. 2362–2367. [Google Scholar]
- Kang, J.; Martelli, D.; Vashista, V.; Martinez-Hernandez, I.; Kim, H.; Agrawal, S.K. Robot-driven downward pelvic pull to improve crouch gait in children with cerebral palsy. Sci. Robot. 2017, 2, eaan2634. [Google Scholar] [CrossRef]
- Musselman, K.E.; Fouad, K.; Misiaszek, J.E.; Yang, J.F. Training of walking skills overground and on the treadmill: Case series on individuals with incomplete spinal cord injury. Phys. Ther. 2009, 89, 601–611. [Google Scholar] [CrossRef]
- Gama, G.L.; Celestino, M.L.; Barela, J.A.; Forrester, L.; Whitall, J.; Barela, A.M. Effects of gait training with body weight support on a treadmill versus overground in individuals with stroke. Arch. Phys. Med. Rehabil. 2017, 98, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Seo, K.H.; Lee, J.J. The development of two mobile gait rehabilitation systems. IEEE Trans. Neural Syst. Rehabil. Eng. 2009, 17, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Zou, Y.; Wang, N.; Wang, X.; Ma, H.; Liu, K. Design and experimental research of movable cable-driven lower limb rehabilitation robot. IEEE Access 2018, 7, 2315–2326. [Google Scholar] [CrossRef]
- Stramel, D.M.; Agrawal, S.K. Validation of a Forward Kinematics Based Controller for a mobile Tethered Pelvic Assist Device to Augment Pelvic Forces during Walking. In Proceedings of the 2020 IEEE International Conference on Robotics and Automation (ICRA), Paris, France, 31 May–31 August 2020; pp. 10133–10139. [Google Scholar]
- Hwang, S.H.; Sun, D.I.; Han, J.; Kim, W.S. Gait pattern generation algorithm for lower-extremity rehabilitation–exoskeleton robot considering wearer’s condition. Intell. Serv. Robot. 2021, 14, 345–355. [Google Scholar] [CrossRef]
- Moon, S.B.; Ji, Y.H.; Jang, H.Y.; Hwang, S.H.; Shin, D.B.; Lee, S.C.; Han, J.S.; Han, C.S.; Lee, Y.G.; Jang, S.H.; et al. Gait analysis of hemiplegic patients in ambulatory rehabilitation training using a wearable lower-limb robot: A pilot study. Int. J. Precis. Eng. Manuf. 2017, 18, 1773–1781. [Google Scholar] [CrossRef]
- Brandstater, M.E.; de Bruin, H.; Gowland, C.; Clark, B.M. Hemiplegic gait: Analysis of temporal variables. Arch. Phys. Med. Rehabil. 1983, 64, 583–587. [Google Scholar] [PubMed]
- Woolley, S.M. Characteristics of gait in hemiplegia. Top. Stroke Rehabil. 2001, 7, 1–18. [Google Scholar] [CrossRef]
- Mauritz, K.H. Gait training in hemiplegia. Eur. J. Neurol. 2002, 9, 23–29. [Google Scholar] [CrossRef]
- Zeilig, G.; Weingarden, H.; Zwecker, M.; Dudkiewicz, I.; Bloch, A.; Esquenazi, A. Safety and tolerance of the ReWalk™ exoskeleton suit for ambulation by people with complete spinal cord injury: A pilot study. J. Spinal Cord Med. 2012, 35, 96–101. [Google Scholar] [CrossRef]
- Jezernik, S.; Colombo, G.; Keller, T.; Frueh, H.; Morari, M. Robotic orthosis lokomat: A rehabilitation and research tool. Neuromodul. Technol. Neural Interface 2003, 6, 108–115. [Google Scholar] [CrossRef]
- Sousa, C.O.; Barela, J.A.; Prado-Medeiros, C.L.; Salvini, T.F.; Barela, A.M. Gait training with partial body weight support during overground walking for individuals with chronic stroke: A pilot study. J. Neuroeng. Rehabil. 2011, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mikolajczyk, T.; Ciobanu, I.; Badea, D.I.; Iliescu, A.; Pizzamiglio, S.; Schauer, T.; Seel, T.; Seiciu, P.L.; Turner, D.L.; Berteanu, M. Advanced technology for gait rehabilitation: An overview. Adv. Mech. Eng. 2018, 10, 3627. [Google Scholar] [CrossRef]
- Castro, M.N.; Rasmussen, J.; Andersen, M.S.; Bai, S. A compact 3-DOF shoulder mechanism constructed with scissors linkages for exoskeleton applications. Mech. Mach. Theory 2019, 132, 264–278. [Google Scholar] [CrossRef]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | m | g | |
|---|---|---|---|
| Value | 100 kg | m/s |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, S.; Lee, S.; Shin, D.; Baek, I.; Ham, S.; Kim, W. Development of a Prototype Overground Pelvic Obliquity Support Robot for Rehabilitation of Hemiplegia Gait. Sensors 2022, 22, 2462. https://doi.org/10.3390/s22072462
Hwang S, Lee S, Shin D, Baek I, Ham S, Kim W. Development of a Prototype Overground Pelvic Obliquity Support Robot for Rehabilitation of Hemiplegia Gait. Sensors. 2022; 22(7):2462. https://doi.org/10.3390/s22072462
Chicago/Turabian StyleHwang, Seunghoon, Seungchan Lee, Dongbin Shin, Inhyuk Baek, Seoyeon Ham, and Wansoo Kim. 2022. "Development of a Prototype Overground Pelvic Obliquity Support Robot for Rehabilitation of Hemiplegia Gait" Sensors 22, no. 7: 2462. https://doi.org/10.3390/s22072462
APA StyleHwang, S., Lee, S., Shin, D., Baek, I., Ham, S., & Kim, W. (2022). Development of a Prototype Overground Pelvic Obliquity Support Robot for Rehabilitation of Hemiplegia Gait. Sensors, 22(7), 2462. https://doi.org/10.3390/s22072462