
Methodological Considerations in Assessing Interlimb Coordination on Poststroke Gait: A Scoping Review of Biomechanical Approaches and Outcomes

 ,
,  , ,
, , 
Abstract
:1. Introduction
- i.
- Which walking conditions have been considered to assess the interlimb coordination in poststroke adults?
- ii.
- What are the main instruments and outcomes that have been used to assess the interlimb coordination in poststroke adults?
2. Inclusion Criteria
3. Methods
3.1. Search Strategy
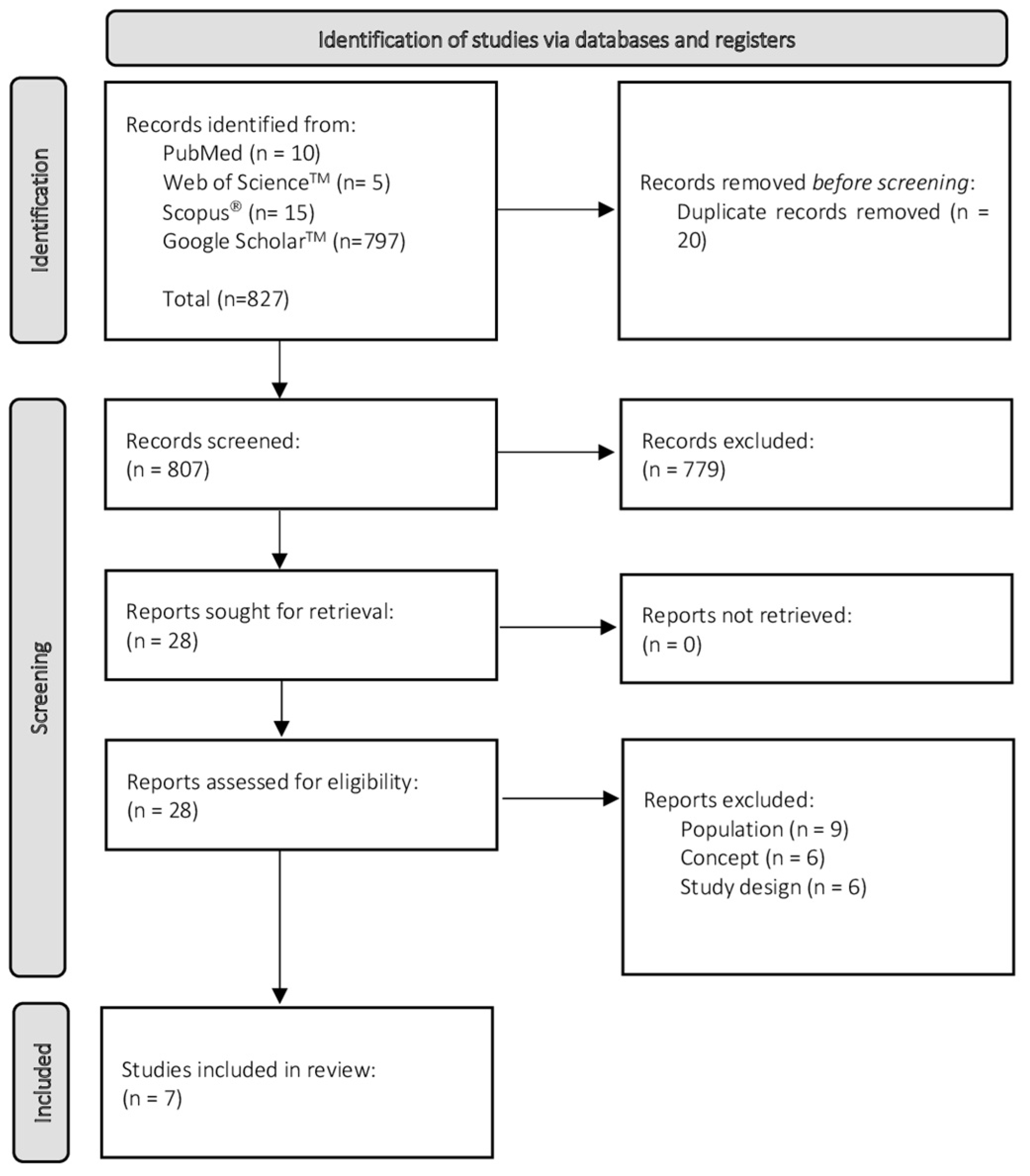
3.2. Source of Evidence Screening and Selection
3.3. Data Extraction
3.4. Analysis and Presentation of Results
4. Results
4.1. Study Design
4.2. Poststroke Participant’s Characteristics
4.3. Walking Conditions
4.4. Instruments
4.5. Main Outcomes and Significant Findings to Assess Interlimb Coordination, during Gait
5. Discussion
5.1. Walking Conditions
5.2. Instruments
5.3. Main Outcomes and Significant Findings to Assess Interlimb Coordination, during Gait
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35 (Suppl. 2), ii7–ii11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Translating Research into Clinical Practice, 5th ed.; Wilkins, L.W., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2017. [Google Scholar]
- Dietz, V. Do human bipeds use quadrupedal coordination? Trends Neurosci. 2002, 25, 462–467. [Google Scholar] [CrossRef]
- Swinnen, S.P.; Carson, R.G. The control and learning of patterns of interlimb coordination: Past and present issues in normal and disordered control. Acta Psychol. 2002, 110, 129–137. [Google Scholar] [CrossRef]
- Sousa, A.S.; Tavares, J.M. Interlimb Coordination During Step-to-Step Transition and Gait Performance. J. Mot. Behav. 2015, 47, 563–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donelan, J.M.; Kram, R.; Kuo, A.D. Mechanical work for step-to-step transitions is a major determinant of the metabolic cost of human walking. J. Exp. Biol. 2002, 205, 3717–3727. [Google Scholar] [CrossRef]
- Donelan, J.M.; Kram, R.; Kuo, A.D. Simultaneous positive and negative external mechanical work in human walking. J. Biomech. 2002, 35, 117–124. [Google Scholar] [CrossRef]
- Kuo, A.D. The six determinants of gait and the inverted pendulum analogy: A dynamic walking perspective. Hum. Mov. Sci. 2007, 26, 617–656. [Google Scholar] [CrossRef]
- Winter, D.A.; Eng, P. Kinetics: Our window into the goals and strategies of the central nervous system. Behav. Brain Res. 1995, 67, 111–120. [Google Scholar] [CrossRef]
- Bajwa, S.; Edgley, S.A.; Harrison, P.J. Crossed actions on group II-activated interneurones in the midlumbar segments of the cat spinal cord. J. Physiol. 1992, 455, 205–217. [Google Scholar] [CrossRef] [Green Version]
- Corna, S.; Galante, M.; Grasso, M.; Nardone, A.; Schieppati, M. Unilateral displacement of lower limb evokes bilateral EMG responses in leg and foot muscles in standing humans. Exp. Brain Res. 1996, 109, 83–91. [Google Scholar] [CrossRef]
- Dietz, V. Human neuronal control of automatic functional movements: Interaction between central programs and afferent input. Physiol. Rev. 1992, 72, 33–69. [Google Scholar] [CrossRef] [PubMed]
- Rossignol, S.; Dubuc, R.; Gossard, J.P. Dynamic sensorimotor interactions in locomotion. Physiol. Rev. 2006, 86, 89–154. [Google Scholar] [CrossRef] [PubMed]
- Zehr, E.P.; Duysens, J. Regulation of arm and leg movement during human locomotion. Neuroscientist 2004, 10, 347–361. [Google Scholar] [CrossRef]
- Drew, T.; Prentice, S.; Schepens, B. Cortical and brainstem control of locomotion. Prog. Brain Res. 2004, 143, 251–261. [Google Scholar] [CrossRef]
- Lacquaniti, F.; Ivanenko, Y.P.; Zago, M. Patterned control of human locomotion. J. Physiol. 2012, 590, 2189–2199. [Google Scholar] [CrossRef] [PubMed]
- Lacquaniti, F.; Ivanenko, Y.P.; Zago, M. Development of human locomotion. Curr. Opin. Neurobiol. 2012, 22, 822–828. [Google Scholar] [CrossRef] [Green Version]
- MacKay-Lyons, M. Central pattern generation of locomotion: A review of the evidence. Phys. Ther. 2002, 82, 69–83. [Google Scholar] [CrossRef]
- Matsuyama, K.; Mori, F.; Nakajima, K.; Drew, T.; Aoki, M.; Mori, S. Locomotor role of the corticoreticular-reticulospinal-spinal interneuronal system. Prog. Brain Res. 2004, 143, 239–249. [Google Scholar] [CrossRef]
- Kuo, A.D.; Donelan, J.M.; Ruina, A. Energetic consequences of walking like an inverted pendulum: Step-to-step transitions. Exerc. Sport Sci. Rev. 2005, 33, 88–97. [Google Scholar] [CrossRef]
- Geyer, H.; Seyfarth, A.; Blickhan, R. Compliant leg behaviour explains basic dynamics of walking and running. Proc. Biol. Sci. 2006, 273, 2861–2867. [Google Scholar] [CrossRef] [Green Version]
- Kuo, A.D. Energetics of actively powered locomotion using the simplest walking model. J. Biomech. Eng. 2002, 124, 113–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olney, S.J.; Richards, C. Hemiparetic gait following stroke. Part I: Characteristics. Gait Posture 1996, 4, 136–148. [Google Scholar] [CrossRef]
- Crafton, K.R.; Mark, A.N.; Cramer, S.C. Improved understanding of cortical injury by incorporating measures of functional anatomy. Brain 2003, 126, 1650–1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiemanck, S.K.; Kwakkel, G.; Post, M.W.; Kappelle, L.J.; Prevo, A.J. Predicting long-term independency in activities of daily living after middle cerebral artery stroke: Does information from MRI have added predictive value compared with clinical information? Stroke 2006, 37, 1050–1054. [Google Scholar] [CrossRef]
- Alagona, G.; Delvaux, V.; Gerard, P.; De Pasqua, V.; Pennisi, G.; Delwaide, P.J.; Nicoletti, F.; Maertens de Noordhout, A. Ipsilateral motor responses to focal transcranial magnetic stimulation in healthy subjects and acute-stroke patients. Stroke 2001, 32, 1304–1309. [Google Scholar] [CrossRef]
- Schaefer, S.Y.; Haaland, K.Y.; Sainburg, R.L. Hemispheric specialization and functional impact of ipsilesional deficits in movement coordination and accuracy. Neuropsychologia 2009, 47, 2953–2966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krasovsky, T.; Levin, M.F. Review: Toward a better understanding of coordination in healthy and poststroke gait. Neurorehabilit. Neural Repair 2010, 24, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Arya, K.N.; Pandian, S. Interlimb neural coupling: Implications for poststroke hemiparesis. Ann. Phys. Rehabil. Med. 2014, 57, 696–713. [Google Scholar] [CrossRef] [Green Version]
- Kuo, A.D.; Donelan, J.M. Dynamic principles of gait and their clinical implications. Phys. Ther. 2010, 90, 157–174. [Google Scholar] [CrossRef] [Green Version]
- Mohan, D.M.; Khandoker, A.H.; Wasti, S.A.; Ismail Ibrahim Ismail Alali, S.; Jelinek, H.F.; Khalaf, K. Assessment Methods of Post-stroke Gait: A Scoping Review of Technology-Driven Approaches to Gait Characterization and Analysis. Front. Neurol. 2021, 12, 885. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.; Sousa, A.S.; Silva, C.; Tavares, J.M.R.; Santos, R.; Sousa, F. Ankle antagonist coactivation in the double-support phase of walking: Stroke vs. healthy subjects. Somatosens. Mot. Res. 2015, 32, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Puh, U.; Baer, G.D. A comparison of treadmill walking and overground walking in independently ambulant stroke patients: A pilot study. Disabil. Rehabil. 2009, 31, 202–210. [Google Scholar] [CrossRef]
- Mahon, C.E.; Farris, D.J.; Sawicki, G.S.; Lewek, M.D. Individual limb mechanical analysis of gait following stroke. J. Biomech. 2015, 48, 984–989. [Google Scholar] [CrossRef] [Green Version]
- Sousa, A.S.P.; Silva, A.; Santos, R.; Sousa, F.; Tavares, J.M.R.S. Interlimb coordination during the stance phase of gait in subjects with stroke. Arch. Phys. Med. Rehabil. 2013, 94, 2515–2522. [Google Scholar] [CrossRef] [Green Version]
- Krasovsky, T.; Lamontagne, A.; Feldman, A.G.; Levin, M.F. Reduced gait stability in high-functioning poststroke individuals. J. Neurophysiol. 2013, 109, 77–88. [Google Scholar] [CrossRef] [Green Version]
- Reisman, D.S.; Wityk, R.; Silver, K.; Bastian, A.J. Split-belt treadmill adaptation transfers to overground walking in persons poststroke. Neurorehabilit. Neural Repair 2009, 23, 735–744. [Google Scholar] [CrossRef] [Green Version]
- Drużbicki, M.; Guzik, A.; Przysada, G.; Kwolek, A.; Brzozowska-Magoń, A.; Sobolewski, M. Changes in Gait Symmetry After Training on a Treadmill with Biofeedback in Chronic Stroke Patients: A 6-Month Follow-Up From a Randomized Controlled Trial. Med. Sci. Monit. 2016, 22, 4859–4868. [Google Scholar] [CrossRef] [Green Version]
- Carpinella, I.; Crenna, P.; Rabuffetti, M.; Ferrarin, M. Coordination between upper- and lower-limb movements is different during overground and treadmill walking. Eur. J. Appl. Physiol. 2010, 108, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Riley, P.O.; Paolini, G.; Della Croce, U.; Paylo, K.W.; Kerrigan, D.C. A kinematic and kinetic comparison of overground and treadmill walking in healthy subjects. Gait Posture 2007, 26, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Hidler, J. Biomechanics of overground vs. treadmill walking in healthy individuals. J. Appl. Physiol. 2008, 104, 747–755. [Google Scholar] [CrossRef]
- Awad, L.N.; Palmer, J.A.; Pohlig, R.T.; Binder-Macleod, S.A.; Reisman, D.S. Walking speed and step length asymmetry modify the energy cost of walking after stroke. Neurorehabilit. Neural Repair 2015, 29, 416–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corazza, S.; Mundermann, L.; Gambaretto, E.; Ferrigno, G.; Andriacchi, T.P. Markerless Motion Capture through Visual Hull, Articulated ICP and Subject Specific Model Generation. Int. J. Comput. Vis. 2010, 87, 156–169. [Google Scholar] [CrossRef]
- Maletsky, L.P.; Sun, J.T.; Morton, N.A. Accuracy of an optical active-marker system to track the relative motion of rigid bodies. J. Biomech. 2007, 40, 682–685. [Google Scholar] [CrossRef]
- van der Kruk, E.; Reijne, M.M. Accuracy of human motion capture systems for sport applications; state-of-the-art review. Eur. J. Sport Sci. 2018, 18, 806–819. [Google Scholar] [CrossRef]
- Panjkota, A.; Stancic, I.; Supuk, T. Outline of a Qualitative Analysis for the Human Motion in Case of Ergometer Rowing. In Proceedings of the 9th WSEAS International Conference on Simulation, Modelling and Optimization, Budapest, Hungary, 3–5 September 2009; pp. 182–186. [Google Scholar]
- Richards, J.G. The measurement of human motion: A comparison of commercially available systems. Hum. Mov. Sci. 1999, 18, 589–602. [Google Scholar] [CrossRef]
- Stancic, I.; Supuk, T.G.; Panjkota, A. Design, development and evaluation of optical motion-tracking system based on active white light markers. IET Sci. Meas. Technol. 2013, 7, 206–214. [Google Scholar] [CrossRef]
- Mantovani, G.; Lamontagne, M. How Different Marker Sets Affect Joint Angles in Inverse Kinematics Framework. J. Biomech. Eng. 2017, 139, 044503. [Google Scholar] [CrossRef]
- Della Croce, U.; Leardini, A.; Chiari, L.; Cappozzo, A. Human movement analysis using stereophotogrammetry Part 4: Assessment of anatomical landmark misplacement and its effects on joint kinematics. Gait Posture 2005, 21, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Garza-Ulloa, J. Chapter 3—Kinematic and kinetic measurements of human body. In Applied Biomechatronics Using Mathematical Models; Garza-Ulloa, J., Ed.; Academic Press: Cambridge, MA, USA, 2018; pp. 119–177. [Google Scholar]
- McManus, L.; De Vito, G.; Lowery, M.M. Analysis and Biophysics of Surface EMG for Physiotherapists and Kinesiologists: Toward a Common Language With Rehabilitation Engineers. Front. Neurol. 2020, 11, 1216. [Google Scholar] [CrossRef] [PubMed]
- Agostini, V.; Ghislieri, M.; Rosati, S.; Balestra, G.; Knaflitz, M. Surface Electromyography Applied to Gait Analysis: How to Improve Its Impact in Clinics? Front. Neurol. 2020, 11, 994. [Google Scholar] [CrossRef]
- Papagiannis, G.I.; Triantafyllou, A.I.; Roumpelakis, I.M.; Zampeli, F.; Garyfallia Eleni, P.; Koulouvaris, P.; Papadopoulos, E.C.; Papagelopoulos, P.J.; Babis, G.C. Methodology of surface electromyography in gait analysis: Review of the literature. J. Med. Eng. Technol. 2019, 43, 59–65. [Google Scholar] [CrossRef] [PubMed]
- PLUX Wireless Biosignals S.A., Biosignalsplux Wearable Body Sensing Platform. Available online: http://www.biosignalsplux.com/ (accessed on 29 December 2021).
- Balasubramanian, C.K.; Bowden, M.G.; Neptune, R.R.; Kautz, S.A. Relationship between step length asymmetry and walking performance in subjects with chronic hemiparesis. Arch. Phys. Med. Rehabil. 2007, 88, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Olney, S.J.; Griffin, M.P.; Mcbride, I.K. Temporal, Kinematic, and Kinetic Variables Related to Gait Speed in Subjects with Hemiplegia—A Regression Approach. Phys. Ther. 1994, 74, 872–885. [Google Scholar] [CrossRef]
- Sato, Y.; Yamada, N. Temporal coordination between ground reaction forces generated by leading and trailing limbs for propulsion during double stance phase in human walking. Gait Posture 2017, 54, 295–299. [Google Scholar] [CrossRef]
- Sousa, A.S.; Santos, R.; Oliveira, F.P.; Carvalho, P.; Tavares, J.M. Analysis of ground reaction force and electromyographic activity of the gastrocnemius muscle during double support. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2012, 226, 397–405. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Author, Year | Study Design | Poststroke Participant’s Characteristics | Walking Conditions | |
|---|---|---|---|---|
| Reisman et al., 2009 | Quasi-experimental |
| Overground walking
| |
| Puh & Bear, 2009 | Observational, transversal, analytical |
| Overground walkingand treadmill walking
| |
| Sousa et al., 2013 | Observational, transversal, analytical |
| Overground walking
| |
| Krasovsky et al., 2013 | Quasi-experimental |
| Treadmill walking
| |
| Mahon et al., 2015 | Observational, transversal, analytical | High-speed group
| Low-speed group
| Treadmill walking
|
| Silva et al., 2015 | Observational, transversal, analytical |
| Overground walking
| |
| Drużbicki et al., 2016 | Randomized Controlled Trial | Intervention group
| Control group
| Treadmill walking
|
| Author, Year | Instruments | Main Outcomes | Significant Findings to Assess Interlimb Coordination |
|---|---|---|---|
| Reisman et al., 2009 | Kinematic
| Spatiotemporal parameters:
| Interlimb symmetry of the spatiotemporal parameters |
| Puh & Bear, 2009 | Kinematic
| Spatiotemporal parameters:
| Interlimb symmetry of the spatiotemporal parameters using the formula: Interlimb symmetry ratio = 2NHP/(NHP + HP) Interlimb symmetry of the mean joint kinematics amplitude |
| Sousa et al., 2013 | Kinetic
| Ground reaction force:
| Percentage of the propulsive impulse = ∫Fytrail/(∫Fytrail + ∫Fylead) × 100 Statistic analisys through a correlation coefficient: Relation between contralesional limb electromyography and ipsilesional limb propulsive/braking impulse |
| Krasovsky et al., 2013 | Kinematic
| Temporal parameters:
| Interlimb symmetry of the double support duration |
| Mahon et al., 2015 | Kinetic
| Ground reaction force:
| Individual limb mechanical power on the CoM Propulsive impulse = Integral of positive Fy over a complete stride (HP and NHP) Paretic propulsion = PI HP/(PI HP + PI NHP) Step length asymmetry = Max NHP + Max HP/(NHP + HP) |
| Silva et al., 2015 | Electromyography
| Electromyograpic activity:
| Ankle antagonist coactivation (%) = (antagonist activity/(agonist + antagonist activity)) × 100 |
| Drużbicki et al., 2016 | Kinematic
| Spatiotemporal parameters:
| Interlimb symmetry index for spatiotemporal parameters and mean joint kinematics amplitude: = [(paretic − non-paretic)/0.5(paretic + non-paretic)] × 100% Interlimb symmetry ratio: = paretic/non-paretic of the spatiotemporal parameters and mean joint kinematics amplitude |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Couto, A.G.B.; Vaz, M.A.P.; Pinho, L.; Félix, J.; Silva, S.; Silva, A.; Sousa, A.S.P. Methodological Considerations in Assessing Interlimb Coordination on Poststroke Gait: A Scoping Review of Biomechanical Approaches and Outcomes. Sensors 2022, 22, 2010. https://doi.org/10.3390/s22052010
Couto AGB, Vaz MAP, Pinho L, Félix J, Silva S, Silva A, Sousa ASP. Methodological Considerations in Assessing Interlimb Coordination on Poststroke Gait: A Scoping Review of Biomechanical Approaches and Outcomes. Sensors. 2022; 22(5):2010. https://doi.org/10.3390/s22052010
Chicago/Turabian StyleCouto, Ana G. B., Mário A. P. Vaz, Liliana Pinho, José Félix, Sandra Silva, Augusta Silva, and Andreia S. P. Sousa. 2022. "Methodological Considerations in Assessing Interlimb Coordination on Poststroke Gait: A Scoping Review of Biomechanical Approaches and Outcomes" Sensors 22, no. 5: 2010. https://doi.org/10.3390/s22052010
APA StyleCouto, A. G. B., Vaz, M. A. P., Pinho, L., Félix, J., Silva, S., Silva, A., & Sousa, A. S. P. (2022). Methodological Considerations in Assessing Interlimb Coordination on Poststroke Gait: A Scoping Review of Biomechanical Approaches and Outcomes. Sensors, 22(5), 2010. https://doi.org/10.3390/s22052010