
Reliability of IMU-Derived Temporal Gait Parameters in Neurological Diseases

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Gait Assessment
2.3. Data Processing
2.4. Statistical Analysis
3. Results
3.1. 4 m Walk
3.2. 20 m Walk
3.3. 20 m Walk (Steady State)
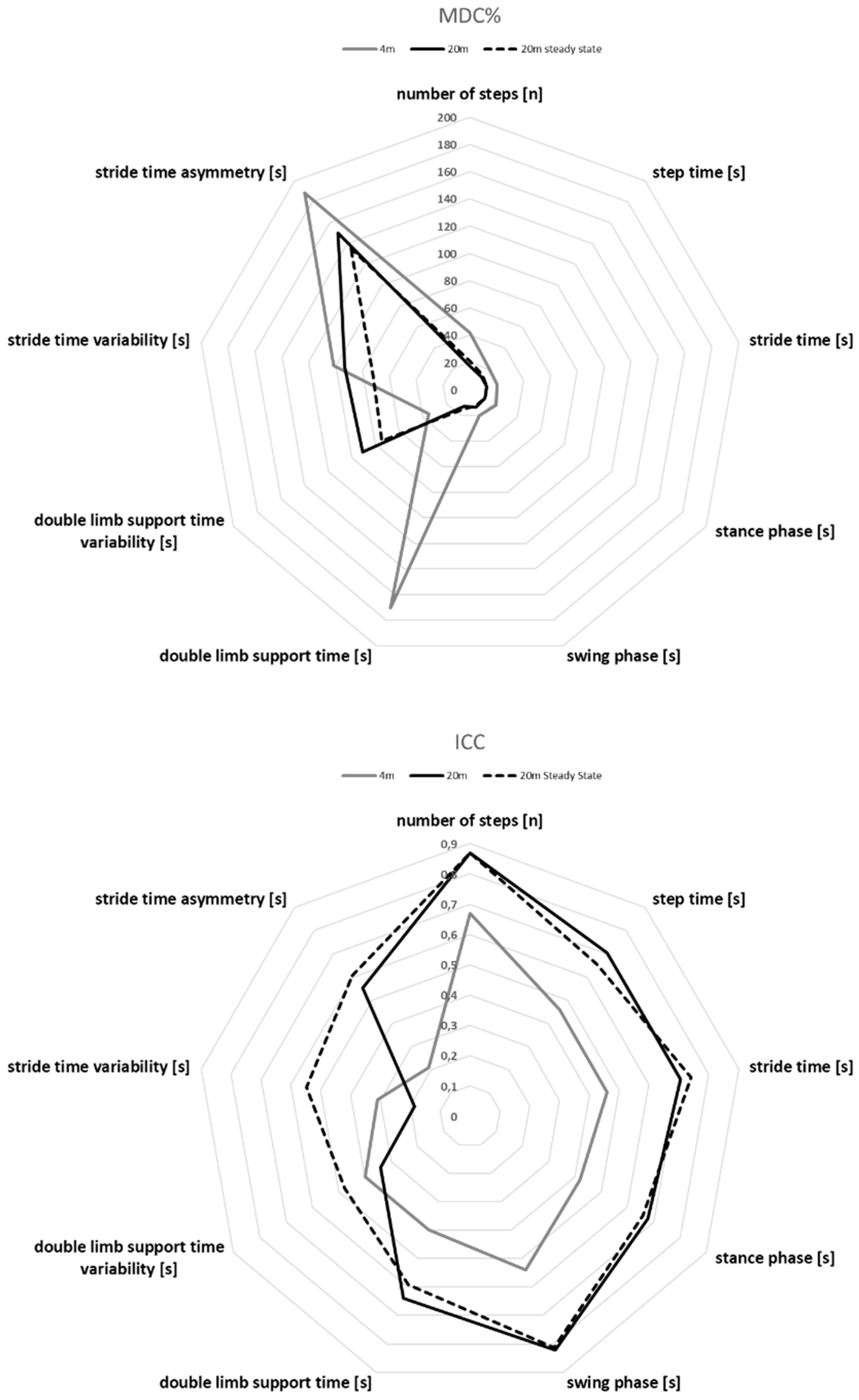
3.4. MDC% Values of All Parameters and Experimental Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schniepp, R.; Möhwald, K.; Wuehr, M. Clinical and automated gait analysis in patients with vestibular, cerebellar, and functional gait disorders: Perspectives and limitations. J. Neurol. 2019, 266, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.; Einarson, E.; Thomson, A.; Whiteley, R.; Witvrouw, E. Hamstring and calf muscle activation as a function of bodyweight support during treadmill running in ACL reconstructed athletes. Gait Posture 2017, 58, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Nigg, B.M.; Nurse, M.A.; Stefanyshyn, D.J. Shoe inserts and orthotics for sport and physical activities. Med. Sci. Sports Exerc. 1999, 31, S421–S428. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef]
- Mancini, M.; Horak, F.B.; Zampieri, C.; Carlson-Kuhta, P.; Nutt, J.G.; Chiari, L. Trunk accelerometry reveals postural instability in untreated Parkinson’s disease. Parkinsonism Relat. Disord. 2011, 17, 557–562. [Google Scholar] [CrossRef]
- Nez, A.; Fradet, L.; Marin, F.; Monnet, T.; Lacouture, P. Identification of noise covarianvce matrices to improve orientation estimation by kalman filter. Sensors 2018, 18, 3490. [Google Scholar] [CrossRef]
- Phan, G.-H.; Hansen, C.; Tommasino, P.; Hussain, A.; Formica, D.; Campolo, D. A complementary filter design on se (3) to identify micro-motions during 3d motion tracking. Sensors 2020, 20, 5864. [Google Scholar] [CrossRef]
- Vilas-Boas, M.d.C.; Choupina, H.M.P.; Rocha, A.P.; Fernandes, J.M.; Cunha, J.P.S. Full-body motion assessment: Concurrent validation of two body tracking depth sensors versus a gold standard system during gait. J. Biomech. 2019, 87, 189–196. [Google Scholar] [CrossRef]
- Hansen, C.; Beckbauer, M.; Romijnders, R.; Warmerdam, E.; Welzel, J.; Geritz, J.; Emmert, K.; Maetzler, W. Reliability of imu-derived static balance parameters in neurological diseases. Int. J. Environ. Res. Public Health 2021, 18, 3644. [Google Scholar] [CrossRef]
- Van der Kooij, H.; Jacobs, R.; Koopman, B.; Grootenboer, H. A multisensory integration model of human stance control. Biol. Cybern. 1999, 80, 299–308. [Google Scholar] [CrossRef]
- Salzman, B. Gait and balance disorders in older adults. Am. Fam. Physician 2010, 82, 61–68. [Google Scholar] [PubMed]
- Nikolaus, T. Gang, gleichgewicht und stürze-Ursachen und Konsequenzen. Dtsch. Med. Wochenschr. 2005, 130, 958–960. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nüesch, C.; Roos, E.; Pagenstert, G.; Mündermann, A. Measuring joint kinematics of treadmill walking and running: Comparison between an inertial sensor based system and a camera-based system. J. Biomech. 2017, 57, 32–38. [Google Scholar] [CrossRef]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Schwenk, M.; Gogulla, S.; Englert, S.; Czempik, A.; Hauer, K. Test-retest reliability and minimal detectable change of repeated sit-to-stand analysis using one body fixed sensor in geriatric patients. Physiol. Meas. 2012, 33, 1931–1946. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, G.; Nevill, A.M. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Hollman, J.H.; Beckman, B.A.; Brandt, R.A.; Merriwether, E.N.; Williams, R.T.; Nordrum, J.T. Minimum detectable change in gait velocity during acute rehabilitation following hip fracture. J. Geriatr. Phys. Ther. 2008, 31, 53–56. [Google Scholar] [CrossRef]
- Goldberg, A.; Casby, A.; Wasielewski, M. Minimum detectable change for single-leg-stance-time in older adults. Gait Posture 2011, 33, 737–739. [Google Scholar] [CrossRef]
- Geritz, J.; Maetzold, S.; Steffen, M.; Pilotto, A.; Corrà, M.F.; Moscovich, M.; Rizzetti, M.C.; Borroni, B.; Padovani, A.; Alpes, A.; et al. Motor, cognitive and mobility deficits in 1000 geriatric patients: Protocol of a quantitative observational study before and after routine clinical geriatric treatment—The ComOn-study. BMC Geriatr. 2020, 20, 45. [Google Scholar] [CrossRef]
- Lawton, M.; Kasten, M.; May, M.T.; Mollenhauer, B.; Schaumburg, M.; Liepelt-Scarfone, I.; Maetzler, W.; Vollstedt, E.-J.; Hu, M.T.M.; Berg, D.; et al. Validation of conversion between mini-mental state examination and Montreal cognitive assessment. Mov. Disord. 2016, 31, 593–596. [Google Scholar] [CrossRef]
- Pham, M.H.; Elshehabi, M.; Haertner, L.; del Din, S.; Srulijes, K.; Heger, T.; Synofzik, M.; Hobert, M.A.; Faber, G.S.; Hansen, C.; et al. Validation of a step detection algorithm during straight walking and turning in Patients with Parkinson’s disease and older adults using an inertial measurement unit at the lower back. Front. Neurol. 2017, 8, 457. [Google Scholar] [CrossRef] [PubMed]
- Strutzenberger, G.; Claußen, L.; Schwameder, H. Analysis of sloped gait: How many steps are needed to reach steady-state walking speed after gait initiation? Gait Posture 2021, 83, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Lexell, J.E.; Downham, D.Y. How to assess the reliability of measurements in rehabilitation. Am. J. Phys. Med. Rehabil. 2005, 84, 719–723. [Google Scholar] [CrossRef] [PubMed]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Haley, S.M.; Fragala-Pinkham, M.A. Interpreting Change Scores of Tests and Measures Used in Physical Therapy. Phys. Ther. 2006, 86, 735–743. [Google Scholar] [CrossRef]
- Kroneberg, D.; Elshehabi, M.; Meyer, A.-C.; Otte, K.; Doss, S.; Paul, F.; Nussbaum, S.; Berg, D.; Kühn, A.A.; Maetzler, W.; et al. Less is more—Estimation of the number of strides required to assess gait variability in spatially confined settings. Front. Aging Neurosci. 2019, 11, 435. [Google Scholar] [CrossRef]
- Paterson, K.L.; Hill, K.D.; Lythgo, N.D.; Maschette, W. The reliability of spatiotemporal gait data for young and older women during continuous overground walking. Arch. Phys. Med. Rehabil. 2008, 89, 2360–2365. [Google Scholar] [CrossRef]
- Brach, J.S.; Perera, S.; Studenski, S.; Newman, A.B. The reliability and validity of measures of gait variability in community-dwelling older adults. Arch. Phys. Med. Rehabil. 2008, 89, 2293–2296. [Google Scholar] [CrossRef]
- Steffen, T.; Seney, M. Test-retest reliability and minimal detectable change on balance and ambulation tests, the 36-item short-form health survey, and the unified parkinson disease rating scale in people with parkinsonism. Phys. Ther. 2008, 88, 733–746. [Google Scholar] [CrossRef]
- Quinn, N.P. Classification of fluctuations in patients with Parkinson’s disease. Neurology 1998, 51, S25–S29. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameter | Mean ± SD Day 1 | Mean ± SD Day 2 | ICC | Consistency Interpretation | SEM | MDC | MDC (%) |
|---|---|---|---|---|---|---|---|
| number of steps [n] | 8 ± 2 | 8 ± 2 | 0.67 | moderate | 1.15 | 3.19 | 42 |
| step time [s] | 0.66 ± 0.07 | 0.64 ± 0.07 | 0.46 | poor | 0.05 | 0.14 | 21 |
| stride time [s] | 1.30 ± 0.13 | 1.26 ± 0.13 | 0.46 | poor | 0.09 | 0.26 | 21 |
| stance time [s] | 0.81 ± 0.08 | 0.78 ± 0.08 | 0.42 | poor | 0.06 | 0.18 | 22 |
| swing time [s] | 0.49 ± 0.06 | 0.48 ± 0.06 | 0.54 | moderate | 0.03 | 0.1 | 20 |
| double limb support time [s] | 0.17 ± 0.03 | 0.16 ± 0.02 | 0.4 | poor | 0.02 | 0.06 | 35 |
| double limb support time variability [s] | 0.05 ± 0.04 | 0.05 ± 0.04 | 0.4 | poor | 0.03 | 0.08 | 170 |
| stride time variability [s] | 0.08 ± 0.04 | 0.09 ± 0.04 | 0.31 | poor | 0.03 | 0.09 | 101 |
| stride time asymmetry [s] | 0.06 ± 0.05 | 0.05 ± 0.04 | 0.21 | poor | 0.04 | 0.11 | 188 |
| Parameter | Mean ± SD Day 1 | Mean ± SD Day 2 | ICC | Consistency Interpretation | SEM | MDC | MDC (%) |
|---|---|---|---|---|---|---|---|
| number of steps [n] | 33 ± 5 | 34 ± 4 | 0.87 | good | 2.23 | 6.17 | 17 |
| step time [s] | 0.59 ± 0.06 | 0.58 ± 0.06 | 0.70 | moderate | 0.03 | 0.07 | 13 |
| stride time [s] | 1.17 ± 0.12 | 1.16 ± 0.11 | 0.71 | moderate | 0.05 | 0.14 | 12 |
| stance time [s] | 0.73 ± 0.08 | 0.72 ± 0.07 | 0.68 | moderate | 0.05 | 0.13 | 13 |
| swing time [s] | 0.45 ± 0.04 | 0.45 ± 0.05 | 0.82 | good | 0.01 | 0.02 | 14 |
| double limb support time [s] | 0.14 ± 0.01 | 0.14 ± 0.01 | 0.64 | moderate | 0.02 | 0.06 | 13 |
| double limb support time variability [s] | 0.01 ± 0.01 | 0.02 ± 0.01 | 0.34 | poor | 0.01 | 0.03 | 91 |
| stride time variability [s] | 0.04 ± 0.02 | 0.04 ± 0.02 | 0.19 | poor | 0.01 | 0.03 | 93 |
| stride time asymmetry [s] | 0.03 ± 0.02 | 0.03 ± 0.02 | 0.55 | moderate | 0.02 | 0.04 | 150 |
| Parameter | Mean ± SD Day 1 | Mean ± SD Day 2 | ICC | Consistency Interpretation | SEM | MDC | MDC (%) |
|---|---|---|---|---|---|---|---|
| number of steps [n] | 30 ± 6 | 31 ± 6 | 0.87 | good | 2.23 | 6.17 | 21 |
| step time [s] | 0.58 ± 0.05 | 0.57 ± 0.05 | 0.65 | moderate | 0.03 | 0.08 | 14 |
| stride time [s] | 1.15 ± 0.10 | 1.15 ± 0.10 | 0.74 | moderate | 0.05 | 0.14 | 12 |
| stance time [s] | 0.71 ± 0.06 | 0.71 ± 0.06 | 0.66 | moderate | 0.05 | 0.13 | 13 |
| swing time [s] | 0.44 ± 0.04 | 0.44 ± 0.04 | 0.81 | moderate | 0.01 | 0.02 | 13 |
| double limb support time [s] | 0.14 ± 0.01 | 0.13 ± 0.01 | 0.59 | moderate | 0.02 | 0.07 | 15 |
| double limb support time variability [s] | 0.01 ± 0.00 | 0.01 ± 0.00 | 0.48 | poor | 0.01 | 0.01 | 75 |
| stride time variability [s] | 0.03 ± 0.01 | 0.02 ± 0.01 | 0.55 | moderate | 0.01 | 0.02 | 72 |
| stride time asymmetry [s] | 0.03 ± 0.02 | 0.03 ± 0.02 | 0.60 | moderate | 0.01 | 0.03 | 135 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hansen, C.; Ortlieb, C.; Romijnders, R.; Warmerdam, E.; Welzel, J.; Geritz, J.; Maetzler, W. Reliability of IMU-Derived Temporal Gait Parameters in Neurological Diseases. Sensors 2022, 22, 2304. https://doi.org/10.3390/s22062304
Hansen C, Ortlieb C, Romijnders R, Warmerdam E, Welzel J, Geritz J, Maetzler W. Reliability of IMU-Derived Temporal Gait Parameters in Neurological Diseases. Sensors. 2022; 22(6):2304. https://doi.org/10.3390/s22062304
Chicago/Turabian StyleHansen, Clint, Christian Ortlieb, Robbin Romijnders, Elke Warmerdam, Julius Welzel, Johanna Geritz, and Walter Maetzler. 2022. "Reliability of IMU-Derived Temporal Gait Parameters in Neurological Diseases" Sensors 22, no. 6: 2304. https://doi.org/10.3390/s22062304
APA StyleHansen, C., Ortlieb, C., Romijnders, R., Warmerdam, E., Welzel, J., Geritz, J., & Maetzler, W. (2022). Reliability of IMU-Derived Temporal Gait Parameters in Neurological Diseases. Sensors, 22(6), 2304. https://doi.org/10.3390/s22062304